
AI-Assisted CBCT Data Management in Modern Dental Practice: Benefits, Limitations and Innovations

 ,
, 
 ,
,  ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- Detecting structures (identifying the presence of normal and abnormal structures);
- Segmenting structures (determining the exact shape of particular structures);
- Classifying structures (distinguishing the sites and establishing the grade of a possible anomaly).
- Image segmentation: CBCT data in orthodontics usually consists of a large number of 3D images. AI algorithms can be used to segment these images, i.e., to identify and separate different anatomical structures (e.g., teeth, bone, and soft tissue) within the images. This can help orthodontists make more accurate diagnoses and treatment plans.
- Diagnosis and treatment planning: AI can help orthodontists make more informed diagnoses and treatment plans by analyzing CBCT data and making suggestions based on patterns and trends in the data. For example, AI can identify common characteristics of patients with similar dental problems and suggest treatment options that have been proven to work in these cases.
- Predictive analytics: AI can be used to predict the likelihood of certain outcomes based on CBCT data. For example, an AI algorithm can be trained to predict the likelihood of a successful treatment outcome for a particular patient based on their CBCT data and other clinical factors.
- Workflow automation: AI can be used to automate certain tasks in the CBCT data management process, such as image analysis and report generation. This can help streamline the workflow and save time for orthodontic professionals.
- Communication with the patient: AI can be used to communicate treatment options and outcomes to patients in a more visual and interactive way. For example, AI can create 3D models of patients’ teeth and show them how their teeth will look like after the treatment.
2. Materials and Methods
2.1. Inclusion Criteria for This Scoping Review
- The research question for this scoping review is: “What are the benefits, limitations and innovations of AI-assisted CBCT data management in modern dental practice?”
- Population of interest: dental professionals and dental assistants involved in CBCT data management in modern dental practice.
- Type of interventions: the use of artificial intelligence (AI) in CBCT data management, including semiautomated segmentation and standard medical diagnostic workflows.
