

The Combined Intervention of Aqua Exercise and Burdock Extract Synergistically Improved Arterial Stiffness: A Randomized, Double-Blind, Controlled Trial

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
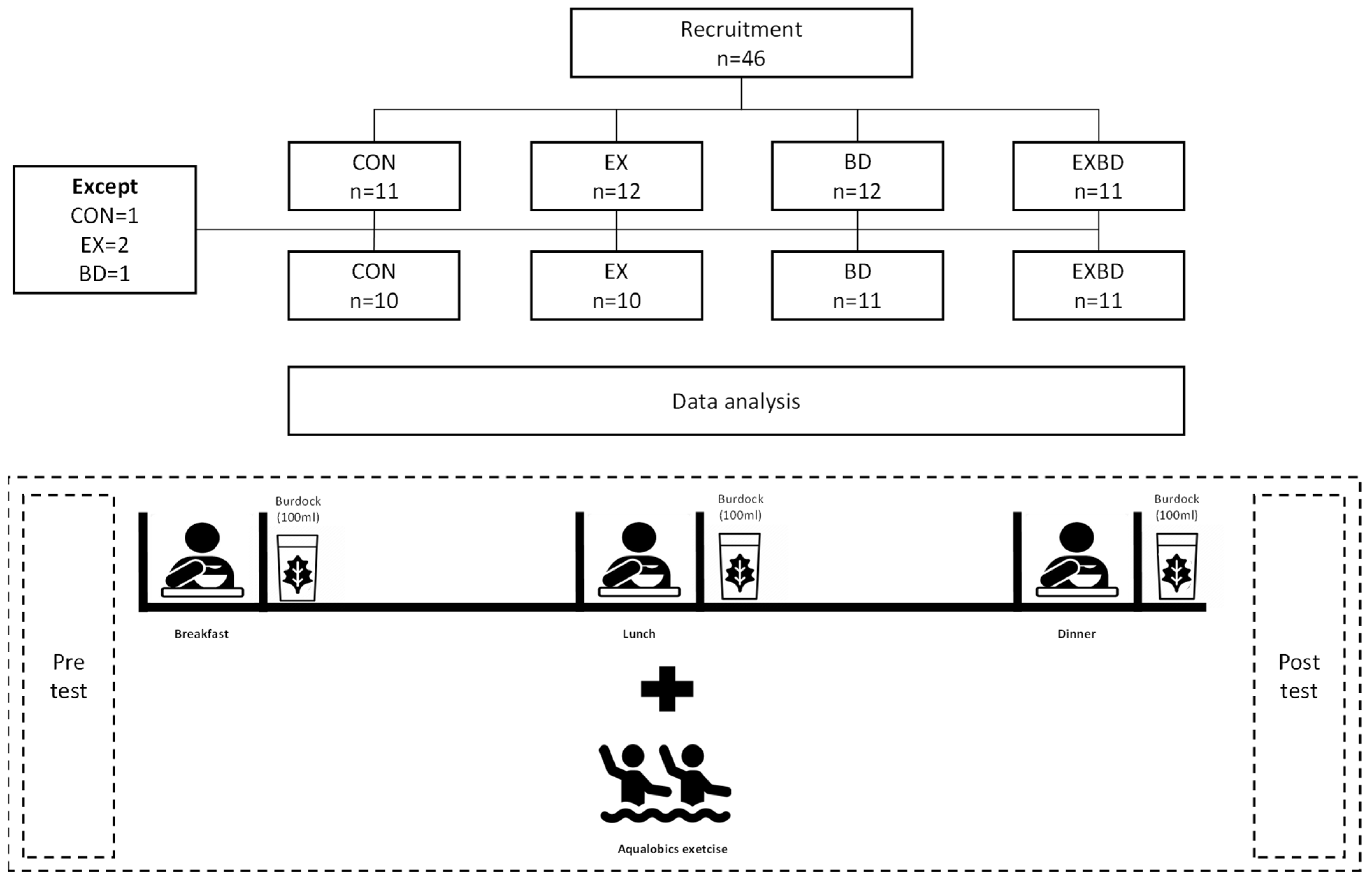
2.1. Participants
2.2. Study Design
2.3. Burdock Extract Preparation and Composition
2.4. Aqua Exercise Program
2.5. Blood Pressure
2.6. Blood Sampling
2.6.1. Glucose
2.6.2. Insulin
2.6.3. Homeostasis Model Assessment of Insulin Resistance and Quantitative Insulin Sensitivity Check Index
QUICKI = 1/[log (fasting insulin) + log (fasting glucose)]
2.6.4. PGI2
2.6.5. TXA2
2.7. Arterial Stiffness
2.8. Sample Size Calculation
2.9. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Blood Pressure
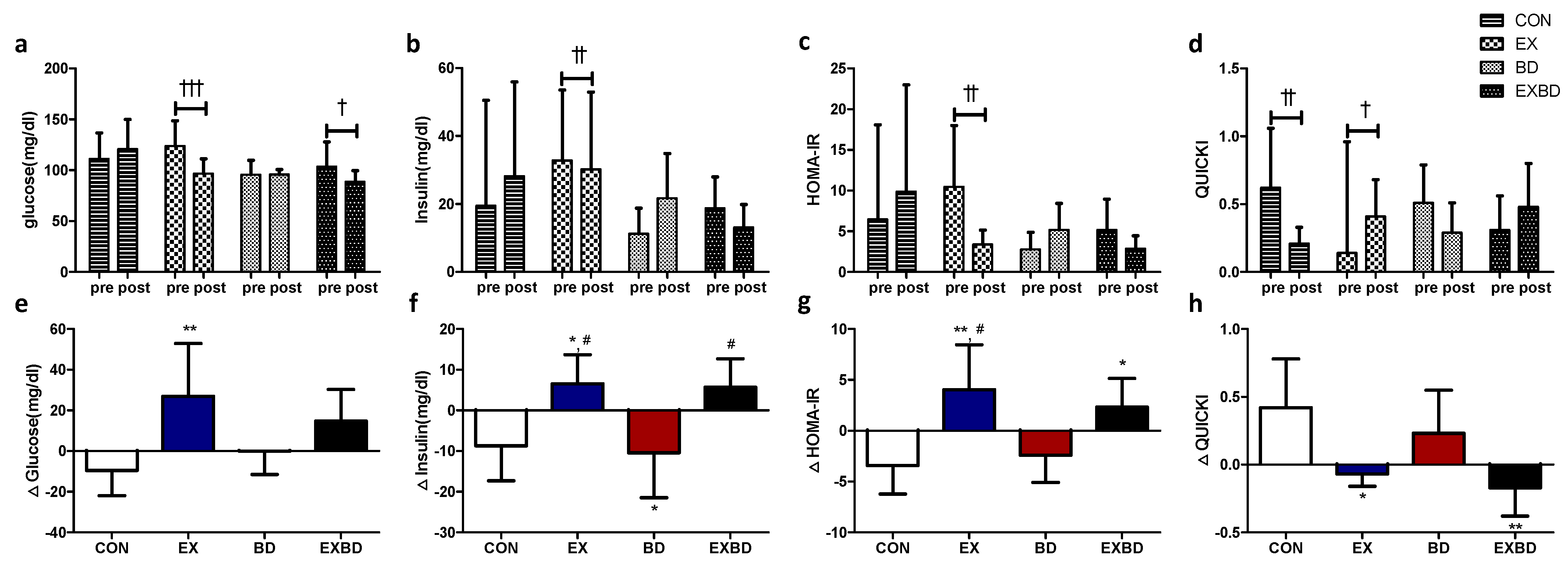
3.3. Insulin Resistance
3.4. Vascular Regulation Factors
3.5. Arterial Stiffness
3.6. Correlation among Variations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vega, G.L. Cardiovascular Outcomes for Obesity and Metabolic Syndrome. Obes. Res. 2002, 10, 27S–32S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Expert Panel on Detection Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Tillin, T.; Forouhi, N.; Johnston, D.G.; McKeigue, P.M.; Chaturvedi, N.; Godsland, I.F. Metabolic Syndrome and Coronary Heart Disease in South Asians, African-Caribbeans and White Europeans: A UK Population-Based Cross-Sectional Study. Diabetologia 2005, 48, 649–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mykkänen, L.; Kuusisto, J.; Pyörälä, K.; Laakso, M. Cardiovascular Disease Risk Factors as Predictors of Type 2 (Non-Insulin-Dependent) Diabetes Mellitus in Elderly Subjects. Diabetologia 1993, 36, 553–559. [Google Scholar] [CrossRef] [Green Version]
- Foright, R.M.; Presby, D.M.; Sherk, V.D.; Kahn, D.; Checkley, L.A.; Giles, E.D.; Bergouignan, A.; Higgins, J.A.; Jackman, M.R.; Hill, J.O.; et al. Is Regular Exercise an Effective Strategy for Weight Loss Maintenance? Physiol. Behav. 2018, 188, 86–93. [Google Scholar] [CrossRef]
- Sypniewska, G. Pro-Inflammatory and Prothrombotic Factors and Metabolic Syndrome. EJIFCC 2007, 18, 39–46. [Google Scholar] [PubMed]
- Brook, R.D.; Bard, R.L.; Rubenfire, M.; Ridker, P.M.; Rajagopalan, S. Usefulness of Visceral Obesity (Waist/Hip Ratio) in Predicting Vascular Endothelial Function in Healthy Overweight Adults. Am. J. Cardiol. 2001, 88, 1264–1269. [Google Scholar] [CrossRef]
