
Assessing the Potential of Untargeted SWATH Mass Spectrometry-Based Metabolomics to Differentiate Closely Related Exposures in Observational Studies

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Samples
2.2. Small-Molecule Profiling
2.3. Data Processing
3. Results and Discussion
3.1. Sample Analysis
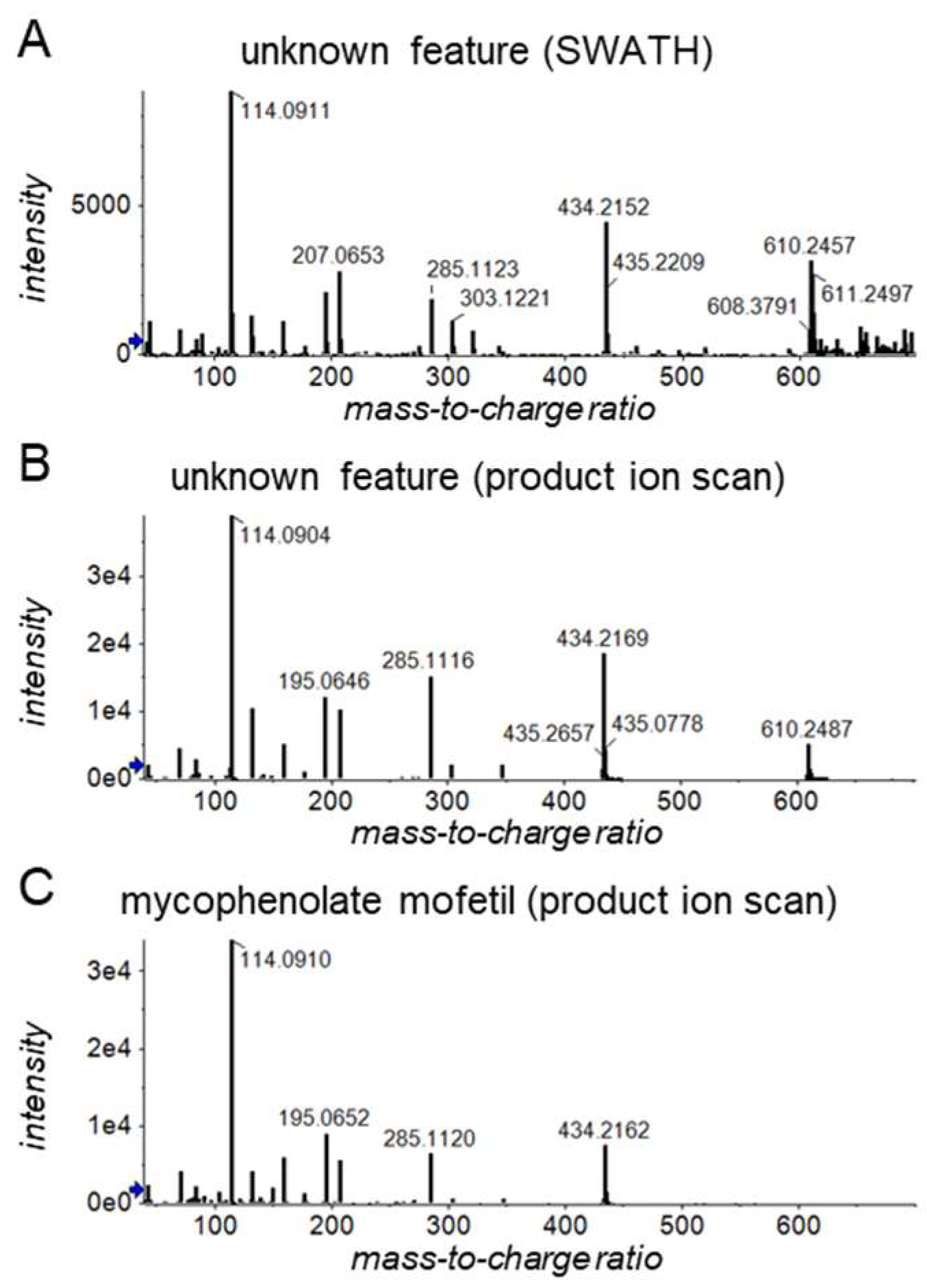
3.2. Mycophenolate Versus Mycophenolate Mofetil
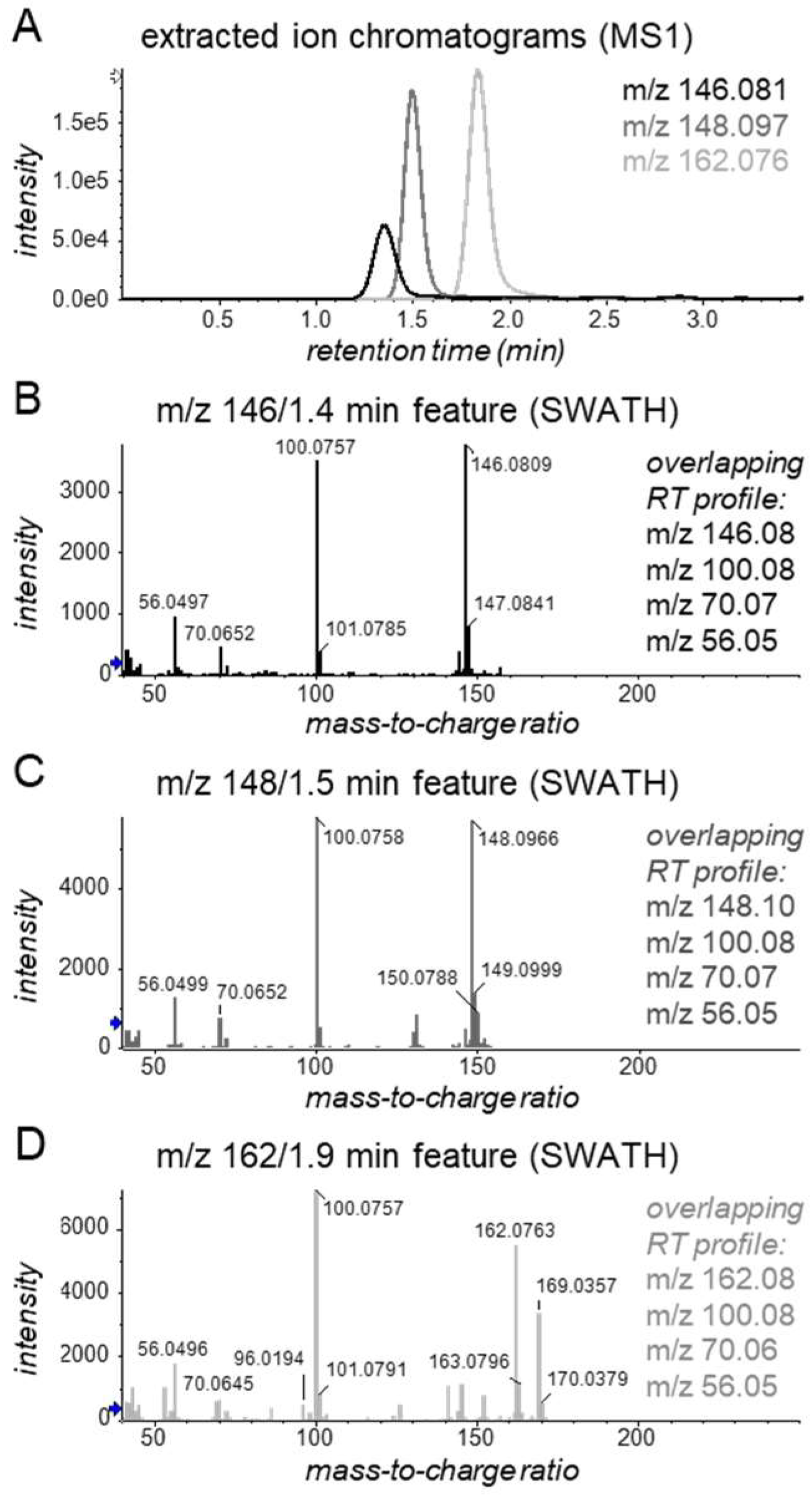
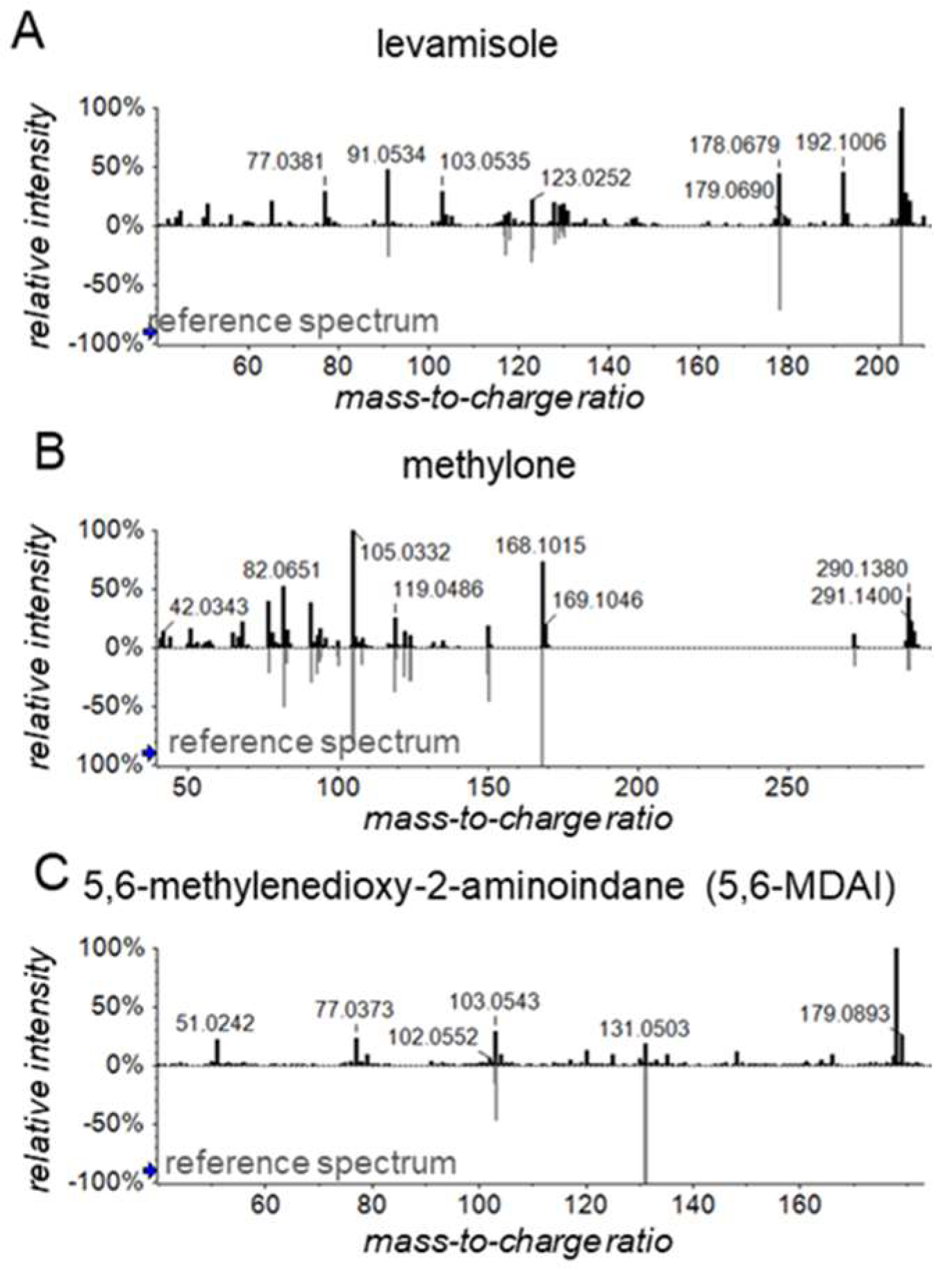
3.3. Cocaine Adulteration
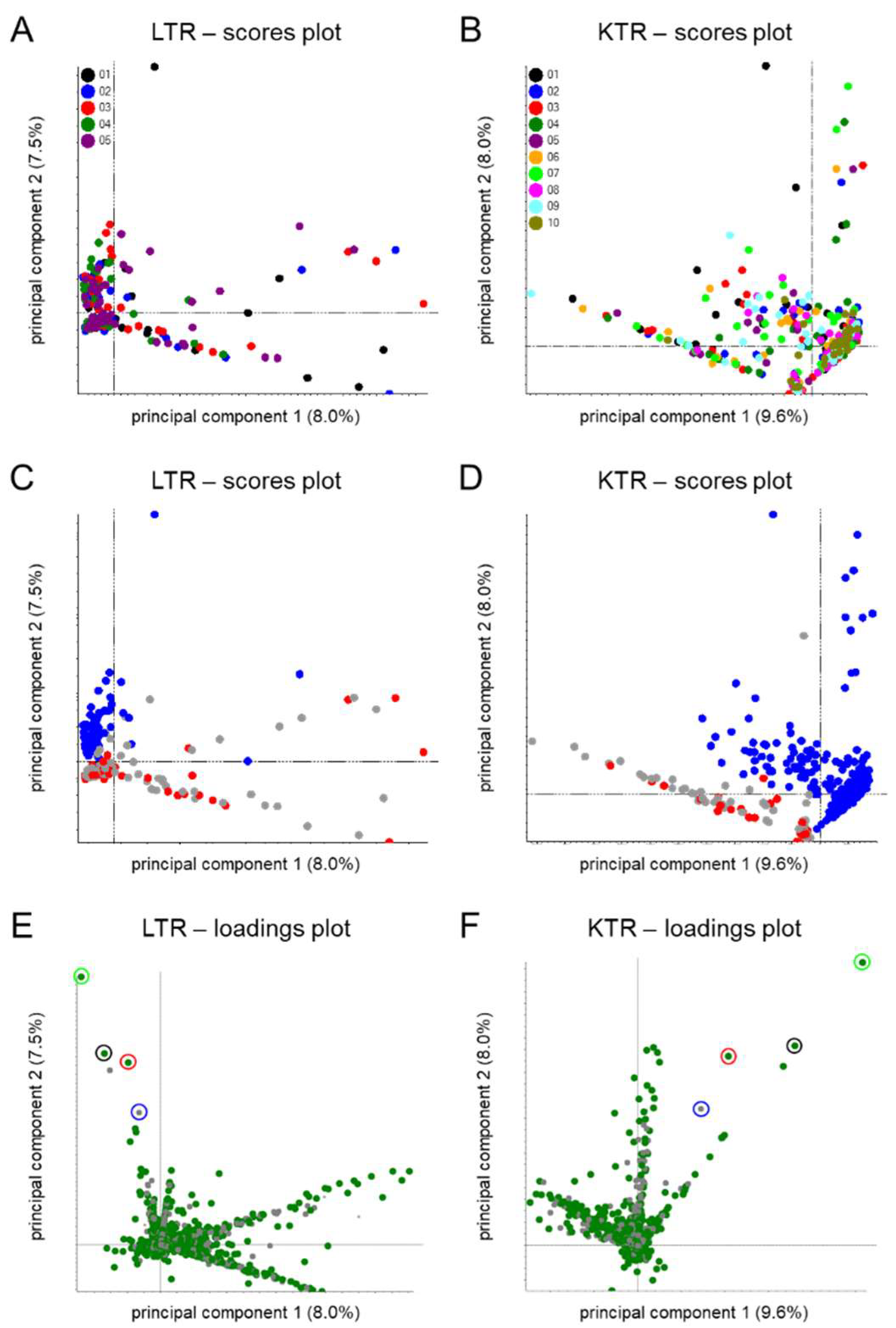
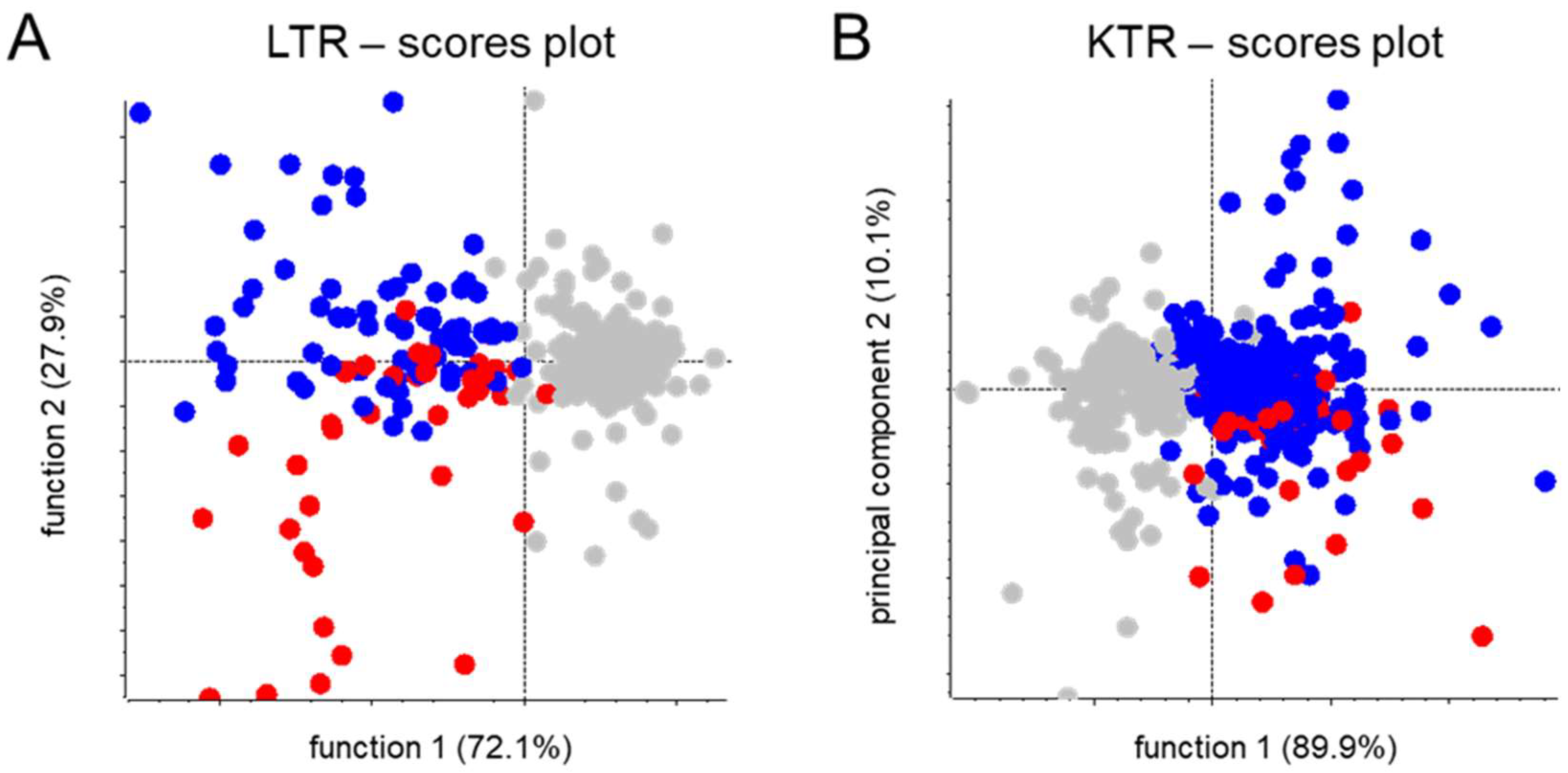
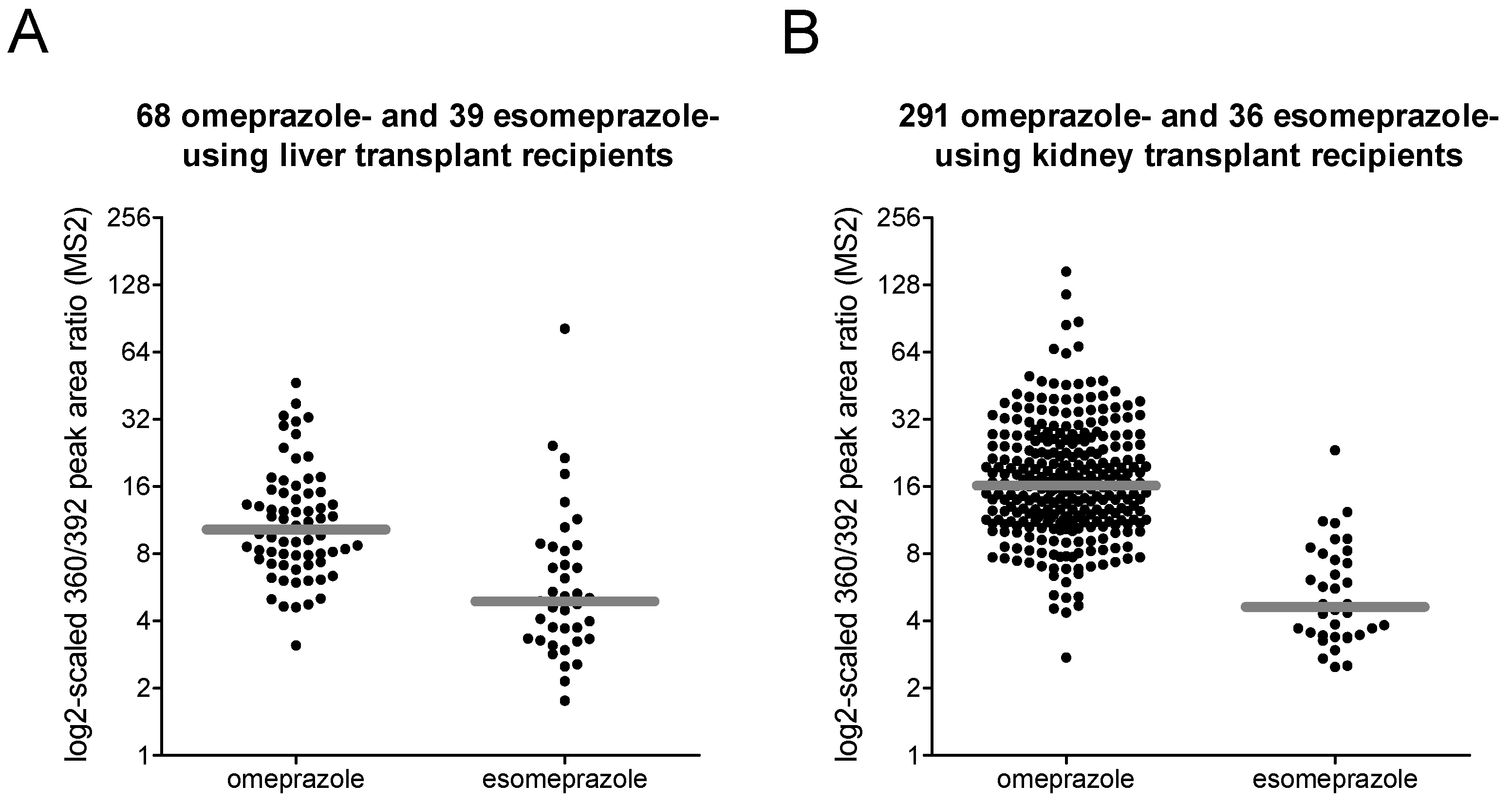
3.4. Omeprazole Versus Esomeprazole
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Braveman, P.; Gottlieb, L. The social determinants of health: It’s time to consider the causes of the causes. Public Health Rep. 2014, 129 (Suppl. S2), 19–31. [Google Scholar] [CrossRef] [Green Version]
- Buermans, H.P.; den Dunnen, J.T. Next generation sequencing technology: Advances and applications. Biochim. Biophys. Acta 2014, 1842, 1932–1941. [Google Scholar] [CrossRef] [Green Version]
- Prince, S.A.; Adamo, K.B.; Hamel, M.E.; Hardt, J.; Connor Gorber, S.; Tremblay, M. A comparison of direct versus self-report measures for assessing physical activity in adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahm, C.C.; Keogh, R.H.; Spencer, E.A.; Greenwood, D.C.; Key, T.J.; Fentiman, I.S.; Shipley, M.J.; Brunner, E.J.; Cade, J.E.; Burley, V.J.; et al. Dietary fiber and colorectal cancer risk: A nested case-control study using food diaries. J. Natl. Cancer Inst. 2010, 102, 614–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellinger, C.; Mohomed Jabbar, M.S.; Zaiane, O.; Osornio-Vargas, A. A systematic review of data mining and machine learning for air pollution epidemiology. BMC Public Health 2017, 17, 907. [Google Scholar] [CrossRef] [Green Version]