- Outcomes of interest: the benefits and limitations of AI implementation for enhancing efficiency and accuracy in CBCT data management, as well as the potential impact on the roles of dental assistants in modern dental practice. Other outcomes of interest include the reliability, effectiveness, and usefulness of AI tools in dental workflows, potential errors and limitations that may occur, and the overall impact of AI-assisted CBCT data management on the quality of patient care.
- PubMed;
- Cochrane Library;
- Scopus;
- Web of Science.
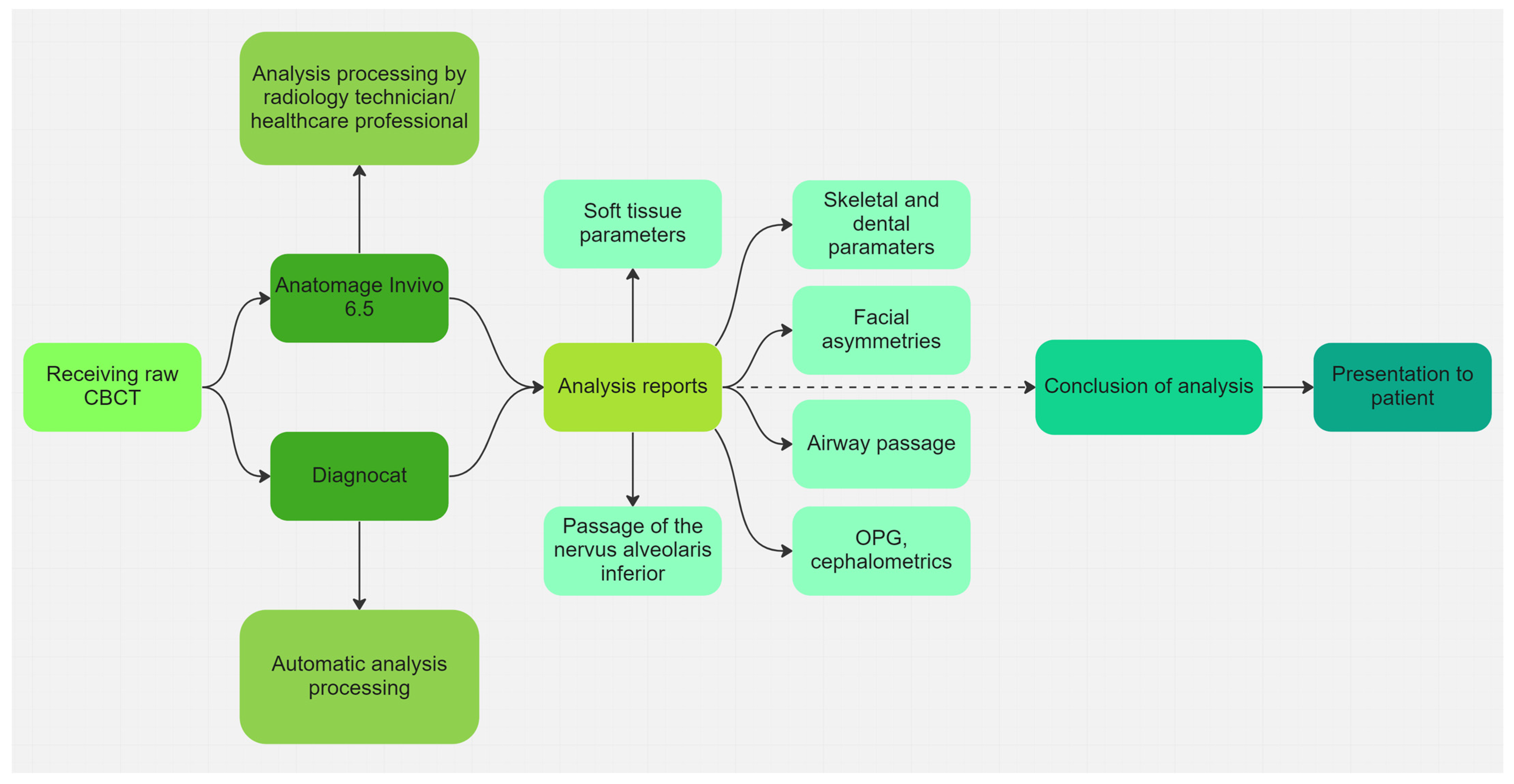
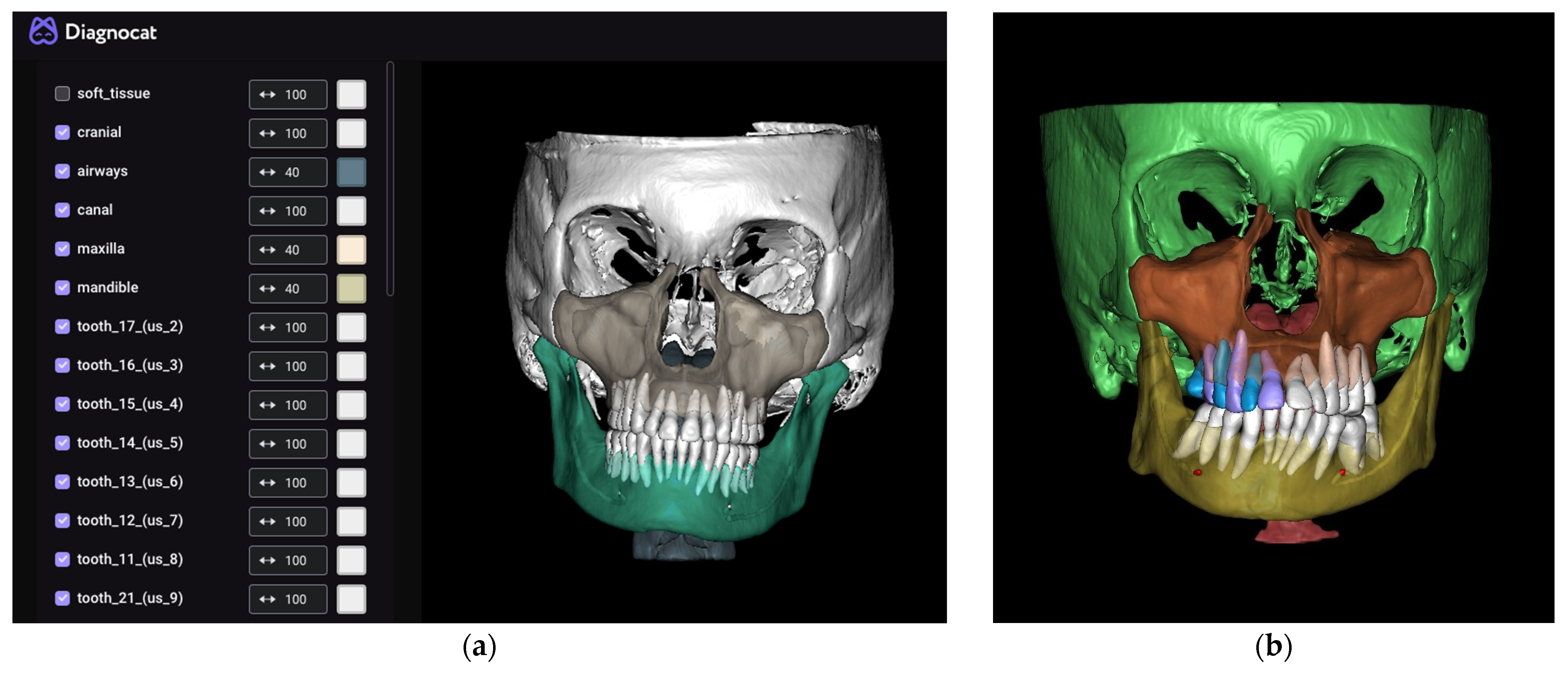
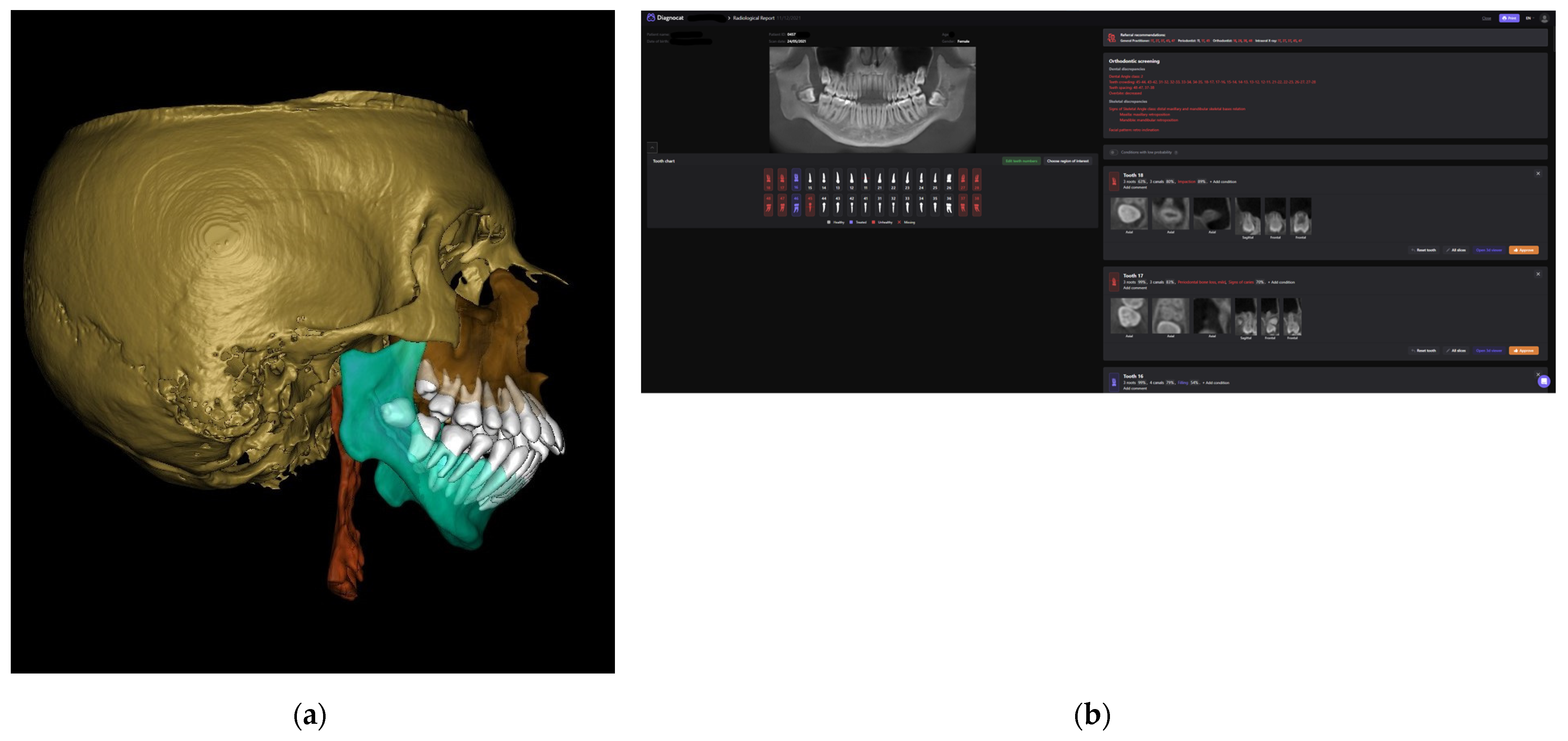
2.2. Software Used
- Diagnocat (USA—Diagnocat LTD, Miami, FL, USA) for AI segmentation;
- Invivo 7.0 (Anatomage, Santa Clara, CA, USA) for segmented model analysis;
2.3. Processing CBCT
3. Discussion
4. Conclusions
- AI-assisted image processing and analysis; AI algorithms can be trained to analyze CBCT images for specific dental conditions, such as by identifying the location and alignment of impacted teeth or assessing bone quality for implant placement.
