A Wireless Body Sensor Network for Clinical Assessment of the Flexion-Relaxation Phenomenon

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
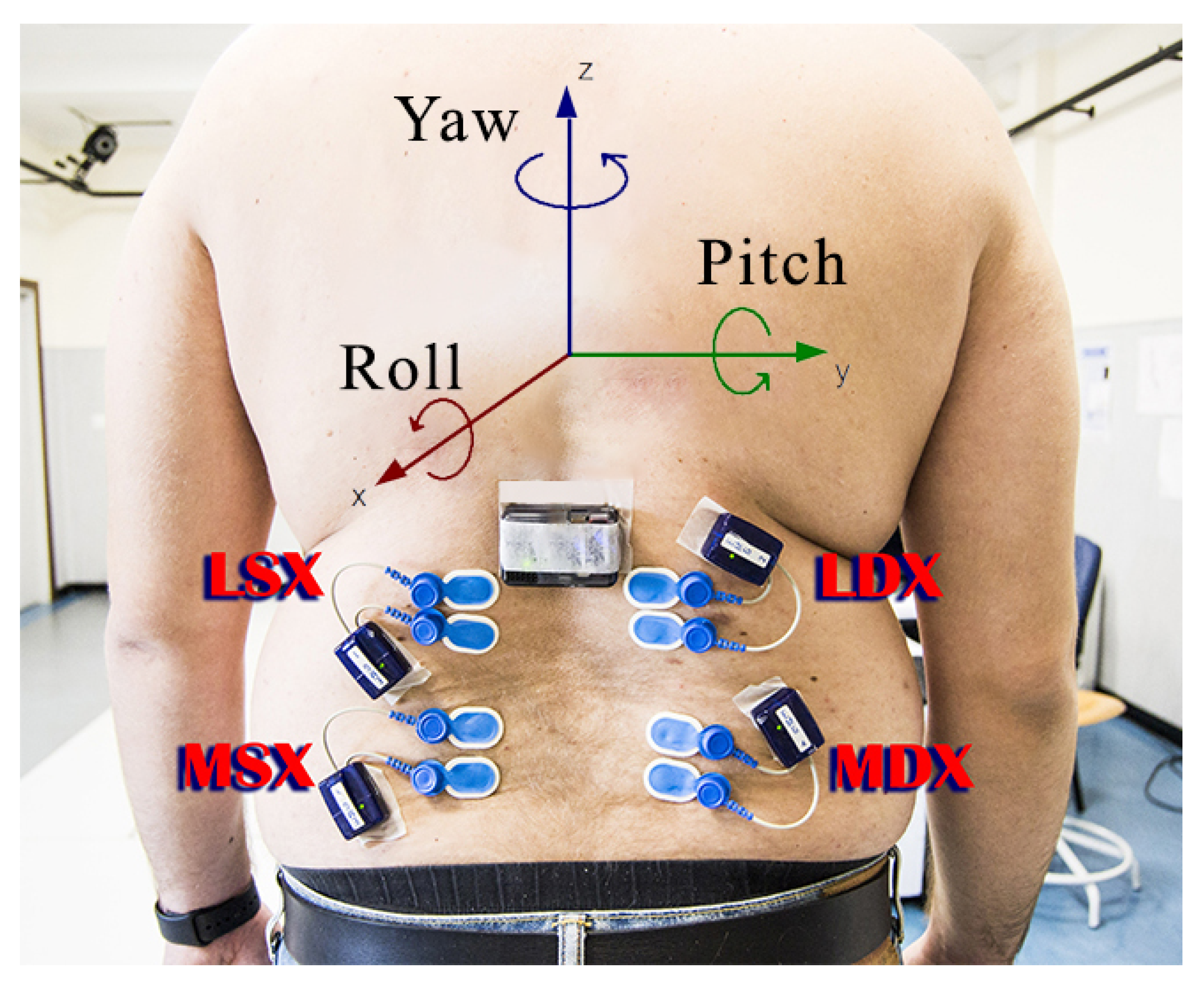
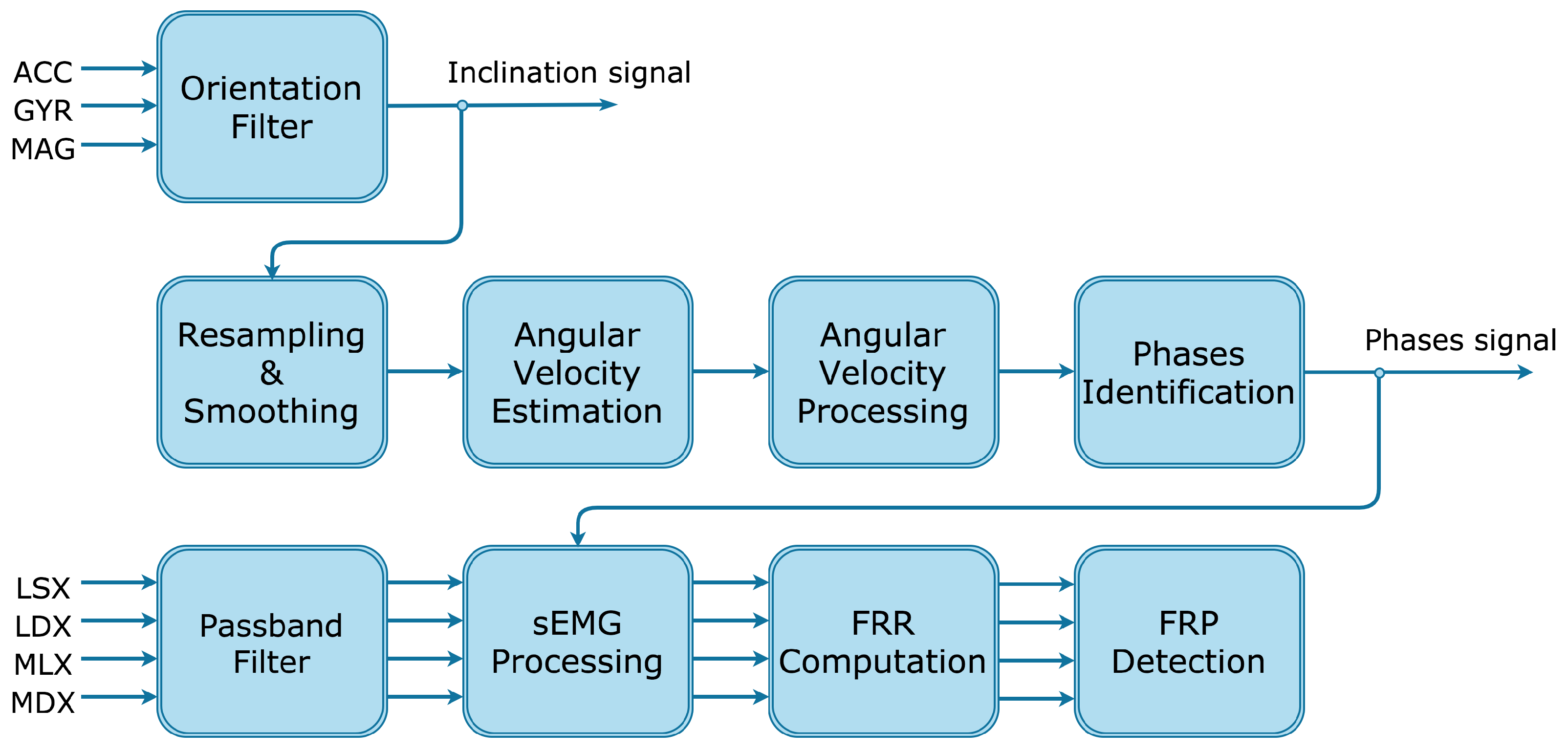
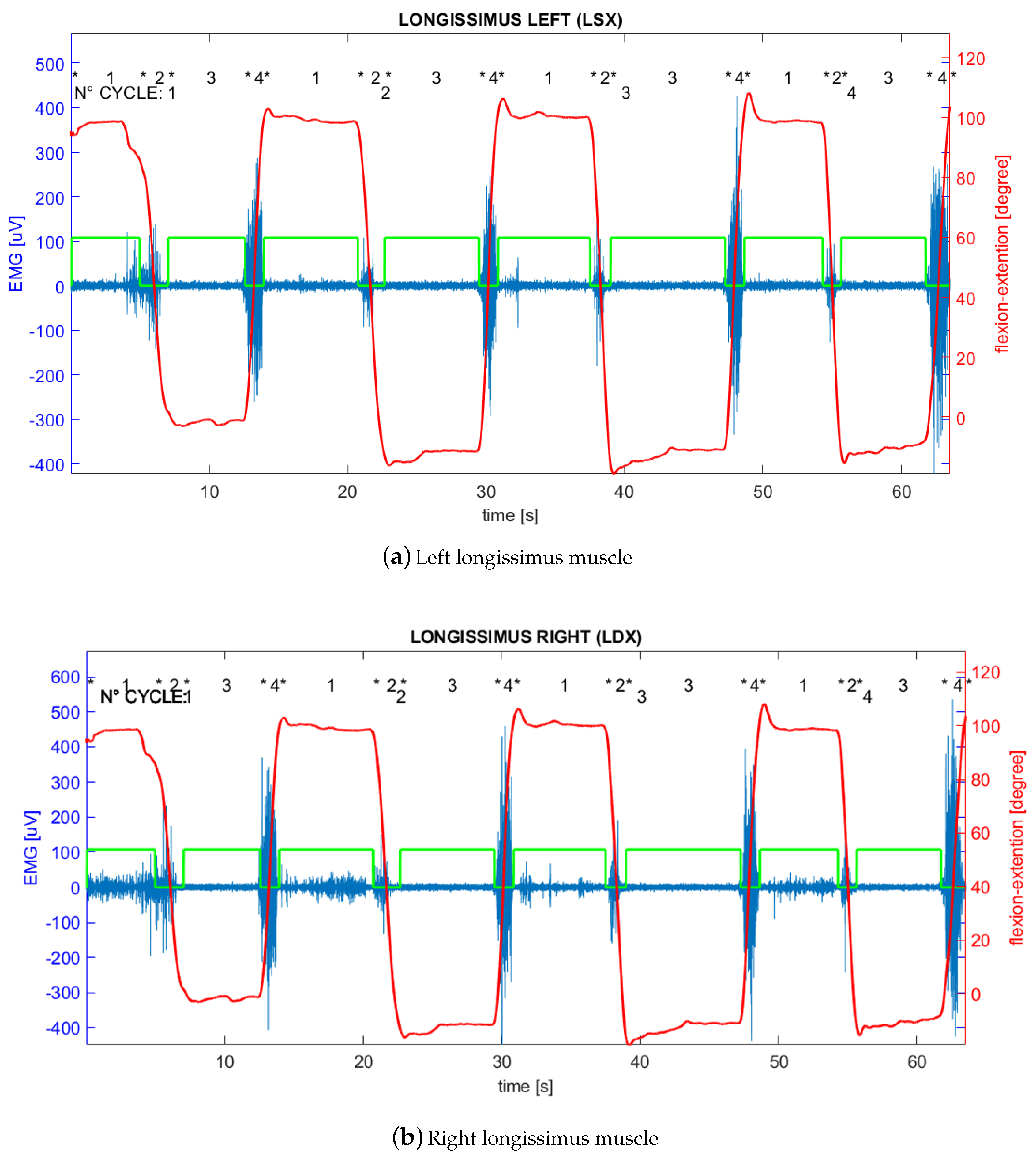
- Electromyography signal on left longissimus channel (LSX);