- Jensen, P.B.; Jensen, L.J.; Brunak, S. Mining electronic health records: Towards better research applications and clinical care. Nat. Rev. Genet 2012, 13, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Hofker, M.H.; Fu, J.; Wijmenga, C. The genome revolution and its role in understanding complex diseases. Biochim. Biophys. Acta 2014, 1842, 1889–1895. [Google Scholar] [CrossRef] [Green Version]
- Collins, F.S.; Morgan, M.; Patrinos, A. The Human Genome Project: Lessons from large-scale biology. Science 2003, 300, 286–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Healey, E.L.; Allen, K.D.; Bennell, K.; Bowden, J.L.; Quicke, J.G.; Smith, R. Self-Report Measures of Physical Activity. Arthritis Care Res. (Hoboken) 2020, 72 (Suppl. S10), 717–730. [Google Scholar] [CrossRef] [PubMed]
- Dao, M.C.; Subar, A.F.; Warthon-Medina, M.; Cade, J.E.; Burrows, T.; Golley, R.K.; Forouhi, N.G.; Pearce, M.; Holmes, B.A. Dietary assessment toolkits: An overview. Public Health Nutr. 2019, 22, 404–418. [Google Scholar] [CrossRef]
- Sediq, R.; van der Schans, J.; Dotinga, A.; Alingh, R.A.; Wilffert, B.; Bos, J.H.; Schuiling-Veninga, C.C.; Hak, E. Concordance assessment of self-reported medication use in the Netherlands three-generation Lifelines Cohort study with the pharmacy database iaDB.nl: The PharmLines initiative. Clin. Epidemiol. 2018, 10, 981–989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunmair, J.; Bileck, A.; Stimpfl, T.; Raible, F.; Del Favero, G.; Meier-Menches, S.M.; Gerner, C. Metabo-tip: A metabolomics platform for lifestyle monitoring supporting the development of novel strategies in predictive, preventive and personalised medicine. EPMA J. 2021, 12, 141–153. [Google Scholar] [CrossRef]
- Scalbert, A.; Brennan, L.; Manach, C.; Andres-Lacueva, C.; Dragsted, L.O.; Draper, J.; Rappaport, S.M.; van der Hooft, J.J.; Wishart, D.S. The food metabolome: A window over dietary exposure. Am. J. Clin. Nutr. 2014, 99, 1286–1308. [Google Scholar] [CrossRef] [Green Version]