- McVeigh, G.E.; Brennan, G.M.; Johnston, G.D.; McDermott, B.J.; McGrath, L.T.; Henry, W.R.; Andrews, J.W.; Hayes, J.R. Impaired Endothelium-Dependent and Independent Vasodilation in Patients with Type 2 (Non-Insulin-Dependent) Diabetes Mellitus. Diabetologia 1992, 35, 771–776. [Google Scholar] [CrossRef]
- Furchgott, R.F.; Zawadzki, J.V. The Obligatory Role of Endothelial Cells in the Relaxation of Arterial Smooth Muscle by Acetylcholine. Nature 1980, 288, 373–376. [Google Scholar] [CrossRef]
- Riddell, D.R.; Owen, J.S. Nitric Oxide and Platelet Aggregation. Vitam. Horm. 1997, 57, 25–48. [Google Scholar] [CrossRef]
- Nicosia, S.; Oliva, D.; Bernini, F.; Fumagalli, R. Prostacyclin-sensitive Adenylate Cyclase and Prostacyclin Binding Sites in Platelets and Smooth Muscle Cells. Adv. Cycl. Nucleotide Protein Phosphorylation Res. 1984, 17, 593–599. [Google Scholar] [PubMed]
- Fournier, S.B.; Reger, B.L.; Donley, D.A.; Bonner, D.E.; Warden, B.E.; Gharib, W.; Failinger, C.F.; Olfert, M.D.; Frisbee, J.C.; Olfert, I.M.; et al. Exercise Reveals Impairments in Left Ventricular Systolic Function in Patients with Metabolic Syndrome. Exp. Physiol. 2014, 99, 149–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scuteri, A.; Najjar, S.S.; Orru’, M.; Usala, G.; Piras, M.G.; Ferrucci, L.; Cao, A.; Schlessinger, D.; Uda, M.; Lakatta, E.G. The Central Arterial Burden of the Metabolic Syndrome Is Similar in Men and Women: The SardiNIA Study. Eur. Heart J. 2010, 31, 602–613. [Google Scholar] [CrossRef] [PubMed]
- Safar, M.E.; Thomas, F.; Blacher, J.; Nzietchueng, R.; Bureau, J.M.; Pannier, B.; Benetos, A. Metabolic Syndrome and Age-Related Progression of Aortic Stiffness. J. Am. Coll. Cardiol. 2006, 47, 72–75. [Google Scholar] [CrossRef]
- Malik, S.; Wong, N.D.; Franklin, S.S.; Kamath, T.V.; L’Italien, G.J.; Pio, J.R.; Williams, G.R. Impact of the Metabolic Syndrome on Mortality from Coronary Heart Disease, Cardiovascular Disease, and All Causes in United States Adults. Circulation 2004, 110, 1245–1250. [Google Scholar] [CrossRef]
- Gami, A.S.; Witt, B.J.; Howard, D.E.; Erwin, P.J.; Gami, L.A.; Somers, V.K.; Montori, V.M. Metabolic Syndrome and Risk of Incident Cardiovascular Events and Death. A Systematic Review and Meta-Analysis of Longitudinal Studies. J. Am. Coll. Cardiol. 2007, 49, 403–414. [Google Scholar] [CrossRef] [Green Version]
- Stachowiak, G.; Pertyński, T.; Pertyńska-Marczewska, M. Metabolic Disorders in Menopause. Prz. Menopauzalny 2015, 14, 59–64. [Google Scholar] [CrossRef]