- Electromyography signal on right longissimus channel (LDX);
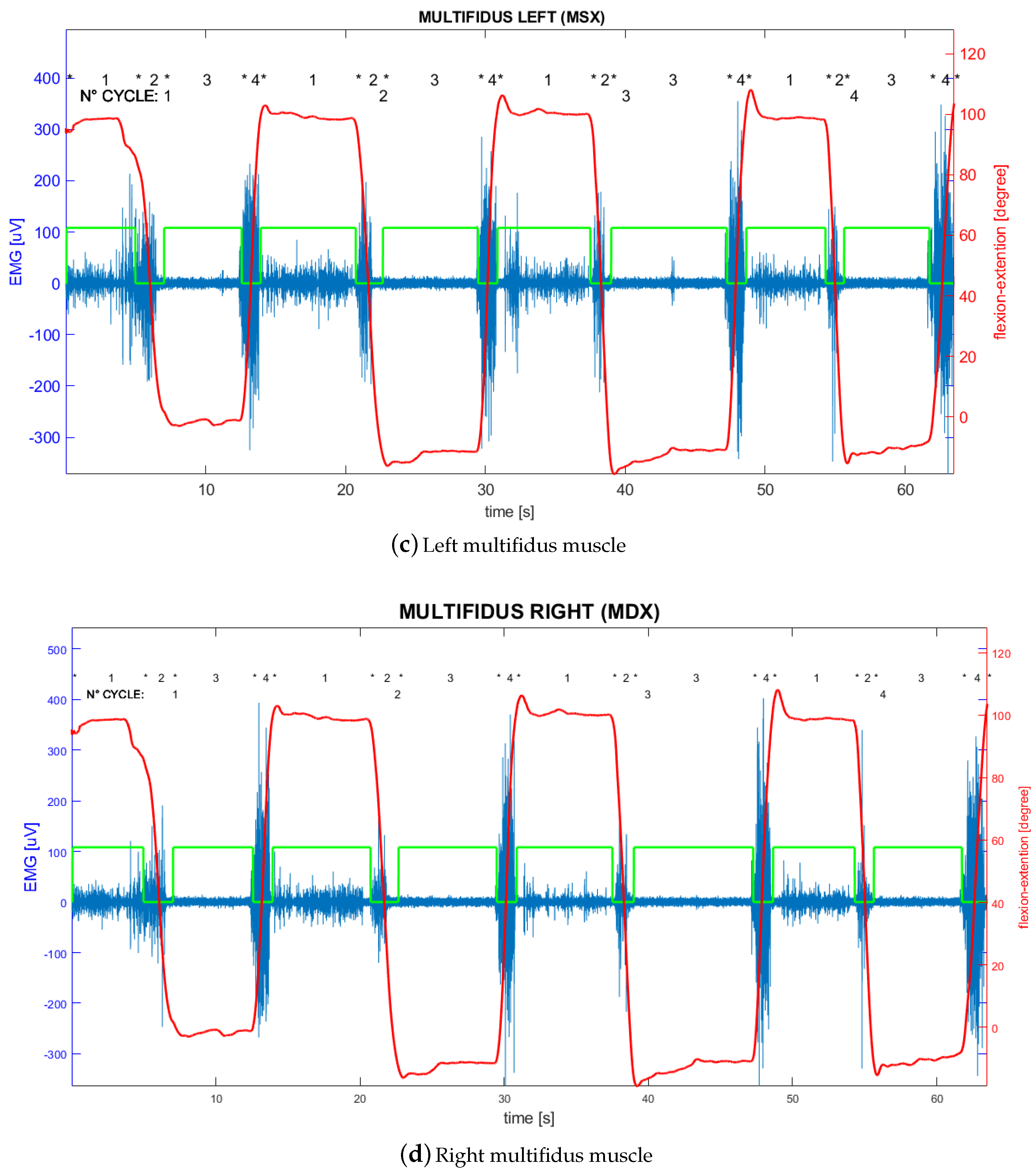
- Electromyography signal on left multifidus channel (MSX);
- Electromyography signal on right multifidus channel (MDX).
- Acceleration measured by the accelerometer (ACC);
- Angular velocity measured by the gyroscope (GYR);
- Magnetic field measured by the magnetometer (MAG).