- Beger, R.D.; Schmidt, M.A.; Kaddurah-Daouk, R. Current Concepts in Pharmacometabolomics, Biomarker Discovery, and Precision Medicine. Metabolites 2020, 10, 129. [Google Scholar] [CrossRef] [Green Version]
- Van de Luitgaarden, I.A.T.; Beulens, J.W.J.; Schrieks, I.C.; Kieneker, L.M.; Touw, D.J.; van Ballegooijen, A.J.; van Oort, S.; Grobbee, D.E.; Bakker, S.J.L. Urinary Ethyl Glucuronide Can Be Used as a Biomarker of Habitual Alcohol Consumption in the General Population. J. Nutr. 2019, 149, 2199–2205. [Google Scholar] [CrossRef] [Green Version]
- Duvivier, W.F.; van Putten, M.R.; van Beek, T.A.; Nielen, M.W. (Un)targeted Scanning of Locks of Hair for Drugs of Abuse by Direct Analysis in Real Time-High-Resolution Mass Spectrometry. Anal. Chem. 2016, 88, 2489–2496. [Google Scholar] [CrossRef]
- Klont, F.; Kremer, D.; Gomes Neto, A.W.; Berger, S.P.; Touw, D.J.; Hak, E.; Bonner, R.; Bakker, S.J.L.; Hopfgartner, G. Metabolomics data complemented drug use information in epidemiological databases: Pilot study of potential kidney donors. J. Clin. Epidemiol. 2021, 135, 10–16. [Google Scholar] [CrossRef]
- Suhre, K.; Stephan, N.; Zaghlool, S.; Triggle, C.R.; Robinson, R.J.; Evans, A.M.; Halama, A. Matching Drug Metabolites from Non-Targeted Metabolomics to Self-Reported Medication in the Qatar Biobank Study. Metabolites 2022, 12, 249. [Google Scholar] [CrossRef] [PubMed]
- Klont, F.; Stepanovic, S.; Kremer, D.; Bonner, R.; Touw, D.J.; Hak, E.; Bakker, S.J.L.; Hopfgartner, G. Untargeted ‘SWATH’ mass spectrometry-based metabolomics for studying chronic and intermittent exposure to xenobiotics in cohort studies. Food Chem. Toxicol. 2022, 165, 113188. [Google Scholar] [CrossRef]
