
Benefits of Metformin Combined with Pemetrexed-Based Platinum Doublets as a First-Line Therapy for Advanced Lung Adenocarcinoma Patients with Diabetes

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
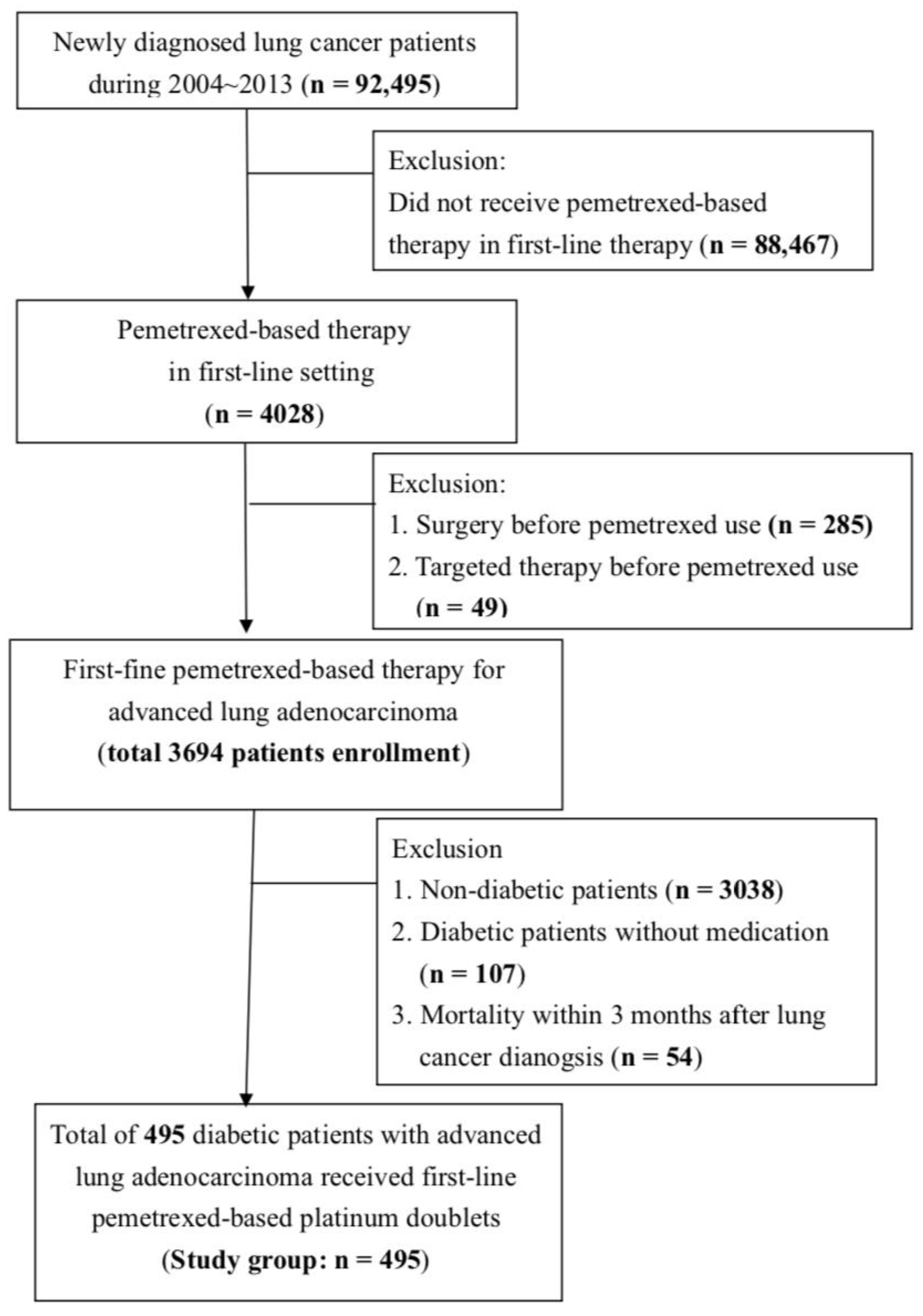
3.1. Flow Chart of Patient Enrollment
3.2. Demographic and Baseline Characteristics of Our Study Group
3.3. Overall Survival Status According to Diabetes Medication
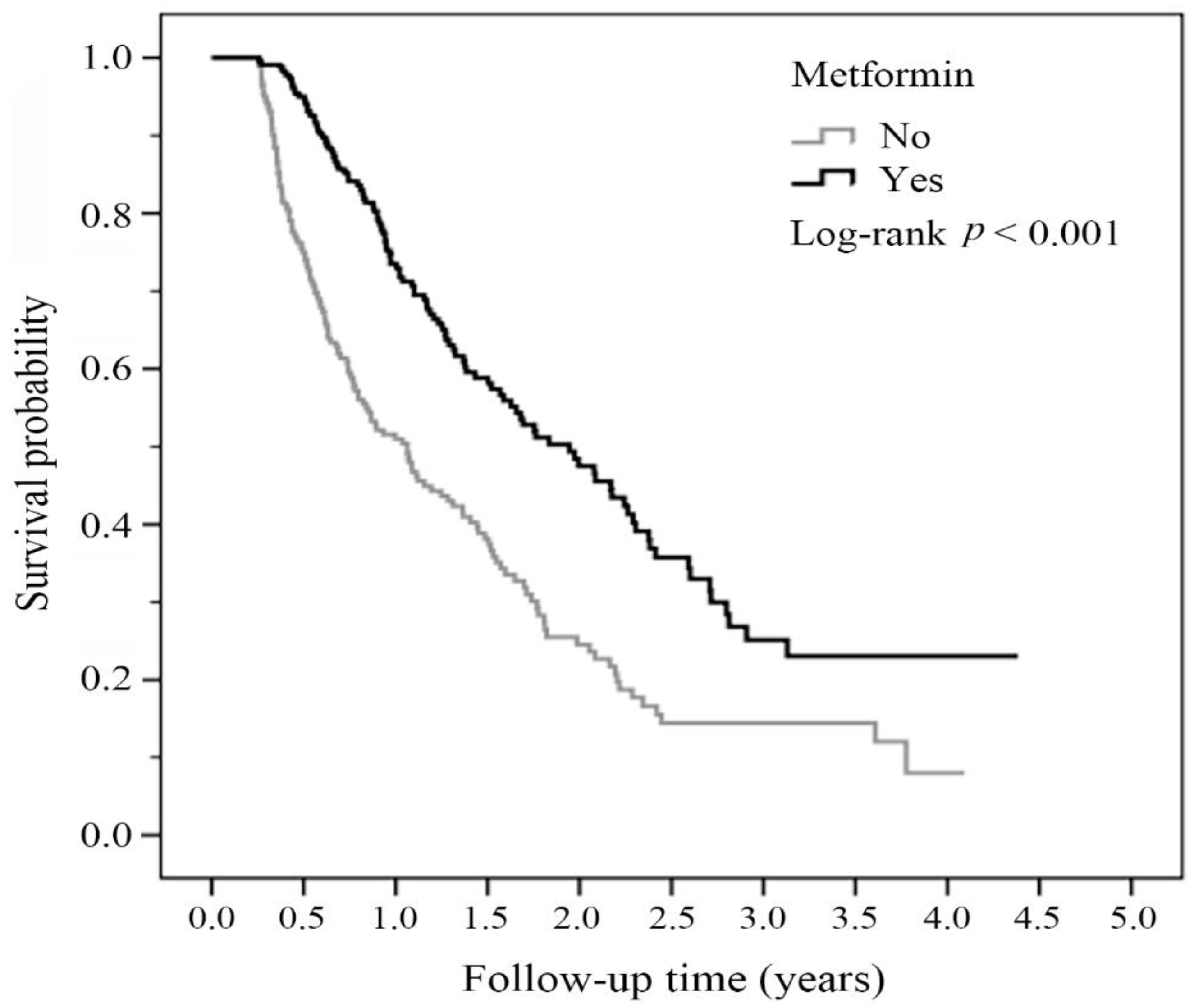
3.4. Overall Survival Status of the Metformin User Group and the Non-Metformin User Group
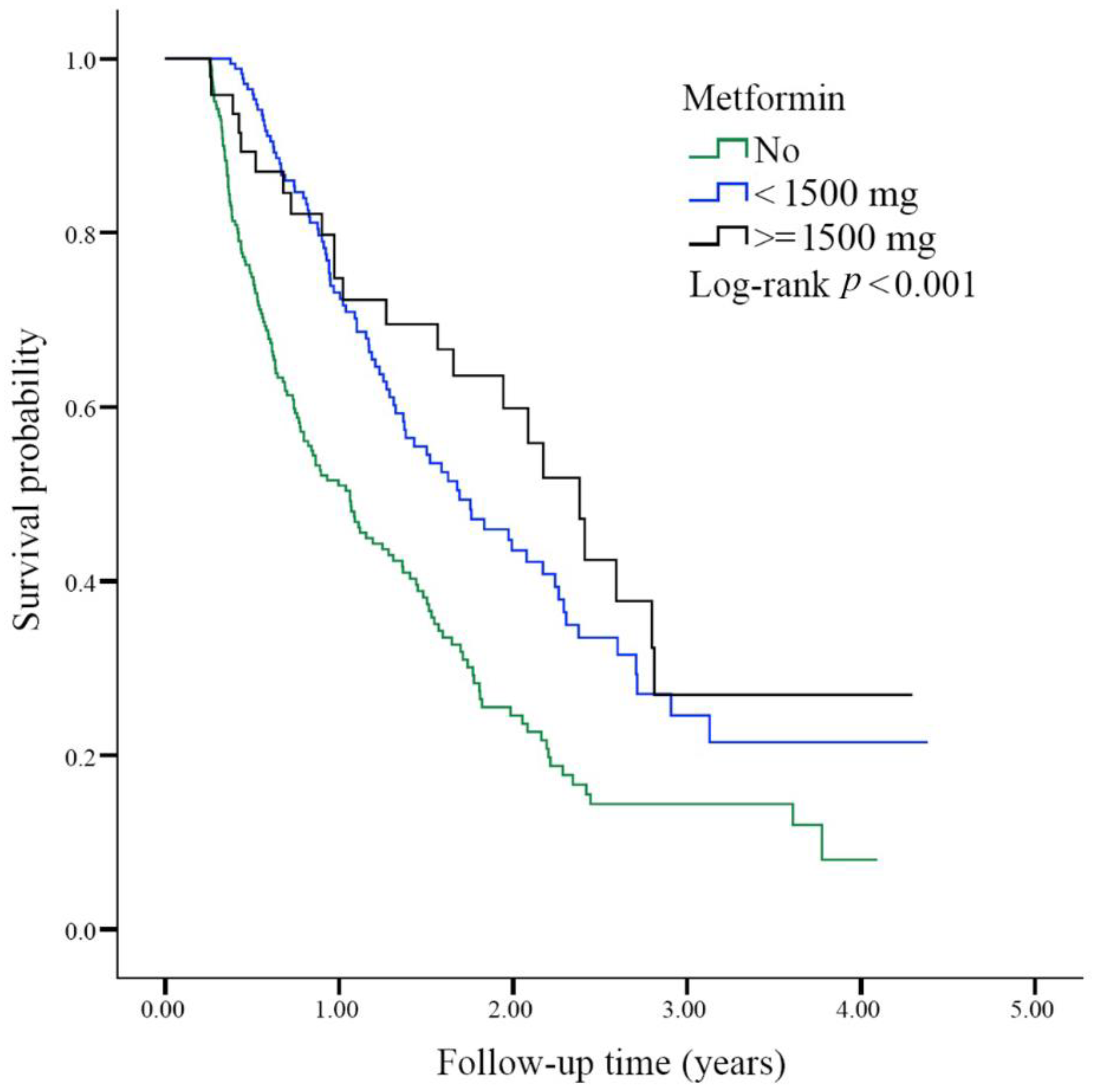
3.5. Overall Survival Status Based on the Daily Dose of Metformin
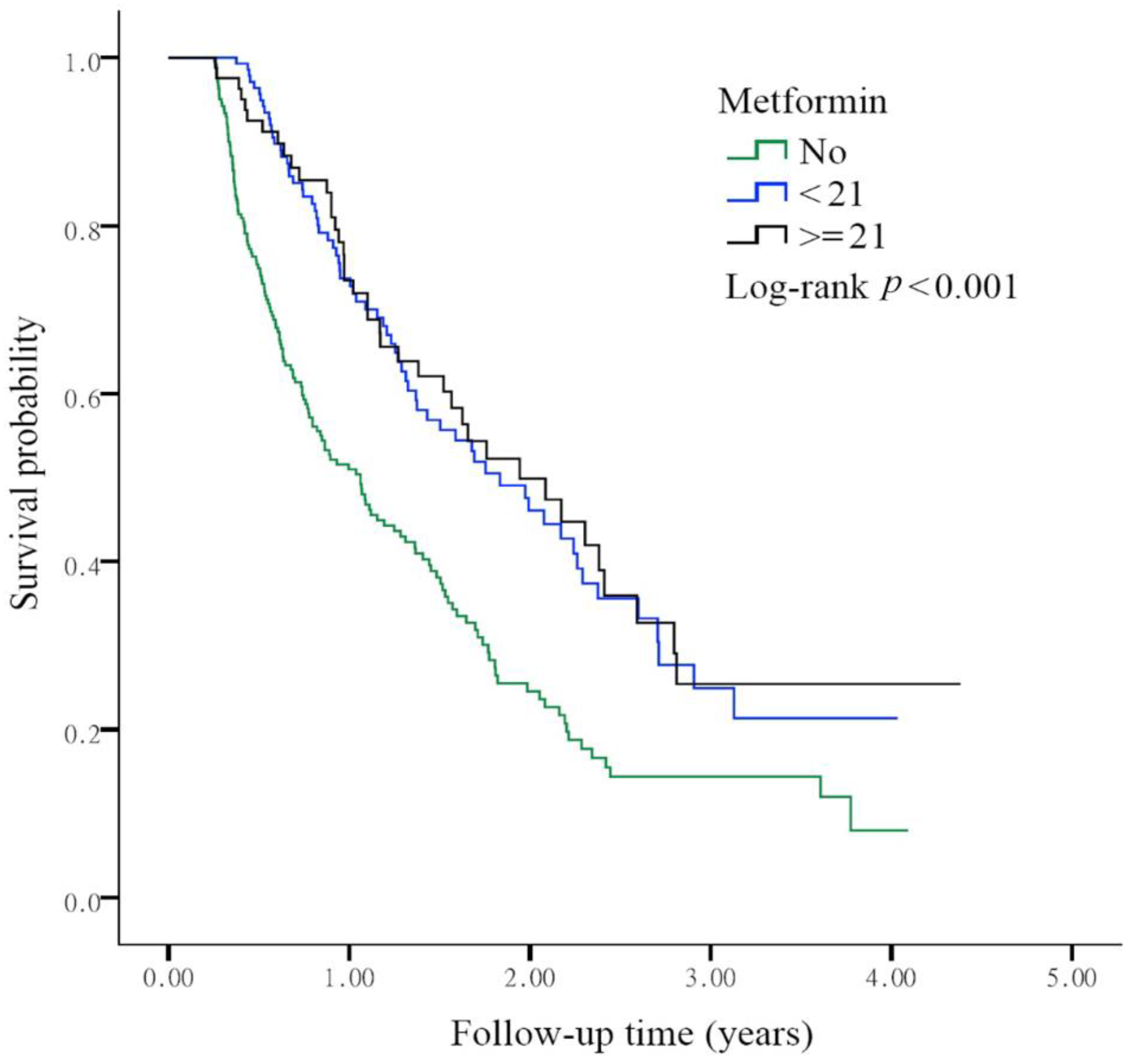
3.6. Overall Survival Status Based on the Cumulative Defined Daily Dose of Metformin
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Levy, A.; Doyen, J. Metformin for non-small cell lung cancer patients: Opportunities and pitfalls. Crit. Rev. Oncol. Hematol. 2018, 125, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Su, V.Y.; Yang, K.Y.; Huang, T.Y.; Hsu, C.C.; Chen, Y.M.; Yen, J.C.; Chou, Y.C.; Chang, Y.L.; He, C.H. The efficacy of first-line yrosine kinase inhibitors combined with co-medications in Asian patients with EGFR mutation non-small cell lung cancer. Sci. Rep. 2020, 10, 14965. [Google Scholar] [CrossRef]
- Mok, T.S.; Wu, Y.L.; Ahn, M.J.; Garassino, M.C.; Kim, H.R.; Ramalingam, S.S.; Shepherd, F.A.; He, Y.; Akamatsu, H.; Theelen, W.S.; et al. Osimertinib or platinum-pemetrexed in EGFR T790M-positive lung cancer. N. Engl. J. Med. 2017, 376, 629–640. [Google Scholar] [CrossRef] [Green Version]
- Soria, J.C.; Tan, D.S.W.; Chiari, R.; Wu, Y.L.; Paz-Ares, L.; Wolf, J.; Geater, S.L.; Orlov, S.; Cortinovis, D.; Yu, C.J.; et al. First-line ceritinib versus platinum-based chemotherapy in advanced ALK-rearranged non-small-cell lung cancer (ASCEND-4): A randomised, open-label, phase 3 study. Lancet 2017, 389, 917–929. [Google Scholar] [CrossRef]