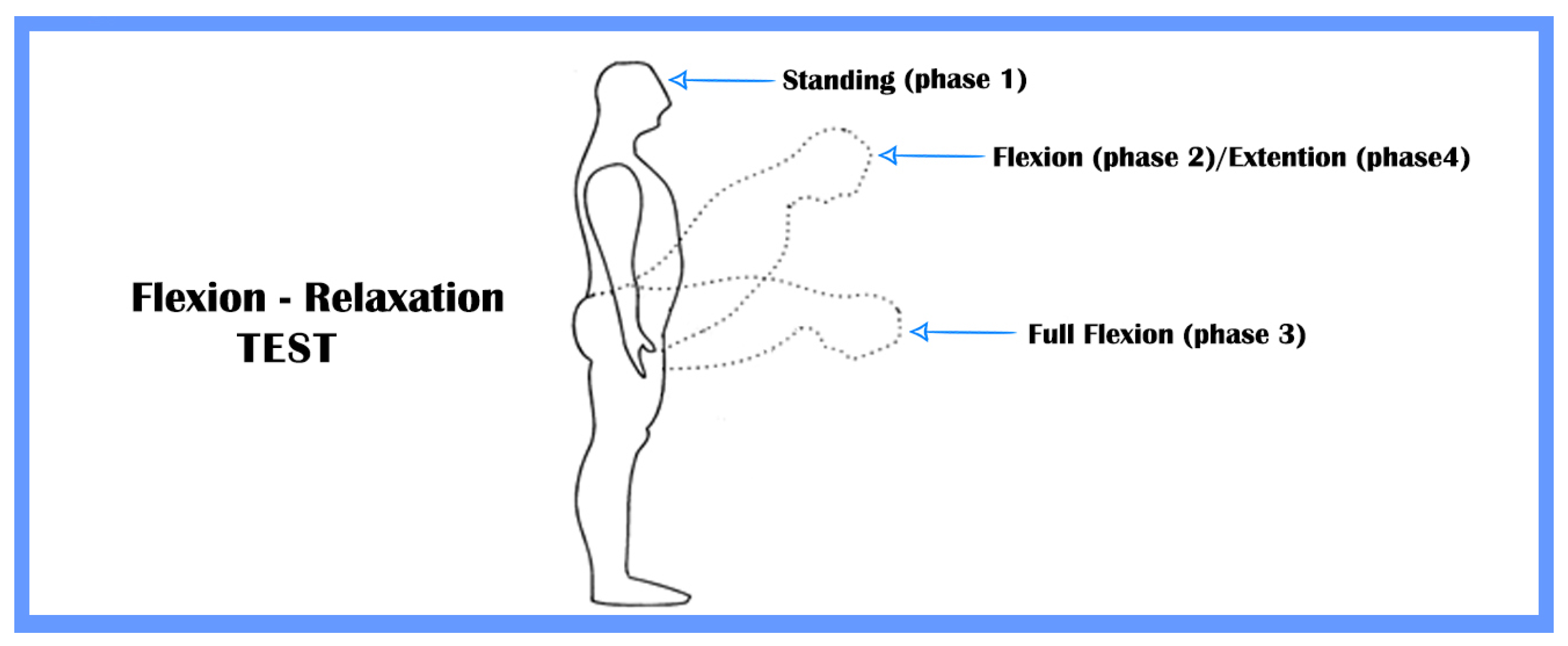
- Standing—The subject keeps the standing position for about 4 s;
- Flexion—The subject bend forward in order to naturally reach the full flexion position;
- Full flexion—The subject keeps the full flexion position for about 4 s;
- Extension—The subject return to standing position.