- Van Tilborgh-de Jong, A.J.; Wiersum-Osselton, J.C.; Touw, D.J.; Schipperus, M.R. Presence of medication taken by blood donors in plasma for transfusion. Vox. Sang 2015, 108, 323–327. [Google Scholar] [CrossRef]
- Ernst, M.; Kang, K.B.; Caraballo-Rodriguez, A.M.; Nothias, L.F.; Wandy, J.; Chen, C.; Wang, M.; Rogers, S.; Medema, M.H.; Dorrestein, P.C.; et al. MolNetEnhancer: Enhanced Molecular Networks by Integrating Metabolome Mining and Annotation Tools. Metabolites 2019, 9, 144. [Google Scholar] [CrossRef] [Green Version]
- Eisenga, M.F.; Gomes-Neto, A.W.; van Londen, M.; Ziengs, A.L.; Douwes, R.M.; Stam, S.P.; Oste, M.C.J.; Knobbe, T.J.; Hessels, N.R.; Buunk, A.M.; et al. Rationale and design of TransplantLines: A prospective cohort study and biobank of solid organ transplant recipients. BMJ Open 2018, 8, e024502. [Google Scholar] [CrossRef] [PubMed]
- Sosnowski, P.; Hopfgartner, G. Application of 3D printed tools for customized open port probe-electrospray mass spectrometry. Talanta 2020, 215, 120894. [Google Scholar] [CrossRef] [PubMed]
- Broadhurst, D.; Goodacre, R.; Reinke, S.N.; Kuligowski, J.; Wilson, I.D.; Lewis, M.R.; Dunn, W.B. Guidelines and considerations for the use of system suitability and quality control samples in mass spectrometry assays applied in untargeted clinical metabolomic studies. Metabolomics 2018, 14, 72. [Google Scholar] [CrossRef] [Green Version]
- Bergan, S.; Brunet, M.; Hesselink, D.A.; Johnson-Davis, K.L.; Kunicki, P.K.; Lemaitre, F.; Marquet, P.; Molinaro, M.; Noceti, O.; Pattanaik, S.; et al. Personalized Therapy for Mycophenolate: Consensus Report by the International Association of Therapeutic Drug Monitoring and Clinical Toxicology. Ther. Drug Monit. 2021, 43, 150–200. [Google Scholar] [CrossRef]
- Bjarnason, I. Enteric coating of mycophenolate sodium: A rational approach to limit topical gastrointestinal lesions and extend the therapeutic index of mycophenolate. Transplant. Proc. 2001, 33, 3238–3240. [Google Scholar] [CrossRef]