- Hsu, K.H.; Ho, C.C.; Hsia, T.C.; Tseng, J.S.; Su, K.Y.; Wu, M.F.; Chiu, K.L.; Yang, T.Y.; Chen, K.C.; Ooi, H.; et al. Identification of five driver gene mutations in patients with treatment-naive lung adenocarcinoma in Taiwan. PLoS One 2015, 10, e0120852. [Google Scholar] [CrossRef] [Green Version]
- Berghmans, T.; Dingemans, A.M.; Hendriks, L.E.L.; Cadranel, J. Immunotherapy for nonsmall cell lung cancer: A new therapeutic algorithm. Eur. Respir. J. 2020, 55, 1901907. [Google Scholar] [CrossRef] [PubMed]
- Gadgeel, S.; Rodriguez-Abreu, D.; Speranza, G.; Esteban, E.; Felip, E.; Domine, M.; Hui, R.; Hochmair, M.J.; Clingan, P.; Powell, S.F.; et al. Updated analysis from KEYNOTE-189: Pembrolizumab or placebo plus pemetrexed and platinum for previously untreated metastatic nonsquamous non-small-cell lung cancer. J. Clin. Oncol. 2020, 38, 1505–1517. [Google Scholar] [CrossRef] [PubMed]
- Satouchi, M.; Nosaki, K.; Takahashi, T.; Nakagawa, K.; Aoe, K.; Kurata, T.; Sekine, A.; Horiike, A.; Fukuhara, T.; Sugawara, S.; et al. First-line pembrolizumab vs chemotherapy in metastatic non-small-cell lung cancer: KEYNOTE-024 Japan subset. Cancer Sci. 2020, 111, 4480–4489. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Lu, S. The effect of PD-L1 categories-directed pembrolizumab plus chemotherapy for newly diagnosed metastatic non-small-cell lung cancer: A cost-effectiveness analysis. Transl. Lung Cancer Res. 2020, 9, 1770–1784. [Google Scholar] [CrossRef]
- Belani, C.P.; Brodowicz, T.; Ciuleanu, T.E.; Krzakowski, M.; Yang, S.H.; Franke, F.; Cucevic, B.; Madhavan, J.; Santoro, A.; Ramlau, R.; et al. Quality of life in patients with advanced non-small-cell lung cancer given maintenance treatment with pemetrexed versus placebo (H3E-MC-JMEN): Results from a randomised, double-blind, phase 3 study. Lancet Oncol. 2012, 13, 292–299. [Google Scholar] [CrossRef]
