
A Framework Integrating Augmented Reality and Wearable Sensors for the Autonomous Execution of Rehabilitation Exercises
 , , , , , and
, , , , , and
Abstract
:1. Introduction
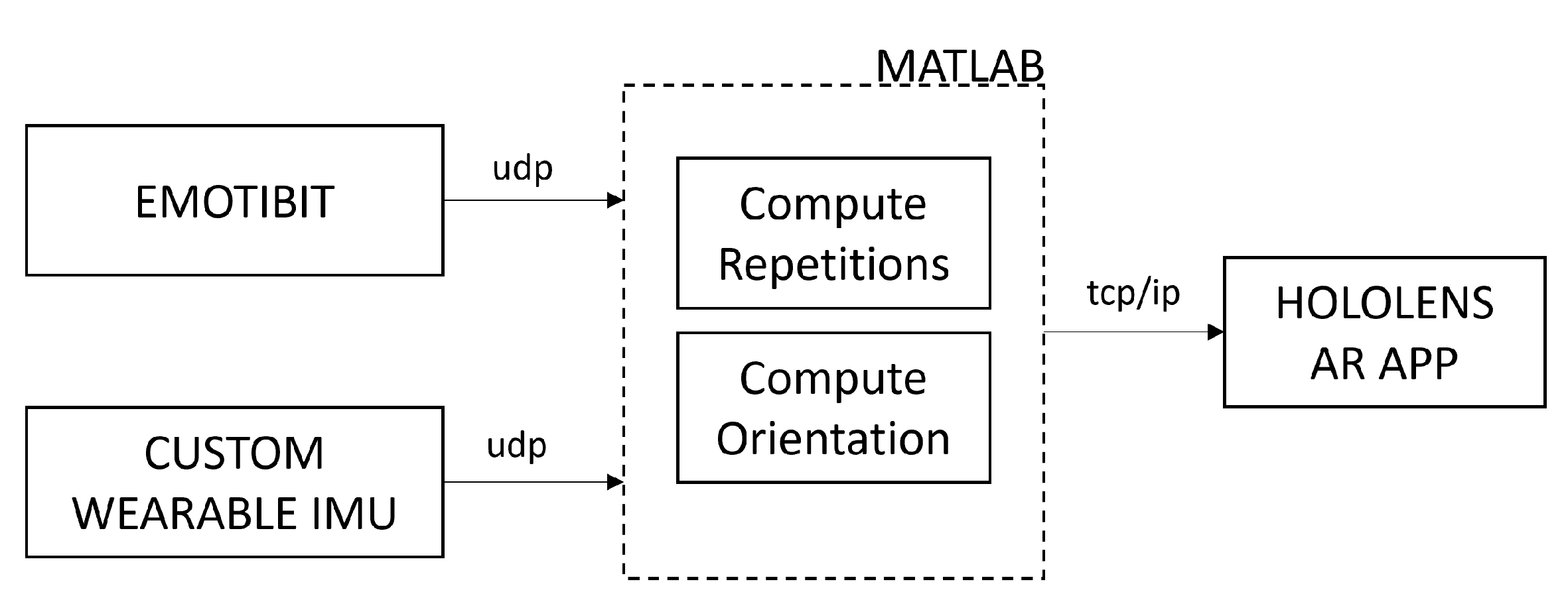
- Two wearable sensors connected to the ankles to acquire biometric and motion data from the patient, which enable