- Martinez-Mier, G.; Salazar-Ramirez, A. The Cost of Gastrointestinal Adverse Events and the Impact of Dose-Reductions/Discontinuations on Acute Rejection in Kidney Transplant Patients of Mycophenolate Mofetil-Related Compared to Enteric-Coated Mycophenolate Sodium: A Pharmacoeconomic Study. Transpl. Proc. 2016, 48, 588–595. [Google Scholar] [CrossRef]
- Partani, P.; Verma, S.M.; Monif, T. Liquid chromatography tandem mass spectrometry method for the quantitation of mycophenolate mofetil in human plasma: Application to a bioequivalence study and metabolite identification. J. Sep. Sci. 2015, 38, 3533–3544. [Google Scholar] [CrossRef]
- Lamba, V.; Sangkuhl, K.; Sanghavi, K.; Fish, A.; Altman, R.B.; Klein, T.E. PharmGKB summary: Mycophenolic acid pathway. Pharm. Genom. 2014, 24, 73–79. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Zhang, D.; Ray, K.; Zhu, M. Mass defect filter technique and its applications to drug metabolite identification by high-resolution mass spectrometry. J. Mass Spectrom. 2009, 44, 999–1016. [Google Scholar] [CrossRef]
- Valente, M.J.; Carvalho, F.; Bastos, M.; de Pinho, P.G.; Carvalho, M. Contribution of oxidative metabolism to cocaine-induced liver and kidney damage. Curr. Med. Chem. 2012, 19, 5601–5606. [Google Scholar] [CrossRef]
- Gresnigt, F.M.J.; Gubbels, N.P.; Riezebos, R.K. The current practice for cocaine-associated chest pain in the Netherlands. Toxicol. Rep. 2021, 8, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Klont, F.; Jahn, S.; Grivet, C.; Konig, S.; Bonner, R.; Hopfgartner, G. SWATH data independent acquisition mass spectrometry for screening of xenobiotics in biological fluids: Opportunities and challenges for data processing. Talanta 2020, 211, 120747. [Google Scholar] [CrossRef] [PubMed]