- Belani, C.P.; Wu, Y.L.; Chen, Y.M.; Kim, J.H.; Yang, S.H.; Zhang, L.; Peterson, P.; Orlando, M. Efficacy and safety of pemetrexed maintenance therapy versus best supportive care in patients from East Asia with advanced, nonsquamous non-small cell lung cancer: An exploratory subgroup analysis of a global, randomized, phase 3 clinical trial. J. Thorac. Oncol. 2012, 7, 567–573. [Google Scholar] [CrossRef] [Green Version]
- Scagliotti, G.V.; Parikh, P.; von Pawel, J.; Biesma, B.; Vansteenkiste, J.; Manegold, C.; Serwatowski, P.; Gatzemeier, U.; Digumarti, R.; Zukin, M.; et al. Phase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naive patients with advanced-stage non-small-cell lung cancer. J. Clin. Oncol. 2008, 26, 3543–3551. [Google Scholar] [CrossRef]
- Saxena, A.; Becker, D.; Preeshagul, I.; Lee, K.; Katz, E.; Levy, B. Therapeutic effects of repurposed therapies in non-small cell lung cancer: What is old is new again. Oncologist 2015, 20, 934–945. [Google Scholar] [CrossRef] [Green Version]
- Evans, J.M.; Donnelly, L.A.; Emslie-Smith, A.M.; Alessi, D.R.; Morris, A.D. Metformin and reduced risk of cancer in diabetic patients. BMJ 2005, 330, 1304–1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Algire, C.; Zakikhani, M.; Blouin, M.J.; Shuai, J.H.; Pollak, M. Metformin attenuates the stimulatory effect of a high-energy diet on in vivo LLC1 carcinoma growth. Endocr. Relat. Cancer 2008, 15, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Currie, C.J.; Poole, C.D.; Jenkins-Jones, S.; Gale, E.A.; Johnson, J.A.; Morgan, C.L. Mortality after incident cancer in people with and without type 2 diabetes: Impact of metformin on survival. Diabetes Care 2012, 35, 299–304. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.M.; Wang, J.L.; Tsai, Y.T.; Jiang, J.H.; Chen, H.L. Repurposing metformin for lung cancer management. In A Global Scientific Vision—Prevention, Diagnosis, and Treatment of Lung Cancer; InTech Publishers, Inc.: London, UK, 2017; Chapter 9; pp. 149–163. [Google Scholar]
