
Sphingolipids in Childhood Asthma and Obesity (SOAP Study): A Protocol of a Cross-Sectional Study
 , , , , add
Show full author list
, , , , add
Show full author list
Abstract
:1. Background
Study Hypothesis and Aims
2. Methods
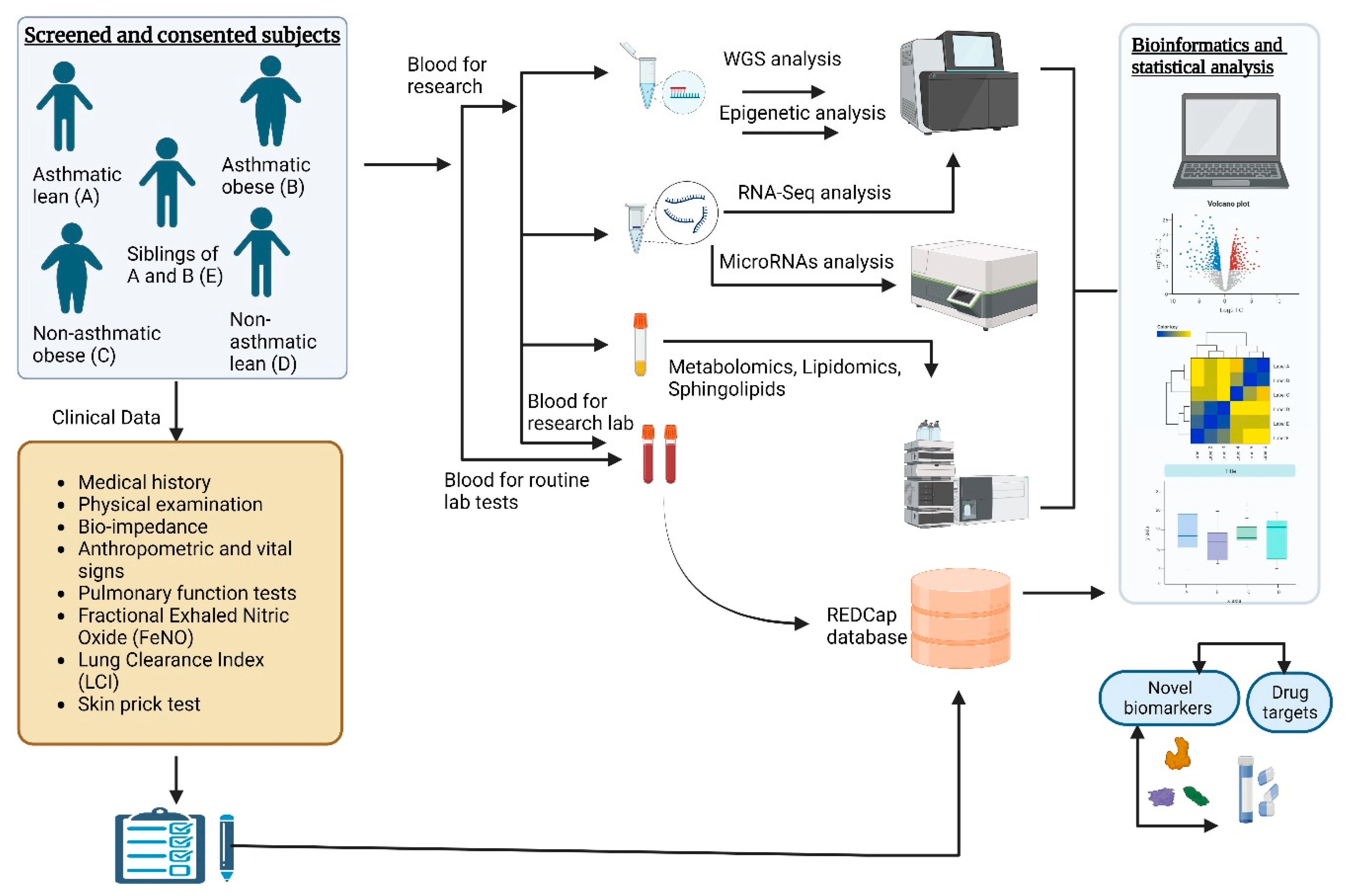
2.1. Study Design and Population
2.2. Testing Procedures and Measurements
2.2.1. Questionnaires (Self-Reported)
2.2.2. Medical History and Physical Examination
2.2.3. Anthropometry
2.2.4. Vital Signs
2.2.5. Bioimpedance
2.2.6. Glucose, Insulin, Lipids, and Other Blood Tests
2.2.7. Pulmonary Function and Plethysmography Tests
2.2.8. Bronchodilator Response
2.2.9. Fractional Exhaled Nitric Oxide (FeNO)
2.2.10. Lung Clearance Index (LCI)
2.2.11. Allergy Test
2.2.12. Allergy Skin Prick Test
2.2.13. Cytokine and Adipokine Measurements
2.2.14. Sphingolipids and SPT Activity
2.2.15. Metabolomics and Lipidomics
2.2.16. DNA Extraction
2.2.17. Whole-Genome Library Construction and Sequencing
2.2.18. Illumina EPIC Methylation
2.2.19. RNA Extraction
2.2.20. Total RNA Library Construction and Sequencing
2.2.21. miRNA Profiling
2.3. Sample Size Calculation and Statistical Analysis
2.4. Data Integration
3. Expected Results and Outcomes
4. Strengths and Limitations
- ➢
- The study will provide comprehensive genetic, epigenetic, metabolomic, and lipidomic data that affect sphingolipid metabolism to characterize endotypes of children with asthma and obesity, which will be critical to understand the underlying pathophysiology and to develop optimal treatment strategies.