- Golbidi, S.; Mesdaghinia, A.; Laher, I. Exercise in the Metabolic Syndrome. Oxid. Med. Cell. Longev. 2012, 2012, 349710. [Google Scholar] [CrossRef] [Green Version]
- Barbosa, T.M.; Garrido, M.F.; Bragada, J. Physiological Adaptations to Head-out Aquatic Exercises with Different Levels of Body Immersion. J. Strength Cond. Res. 2007, 21, 1255–1259. [Google Scholar] [CrossRef]
- Ha, M.-S.; Kim, J.-H.; Ha, S.-M.; Kim, Y.-S.; Kim, D.-Y. Positive Influence of Aqua Exercise and Burdock Extract Intake on Fitness Factors and Vascular Regulation Substances in Elderly. J. Clin. Biochem. Nutr. 2019, 64, 73–78. [Google Scholar] [CrossRef]
- Ha, M.S.; Yook, J.S.; Lee, M.; Suwabe, K.; Jeong, W.M.; Kwak, J.-J.; Soya, H. Exercise Training and Burdock Root (Arctium Lappa L.) Extract Independently Improve Abdominal Obesity and Sex Hormones in Elderly Women with Metabolic Syndrome. Sci. Rep. 2021, 11, 5175. [Google Scholar] [CrossRef] [PubMed]
- Cunha, R.M.; Macedo, C.B.; Araújo, S.F.M.; Santos, J.C.; Borges, V.S.; Soares, A.A.; Ayres, F.; Pfrimer, L.M. Subacute Blood Pressure Response in Elderly Hypertensive Women after a Water Exercise Session: A Controlled Clinical Trial. High Blood Press. Cardiovasc. Prev. 2012, 19, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Ha, M.S.; Ha, S.M.; Kim, D.Y. Aquatic Exercise Positively Affects Physiological Frailty among Postmenopausal Women: A Randomized Controlled Clinical Trial. Healthcare 2021, 9, 409. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Li, C.; Zhang, P.; Cao, X.; Huang, T.; Bai, Y.; Chen, K. Antidiabetic Effect of Burdock (Arctium Lappa L.) Root Ethanolic Extract on Streptozotocin-induced Diabetic Rats. African J. Biotechnol. 2012, 11, 9079–9085. [Google Scholar] [CrossRef]
- Ha, M.S.; Kim, J.H.; Kim, Y.S.; Kim, D.Y. Effects of Aquarobic Exercise and Burdock Intake on Serum Blood Lipids and Vascular Elasticity in Korean Elderly Women. Exp. Gerontol. 2018, 101, 63–68. [Google Scholar] [CrossRef]
- Wang, B.-S.; Yen, G.C.; Chang, L.W.; Yen, W.J.; Duh, P. Protective Effects of Burdock (Arctium Lappa Linne) on Oxidation of Low-Density Lipoprotein and Oxidative Stress in RAW 264.7 Macrophages. Food Chem. 2007, 101, 729–738. [Google Scholar] [CrossRef]
- Kim, B.Y.; Kang, S.M.; Kang, J.H.; Kang, S.Y.; Kim, K.K.; Kim, K.B.; Kim, B.; Kim, S.J.; Kim, Y.H.; Kim, J.H.; et al. 2020 Korean Society for the Study of Obesity Guidelines for the Management of Obesity in Korea. J. Obes. Metab. Syndr. 2021, 30, 81–92. [Google Scholar] [CrossRef]