- Broseus, J.; Gentile, N.; Bonadio Pont, F.; Garcia Gongora, J.M.; Gaste, L.; Esseiva, P. Qualitative, quantitative and temporal study of cutting agents for cocaine and heroin over 9 years. Forensic. Sci. Int. 2015, 257, 307–313. [Google Scholar] [CrossRef]
- Brunt, T.M.; Nagy, C.; Bucheli, A.; Martins, D.; Ugarte, M.; Beduwe, C.; Ventura Vilamala, M. Drug testing in Europe: Monitoring results of the Trans European Drug Information (TEDI) project. Drug Test Anal. 2017, 9, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Gatch, M.B.; Dolan, S.B.; Forster, M.J. Locomotor, discriminative stimulus, and place conditioning effects of MDAI in rodents. Behav. Pharmacol. 2016, 27, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Hondebrink, L.; Nugteren-van Lonkhuyzen, J.J.; Hunault, C.C.; van den Berg, J.; van der Gouwe, D.; van Riel, A. New psychoactive substances (NPS) in the Netherlands: Occurrence in forensic drug samples, consumer drug samples and poisons center exposures between 2013 and 2017. Addiction 2020, 115, 716–725. [Google Scholar] [CrossRef] [Green Version]
- Van Amsterdam, J.; Nutt, D.; van den Brink, W. Generic legislation of new psychoactive drugs. J. Psychopharmacol. 2013, 27, 317–324. [Google Scholar] [CrossRef]
- Casale, J.F.; Hays, P.A. Characterization of the “Methylenedioxy-2-aminoindans”. Microgram J. 2011, 8, 43–52. [Google Scholar]
- Strand, D.S.; Kim, D.; Peura, D.A. 25 Years of Proton Pump Inhibitors: A Comprehensive Review. Gut Liver 2017, 11, 27–37. [Google Scholar] [CrossRef]
- Olbe, L.; Carlsson, E.; Lindberg, P. A proton-pump inhibitor expedition: The case histories of omeprazole and esomeprazole. Nat. Rev. Drug Discov. 2003, 2, 132–139. [Google Scholar] [CrossRef]
- Abelo, A.; Andersson, T.B.; Antonsson, M.; Naudot, A.K.; Skanberg, I.; Weidolf, L. Stereoselective metabolism of omeprazole by human cytochrome P450 enzymes. Drug Metab. Dispos. 2000, 28, 966–972. [Google Scholar]