- ➢
- The study will use harmonized procedures for measuring anthropometry, lung function, biochemical risk factors, sphingolipid synthesis, and multi-omics data.
- ➢
- The study will include a nested family group of healthy siblings of asthmatic children to assess environmental and genetic factors associated with asthma and obesity.
- ➢
- For the assessment of sphingolipids, we will rely on measurements of blood, since it cannot be measured noninvasively in the airways of children with asthma. Whole-blood sphingolipids have been shown to be correlated with asthma in children.
- ➢
- Body mass index (BMI) will be used to categorize overweight and obese children, as it can be easily assessed at the time of recruitment, with the caveat that BMI does not distinguish either subcutaneous fat from visceral adiposity or fat mass from lean mass.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pavord, I.D.; Beasley, R.; Agusti, A.; Anderson, G.P.; Bel, E.; Brusselle, G.; Cullinan, P.; Custovic, A.; Ducharme, F.M.; Fahy, J.V.; et al. After Asthma: Redefining Airways Diseases. Lancet 2018, 391, 350–400. [Google Scholar] [CrossRef] [PubMed]
- Asher, I.; Pearce, N. Global Burden of Asthma among Children. Int. J. Tuberc. Lung. Dis. 2014, 18, 1269–1278. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, G.; La Grutta, S. The Burden of Pediatric Asthma. Front. Pediatr. 2018, 6, 186. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Dong, G.H.; Lin, K.C.; Lee, Y.L. Gender Difference of Childhood Overweight and Obesity in Predicting the Risk of Incident Asthma: A Systematic Review and Meta-Analysis. Obes. Rev. 2013, 14, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Deng, X.; Ma, J.; Yuan, Y.; Zhang, Z.; Niu, W. Association between Overweight or Obesity and the Risk for Childhood Asthma and Wheeze: An Updated Meta-Analysis on 18 Articles and 73,252 Children. Pediatr. Obes. 2019, 14, e12532. [Google Scholar] [CrossRef] [PubMed]
- Janahi, I.A.; Bener, A.; Bush, A. Prevalence of Asthma among Qatari Schoolchildren: International Study of Asthma and Allergies in Childhood, Qatar. Pediatr. Pulmonol. 2006, 41, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Hammoudeh, S.; Hani, Y.; Alfaki, M.; Omar, N.; El Dimassi, D.; Nowir, K.; Gadelhaq, W.; AlNaimi, A.; Elizabeth, C.; Khashfeh, S.; et al. The Prevalence of Asthma, Allergic Rhinitis, and Eczema among School-Aged Children in Qatar: A Global Asthma Network Study. Pediatr. Pulmonol. 2022, 57, 1440–1446. [Google Scholar] [CrossRef]