- Guariguata, L.; Whiting, D.R.; Hambleton, I.; Beagley, J.; Linnenkamp, U.; Shaw, J.E. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res. Clin. Pract. 2014, 103, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Tian, R.H.; Zhang, Y.G.; Wu, Z.; Liu, X.; Yang, J.W.; Ji, H.L. Effects of metformin on survival outcomes of lung cancer patients with type 2 diabetes mellitus: A meta-analysis. Clin. Transl. Oncol. 2016, 18, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H. Metformin and lung cancer risk in patients with type 2 diabetes mellitus. Oncotarget 2017, 8, 41132–41142. [Google Scholar] [CrossRef]
- Vicentini, M.; Ballotari, P.; Giorgi Rossi, P.; Venturelli, F.; Sacchettini, C.; Greci, M.; Mangone, L.; Pezzarossi, A.; Manicardi, V. Effect of different glucose-lowering therapies on cancer incidence in type 2 diabetes: An observational population-based study. Diabetes Res. Clin. Pract. 2018, 143, 398–408. [Google Scholar] [CrossRef]
- Wan, G.; Yu, X.; Chen, P.; Wang, X.; Pan, D.; Wang, X.; Li, L.; Cai, X.; Cao, F. Metformin therapy associated with survival benefit in lung cancer patients with diabetes. Oncotarget 2016, 7, 35437–35445. [Google Scholar] [CrossRef] [Green Version]
- Zhu, N.; Zhang, Y.; Gong, Y.I.; He, J.; Chen, X. Metformin and lung cancer risk of patients with type 2 diabetes mellitus: A meta-analysis. Biomed. Rep. 2015, 3, 235–241. [Google Scholar] [CrossRef] [Green Version]
- Arrieta, O.; Varela-Santoyo, E.; Soto-Perez-de-Celis, E.; Sanchez-Reyes, R.; De la Torre-Vallejo, M.; Muniz-Hernandez, S.; Cardona, A.F. Metformin use and its effect on survival in diabetic patients with advanced non-small cell lung cancer. BMC Cancer 2016, 16, 633. [Google Scholar] [CrossRef] [Green Version]
- Brancher, S.; Stoer, N.C.; Weiderpass, E.; Damhuis, R.A.M.; Johannesen, T.B.; Botteri, E.; Strand, T.E. Metformin use and lung cancer survival: A population-based study in Norway. Br. J. Cancer. 2020, 124, 1018–1025. [Google Scholar] [CrossRef]