- Oosterhuis, B.; Jonkman, J.H. Omeprazole: Pharmacology, pharmacokinetics and interactions. Digestion 1989, 44 (Suppl. S1), 9–17. [Google Scholar] [CrossRef]
- Bahar, M.A.; Lanting, P.; Bos, J.H.J.; Sijmons, R.H.; Hak, E.; Wilffert, B. Impact of Drug-Gene-Interaction, Drug-Drug-Interaction, and Drug-Drug-Gene-Interaction on (es)Citalopram Therapy: The PharmLines Initiative. J. Pers. Med. 2020, 10, 256. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Database-Derived Drug Use | ||||
|---|---|---|---|---|
| Non-User | Omeprazole | Esomeprazole | Total | |
| Liver transplant recipients: | 196 (62%) | 77 (24%) | 43 (14%) | 316 |
| 0 metabolite signals | 184 1 | 7 | 3 | 194 (61%) |
| 1–2 metabolite signals | 2 | 2 | 1 | 5 (2%) |
| ≥3 metabolite signals | 10 | 68 2 | 39 2 | 117 (37%) |
| Kidney transplant recipients: | 214 (38%) | 316 (56%) | 39 (7%) | 569 |
| 0 metabolite signals | 198 1 | 16 | 2 | 216 (38%) |
| 1–2 metabolite signals | 3 | 9 | 1 | 13 (2%) |
| ≥3 metabolite signals | 13 | 291 2 | 36 2 | 340 (60%) |
| m/z | Possible Biotransformation(s) | Possible Signals |
|---|---|---|
| 268 | various (cysteine metabolite) | 1 |
| 310 | various (mercapturate metabolite) | 1 |
| 316 | dehydroxylation (−16), demethylation (−14) | 2 |
| 330 | dehydroxylation (−16) | 1 |
| 332 | demethylation (−14) | 2 |
| 346 | none (omeprazole) | not detected |
| 360 | dehydroxylation (−16), carboxylation (+30) | 2 |
| 362 | hydroxylation (+16) | 3 |
| 376 | carboxylation (+30) | 3 |
| 378 | dihydroxylation (+32) | 5 |
| 392 | hydroxylation (+16), carboxylation (+30) | 1 |
| 492 | dehydroxylation (−16), demethylation (−14), glucuronidation (+176) | 4 |
| 506 | dehydroxylation (−16), glucuronidation (+176) | 2 |
| 508 | demethylation (−14), glucuronidation (+176) | 8 |
| 522 | glucuronidation (+176) | 7 |
| 536 | dehydroxylation (−16), carboxylation (+30), glucuronidation (+176) | 1 |
| 538 | hydroxylation (+16), glucuronidation (+176) | 5 |