- Al-Thani, M.; Al-Thani, A.; Alyafei, S.; Al-Chetachi, W.; Khalifa, S.E.; Ahmed, A.; Ahmad, A.; Vinodson, B.; Akram, H. The Prevalence and Characteristics of Overweight and Obesity among Students in Qatar. Public Health 2018, 160, 143–149. [Google Scholar] [CrossRef]
- Shailesh, H.; Bhat, A.A.; Janahi, I.A. Obesity-Associated Non-T2 Mechanisms in Obese Asthmatic Individuals. Biomedicines 2023, 11, 2797. [Google Scholar] [CrossRef]
- Shailesh, H.; Janahi, I.A. Role of Obesity in Inflammation and Remodeling of Asthmatic Airway. Life 2022, 12, 948. [Google Scholar] [CrossRef]
- Lee, M.; Lee, S.Y.; Bae, Y.-S. Functional Roles of Sphingolipids in Immunity and Their Implication in Disease. Exp. Mol. Med. 2023, 55, 1110–1130. [Google Scholar] [CrossRef] [PubMed]
- Moffatt, M.F.; Kabesch, M.; Liang, L.; Dixon, A.L.; Strachan, D.; Heath, S.; Depner, M.; von Berg, A.; Bufe, A.; Rietschel, E.; et al. Genetic Variants Regulating ORMDL3 Expression Contribute to the Risk of Childhood Asthma. Nature 2007, 448, 470–473. [Google Scholar] [CrossRef] [PubMed]
- Stein, M.M.; Thompson, E.E.; Schoettler, N.; Helling, B.A.; Magnaye, K.M.; Stanhope, C.; Igartua, C.; Morin, A.; Washington, C.; Nicolae, D.; et al. A Decade of Research on the 17q12-21 Asthma Locus: Piecing Together the Puzzle. J. Allergy Clin. Immunol. 2018, 142, 749–764.e3. [Google Scholar] [CrossRef] [PubMed]
- Halapi, E.; Gudbjartsson, D.F.; Jonsdottir, G.M.; Bjornsdottir, U.S.; Thorleifsson, G.; Helgadottir, H.; Williams, C.; Koppelman, G.H.; Heinzmann, A.; Boezen, H.M.; et al. A Sequence Variant on 17q21 Is Associated with Age at Onset and Severity of Asthma. Eur. J. Hum. Genet. 2010, 18, 902–908. [Google Scholar] [CrossRef] [PubMed]
- Almqvist, C.; Worm, M.; Leynaert, B.; Working Group of GA2LEN WP 2.5 Gender. Impact of Gender on Asthma in Childhood and Adolescence: A GA2LEN Review. Allergy 2008, 63, 47–57. [Google Scholar] [CrossRef] [PubMed]
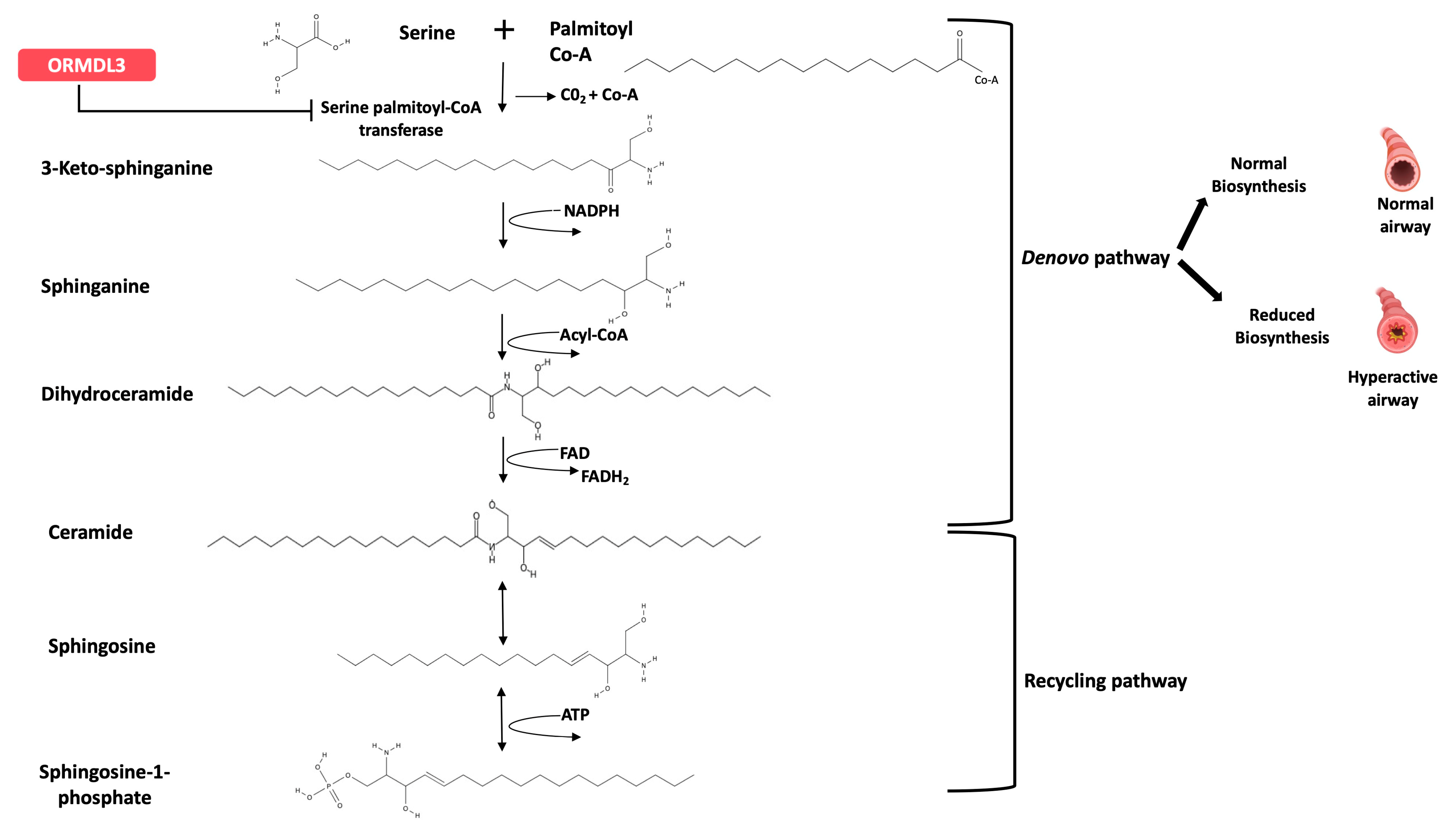
- Worgall, T.S.; Veerappan, A.; Sung, B.; Kim, B.I.; Weiner, E.; Bholah, R.; Silver, R.B.; Jiang, X.-C.; Worgall, S. Impaired Sphingolipid Synthesis in the Respiratory Tract Induces Airway Hyperreactivity. Sci. Transl. Med. 2013, 5, 186ra67. [Google Scholar] [CrossRef] [PubMed]