3. Algorithm for FRP Clinical Assessment
- i = i-th cycle;
- j = j-th sample in full-flexion phase;
- k = k-th sample in extension phase;
- n = total samples in full-flexion phase;
- m = total samples in extension phase;
- sEMGi(t) = represents the total signal filtered and synchronized in the i-th cycle, where t is a discrete-time variable multiple of the sample time;
- sEMGj = represents the j-th amplitude of the sEMG signal (filtered and synchronized) in full flexion phase;
- sEMGk = represents the k-th amplitude of the sEMG signal (filtered and synchronized) in extension phase;
- C = type of Channel (LSX, LDX, MSX, MDX).
4. Results
- True Positive (TP)—The algorithm correctly reported FRP presence in an event with a positive outcome;
- False Positive (FP)—The algorithm incorrectly reported FRP presence in an event with a negative outcome;
- True Negative (TN)—The algorithm correctly reported FRP absence in an event with a negative outcome;
- False Negative (FN)—The algorithm incorrectly reported FRP absence in an event with a positive outcome.
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ACC | Acceleration |
| BSN | Body Sensor Network |
| ECG | Electrocardiogram |
| FN | False Negative |
| FP | False Positive |
| FER | Flexion Extension Ratio |
| FRP | Flexion Relaxation Phenomenon |
| FRR (or plural FRRs) | Flexion Relaxation Ratio (s) |
| GYR | Gyroscope |
| ID | Identification Number |
| LBP | Low Back Pain |
| LDX | Longissimus Right |
| LSX | Longissimus Left |
| MAG | Magnetic field |
| MDX | Multifidus Right |
| MSX | Multifidus Left |
| NRS-11 | Numeric Rating Scale |
| RMS | Root Mean Square |
| sEMG | Surface Electromyography |
| TP | True Positive |
| TN | True Negative |
| VIS | Visual Inspection |
| WBSN | Wireless Body Sensor Network |
References
- Floyd, W.; Silver, P. The function of the erectores spinae muscles in certain movements and postures in man. J. Physiol. 1955, 129, 184–203. [Google Scholar] [CrossRef] [PubMed]
- McGill, S.M.; Kippers, V. Transfer of loads between lumbar tissues during the flexion-relaxation phenomenon. Spine 1994, 19, 2190–2196. [Google Scholar] [CrossRef] [PubMed]
- Andersson, E.; Oddsson, L.; Grundström, H.; Nilsson, J.; Thorstensson, A. EMG activities of the quadratus lumborum and erector spinae muscles during flexion-relaxation and other motor tasks. Clin. Biomech. 1996, 11, 392–400. [Google Scholar] [CrossRef]
- Hodges, P.W.; Moseley, G.L. Pain and motor control of the lumbopelvic region: Effect and possible mechanisms. J. Electromyogr. Kinesiol. 2003, 13, 361–370. [Google Scholar] [CrossRef]
- Hodges, P.W.; Tucker, K. Moving differently in pain: A new theory to explain the adaptation to pain. Pain 2011, 152, S90–S98. [Google Scholar] [CrossRef]
- Van Dieën, J.H.; Selen, L.P.; Cholewicki, J. Trunk muscle activation in low-back pain patients, an analysis of the literature. J. Electromyogr. Kinesiol. 2003, 13, 333–351. [Google Scholar] [CrossRef]
- Golding, J. Electromyography of the erector spinae in low back pain. Postgrad. Med. J. 1952, 28, 401. [Google Scholar] [CrossRef] [Green Version]
- Bhms, V.K.; Parker, A. Posture related to myoelectric silence of erectores spinae during trunk flexion. Spine 1984, 9, 740. [Google Scholar]
- Sarti, M.; Lison, J.; Monfort, M.; Fuster, M. Response of the flexion–relaxation phenomenon relative to the lumbar motion to load and speed. Spine 2001, 26, E421–E426. [Google Scholar] [CrossRef] [PubMed]
- Watson, P.J.; Booker, C.; Main, C.; Chen, A. Surface electromyography in the identification of chronic low back pain patients: The development of the flexion relaxation ratio. Clin. Biomech. 1997, 12, 165–171. [Google Scholar] [CrossRef]
- Sihvonen, T.; Partanen, J.; Hänninen, O.; Soimakallio, S. Electric behavior of low back muscles during lumbar pelvic rhythm in low back pain patients and healthy controls. Arch. Phys. Med. Rehabil. 1991, 72, 1080–1087. [Google Scholar] [PubMed]
- McGorry, R.W.; Lin, J.H. Flexion relaxation and its relation to pain and function over the duration of a back pain episode. PLoS ONE 2012, 7, e39207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neblett, R. Surface electromyographic (SEMG) biofeedback for chronic low back pain. Healthcare 2016, 4, 27. [Google Scholar] [CrossRef] [Green Version]
- Othman, S.H.; Ibrahim, F.; Omar, S.; Rahim, R. Flexion relaxation phenomenon of back muscles in discriminating between healthy and chronic low back pain women. In Proceedings of the 4th Kuala Lumpur International Conference on Biomedical Engineering 2008, Kuala Lumpur, Malaysia, 25–28 June 2008; pp. 199–203. [Google Scholar]