- Data integration and management; CBCT data can be integrated with other patient data, such as intraoral scans and electronic dental records, to provide a comprehensive overview of the patient’s dental health.
- Patient communication and education; AI tools can help dental assistants communicate CBCT findings clearly to patients, helping them better understand their dental health and treatment options.
- Quality assurance; AI algorithms can be used to ensure the quality of CBCT images, such as by detecting artifacts or image distortions that could affect image interpretation.
- The assessment of the quality of the literature indicates a high risk of bias due to the inadequate sample size and incomplete reporting in many studies. High-quality annotated datasets and external validation are needed to improve AI-based dental imaging. AI can improve dental care, but further research and validation are needed before its clinical use, especially in view of the limited availability of data.
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gillot, M.; Miranda, F.; Baquero, B.; Ruellas, A.; Gurgel, M.; al Turkestani, N.; Anchling, L.; Hutin, N.; Biggs, E.; Yatabe, M.; et al. Automatic Landmark Identification in Cone-Beam Computed Tomography. Orthod. Craniofacial Res. 2023. [Google Scholar] [CrossRef]
- Benčević, M.; Galić, I.; Habijan, M.; Pižurica, A. Recent Progress in Epicardial and Pericardial Adipose Tissue Segmentation and Quantification Based on Deep Learning: A Systematic Review. Appl. Sci. 2022, 12, 5217. [Google Scholar] [CrossRef]
- Singh, S.P.; Wang, L.; Gupta, S.; Goli, H.; Padmanabhan, P.; Gulyás, B. 3D Deep Learning on Medical Images: A Review. Sensors 2020, 20, 5097. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Guo, X.; Mu, C.; Qi, S.; Li, G. Detection of Vertical Root Fractures by Cone-Beam Computed Tomography Based on Deep Learning. Dentomaxillofacial Radiol. 2023, 52, 20220345. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Fan, L.; Zhang, S.; Zhao, J.; Gu, Y. Deep Learning Based Dental Implant Failure Prediction from Periapical and Panoramic Films. Quant. Imaging Med. Surg. 2023, 13, 935–945. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.K.; Raza, K. Progress in Deep Learning-Based Dental and Maxillofacial Image Analysis: A Systematic Review. Expert Syst. Appl. 2022, 199, 116968. [Google Scholar] [CrossRef]
- Murata, M.; Ariji, Y.; Ohashi, Y.; Kawai, T.; Fukuda, M.; Funakoshi, T.; Kise, Y.; Nozawa, M.; Katsumata, A.; Fujita, H.; et al. Deep-Learning Classification Using Convolutional Neural Network for Evaluation of Maxillary Sinusitis on Panoramic Radiography. Oral Radiol. 2019, 35, 301–307. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, D.H.; Jeong, S.N.; Choi, S.H. Detection and Diagnosis of Dental Caries Using a Deep Learning-Based Convolutional Neural Network Algorithm. J. Dent. 2018, 77, 106–111. [Google Scholar] [CrossRef]
- Fatima, A.; Shahid, A.R.; Raza, B.; Madni, T.M.; Janjua, U.I. State-of-the-Art Traditional to the Machine- and Deep-Learning-Based Skull Stripping Techniques, Models, and Algorithms. J. Digit. Imaging 2020, 33, 1443–1464. [Google Scholar] [CrossRef]
- Wang, H.; Minnema, J.; Batenburg, K.J.; Forouzanfar, T.; Hu, F.J.; Wu, G. Multiclass CBCT Image Segmentation for Orthodontics with Deep Learning. J. Dent. Res. 2021, 100, 943–949. [Google Scholar] [CrossRef]
- Thurzo, A.; Kosnáčová, H.S.; Kurilová, V.; Kosmeľ, S.; Beňuš, R.; Moravanský, N.; Kováč, P.; Kuracinová, K.M.; Palkovič, M.; Varga, I. Use of Advanced Artificial Intelligence in Forensic Medicine, Forensic Anthropology and Clinical Anatomy. Healthcare 2021, 9, 1545. [Google Scholar] [CrossRef] [PubMed]