- Sajuthi, S.P.; Everman, J.L.; Jackson, N.D.; Saef, B.; Rios, C.L.; Moore, C.M.; Mak, A.C.Y.; Eng, C.; Fairbanks-Mahnke, A.; Salazar, S.; et al. Nasal Airway Transcriptome-Wide Association Study of Asthma Reveals Genetically Driven Mucus Pathobiology. Nat. Commun. 2022, 13, 1632. [Google Scholar] [CrossRef] [PubMed]
- Breslow, D.K.; Weissman, J.S. Membranes in Balance: Mechanisms of Sphingolipid Homeostasis. Mol. Cell 2010, 40, 267–279. [Google Scholar] [CrossRef]
- Han, S.; Lone, M.A.; Schneiter, R.; Chang, A. Orm1 and Orm2 Are Conserved Endoplasmic Reticulum Membrane Proteins Regulating Lipid Homeostasis and Protein Quality Control. Proc. Natl. Acad. Sci. USA 2010, 107, 5851–5856. [Google Scholar] [CrossRef]
- Hornemann, T.; Wei, Y.; von Eckardstein, A. Is the Mammalian Serine Palmitoyltransferase a High-Molecular-Mass Complex? Biochem. J. 2007, 405, 157–164. [Google Scholar] [CrossRef]
- Breslow, D.K.; Collins, S.R.; Bodenmiller, B.; Aebersold, R.; Simons, K.; Shevchenko, A.; Ejsing, C.S.; Weissman, J.S. Orm Family Proteins Mediate Sphingolipid Homeostasis. Nature 2010, 463, 1048–1053. [Google Scholar] [CrossRef] [PubMed]
- Hornemann, T.; Worgall, T.S. Sphingolipids and Atherosclerosis. Atherosclerosis 2013, 226, 16–28. [Google Scholar] [CrossRef] [PubMed]
- Oyeniran, C.; Sturgill, J.L.; Hait, N.C.; Huang, W.-C.; Avni, D.; Maceyka, M.; Newton, J.; Allegood, J.C.; Montpetit, A.; Conrad, D.H.; et al. Aberrant ORM (Yeast)-like Protein Isoform 3 (ORMDL3) Expression Dysregulates Ceramide Homeostasis in Cells and Ceramide Exacerbates Allergic Asthma in Mice. J. Allergy Clin. Immunol. 2015, 136, 1035–1046.e6. [Google Scholar] [CrossRef] [PubMed]
- Siow, D.; Sunkara, M.; Dunn, T.M.; Morris, A.J.; Wattenberg, B. ORMDL/Serine Palmitoyltransferase Stoichiometry Determines Effects of ORMDL3 Expression on Sphingolipid Biosynthesis. J. Lipid Res. 2015, 56, 898–908. [Google Scholar] [CrossRef] [PubMed]
- Siow, D.L.; Wattenberg, B.W. Mammalian ORMDL Proteins Mediate the Feedback Response in Ceramide Biosynthesis. J. Biol. Chem. 2012, 287, 40198–40204. [Google Scholar] [CrossRef] [PubMed]
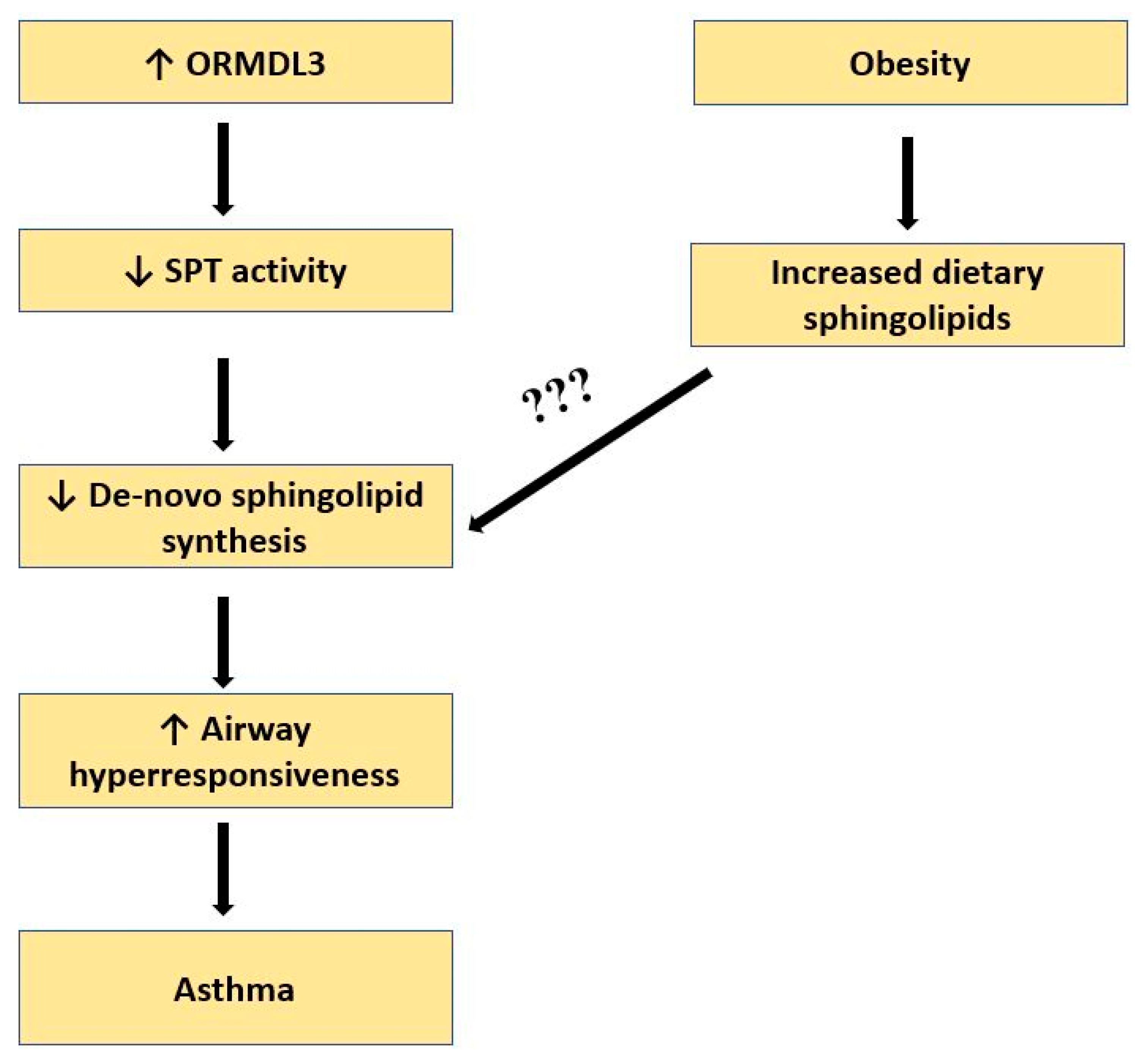
- Ono, J.G.; Kim, B.I.; Zhao, Y.; Christos, P.J.; Tesfaigzi, Y.; Worgall, T.S.; Worgall, S. Decreased Sphingolipid Synthesis in Children with 17q21 Asthma–Risk Genotypes. J. Clin. Investig. 2020, 130, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Wills-Karp, M. At Last—Linking ORMDL3 Polymorphisms, Decreased Sphingolipid Synthesis, and Asthma Susceptibility. J. Clin. Investig. 2020, 130, 604–607. [Google Scholar] [CrossRef] [PubMed]