- Alschuler, K.N.; Neblett, R.; Wiggert, E.; Haig, A.J.; Geisser, M.E. Flexion-relaxation and clinical features associated with chronic low back pain: A comparison of different methods of quantifying flexion-relaxation. Clin. J. Pain 2009, 25, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Geisser, M.E.; Ranavaya, M.; Haig, A.J.; Roth, R.S.; Zucker, R.; Ambroz, C.; Caruso, M. A meta-analytic review of surface electromyography among persons with low back pain and normal, healthy controls. J. Pain 2005, 6, 711–726. [Google Scholar] [CrossRef] [PubMed]
- Neblett, R.; Mayer, T.G.; Gatchel, R.J.; Proctor, T. Quantifying lumbar flexion-relaxation phenomenon: Theory and clinical applications. Spine J. 2002, 2, 97. [Google Scholar] [CrossRef]
- Schinkel-Ivy, A.; Nairn, B.C.; Drake, J.D. Quantification of the lumbar flexion-relaxation phenomenon: Comparing outcomes of lumbar erector spinae and superficial lumbar multifidus in standing full trunk flexion and slumped sitting postures. J. Manip. Physiol. Ther. 2014, 37, 494–501. [Google Scholar] [CrossRef]
- Jin, S.; Ning, X.; Mirka, G.A. An algorithm for defining the onset and cessation of the flexion-relaxation phenomenon in the low back musculature. J. Electromyogr. Kinesiol. 2012, 22, 376–382. [Google Scholar] [CrossRef] [Green Version]
- Schinkel-Ivy, A.; Nairn, B.C.; Drake, J.D. Evaluation of methods for the quantification of the flexion-relaxation phenomenon in the lumbar erector spinae muscles. J. Manip. Physiol. Ther. 2013, 36, 349–358. [Google Scholar] [CrossRef]
- Nougarou, F.; Massicotte, D.; Descarreaux, M. Detection method of flexion relaxation phenomenon based on wavelets for patients with low back pain. EURASIP J. Adv. Signal Process. 2012, 2012, 151. [Google Scholar] [CrossRef] [Green Version]
- Ritvanen, T.; Zaproudina, N.; Nissen, M.; Leinonen, V.; Hänninen, O. Dynamic surface electromyographic responses in chronic low back pain treated by traditional bone setting and conventional physical therapy. J. Manip. Physiol. Ther. 2007, 30, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Sihvonen, T. Flexion relaxation of the hamstring muscles during lumbar-pelvic rhythm. Arch. Phys. Med. Rehabil. 1997, 78, 486–490. [Google Scholar] [CrossRef]
- CARLSÖÖ, S. The static muscle load in different work positions: An electromyographic study. Ergonomics 1961, 4, 193–211. [Google Scholar] [CrossRef]
- Mayer, T.; Tencer, A.F.; Kristoferson, S.; Mooney, V. Use of noninvasive techniques for quantification of spinal range-of-motion in normal subjects and chronic low-back dysfunction patients. Spine 1984, 9, 588–595. [Google Scholar] [CrossRef]
- Mayer, T.G.; Neblett, R.; Brede, E.; Gatchel, R.J. The quantified lumbar flexion-relaxation phenomenon is a useful measurement of improvement in a functional restoration program. Spine 2009, 34, 2458–2465. [Google Scholar] [CrossRef]
- Leardini, A.; Biagi, F.; Belvedere, C.; Benedetti, M.G. Quantitative comparison of current models for trunk motion in human movement analysis. Clin. Biomech. 2009, 24, 542–550. [Google Scholar] [CrossRef]
- Solomonow, M.; Baratta, R.V.; Banks, A.; Freudenberger, C.; Zhou, B.H. Flexion–relaxation response to static lumbar flexion in males and females. Clin. Biomech. 2003, 18, 273–279. [Google Scholar] [CrossRef]
- Chen, Y.L.; Chen, Y.; Lin, W.C.; Liao, Y.H.; Lin, C.J. Lumbar posture and individual flexibility influence back muscle flexion-relaxation phenomenon while sitting. Int. J. Ind. Ergon. 2019, 74, 102840. [Google Scholar] [CrossRef]
- Roghani, T.; Zavieh, M.K.; Talebian, S.; Baghban, A.A.; Katzman, W. Back Muscle Function in Older Women With Age-Related Hyperkyphosis: A Comparative Study. J. Manip. Physiol. Ther. 2019, 42, 284–294. [Google Scholar] [CrossRef]
- Goodvin, C.; Park, E.J.; Huang, K.; Sakaki, K. Development of a real-time three-dimensional spinal motion measurement system for clinical practice. Med Biol. Eng. Comput. 2006, 44, 1061–1075. [Google Scholar] [CrossRef]
- Wong, W.Y.; Wong, M.S. Trunk posture monitoring with inertial sensors. Eur. Spine J. 2008, 17, 743–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronchi, A.J.; Lech, M.; Taylor, N.; Cosic, I. A reliability study of the new Back Strain Monitor based on clinical trials. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–24 August 2008; pp. 693–696. [Google Scholar]