- Habijan, M.; Galić, I.; Romić, K.; Leventić, H. AB-ResUNet+: Improving Multiple Cardiovascular Structure Segmentation from Computed Tomography Angiography Images. Appl. Sci. 2022, 12, 3024. [Google Scholar] [CrossRef]
- Habijan, M.; Leventić, H.; Galić, I.; Babin, D. Neural Network Based Whole Heart Segmentation from 3D CT Images. Int. J. Electr. Comput. Eng. Syst. 2020, 11, 25–31. [Google Scholar] [CrossRef]
- Lascala, C.A.; Panella, J.; Marques, M.M. Analysis of the Accuracy of Linear Measurements Obtained by Cone Beam Computed Tomography (CBCT-NewTom). Dentomaxillofacial Radiol. 2014, 33, 291–294. [Google Scholar] [CrossRef] [PubMed]
- Thurzo, A.; Javorka, V.; Stanko, P.; Lysy, J.; Suchancova, B.; Lehotska, V.; Valkovic, L.; Makovnik, M. Digital and Manual Cephalometric Analysis. Bratisl. Med. J. 2010, 111, 97–100. [Google Scholar]
- Alamri, H.M.; Sadrameli, M.; Alshalhoob, M.A.; Sadrameli, M.; Alshehri, M.A. Applications of CBCT in Dental Practice: A Review of the Literature. Gen. Dent. 2012, 60, 390–400. [Google Scholar]
- Chen, Y.-W.; Stanley, K.; Att, W.; Dent, M. Artificial Intelligence in Dentistry: Current Applications and Future Perspectives. Quintessence Int. 2020, 51, 248–257. [Google Scholar] [CrossRef]
- Palanivel, J.; Davis, D.; Srinivasan, D.; Nc, S.C.; Kalidass, P.; Kishore, S.; Suvetha, S. Artificial Intelligence—Creating the Future in Orthodontics—A Review. J. Evol. Med. Dent. Sci. 2021, 10, 2108–2113. [Google Scholar] [CrossRef]
- Ezhov, M.; Gusarev, M.; Golitsyna, M.; Yates, J.M.; Kushnerev, E.; Tamimi, D.; Aksoy, S.; Shumilov, E.; Sanders, A.; Orhan, K. Clinically Applicable Artificial Intelligence System for Dental Diagnosis with CBCT. Sci. Rep. 2021, 11, 15006. [Google Scholar] [CrossRef]
- Ghazal, J. Application of Artificial Intelligence Diagnocat in Diagnostics of Maxillary Sinusitis; Boiarina, Ed.; Belarusian State Medical University: Minsk, Belarus, 2021; Volume 1, p. 1330. ISBN 978-985-21-0765-5. [Google Scholar]
- Benavides, E.; Edwards, P.C. Detection of Incidental Findings in Cone Beam Computed Tomography Imaging and Their Clinical Implications. Cone Beam Comput. Tomogr. Orthod. Indic. Insights Innov. 2014, 185–219. [Google Scholar] [CrossRef]
- Mureșanu, S.; Almășan, O.; Hedeșiu, M.; Dioșan, L.; Dinu, C.; Jacobs, R. Artificial Intelligence Models for Clinical Usage in Dentistry with a Focus on Dentomaxillofacial CBCT: A Systematic Review. Oral Radiol. 2023, 39, 18–40. [Google Scholar] [CrossRef]
- Gerhardt, M.D.N.; Fontenele, R.C.; Willems, H.; Jacobs, R. Accuracy of an Artificial Intelligence-Driven Tool for the Detection of Small Edentulous Regions on Cone-Beam Computed Tomography. J. Dent. 2022, 121, 103989. [Google Scholar] [CrossRef]
- Tsolakis, I.A.; Kolokitha, O.-E.; Papadopoulou, E.; Tsolakis, A.I.; Kilipiris, E.G.; Palomo, J.M. Artificial Intelligence as an Aid in CBCT Airway Analysis: A Systematic Review. Life 2022, 12, 1894. [Google Scholar] [CrossRef] [PubMed]
- Aung, N.M.; Myint, K.K. Diagnostic Accuracy of CBCT for Detection of Second Canal of Permanent Teeth: A Systematic Review and Meta-Analysis. Int. J. Dent. 2021, 2021, 1107471. [Google Scholar] [CrossRef]
- Olczak, K.; Pawlicka, H.; Szymański, W. Root and Canal Morphology of the Maxillary Second Premolars as Indicated by Cone Beam Computed Tomography. Aust. Endod. J. 2022. [Google Scholar] [CrossRef] [PubMed]