| 552 | carboxylation (+30), glucuronidation (+176) | 1 |
| 554 | dihydroxylation (+32), glucuronidation (+176) | 2 |
| m/z | 332 | 360 | 362 | 376 | 378 | 392 | ||
|---|---|---|---|---|---|---|---|---|
| RT (min) | 7.9 | 8.3 | 10.3 | 7.2 | 7.7 | 8.5 | ||
| 332 | 7.9 | 1.4 × 10−4 | 1.2 × 10−8 | 0.18 | 1.4 × 10−4 | 3.9 × 10−10 | KTR | |
| 360 | 8.3 | 0.54 | 4.7 × 10−11 | 0.03 | 0.06 | 2.7 × 10−17 | ||
| 362 | 10.3 | 1.8 × 10−4 | 6.3 × 10−5 | 1.5 × 10−9 | 1.9 × 10−12 | 0.05 | ||
| 376 | 7.2 | 0.95 | 0.61 | 2.2 × 10−4 | 0.013 | 2.8 × 10−15 | ||
| 378 | 7.7 | 3.2 × 10−3 | 3.2 × 10−3 | 3.8 × 10−6 | 0.01 | 4.5 × 10−11 | ||
| 392 | 8.5 | 3.5 × 10−6 | 8.1 × 10−7 | 0.06 | 6.2 × 10−6 | 1.2 × 10−6 | ||
| LTR | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klont, F.; Sosnowski, P.; Kremer, D.; Knobbe, T.J.; Bonner, R.; Blokzijl, H.; Weersma, R.K.; Bakker, S.J.L.; Investigators, T.; Hak, E.; et al. Assessing the Potential of Untargeted SWATH Mass Spectrometry-Based Metabolomics to Differentiate Closely Related Exposures in Observational Studies. Metabolites 2022, 12, 942. https://doi.org/10.3390/metabo12100942
Klont F, Sosnowski P, Kremer D, Knobbe TJ, Bonner R, Blokzijl H, Weersma RK, Bakker SJL, Investigators T, Hak E, et al. Assessing the Potential of Untargeted SWATH Mass Spectrometry-Based Metabolomics to Differentiate Closely Related Exposures in Observational Studies. Metabolites. 2022; 12(10):942. https://doi.org/10.3390/metabo12100942
Chicago/Turabian StyleKlont, Frank, Piotr Sosnowski, Daan Kremer, Tim J. Knobbe, Ron Bonner, Hans Blokzijl, Rinse K. Weersma, Stephan J. L. Bakker, TransplantLines Investigators, Eelko Hak, and et al. 2022. "Assessing the Potential of Untargeted SWATH Mass Spectrometry-Based Metabolomics to Differentiate Closely Related Exposures in Observational Studies" Metabolites 12, no. 10: 942. https://doi.org/10.3390/metabo12100942