- Kreiner-Møller, E.; Strachan, D.P.; Linneberg, A.; Husemoen, L.L.N.; Bisgaard, H.; Bønnelykke, K. 17q21 Gene Variation Is Not Associated with Asthma in Adulthood. Allergy 2015, 70, 107–114. [Google Scholar] [CrossRef]
- Chen, J.; Miller, M.; Unno, H.; Rosenthal, P.; Sanderson, M.J.; Broide, D.H. Orosomucoid-like 3 (ORMDL3) Upregulates Airway Smooth Muscle Proliferation, Contraction, and Ca2+ Oscillations in Asthma. J. Allergy Clin. Immunol. 2018, 142, 207–218.e6. [Google Scholar] [CrossRef]
- Haus, J.M.; Kashyap, S.R.; Kasumov, T.; Zhang, R.; Kelly, K.R.; Defronzo, R.A.; Kirwan, J.P. Plasma Ceramides Are Elevated in Obese Subjects with Type 2 Diabetes and Correlate with the Severity of Insulin Resistance. Diabetes 2009, 58, 337–343. [Google Scholar] [CrossRef]
- Hammerschmidt, P.; Brüning, J.C. Contribution of Specific Ceramides to Obesity-Associated Metabolic Diseases. Cell. Mol. Life Sci. 2022, 79, 395. [Google Scholar] [CrossRef] [PubMed]
- Torretta, E.; Barbacini, P.; Al-Daghri, N.M.; Gelfi, C. Sphingolipids in Obesity and Correlated Co-Morbidities: The Contribution of Gender, Age and Environment. Int. J. Mol. Sci. 2019, 20, 5901. [Google Scholar] [CrossRef] [PubMed]
- Asher, M.I.; Keil, U.; Anderson, H.R.; Beasley, R.; Crane, J.; Martinez, F.; Mitchell, E.A.; Pearce, N.; Sibbald, B.; Stewart, A.W. International Study of Asthma and Allergies in Childhood (ISAAC): Rationale and Methods. Eur. Respir. J. 1995, 8, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Hammer, L.D.; Kraemer, H.C.; Wilson, D.M.; Ritter, P.L.; Dornbusch, S.M. Standardized Percentile Curves of Body-Mass Index for Children and Adolescents. Am. J. Dis. Child. 1991, 145, 259–263. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and Beta-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Conwell, L.S.; Trost, S.G.; Brown, W.J.; Batch, J.A. Indexes of Insulin Resistance and Secretion in Obese Children and Adolescents: A Validation Study. Diabetes Care 2004, 27, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Keskin, M.; Kurtoglu, S.; Kendirci, M.; Atabek, M.E.; Yazici, C. Homeostasis Model Assessment Is More Reliable Than the Fasting Glucose/Insulin Ratio and Quantitative Insulin Sensitivity Check Index for Assessing Insulin Resistance Among Obese Children and Adolescents. Pediatrics 2005, 115, e500–e503. [Google Scholar] [CrossRef] [PubMed]