- Alhammadi, M.S.; Al-mashraqi, A.A.; Alnami, R.H.; Ashqar, N.M.; Alamir, O.H.; Halboub, E.; Reda, R.; Testarelli, L.; Patil, S. Accuracy and Reproducibility of Facial Measurements of Digital Photographs and Wrapped Cone Beam Computed Tomography (CBCT) Photographs. Diagnostics 2021, 11, 757. [Google Scholar] [CrossRef]
- Vasiljevic, M.; Milanovic, P.; Jovicic, N.; Vasovic, M.; Milovanovic, D.; Vojinovic, R.; Selakovic, D.; Rosic, G. Morphological and Morphometric Characteristics of Anterior Maxilla Accessory Canals and Relationship with Nasopalatine Canal Type—A CBCT Study. Diagnostics 2021, 11, 1510. [Google Scholar] [CrossRef]
- Leonardi, R.; Ronsivalle, V.; Lagravere, M.O.; Barbato, E.; Isola, G.; lo Giudice, A. Three-Dimensional Assessment of the Spheno-Occipital Synchondrosis and Clivus after Tooth-Borne and Bone-Borne Rapid Maxillary Expansion. Angle Orthod. 2021, 91, 822–829. [Google Scholar] [CrossRef]
- Dong, Q.; Shi, H.; Jia, Q.; Tian, Y.; Zhi, K.; Zhang, L. Analysis of Three-Dimensional Morphological Differences in the Mandible between Skeletal Class I and Class II with CBCT Fixed-Point Measurement Method. Scanning 2021, 2021, 9996857. [Google Scholar] [CrossRef]
- Thurzo, A.; Šufliarsky, B.; Urbanová, W.; Čverha, M.; Strunga, M.; Varga, I. Pierre Robin Sequence and 3D Printed Personalized Composite Appliances in Interdisciplinary Approach. Polymers 2022, 14, 3858. [Google Scholar] [CrossRef]
- Orhan, K.; Shamshiev, M.; Ezhov, M.; Plaksin, A.; Kurbanova, A.; Ünsal, G.; Gusarev, M.; Golitsyna, M.; Aksoy, S.; Mısırlı, M.; et al. AI-Based Automatic Segmentation of Craniomaxillofacial Anatomy from CBCT Scans for Automatic Detection of Pharyngeal Airway Evaluations in OSA Patients. Sci. Rep. 2022, 12, 11863. [Google Scholar] [CrossRef] [PubMed]
- Almalki, Y.E.; Din, A.I.; Ramzan, M.; Irfan, M.; Aamir, K.M.; Almalki, A.; Alotaibi, S.; Alaglan, G.; Alshamrani, H.A.; Rahman, S. Deep Learning Models for Classification of Dental Diseases Using Orthopantomography X-ray OPG Images. Sensors 2022, 22, 7370. [Google Scholar] [CrossRef]
- Opris, H.; Baciut, M.; Bran, S.; Onisor, F.; Almasan, O.; Manea, A.; Tamas, T.; Stoia, S.; Gabriel, A.; Baciut, G.; et al. Lateral Cephalometric Analytical Uses for Temporomandibular Joint Disorders: The Importance of Cervical Posture and Hyoid Position. Int. J. Environ. Res. Public Health 2022, 19, 11077. [Google Scholar] [CrossRef] [PubMed]
- Zadrożny, Ł.; Regulski, P.; Brus-Sawczuk, K.; Czajkowska, M.; Parkanyi, L.; Ganz, S.; Mijiritsky, E. Artificial Intelligence Application in Assessment of Panoramic Radiographs. Diagnostics 2022, 12, 224. [Google Scholar] [CrossRef] [PubMed]
- Lupi, S.M.; Landini, J.; Olivieri, G.; Todaro, C.; Scribante, A.; Rodriguez y Baena, R. Correlation between the Mandibular Lingula Position and Some Anatomical Landmarks in Cone Beam CT. Healthcare 2021, 9, 1747. [Google Scholar] [CrossRef]
- Patel, A.R.; Vathare, A.; Mall, P.; Ghunawat, D.B.; Thole, L.; Dhande, P.; Kulkarni, D. Correlation between Clinical Symptoms and Cone Beam Computed Tomography Finding in Temporomandibular Disorders Patients. Int. J. Health Sci. 2022, 6, 2381–2387. [Google Scholar] [CrossRef]
- Thurzo, A.; Strunga, M.; Havlínová, R.; Reháková, K.; Urban, R.; Surovková, J.; Kurilová, V. Smartphone-Based Facial Scanning as a Viable Tool for Facially Driven Orthodontics? Sensors 2022, 22, 7752. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-C.; Hwang, H.-S.; Lee, K.C. Accuracy of Deep Learning-Based Integrated Tooth Models by Merging Intraoral Scans and CBCT Scans for 3D Evaluation of Root Position during Orthodontic Treatment. Prog. Orthod. 2022, 23, 15. [Google Scholar] [CrossRef]