- Valencia-Jimenez, N.; Leal-Junior, A.; Avellar, L.; Vargas-Valencia, L.; Caicedo-Rodríguez, P.; Ramírez-Duque, A.A.; Lyra, M.; Marques, C.; Bastos, T.; Frizera, A. A Comparative Study of Markerless Systems Based on Color-Depth Cameras, Polymer Optical Fiber Curvature Sensors, and Inertial Measurement Units: Towards Increasing the Accuracy in Joint Angle Estimation. Electronics 2019, 8, 173. [Google Scholar] [CrossRef] [Green Version]
- Mjøsund, H.L.; Boyle, E.; Kjaer, P.; Mieritz, R.M.; Skallgård, T.; Kent, P. Clinically acceptable agreement between the ViMove wireless motion sensor system and the Vicon motion capture system when measuring lumbar region inclination motion in the sagittal and coronal planes. BMC Musculoskelet. Disord. 2017, 18, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, P.; Saini, R.; Tumma, C.S.; Roy, P.P.; Dogra, D.P. Gait Analysis Using Shadow Motion. In Proceedings of the 2017 4th IAPR Asian Conference on Pattern Recognition (ACPR), Nanjing, China, 26–29 November 2017; pp. 453–458. [Google Scholar]
- Kumar, P.; Mukherjee, S.; Saini, R.; Kaushik, P.; Roy, P.P.; Dogra, D.P. Multimodal gait recognition with inertial sensor data and video using evolutionary algorithm. IEEE Trans. Fuzzy Syst. 2018, 27, 956–965. [Google Scholar] [CrossRef]
- Bergmann, J.H.; Chandaria, V.; McGregor, A. Wearable and implantable sensors: The patient’s perspective. Sensors 2012, 12, 16695–16709. [Google Scholar] [CrossRef] [Green Version]
- Mokhlespour Esfahani, M.I.; Nussbaum, M.A. Preferred placement and usability of a smart textile system vs. inertial measurement units for activity monitoring. Sensors 2018, 18, 2501. [Google Scholar] [CrossRef] [Green Version]
- Rose-Dulcina, K.; Genevay, S.; Dominguez, D.; Armand, S.; Vuillerme, N. Flexion-Relaxation Ratio Asymmetry and Its Relation With Trunk Lateral ROM in Individuals With and Without Chronic Nonspecific Low Back Pain. Spine 2020, 45, E1–E9. [Google Scholar] [CrossRef]
- Carrillo-Perez, F.; Diaz-Reyes, I.; Damas, M.; Banos, O.; Soto-Hermoso, V.M.; Molina-Molina, A. A Novel Automated Algorithm for Computing Lumbar Flexion Test Ratios Enhancing Athletes Objective Assessment of Low Back Pain. In Proceedings of the 2018 6th International Congress on Sport Sciences Research and Technology Support, Seville, Spain, 20–21 September 2018; pp. 34–39. [Google Scholar]
- Laird, R.A.; Keating, J.L.; Ussing, K.; Li, P.; Kent, P. Does movement matter in people with back pain? Investigating ‘atypical’ lumbo-pelvic kinematics in people with and without back pain using wireless movement sensors. BMC Musculoskelet. Disord. 2019, 20, 28. [Google Scholar] [CrossRef] [Green Version]
- Paoletti, M.; Belli, A.; Palma, L.; Paniccia, M.; Tombolini, F.; Ruggiero, A.; Vallasciani, M.; Pierleoni, P. Data acquired by wearable sensors for the evaluation of the flexion-relaxation phenomenon. Data Brief 2020. under review. [Google Scholar]
- Morbidoni, C.; Cucchiarelli, A.; Fioretti, S.; Di Nardo, F. A deep learning approach to EMG-based classification of gait phases during level ground walking. Electronics 2019, 8, 894. [Google Scholar] [CrossRef] [Green Version]
- Hermens, H.J.; Freriks, B.; Merletti, R.; Stegeman, D.; Blok, J.; Rau, G.; Disselhorst-Klug, C.; Hägg, G. European recommendations for surface electromyography. Roessingh Res. Dev. 1999, 8, 13–54. [Google Scholar]
- Li, Z.; Guan, X.; Zou, K.; Xu, C. Estimation of Knee Movement from Surface EMG Using Random Forest with Principal Component Analysis. Electronics 2020, 9, 43. [Google Scholar] [CrossRef] [Green Version]
- Acar, G.; Ozturk, O.; Golparvar, A.J.; Elboshra, T.A.; Böhringer, K.; Yapici, M.K. Wearable and flexible textile electrodes for biopotential signal monitoring: A review. Electronics 2019, 8, 479. [Google Scholar] [CrossRef] [Green Version]
- Hartrick, C.T.; Kovan, J.P.; Shapiro, S. The numeric rating scale for clinical pain measurement: A ratio measure? Pain Pract. 2003, 3, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Tesio, L.; Granger, C.V.; Fiedler, R.C. A unidimensional pain/disability measure for low-back pain syndromes. Pain 1997, 69, 269–278. [Google Scholar] [CrossRef]
- Madgwick, S.O.; Harrison, A.J.; Vaidyanathan, R. Estimation of IMU and MARG orientation using a gradient descent algorithm. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011; pp. 1–7. [Google Scholar]