- Borg, G. Perceived Exertion as an Indicator of Somatic Stress. Scand. J. Rehabil. Med. 1970, 2, 92–98. [Google Scholar]
- Ha, M.-S.; Baek, H. Floor Exercise Improves on Senior Fitness Test, Blood Lipids and Arterial Stiffness in Elderly Women with Metabolic Syndrome. J. Korean Appl. Sci. Technol. 2017, 34, 899–907. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and β-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Katz, A.; Nambi, S.S.; Mather, K.; Baron, A.D.; Follmann, D.A.; Sullivan, G.; Quon, M.J. Quantitative Insulin Sensitivity Check Index: A Simple, Accurate Method for Assessing Insulin Sensitivity in Humans. J. Clin. Endocrinol. Metab. 2000, 85, 2402–2410. [Google Scholar] [CrossRef] [PubMed]
- Van Bortel, L.M.; Duprez, D.; Starmans-Kool, M.J.; Safar, M.E.; Giannattasio, C.; Cockcroft, J.; Kaiser, D.R.; Thuillez, C. Clinical Applications of Arterial Stiffness, Task Force III: Recommendations for User Procedures. Am. J. Hypertens. 2002, 15, 445–452. [Google Scholar] [CrossRef] [Green Version]
- Laurent, S.; Cockcroft, J.; Van Bortel, L.; Boutouyrie, P.; Giannattasio, C.; Hayoz, D.; Pannier, B.; Vlachopoulos, C.; Wilkinson, I.; Struijker-Boudier, H. Expert Consensus Document on Arterial Stiffness: Methodological Issues and Clinical Applications. Eur. Heart J. 2006, 27, 2588–2605. [Google Scholar] [CrossRef] [Green Version]
- Kelly, R.; Hayward, C.; Avolio, A.; O’Rourke, M. Noninvasive Determination of Age-Related Changes in the Human Arterial Pulse. Circulation 1989, 80, 1652–1659. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Morino, K.; Petersen, K.F.; Shulman, G.I. Molecular Mechanisms of Insulin Resistance in Humans and Their Potential Links with Mitochondrial Dysfunction. Diabetes 2006, 55, S9–S15. [Google Scholar] [CrossRef] [Green Version]
- McLaughlin, T.; Abbasi, F.; Cheal, K.; Chu, J.; Lamendola, C.; Reaven, G. Use of Metabolic Markers to Identify Overweight Individuals Who Are Insulin Resistant. Ann. Intern. Med. 2003, 139, 802–809. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.A.; Montagnani, M.; Kwang, K.K.; Quon, M.J. Reciprocal Relationships between Insulin Resistance and Endothelial Dysfunction: Molecular and Pathophysiological Mechanisms. Circulation 2006, 113, 1888–1904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carr, M.C. The Emergence of the Metabolic Syndrome with Menopause. J. Clin. Endocrinol. Metab. 2003, 88, 2404–2411. [Google Scholar] [CrossRef] [Green Version]