- Retrouvey, J.-M.; Conley, R.S. Decoding Deep Learning Applications for Diagnosis and Treatment Planning. Dent. Press J. Orthod. 2022, 27, 22–27. [Google Scholar] [CrossRef]
- Issa, J.; Olszewski, R.; Dyszkiewicz-Konwińska, M. The Effectiveness of Semi-Automated and Fully Automatic Segmentation for Inferior Alveolar Canal Localization on CBCT Scans: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 560. [Google Scholar] [CrossRef]
- D’Addazio, G.; Xhajanka, E.; Traini, T.; Santilli, M.; Rexhepi, I.; Murmura, G.; Caputi, S.; Sinjari, B. Accuracy of DICOM–DICOM vs. DICOM–STL Protocols in Computer-Guided Surgery: A Human Clinical Study. J. Clin. Med. 2022, 11, 2336. [Google Scholar] [CrossRef]
- da Silva Rocha, É.; Endo, P.T. A Comparative Study of Deep Learning Models for Dental Segmentation in Panoramic Radiograph. Appl. Sci. 2022, 12, 3103. [Google Scholar] [CrossRef]
- Thurzo, A.; Jančovičová, V.; Hain, M.; Thurzo, M.; Novák, B.; Kosnáčová, H.; Lehotská, V.; Moravanský, N.; Varga, I. Human Remains Identification Using Micro-CT, Spectroscopic and A.I. Methods in Forensic Experimental Reconstruction of Dental Patterns After Concentrated Acid Significant Impact. Molecules 2022, 27, 4035. [Google Scholar] [CrossRef] [PubMed]
- Strunga, M.; Urban, R.; Surovková, J.; Thurzo, A. Artificial Intelligence Systems Assisting in the Assessment of the Course and Retention of Orthodontic Treatment. Healthcare 2023, 11, 683. [Google Scholar] [CrossRef]
- Kurt Bayrakdar, S.; Orhan, K.; Bayrakdar, I.S.; Bilgir, E.; Ezhov, M.; Gusarev, M.; Shumilov, E. A Deep Learning Approach for Dental Implant Planning in Cone-Beam Computed Tomography Images. BMC Med. Imaging 2021, 21, 86. [Google Scholar] [CrossRef] [PubMed]
- Khabadze, Z.; Makeeva, I.; Mordanov, O.; Nazarova, D. Processing of cbct data with artificial intelligence in the diagnosis of caries and its complications. Actual Probl. Dent. 2022, 18, 78–86. [Google Scholar] [CrossRef]
- Izham, A.; Auerkari, E.I. The Use of Radiology CBCT in Odontology Forensic. AIP Conf. Proc. 2021, 2344, 050012. [Google Scholar] [CrossRef]
- Kim, S.-H.; Kim, K.B.; Choo, H. New Frontier in Advanced Dentistry: CBCT, Intraoral Scanner, Sensors, and Artificial Intelligence in Dentistry. Sensors 2022, 22, 2942. [Google Scholar] [CrossRef]
- Qiu, B.; van der Wel, H.; Kraeima, J.; Glas, H.H.; Guo, J.; Borra, R.J.H.; Witjes, M.J.H.; van Ooijen, P.M.A. Robust and Accurate Mandible Segmentation on Dental CBCT Scans Affected by Metal Artifacts Using a Prior Shape Model. J. Pers. Med. 2021, 11, 364. [Google Scholar] [CrossRef]
- Duman, Ş.B.; Syed, A.Z.; Celik Ozen, D.; Bayrakdar, İ.Ş.; Salehi, H.S.; Abdelkarim, A.; Celik, Ö.; Eser, G.; Altun, O.; Orhan, K. Convolutional Neural Network Performance for Sella Turcica Segmentation and Classification Using CBCT Images. Diagnostics 2022, 12, 2244. [Google Scholar] [CrossRef]
- Jang, T.J.; Kim, K.C.; Cho, H.C.; Seo, J.K. A Fully Automated Method for 3D Individual Tooth Identification and Segmentation in Dental CBCT. IEEE Trans. Pattern Anal. Mach. Intell. 2021, 10, 6562–6568. [Google Scholar] [CrossRef]
- Švábová nee Uhrová, P.; Beňuš, R.; Chovancová nee Kondeková, M.; Vojtušová, A.; Novotný, M.; Thurzo, A. Use of Third Molar Eruption Based on Gambier’s Criteria in Assessing Dental Age. Int. J. Leg. Med. 2023. [Google Scholar] [CrossRef]
- Thurzo, A.; Strunga, M.; Urban, R.; Surovková, J.; Afrashtehfar, K.I. Impact of Artificial Intelligence on Dental Education: A Review and Guide for Curriculum Update. Educ. Sci. 2023, 13, 150. [Google Scholar] [CrossRef]