the real-time analysis of the exercise execution;
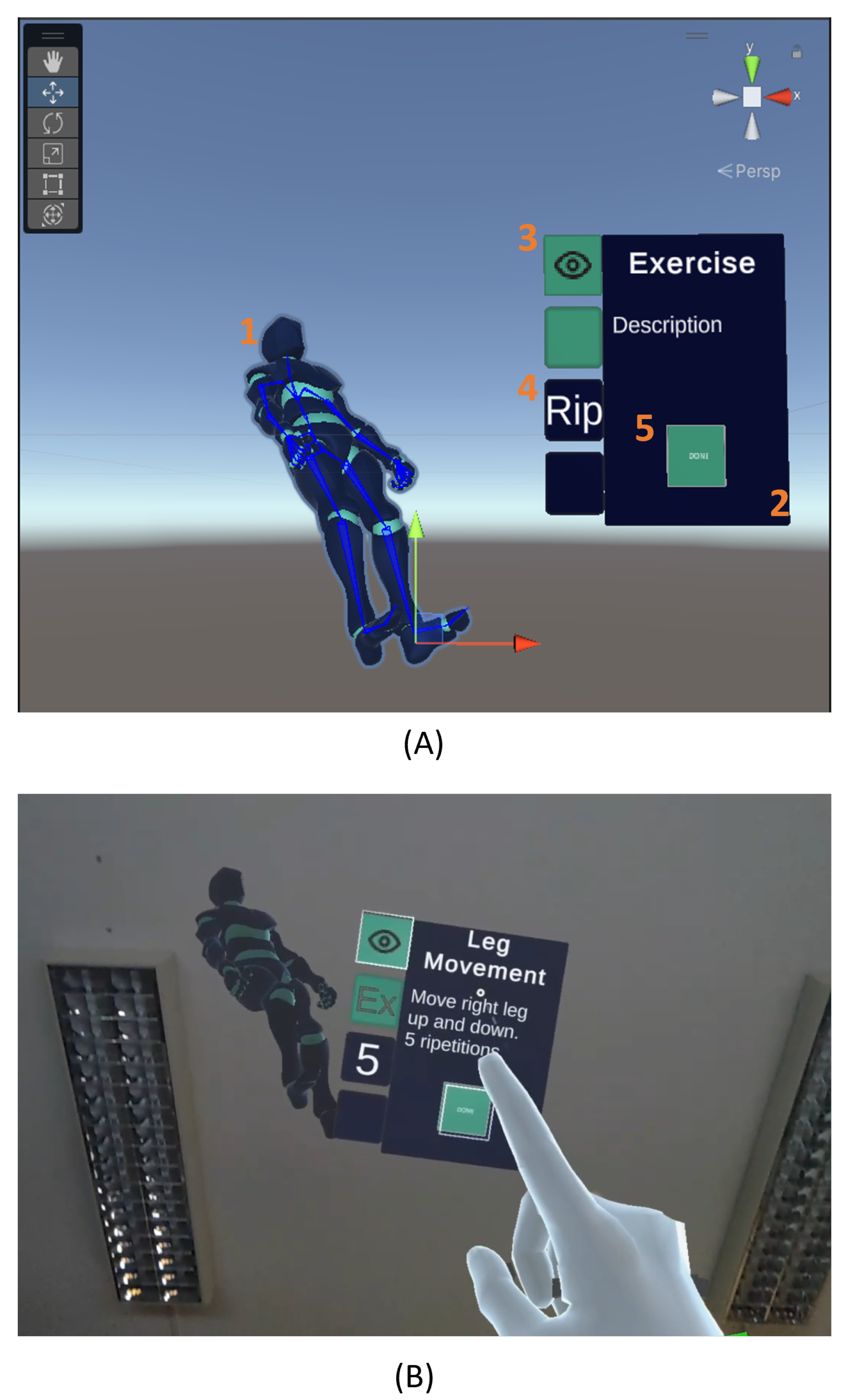
- The AR application that guides the patients in the execution of a set of rehabilitation exercises, by projecting a virtual avatar showing the movements to perform and providing real-time feedback on the execution of the current exercise.