- Kitahara, C.M.; Trabert, B.; Katki, H.A.; Chaturvedi, A.K.; Kemp, T.J.; Pinto, L.A.; Moore, S.C.; Purdue, M.P.; Wentzensen, N.; Hildesheim, A.; et al. Body Mass Index, Physical Activity, and Serum Markers of Inflammation, Immunity, and Insulin Resistance. Cancer Epidemiol. Biomark. Prev. 2014, 23, 2840–2849. [Google Scholar] [CrossRef] [Green Version]
- Balkau, B.; Mhamdi, L.; Oppert, J.M.; Nolan, J.; Golay, A.; Porcellati, F.; Laakso, M.; Ferrannini, E. Physical Activity and Insulin Sensitivity: The RISC Study. Diabetes 2008, 57, 2613–2618. [Google Scholar] [CrossRef] [Green Version]
- National High Blood Pressure Education Program Working Group Report on Hypertension in the Elderly. National High Blood Pressure Education Program Working Group. Hypertension 1994, 23, 275–285. [Google Scholar] [CrossRef]
- Sanz, C.; Gautier, J.-F.; Hanaire, H. Physical Exercise for the Prevention and Treatment of Type 2 Diabetes. Diabetes Metab. 2010, 36, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Rezaeimanesh, D.; Farsani, P.A. The Effect of an 8-Week Selected Aquatic Aerobic Training Period on Plasma Leptin and Insulin Resistance in Men with Type 2 Diabetes. J. Adv. Pharm. Educ. Res. 2019, 9, 121–124. [Google Scholar]
- Lupattelli, G.; Lombardini, R.; Schillaci, G.; Ciuffetti, G.; Marchesi, S.; Siepi, D.; Mannarino, E. Flow-mediated Vasoactivity and Circulating Adhesion Molecules in Hypertriglyceridemia: Association with Small, Dense LDL Cholesterol Particles. Am. Heart J. 2000, 140, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Vanhoutte, P.M.; Shimokawa, H.; Tang, E.H.C.; Feletou, M. Endothelial Dysfunction and Vascular Disease. Acta Physiol. 2009, 196, 193–222. [Google Scholar] [CrossRef] [Green Version]
- Bunting, S.; Moncada, S.; Vane, J.R.; Gryglewski, R. Arterial Walls Generate from Prostaglandin Endoperoxides a Substance (Prostaglandin X) Which Relaxes Strips of Mesenteric and Coeliac Arteries and Inhibits Platelet Aggregation. Prostaglandins 1976, 12, 897–913. [Google Scholar] [CrossRef]
- Moncada, S.; Higgs, E.A.; Vane, J.R. Human Arterial and Venous Tissues Generate Prostacyclin (Prostaglandin X), a Potent Inhibitor of Platelet Aggregation. Lancet 1977, 309, 18–21. [Google Scholar] [CrossRef]
- Gamez-Mendez, A.M.; Vargas-Robles, H.; Ríos, A.; Escalante, B. Oxidative Stress-dependent Coronary Endothelial Dysfunction in Obese Mice. PLoS ONE 2015, 10, e0138609. [Google Scholar] [CrossRef] [Green Version]