- Pierleoni, P.; Belli, A.; Palma, L.; Pernini, L.; Valenti, S. An accurate device for real-time altitude estimation using data fusion algorithms. In Proceedings of the 2014 IEEE/ASME 10th International Conference on Mechatronic and Embedded Systems and Applications (MESA), Ancona, Italy, 10–12 September 2014; pp. 1–5. [Google Scholar]
- Sabatini, A.M. Estimating three-dimensional orientation of human body parts by inertial/magnetic sensing. Sensors 2011, 11, 1489–1525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redfern, M.S.; Hughes, R.E.; Chaffin, D.B. High-pass filtering to remove electrocardiographic interference from torso EMG recordings. Clin. Biomech. 1993, 8, 44–48. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Zuriaga, D.; López-Pascual, J.; Garrido-Jaén, D.; García-Mas, M.A. A comparison of lumbopelvic motion patterns and erector spinae behavior between asymptomatic subjects and patients with recurrent low back pain during pain-free periods. J. Manip. Physiol. Ther. 2015, 38, 130–137. [Google Scholar] [CrossRef]
- Fernandes, W.V.B.; Blanco, C.R.; Politti, F.; de Cordoba Lanza, F.; Lucareli, P.R.G.; Corrêa, J.C.F. The effect of a six-week osteopathic visceral manipulation in patients with non-specific chronic low back pain and functional constipation: study protocol for a randomized controlled trial. Trials 2018, 19, 151. [Google Scholar] [CrossRef]
- Descarreaux, M.; Lafond, D.; Jeffrey-Gauthier, R.; Centomo, H.; Cantin, V. Changes in the flexion relaxation response induced by lumbar muscle fatigue. BMC Musculoskelet. Disord. 2008, 9, 10. [Google Scholar] [CrossRef] [Green Version]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject ID | SEX | AGE | GROUP | LSX | LDX | MSX | MDX | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 | ||||
| 1 | F | 51 | LBP | P | P | P | P | P | P | P | P | P | P | P | P | P | P | P | P |
| 2 | F | 40 | HEALTHY | P | P | P | P | P | P | P | P | P | P | P | P | P | P | P | P |
| 3 | F | 34 | HEALTHY | P | P | P | P | P | P | P | P | P | P | P | P | P | P | P | P |
| 4 | M | 57 | LBP | N | P | P | P | N | P | P | P | N | N | N | N | N | N | P | P |
| 5 | M | 30 | LBP | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N |
| 6 | M | 31 | HEALTHY | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N |
| 7 | M | 35 | HEALTHY | P | P | P | P | P | P | P | P | N | P | P | P | P | P | P | P |
| 8 | M | 25 | HEALTHY | P | P | P | P | P | P | P | P | P | P | P | P | P | P | P | P |
| 9 | M | 58 | LBP | N | P | P | P | N | P | P | P | N | N | N | P | N | N | N | N |
| 10 | F | 52 | LBP | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N |
| 11 | F | 46 | LBP | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N |
| 12 | F | 40 | HEALTHY | P | P | P | P | P | P | P | P | P | P | P | P | P | P | P | P |
| 13 | M | 49 | LBP | N | N | N | N | P | P | P | P | N | N | N | N | N | N | N | N |
| 14 | F | 49 | LBP | P | P | P | P | P | P | P | P | N | N | N | N | N | N | N | N |
| 15 | F | 51 | LBP | N | P | P | P | N | P | P | P | N | N | N | N | N | N | N | N |
| 16 | F | 60 | HEALTHY | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N |
| 17 | F | 36 | HEALTHY | P | P | P | P | P | P | P | P | P | P | P | P | P | P | P | P |
| 18 | M | 22 | HEALTHY | P | P | P | P | P | P | P | P | P | P | P | P | P | P | P | P |
| 19 | M | 52 | LBP | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N |
| 20 | F | 22 | HEALTHY | P | P | P | P | P | P | P | P | P | P | P | P | P | P | P | P |
| 21 | M | 60 | HEALTHY | P | P | P | P | P | P | P | P | P | P | P | P | P | P | P | P |
| 22 | F | 51 | HEALTHY | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N |
| 23 | M | 60 | LBP | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N | N |
| 24 | M | 61 | LBP | N | N | N | N | N | N | N | N | N | N | N | N | N | N | P | P |
| 25 | M | 52 | HEALTHY | P | P | P | P | N | N | N | N | N | N | N | N | N | N | N | N |
| Subject ID | LSX | LDX | MSX | MDX | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 | 1 | 2 | 3 | 4 | |
| 1 | TP-0.07 | TP-0.07 | TP-0.07 | TP-0.07 | TP-0.08 | TP-0.08 | TP-0.08 | TP-0.08 | TP-0.09 | TP-0.07 | TP-0.08 | TP-0.08 | TP-0.08 | TP-0.08 | TP-0.08 | TP-0.08 |
| 2 | TP-0.08 | TP-0.08 | TP-0.08 | TP-0.09 | TP-0.08 | TP-0.08 | TP-0.11 | TP-0.06 | TP-0.08 | TP-0.07 | TP-0.08 | TP-0.07 | TP-0.09 | TP-0.09 | TP-0.09 | TP-0.08 |
| 3 | TP-0.06 | TP-0.07 | TP-0.06 | TP-0.05 | TP-0.05 | TP-0.05 | TP-0.05 | TP-0.04 | TP-0.07 | TP-0.08 | TP-0.07 | TP-0.07 | TP-0.06 | TP-0.06 | TP-0.05 | TP-0.06 |