2. Wearables: Hardware and Algorithms
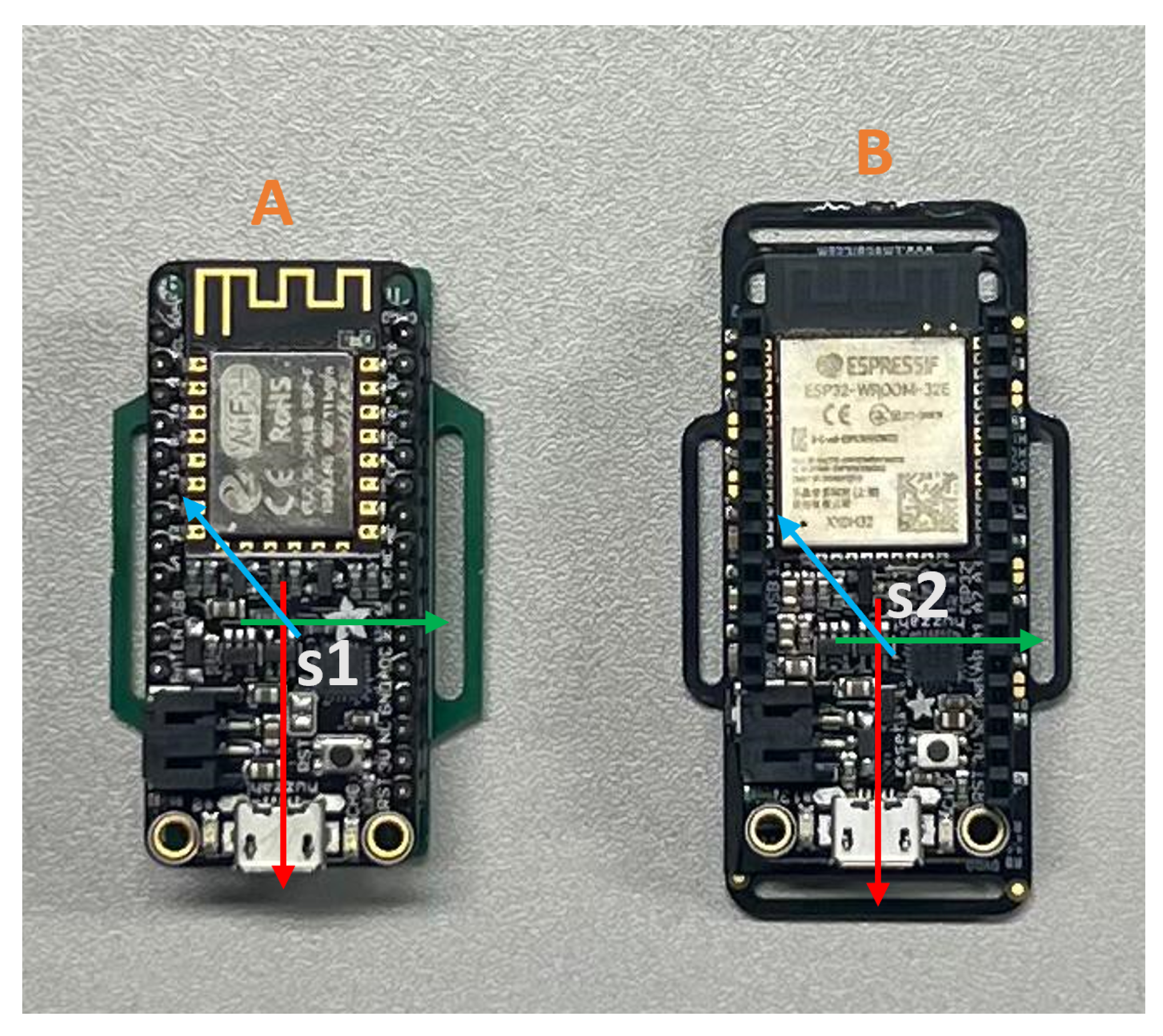