- Nakahata, N. Thromboxane A2: Physiology/Pathophysiology, Cellular Signal Transduction and Pharmacology. Pharmacol. Ther. 2008, 118, 18–35. [Google Scholar] [CrossRef]
- Erhart, S.; Beer, J.H.; Reinhart, W.H. Influence of Aspirin on Platelet Count and Volume in Humans. Acta Haematol. 1999, 101, 140–144. [Google Scholar] [CrossRef]
- Pahakis, M.Y.; Kosky, J.R.; Dull, R.O.; Tarbell, J.M. The Role of Endothelial Glycocalyx Components in Mechanotransduction of Fluid Shear Stress. Biochem. Biophys. Res. Commun. 2007, 355, 228–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, A.H.; Nyberg, M.; Bangsbo, J.; Saltin, B.; Hellsten, Y. Exercise Training Alters the Balance between Vasoactive Compounds in Skeletal Muscle of Individuals with Essential Hypertension. Hypertension 2011, 58, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Lee, Y.; Sohn, H. Anti-Thrombosis and Anti-Oxidative Activity of the Root of Arctium Lappa L. Korean J. Food Preserv. 2014, 21, 727–734. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.J.; Choi, D.H.; Cho, G.H.; Kim, J.S.; Kang, D.G.; Lee, H.S. Arctium Lappa Ameliorates Endothelial Dysfunction in Rats Fed with High Fat/Cholesterol Diets. BMC Complement. Altern. Med. 2012, 12, 116. [Google Scholar] [CrossRef] [Green Version]
- Furukawa, S.; Fujita, T.; Shimabukuro, M.; Iwaki, M.; Yamada, Y.; Nakajima, Y.; Nakayama, O.; Makishima, M.; Matsuda, M.; Shimomura, I. Increased Oxidative Stress in Obesity and Its Impact on Metabolic Syndrome. J. Clin. Investig. 2004, 114, 1752–1761. [Google Scholar] [CrossRef]
- Stocker, R.; Keaney, J.F. Role of Oxidative Modifications in Atherosclerosis. Physiol. Rev. 2004, 84, 1381–1478. [Google Scholar] [CrossRef]
- MalaisseI, W.J.; Conget, I.; Sener, A.; Rorsman, P. Insulinotropic Action of AICA Riboside. II. Secretory, Metabolic and Cationic Aspects. Diabetes Res. 1994, 25, 25–37. [Google Scholar] [PubMed]
- Vlachopoulos, C.; Xaplanteris, P.; Aboyans, V.; Brodmann, M.; Cífková, R.; Cosentino, F.; De Carlo, M.; Gallino, A.; Landmesser, U.; Laurent, S.; et al. The Role of Vascular Biomarkers for Primary and Secondary Prevention. A Position Paper from the European Society of Cardiology Working Group on Peripheral Circulation: Endorsed by the Association for Research into Arterial Structure and Physiology (ARTERY) Society. Atherosclerosis 2015, 241, 507–532. [Google Scholar] [CrossRef] [Green Version]