- Chuang, M.C.; Yang, Y.H.; Tsai, Y.H.; Hsieh, M.J.; Lin, Y.C.; Lin, C.K.; Chen, P.C.; Yang, T.M. Survival benefit associated with metformin use in inoperable non-small cell lung cancer patients with diabetes: A population-based retrospective cohort study. PLoS One 2018, 13, e0191129. [Google Scholar] [CrossRef] [Green Version]
- Kang, J.; Jeong, S.M.; Shin, D.W.; Cho, M.; Cho, J.H.; Kim, J. The associations of aspirin, statins, and metformin with lung cancer risk and related mortality: A time-dependent analysis of population-based nationally representative data. J. Thorac. Oncol. 2021, 16, 76–88. [Google Scholar] [CrossRef]
- Lin, J.J.; Gallagher, E.J.; Sigel, K.; Mhango, G.; Galsky, M.D.; Smith, C.B.; LeRoith, D.; Wisnivesky, J.P. Survival of patients with stage IV lung cancer with diabetes treated with metformin. Am. J. Respir. Crit. Care Med. 2015, 191, 448–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henderson, D.; Frieson, D.; Zuber, J.; Solomon, S.S. Metformin has positive therapeutic effects in colon cancer and lung cancer. Am. J. Med. Sci. 2017, 354, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Arrieta, O.; Ramirez-Tirado, L.A.; Zatarain-Barron, Z.L. Metformin plus tyrosine kinase inhibitors in epidermal growth factor receptor-mutated non-small cell lung cancer-reply. JAMA Oncol. 2020, 6, 782–783. [Google Scholar] [CrossRef] [PubMed]
- Marrone, K.A.; Zhou, X.; Forde, P.M.; Purtell, M.; Brahmer, J.R.; Hann, C.L.; Kelly, R.J.; Coleman, B.; Gabrielson, E.; Rosner, G.L.; et al. A randomized phase II study of metformin plus paclitaxel/carboplatin/bevacizumab in patients with chemotherapy-naive advanced or metastatic nonsquamous non-small cell lung cancer. Oncologist 2018, 23, 859–865. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Joo, J.; Lee, Y.J.; Lee, E.K.; Park, S.; Kim, T.S.; Lee, S.H.; Kim, S.Y.; Wie, G.A.; Park, M.; et al. Randomized phase II study of platinum-based chemotherapy plus controlled diet with or without metformin in patients with advanced non-small cell lung cancer. Lung Cancer 2021, 151, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Parikh, A.B.; Marrone, K.A.; Becker, D.J.; Brahmer, J.R.; Ettinger, D.S.; Levy, B.P. A pooled analysis of two phase II trials evaluating metformin plus platinum-based chemotherapy in advanced non-small cell lung cancer. Cancer Treat. Res. Commun. 2019, 20, 100150. [Google Scholar] [CrossRef] [PubMed]
- Parikh, A.B.; Kozuch, P.; Rohs, N.; Becker, D.J.; Levy, B.P. Metformin as a repurposed therapy in advanced non-small cell lung cancer (NSCLC): Results of a phase II trial. Invest. New Drugs 2017, 35, 813–819. [Google Scholar] [CrossRef]
- Vernieri, C.; Signorelli, D.; Galli, G.; Ganzinelli, M.; Moro, M.; Fabbri, A.; Tamborini, E.; Marabese, M.; Caiola, E.; Broggini, M.; et al. Exploiting FAsting-mimicking diet and MEtformin to improve the efficacy of platinum-pemetrexed chemotherapy in advanced LKB1-inactivated lung adenocarcinoma: The FAME trial. Clin. Lung Cancer 2019, 20, e413–e417. [Google Scholar] [CrossRef] [PubMed]
- WHO Collaborating Centre for Drug Statistics Methodology. Guidelines for ATC Classification and DDD Assignment 2021; Norwegian Institute of Public Health: Oslo, Norway, 2021; pp. 23–31. [Google Scholar]
- Sinnett-Smith, J.; Kisfalvi, K.; Kui, R.; Rozengurt, E. Metformin inhibition of mTORC1 activation, DNA synthesis and proliferation in pancreatic cancer cells: Dependence on glucose concentration and role of AMPK. Biochem. Biophys. Res. Commun. 2013, 430, 352–357. [Google Scholar] [CrossRef] [Green Version]
- Zakikhani, M.; Dowling, R.; Fantus, I.G.; Sonenberg, N.; Pollak, M. Metformin is an AMP kinase-dependent growth inhibitor for breast cancer cells. Cancer Res. 2006, 66, 10269–10273. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.H.; Guo, X.L. Combinational strategies of metformin and chemotherapy in cancers. Cancer Chemother. Pharmacol. 2016, 78, 13–26. [Google Scholar] [CrossRef]