- Hannun, Y.A.; Obeid, L.M. Principles of Bioactive Lipid Signalling: Lessons from Sphingolipids. Nat. Rev. Mol. Cell Biol. 2008, 9, 139–150. [Google Scholar] [CrossRef]
- Dennis, E.A.; Deems, R.A.; Harkewicz, R.; Quehenberger, O.; Brown, H.A.; Milne, S.B.; Myers, D.S.; Glass, C.K.; Hardiman, G.; Reichart, D.; et al. A Mouse Macrophage Lipidome. J. Biol. Chem. 2010, 285, 39976–39985. [Google Scholar] [CrossRef]
- Hammad, S.M.; Pierce, J.S.; Soodavar, F.; Smith, K.J.; Al Gadban, M.M.; Rembiesa, B.; Klein, R.L.; Hannun, Y.A.; Bielawski, J.; Bielawska, A. Blood Sphingolipidomics in Healthy Humans: Impact of Sample Collection Methodology. J. Lipid Res. 2010, 51, 3074–3087. [Google Scholar] [CrossRef]
- Park, H.; Haynes, C.A.; Nairn, A.V.; Kulik, M.; Dalton, S.; Moremen, K.; Merrill, A.H. Transcript Profiling and Lipidomic Analysis of Ceramide Subspecies in Mouse Embryonic Stem Cells and Embryoid Bodies. J. Lipid Res. 2010, 51, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Shaner, R.L.; Allegood, J.C.; Park, H.; Wang, E.; Kelly, S.; Haynes, C.A.; Sullards, M.C.; Merrill, A.H. Quantitative Analysis of Sphingolipids for Lipidomics Using Triple Quadrupole and Quadrupole Linear Ion Trap Mass Spectrometers. J. Lipid Res. 2009, 50, 1692–1707. [Google Scholar] [CrossRef] [PubMed]
- Quehenberger, O.; Armando, A.M.; Brown, A.H.; Milne, S.B.; Myers, D.S.; Merrill, A.H.; Bandyopadhyay, S.; Jones, K.N.; Kelly, S.; Shaner, R.L.; et al. Lipidomics Reveals a Remarkable Diversity of Lipids in Human Plasma. J. Lipid Res. 2010, 51, 3299–3305. [Google Scholar] [CrossRef] [PubMed]
- Quehenberger, O.; Dennis, E.A. The Human Plasma Lipidome. N. Engl. J. Med. 2011, 365, 1812–1823. [Google Scholar] [CrossRef] [PubMed]
- Berdyshev, E.V.; Gorshkova, I.A.; Usatyuk, P.; Zhao, Y.; Saatian, B.; Hubbard, W.; Natarajan, V. De Novo Biosynthesis of Dihydrosphingosine-1-Phosphate by Sphingosine Kinase 1 in Mammalian Cells. Cell Signal. 2006, 18, 1779–1792. [Google Scholar] [CrossRef] [PubMed]
- McKenna, A.; Hanna, M.; Banks, E.; Sivachenko, A.; Cibulskis, K.; Kernytsky, A.; Garimella, K.; Altshuler, D.; Gabriel, S.; Daly, M.; et al. The Genome Analysis Toolkit: A MapReduce Framework for Analyzing next-Generation DNA Sequencing Data. Genome Res. 2010, 20, 1297–1303. [Google Scholar] [CrossRef] [PubMed]
- DESeq2. Available online: https://www.bioconductor.org/packages/release/bioc/html/DESeq2.html (accessed on 7 October 2023).