- Laurent, S.; Boutouyrie, P.; Asmar, R.; Gautier, I.; Laloux, B.; Guize, L.; Ducimetiere, P.; Benetos, A. Aortic Stiffness Is an Independent Predictor of All-cause and Cardiovascular Mortality in Hypertensive Patients. Hypertension 2001, 37, 1236–1241. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.J.; Kim, Y.J.; Cho, B.M.; Lee, S. Metabolic Syndrome and Arterial Pulse Wave Velocity. Acta Cardiol. 2010, 65, 315–321. [Google Scholar] [CrossRef]
- Padilla, J.; Harris, R.A.; Wallace, J.P. Can the Measurement of Brachial Artery Flow-mediated Dilation Be Applied to the Acute Exercise Model? Cardiovasc. Ultrasound 2007, 5, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donley, D.A.; Fournier, S.B.; Reger, B.L.; DeVallance, E.; Bonner, D.E.; Olfert, I.M.; Frisbee, J.C.; Chantler, P.D. Aerobic Exercise Training Reduces Arterial Stiffness in Metabolic Syndrome. J. Appl. Physiol. 2014, 116, 1396–1404. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.A.; Wu, A.B.; Chen, C.Y. The Influence of Different Treatments on the Free Radical Scavenging Activity of Burdock and Variations of Its Active Components. Food Chem. 2004, 86, 479–484. [Google Scholar] [CrossRef]
- Wang, P.; Zweier, J.L. Measurement of Nitric Oxide and Peroxynitrite Generation in the Postischemic Heart: Evidence for Peroxynitrite-mediated Reperfusion Injury. J. Biol. Chem. 1996, 271, 29223–29230. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Ha, S.J.; Park, J.; Kim, Y.H.; Lee, N.H.; Kim, Y.E.; Hong, Y.S.; Song, K.M. Arctium Lappa Root Extract Containing L-Arginine Prevents TNF-α-induced Early Atherosclerosis in Vitro and in Vivo. Nutr. Res. 2020, 77, 85–96. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ha, M.-S.; Lee, J.-H.; Jeong, W.-M.; Kim, H.R.; Son, W.H. The Combined Intervention of Aqua Exercise and Burdock Extract Synergistically Improved Arterial Stiffness: A Randomized, Double-Blind, Controlled Trial. Metabolites 2022, 12, 970. https://doi.org/10.3390/metabo12100970
Ha M-S, Lee J-H, Jeong W-M, Kim HR, Son WH. The Combined Intervention of Aqua Exercise and Burdock Extract Synergistically Improved Arterial Stiffness: A Randomized, Double-Blind, Controlled Trial. Metabolites. 2022; 12(10):970. https://doi.org/10.3390/metabo12100970
Chicago/Turabian StyleHa, Min-Seong, Jae-Hoon Lee, Woo-Min Jeong, Hyun Ryun Kim, and Woo Hyeon Son. 2022. "The Combined Intervention of Aqua Exercise and Burdock Extract Synergistically Improved Arterial Stiffness: A Randomized, Double-Blind, Controlled Trial" Metabolites 12, no. 10: 970. https://doi.org/10.3390/metabo12100970