| 4 | TN-0.47 | TP-0.20 | TP-0.15 | TP-0.18 | TN-0.36 | TP-0.14 | TP-0.10 | TP-0.11 | TN-0.67 | TN-0.37 | FP-0.26 | FP-0.20 | TN-0.83 | FP-0.32 | TP-0.18 | TP-0.17 |
| 5 | TN-0.71 | TN-0.58 | TN-0.50 | TN-0.35 | TN-0.79 | TN-0.65 | TN-0.57 | TN-0.37 | TN-0.67 | TN-0.61 | TN-0.55 | TN-0.36 | TN-0.81 | TN-0.74 | TN-0.68 | TN-0.41 |
| 6 | TN-0.61 | TN-0.58 | TN-0.89 | TN-0.63 | TN-0.59 | TN-0.51 | TN-0.84 | TN-0.69 | TN-0.43 | TN-0.36 | TN-0.67 | TN-0.49 | TN-0.35 | FP-0.33 | TN-0.48 | TN-0.35 |
| 7 | TP-0.19 | TP-0.15 | TP-0.13 | TP-0.13 | TP-0.21 | TP-0.19 | TP-0.16 | TP-0.20 | TN-0.38 | TP-0.28 | TP-0.24 | TP-0.21 | TP-0.33 | TP-0.28 | TP-0.26 | TP-0.28 |
| 8 | TP-0.08 | TP-0.08 | TP-0.10 | TP-0.08 | TP-0.17 | TP-0.14 | TP-0.18 | TP-0.16 | TP-0.10 | TP-0.10 | TP-0.12 | TP-0.10 | TP-0.14 | TP-0.13 | TP-0.15 | TP-0.15 |
| 9 | FP-0.18 | TP-0.13 | TP-0.11 | TP-0.14 | FP-0.25 | TP-0.16 | TP-0.13 | TP-0.17 | TN-0.58 | TN-0.40 | TN-0.36 | TP-0.30 | TN-0.54 | TN-0.42 | TN-0.42 | TN-0.35 |
| 10 | TN-0.74 | TN-0.84 | TN-0.85 | TN-1.27 | TN-0.65 | TN-0.91 | TN-0.92 | TN-1.25 | TN-0.88 | TN-0.90 | TN-0.79 | TN-1.16 | TN-0.73 | TN-0.91 | TN-0.78 | TN-1.11 |
| 11 | TN-0.97 | TN-1.34 | TN-0.76 | TN-0.42 | TN-1.07 | TN-1.11 | TN-1.00 | TN-0.52 | TN-1.08 | TN-1.58 | TN-1.00 | TN-0.50 | TN-1.06 | TN-1.21 | TN-0.99 | TN-0.49 |
| 12 | TP-0.10 | TP-0.07 | TP-0.06 | TP-0.06 | TP-0.11 | TP-0.09 | TP-0.10 | TP-0.09 | TP-0.07 | TP-0.04 | TP-0.04 | TP-0.04 | TP-0.09 | TP-0.07 | TP-0.08 | TP-0.07 |
| 13 | TN-0.57 | TN-0.41 | TN-0.36 | TN-0.39 | TP-0.28 | TP-0.25 | TP-0.17 | TP-0.23 | TN-0.68 | TN-0.62 | TN-0.70 | TN-0.62 | TN-0.61 | TN-0.56 | TN-0.63 | TN-0.55 |
| 14 | TP-0.24 | TP-0.15 | TP-0.25 | FN-1.04 | TP-0.25 | TP-0.18 | TP-0.32 | FN-0.90 | TN-0.60 | TN-0.40 | TN-0.52 | TN-0.97 | TN-0.71 | TN-0.52 | TN-0.55 | TN-0.83 |
| 15 | TN-0.45 | TP-0.26 | TP-0.30 | TP-0.22 | TN-0.49 | TP-0.34 | TP-0.33 | TP-0.29 | TN-0.68 | TN-0.48 | TN-0.52 | TN-0.40 | TN-0.68 | TN-0.52 | TN-0.52 | TN-0.44 |
| 16 | TN-0.48 | TN-0.44 | FP-0.33 | FP-0.32 | TN-0.52 | TN-0.43 | TN-0.37 | TN-0.39 | TN-1.00 | TN-0.92 | TN-0.84 | TN-0.86 | TN-0.80 | TN-0.64 | TN-0.54 | TN-0.47 |
| 17 | TP-0.13 | TP-0.11 | TP-0.14 | TP-0.15 | TP-0.22 | TP-0.20 | TP-0.18 | TP-0.24 | TP-0.19 | TP-0.17 | TP-0.21 | TP-0.23 | TP-0.26 | TP-0.22 | TP-0.24 | TP-0.28 |
| 18 | TP-0.08 | TP-0.06 | TP-0.06 | TP-0.06 | TP-0.13 | TP-0.09 | TP-0.09 | TP-0.10 | TP-0.06 | TP-0.04 | TP-0.04 | TP-0.03 | TP-0.18 | TP-0.05 | TP-0.05 | TP-0.05 |
| 19 | TN-0.83 | TN-0.69 | TN-0.60 | TN-0.64 | TN-0.65 | TN-0.50 | TN-0.43 | TN-0.39 | TN-0.75 | TN-0.71 | TN-0.62 | TN-0.79 | TN-0.73 | TN-0.67 | TN-0.62 | TN-0.72 |
| 20 | TP-0.13 | TP-0.14 | TP-0.14 | TP-0.22 | TP-0.12 | TP-0.11 | TP-0.15 | TP-0.23 | TP-0.09 | TP-0.08 | TP-0.10 | TP-0.14 | TP-0.07 | TP-0.07 | TP-0.09 | TP-0.12 |
| 21 | TP-0.32 | TP-0.25 | TP-0.26 | TP-0.22 | TP-0.15 | TP-0.13 | TP-0.15 | TP-0.13 | TP-0.20 | TP-0.19 | TP-0.21 | TP-0.21 | TP-0.21 | TP-0.22 | TP-0.29 | TP-0.21 |
| 22 | TN-0.57 | TN-0.58 | TN-0.53 | FP-0.33 | TN-0.58 | TN-0.58 | TN-0.58 | FP-0.34 | TN-0.70 | TN-0.48 | TN-0.49 | TN-0.36 | TN-0.76 | TN-0.43 | TN-0.37 | FP-0.32 |
| 23 | TN-0.45 | TN-0.56 | TN-0.56 | TN-0.36 | TN-0.86 | TN-0.85 | TN-0.80 | TN-0.68 | TN-1.16 | TN-1.36 | TN-1.18 | TN-1.30 | TN-0.74 | TN-0.79 | TN-0.72 | TN-0.75 |
| 24 | TN-0.67 | TN-0.61 | TN-0.53 | TN-0.87 | TN-0.61 | TN-0.59 | TN-0.46 | TN-0.66 | TN-0.62 | TN-0.60 | TN-0.38 | TN-0.61 | TN-0.46 | TN-0.49 | TP-0.20 | FN-0.55 |
| 25 | TP-0.28 | TP-0.21 | TP-0.21 | TP-0.25 | TN-0.49 | TN-0.53 | TN-0.58 | TN-0.55 | TN-0.55 | TN-0.62 | TN-0.66 | TN-0.64 | FP-0.34 | FP-0.26 | FP-0.27 | FP-0.28 |
| GROUP | FRR |
|---|---|
| HEALTHY | |
| LBP |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paoletti, M.; Belli, A.; Palma, L.; Vallasciani, M.; Pierleoni, P. A Wireless Body Sensor Network for Clinical Assessment of the Flexion-Relaxation Phenomenon. Electronics 2020, 9, 1044. https://doi.org/10.3390/electronics9061044
Paoletti M, Belli A, Palma L, Vallasciani M, Pierleoni P. A Wireless Body Sensor Network for Clinical Assessment of the Flexion-Relaxation Phenomenon. Electronics. 2020; 9(6):1044. https://doi.org/10.3390/electronics9061044
Chicago/Turabian StylePaoletti, Michele, Alberto Belli, Lorenzo Palma, Massimo Vallasciani, and Paola Pierleoni. 2020. "A Wireless Body Sensor Network for Clinical Assessment of the Flexion-Relaxation Phenomenon" Electronics 9, no. 6: 1044. https://doi.org/10.3390/electronics9061044