- Gentleman, R.C.; Carey, V.J.; Bates, D.M.; Bolstad, B.; Dettling, M.; Dudoit, S.; Ellis, B.; Gautier, L.; Ge, Y.; Gentry, J.; et al. Bioconductor: Open Software Development for Computational Biology and Bioinformatics. Genome. Biol. 2004, 5, R80. [Google Scholar] [CrossRef]
- Shannon, P.; Markiel, A.; Ozier, O.; Baliga, N.S.; Wang, J.T.; Ramage, D.; Amin, N.; Schwikowski, B.; Ideker, T. Cytoscape: A Software Environment for Integrated Models of Biomolecular Interaction Networks. Genome. Res. 2003, 13, 2498–2504. [Google Scholar] [CrossRef]
- Tian, Y.; Morris, T.J.; Webster, A.P.; Yang, Z.; Beck, S.; Feber, A.; Teschendorff, A.E. ChAMP: Updated Methylation Analysis Pipeline for Illumina BeadChips. Bioinformatics 2017, 33, 3982–3984. [Google Scholar] [CrossRef]
- Aryee, M.J.; Jaffe, A.E.; Corrada-Bravo, H.; Ladd-Acosta, C.; Feinberg, A.P.; Hansen, K.D.; Irizarry, R.A. Minfi: A Flexible and Comprehensive Bioconductor Package for the Analysis of Infinium DNA Methylation Microarrays. Bioinformatics 2014, 30, 1363–1369. [Google Scholar] [CrossRef]
- Love, M.I.; Huber, W.; Anders, S. Moderated Estimation of Fold Change and Dispersion for RNA-Seq Data with DESeq2. Genome Biol. 2014, 15, 550. [Google Scholar] [CrossRef] [PubMed]
- Rago, D.; Pedersen, C.-E.T.; Huang, M.; Kelly, R.S.; Gürdeniz, G.; Brustad, N.; Knihtilä, H.; Lee-Sarwar, K.A.; Morin, A.; Rasmussen, M.A.; et al. Characteristics and Mechanisms of a Sphingolipid-Associated Childhood Asthma Endotype. Am. J. Respir. Crit. Care Med. 2021, 203, 853–863. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, D.; Johnston, A.D.; Nico, J.; Loh, L.N.; Jorge, Y.; Suzuki, M.; Macian, F.; Greally, J.M. Functional Genomics of the Pediatric Obese Asthma Phenotype Reveal Enrichment of Rho-GTPase Pathways. Am. J. Respir. Crit. Care Med. 2020, 202, 259–274. [Google Scholar] [CrossRef] [PubMed]
- Maffeis, L.; Agostoni, C.V.; Marafon, D.P.; Terranova, L.; Giavoli, C.; Milani, G.P.; Lelii, M.; Madini, B.; Marchisio, P.; Patria, M.F. Cytokines Profile and Lung Function in Children with Obesity and Asthma: A Case Control Study. Children 2022, 9, 1462. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, D.; Holguin, F. Metabolic Dysregulation, Systemic Inflammation, and Pediatric Obesity-Related Asthma. Ann. Am. Thorac. Soc. 2017, 14, S363–S367. [Google Scholar] [CrossRef] [PubMed]
- Lam, S.S.W.; Fang, A.H.S.; Koh, M.S.; Shantakumar, S.; Yeo, S.H.; Matchar, D.B.; Ong, M.E.H.; Poon, K.M.T.; Huang, L.; Harikrishan, S.; et al. Development of a Real-World Database for Asthma and COPD: The SingHealth-Duke-NUS-GSK COPD and Asthma Real-World Evidence (SDG-CARE) Collaboration. BMC Med. Inform. Decis. Mak. 2023, 23, 4. [Google Scholar] [CrossRef] [PubMed]