2.1. Hardware
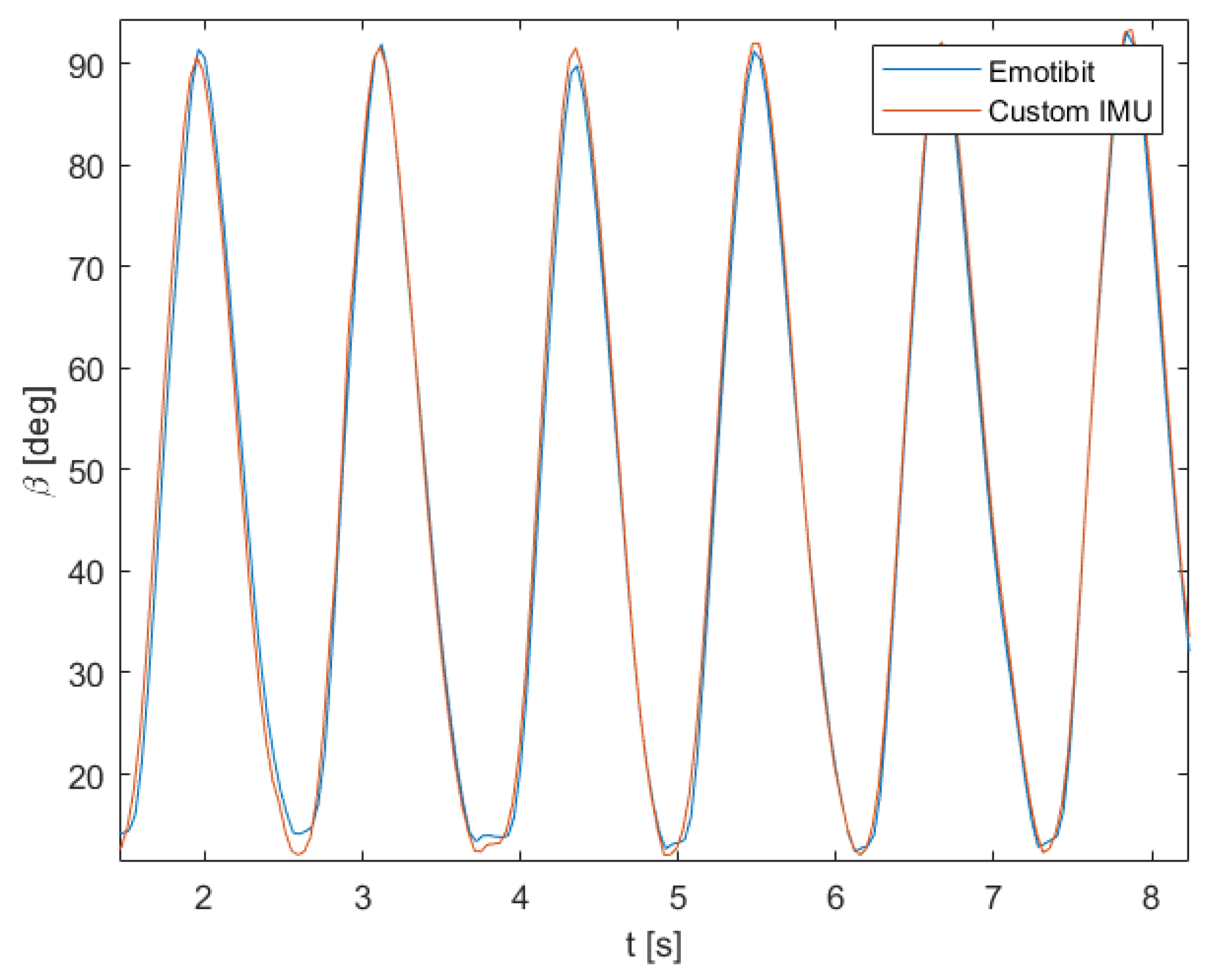