- Thurzo, A.; Kurilová, V.; Varga, I. Artificial Intelligence in Orthodontic Smart Application for Treatment Coaching and Its Impact on Clinical Performance of Patients Monitored with AI-Telehealth System. Healthcare 2021, 9, 1695. [Google Scholar] [CrossRef] [PubMed]
- Thurzo, A.; Urbanová, W.; Neuschlová, I.; Paouris, D.; Čverha, M. Use of Optical Scanning and 3D Printing to Fabricate Customized Appliances for Patients with Craniofacial Disorders. Semin. Orthod. 2022, 28, 92–99. [Google Scholar] [CrossRef]
- Caruso, S.; Caruso, S.; Pellegrino, M.; Skafi, R.; Nota, A.; Tecco, S. A Knowledge-Based Algorithm for Automatic Monitoring of Orthodontic Treatment: The Dental Monitoring System. Two Cases. Sensors 2021, 21, 1856. [Google Scholar] [CrossRef]
- Morabito, A.E.; Guardiani, E.; Mandolini, M.; Brunzini, A.; Facco, G.; Mazzoli, A.; Forcellese, A.; Gigante, A. Comparison of Three 3D Segmentation Software Tools for Hip Surgical Planning. Sensors 2022, 22, 5242. [Google Scholar] [CrossRef]
- Lee, S.; Kim, J.E. Evaluating the Precision of Automatic Segmentation of Teeth, Gingiva and Facial Landmarks for 2D Digital Smile Design Using Real-Time Instance Segmentation Network. J. Clin. Med. 2022, 11, 852. [Google Scholar] [CrossRef] [PubMed]
- Thurzo, A.; Urbanová, W.; Novák, B.; Czako, L.; Siebert, T.; Stano, P.; Mareková, S.; Fountoulaki, G.; Kosnáčová, H.; Varga, I. Where Is the Artificial Intelligence Applied in Dentistry? Systematic Review and Literature Analysis. Healthcare 2022, 10, 1269. [Google Scholar] [CrossRef]
- Artificial Intelligence and Deep Learning in Dental Radiology. Available online: https://www.oralhealthgroup.com/features/artificial-intelligence-and-deep-learning-in-dental-radiology-a-way-forward-in-point-of-care-radiology/ (accessed on 24 March 2023).
- 6 Innovative Artificial Intelligence Applications in Dentistry. Available online: https://www.v7labs.com/blog/ai-in-dentistry (accessed on 24 March 2023).
- Albitar, L.; Zhao, T.; Huang, C.; Mahdian, M. Artificial Intelligence (AI) for Detection and Localization of Unobturated Second Mesial Buccal (MB2) Canals in Cone-Beam Computed Tomography (CBCT). Diagnostics 2022, 12, 3214. [Google Scholar] [CrossRef]
- How Accurate Are Facial Recognition Systems—And Why Does It Matter?|Strategic Technologies Blog|CSIS. Available online: https://www.csis.org/blogs/strategic-technologies-blog/how-accurate-are-facial-recognition-systems-and-why-does-it (accessed on 24 March 2023).
- Chung, E.-J.; Yang, B.-E.; Byun, S.-H.; Yi, S.; Kim, Y.-H.; Kang, S.-H. Effectiveness Of Cone-Beam Computed Tomography (CBCT)-Generated Cephalograms Using Artificial Intelligence (AI) Cephalometric Analysis. Sci. Rep. 2022, 12, 20585. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urban, R.; Haluzová, S.; Strunga, M.; Surovková, J.; Lifková, M.; Tomášik, J.; Thurzo, A. AI-Assisted CBCT Data Management in Modern Dental Practice: Benefits, Limitations and Innovations. Electronics 2023, 12, 1710. https://doi.org/10.3390/electronics12071710
Urban R, Haluzová S, Strunga M, Surovková J, Lifková M, Tomášik J, Thurzo A. AI-Assisted CBCT Data Management in Modern Dental Practice: Benefits, Limitations and Innovations. Electronics. 2023; 12(7):1710. https://doi.org/10.3390/electronics12071710
Chicago/Turabian StyleUrban, Renáta, Sára Haluzová, Martin Strunga, Jana Surovková, Michaela Lifková, Juraj Tomášik, and Andrej Thurzo. 2023. "AI-Assisted CBCT Data Management in Modern Dental Practice: Benefits, Limitations and Innovations" Electronics 12, no. 7: 1710. https://doi.org/10.3390/electronics12071710