- Boue, S.; Fields, B.; Hoeng, J.; Park, J.; Peitsch, M.C.; Schlage, W.K.; Talikka, M.; Binenbaum, I.; Bondarenko, V.; Bulgakov, O.V.; et al. Enhancement of COPD Biological Networks Using a Web-Based Collaboration Interface. F1000Research 2015, 4, 32. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Schedule of Assessments, Tests, and Procedures | Group A | Group B | Group C | Group D | Group E | |
|---|---|---|---|---|---|---|
| Asthma and Normal Weight | Asthma and Overweight or Obese | Obese or Overweight and No Asthma | Normal Weight and No Asthma | Siblings of Groups A and B | ||
| Demographics and Medical History | ◎ | ◎ | ◎ | ◉ | ◉ | |
| Questionnaires SOAP questionnaire (age 6–12 years, 13–17 years) Peds QL (asthma and quality of life modules (ages 5–7, 8–12, and 13–17 years) Food frequency questionnaire (FFQ) and 3-day food diary | ◉ | ◉ | ◉ | ◉ | ◉ | |
| Anthropometry (height, weight, NC, CC, WC, HC) | ◎ | ◎ | ◎ | ◉ | ◉ | |
| Physical examination (blood pressure (systolic/diastolic), heart rate, respiratory rate, body temperature) | ◎ | ◎ | ◎ | ◉ | ◉ | |
| Bioimpedance measures (BMI, fat %, fat mass, free fat mass (FFT), total body water (TBW), basal metabolic rate (BMR)) | ◉ | ◉ | ◉ | ◉ | ◉ | |
| Pulmonary function tests (PFTs) Spirometry (FVC, FEV1, FEV1/ FVC, FEF 25–75%, PEF, PIF, FET) Plethysmography (sRAW, VC, IC, FRCpleth, ERV, RV, TLC, RV/TLC) | ◎ | ◎ | ◉ | ◉ | ◉ | |
| Bronchodilator response | ◎ | ◎ | ||||
| Fractional exhaled nitric oxide (FeNO) | ◎ | ◎ | ◉ | ◉ | ◉ | |
| Lung clearance index (LCI) | ◎ | ◎ | ◉ | ◉ | ◉ | |
| Allergy test (skin prick) | ◎ | ◎ | ||||
| Blood tests | ||||||
| FBC, biochemistry, vitamin D, TSH, FT4 | ◎ | ◎ | ◎ | ◎ | ◎ | |
| Allergy test | ◎ | ◎ | ||||
| HbA1c, insulin, C-peptide | ◉ | ◉ | ◎ | |||
| Oral glucose tolerance test (OGTT), HOMA-IR, lipid profile | ◉ | ◎ | ||||
| Biological samples (fasted for at least 2 h) | ||||||
| Blood | Sphingolipids, SPT assay, lipidomics, metabolomics, cytokines, whole-genome sequencing, DNA methylation, RNA-Seq, miRNA | ◉ | ◉ | ◉ | ◉ | ◉ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antonisamy, B.; Shailesh, H.; Hani, Y.; Ahmed, L.H.M.; Noor, S.; Ahmed, S.Y.; Alfaki, M.; Muhayimana, A.; Jacob, S.S.; Balayya, S.K.; et al. Sphingolipids in Childhood Asthma and Obesity (SOAP Study): A Protocol of a Cross-Sectional Study. Metabolites 2023, 13, 1146. https://doi.org/10.3390/metabo13111146
Antonisamy B, Shailesh H, Hani Y, Ahmed LHM, Noor S, Ahmed SY, Alfaki M, Muhayimana A, Jacob SS, Balayya SK, et al. Sphingolipids in Childhood Asthma and Obesity (SOAP Study): A Protocol of a Cross-Sectional Study. Metabolites. 2023; 13(11):1146. https://doi.org/10.3390/metabo13111146
Chicago/Turabian StyleAntonisamy, Belavendra, Harshita Shailesh, Yahya Hani, Lina Hayati M. Ahmed, Safa Noor, Salma Yahya Ahmed, Mohamed Alfaki, Abidan Muhayimana, Shana Sunny Jacob, Saroja Kotegar Balayya, and et al. 2023. "Sphingolipids in Childhood Asthma and Obesity (SOAP Study): A Protocol of a Cross-Sectional Study" Metabolites 13, no. 11: 1146. https://doi.org/10.3390/metabo13111146