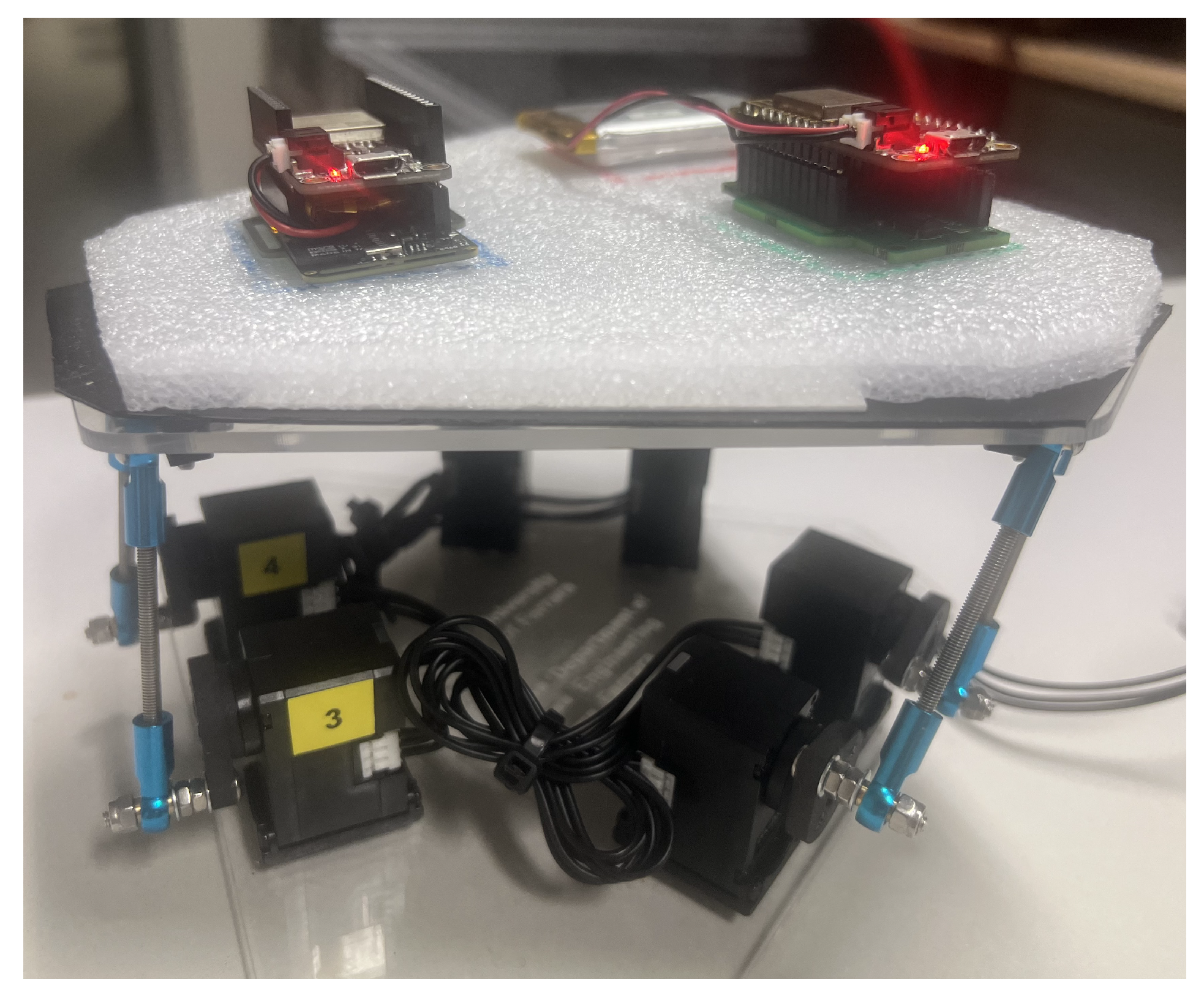