- Luo, Z.; Chen, W.; Wu, W.; Luo, W.; Zhu, T.; Guo, G.; Zhang, L.; Wang, C.; Li, M.; Shi, S. Metformin promotes survivin degradation through AMPK/PKA/GSK-3beta-axis in non-small cell lung cancer. J. Cell Biochem. 2019, 120, 11890–11899, Epub 2019/02/23. [Google Scholar] [CrossRef]
- Zhang, Y.; Feng, X.; Li, T.; Yi, E.; Li, Y. Metformin synergistic pemetrexed suppresses non-small-cell lung cancer cell proliferation and invasion in vitro. Cancer Med. 2017, 6, 1965–1975. [Google Scholar] [CrossRef]
- Fatehi Hassanabad, A.; MacQueen, K.T. Molecular mechanisms underlining the role of metformin as a therapeutic agent in lung cancer. Cell Oncol. (Dordr.) 2020, 44, 1–18. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total | Non-Metformin User (n = 270) | Metformin User (n = 225) | p Value | |||
|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | (%) | ||
| Age, mean ± SD | 67.4 ± 9.5 | 68.3 ± 9.6 | 66.4 ± 9.2 | 0.026 | |||
| <60 | 105 | (21.2) | 53 | (19.6) | 52 | (23.1) | 0.079 |
| 60–70 | 187 | (37.8) | 94 | (34.8) | 93 | (41.3) | |
| ≥70 | 203 | (41.0) | 123 | (45.6) | 80 | (35.6) | |
| Gender | 0.112 | ||||||
| Female | 214 | (43.2) | 108 | (40.0) | 106 | (47.1) | |
| Male | 281 | (56.8) | 162 | (60.0) | 119 | (52.9) | |
| Diabetes medication | |||||||
| Insulin | 39 | (7.9) | 26 | (9.6) | 13 | (5.8) | 0.113 |
| Acarbose/SU #/TZD * | 221 | (44.7) | 59 | (21.9) | 162 | (72.0) | <0.001 |
| Platinum reagents | |||||||
| Cisplatin | 373 | (75.4) | 199 | (73.7) | 174 | (77.3) | 0.351 |
| Carboplatin | 114 | (23.0) | 63 | (23.3) | 51 | (22.7) | 0.861 |
| Statin | 82 | (16.6) | 38 | (14.1) | 44 | (19.6) | 0.102 |
| Comorbidity | |||||||
| CVA 1 | 95 | (19.2) | 57 | (21.1) | 38 | (16.9) | 0.235 |
| CAD 2 | 186 | (37.6) | 107 | (39.6) | 79 | (35.1) | 0.301 |
| Congestive heart failure | 40 | (8.1) | 25 | (9.3) | 15 | (6.7) | 0.292 |
| COPD 3 | 222 | (44.9) | 126 | (46.7) | 96 | (42.7) | 0.373 |
| CRD 4 | 22 | (4.4) | 12 | (4.4) | 10 | (4.4) | 1.000 |
| Variables | Study Subjects | Model 1 | Model 2 | |||||
|---|---|---|---|---|---|---|---|---|
| n | (%) | aHR | (95%CI) | p Value | aHR | (95%CI) | p Value | |
| Metformin | ||||||||
| No | 270 | (54.6) | 1.00 | (reference) | 1.00 | (reference) | ||
| Yes | 225 | (45.5) | 0.50 | (0.39–0.64) | <0.001 | 0.61 | (0.46–0.79) | <0.001 |
| Insulin | ||||||||
| No | 456 | (92.1) | 1.00 | (reference) | 1.00 | (reference) | ||
| Yes | 39 | (7.9) | 0.93 | (0.59–1.47) | 0.760 | 0.75 | (0.47–1.19) | 0.214 |
| Others * | ||||||||
| No | 274 | (55.4) | 1.00 | (reference) | 1.00 | (reference) | ||
| Yes | 221 | (44.7) | 0.46 | (0.36–0.60) | <0.001 | 0.55 | (0.42–0.71) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.-L.; Tsai, Y.-T.; Lin, C.-H.; Cidem, A.; Staniczek, T.; Chang, G.R.-L.; Yen, C.-C.; Chen, W.; Chong, K.-Y.; Chen, C.-M. Benefits of Metformin Combined with Pemetrexed-Based Platinum Doublets as a First-Line Therapy for Advanced Lung Adenocarcinoma Patients with Diabetes. Biomolecules 2021, 11, 1252. https://doi.org/10.3390/biom11081252
Wang J-L, Tsai Y-T, Lin C-H, Cidem A, Staniczek T, Chang GR-L, Yen C-C, Chen W, Chong K-Y, Chen C-M. Benefits of Metformin Combined with Pemetrexed-Based Platinum Doublets as a First-Line Therapy for Advanced Lung Adenocarcinoma Patients with Diabetes. Biomolecules. 2021; 11(8):1252. https://doi.org/10.3390/biom11081252
Chicago/Turabian StyleWang, Jiun-Long, Yi-Ting Tsai, Ching-Heng Lin, Abdulkadir Cidem, Theresa Staniczek, Gary Ro-Lin Chang, Chih-Ching Yen, Wei Chen, Kowit-Yu Chong, and Chuan-Mu Chen. 2021. "Benefits of Metformin Combined with Pemetrexed-Based Platinum Doublets as a First-Line Therapy for Advanced Lung Adenocarcinoma Patients with Diabetes" Biomolecules 11, no. 8: 1252. https://doi.org/10.3390/biom11081252