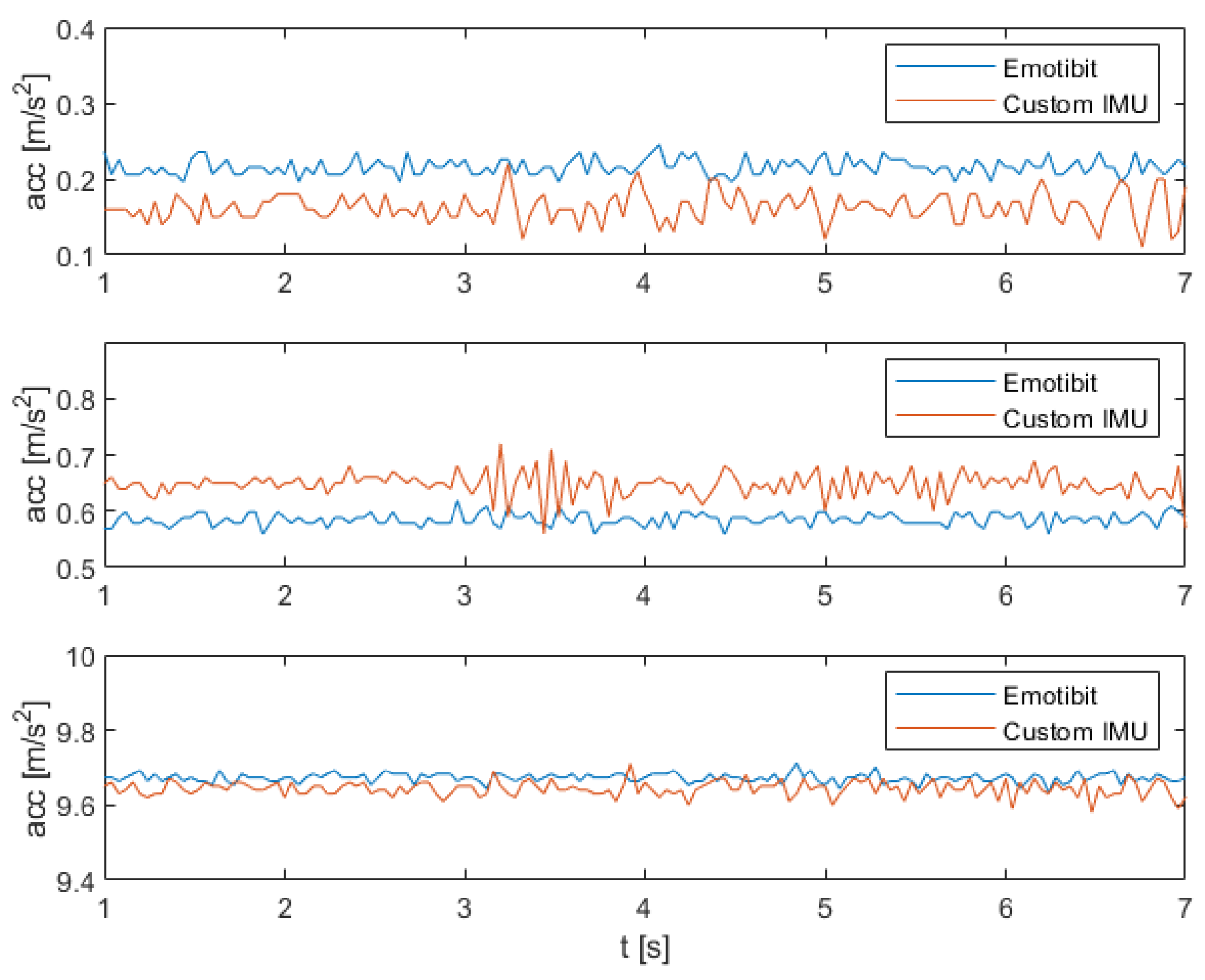
2.2. Comparative Analysis
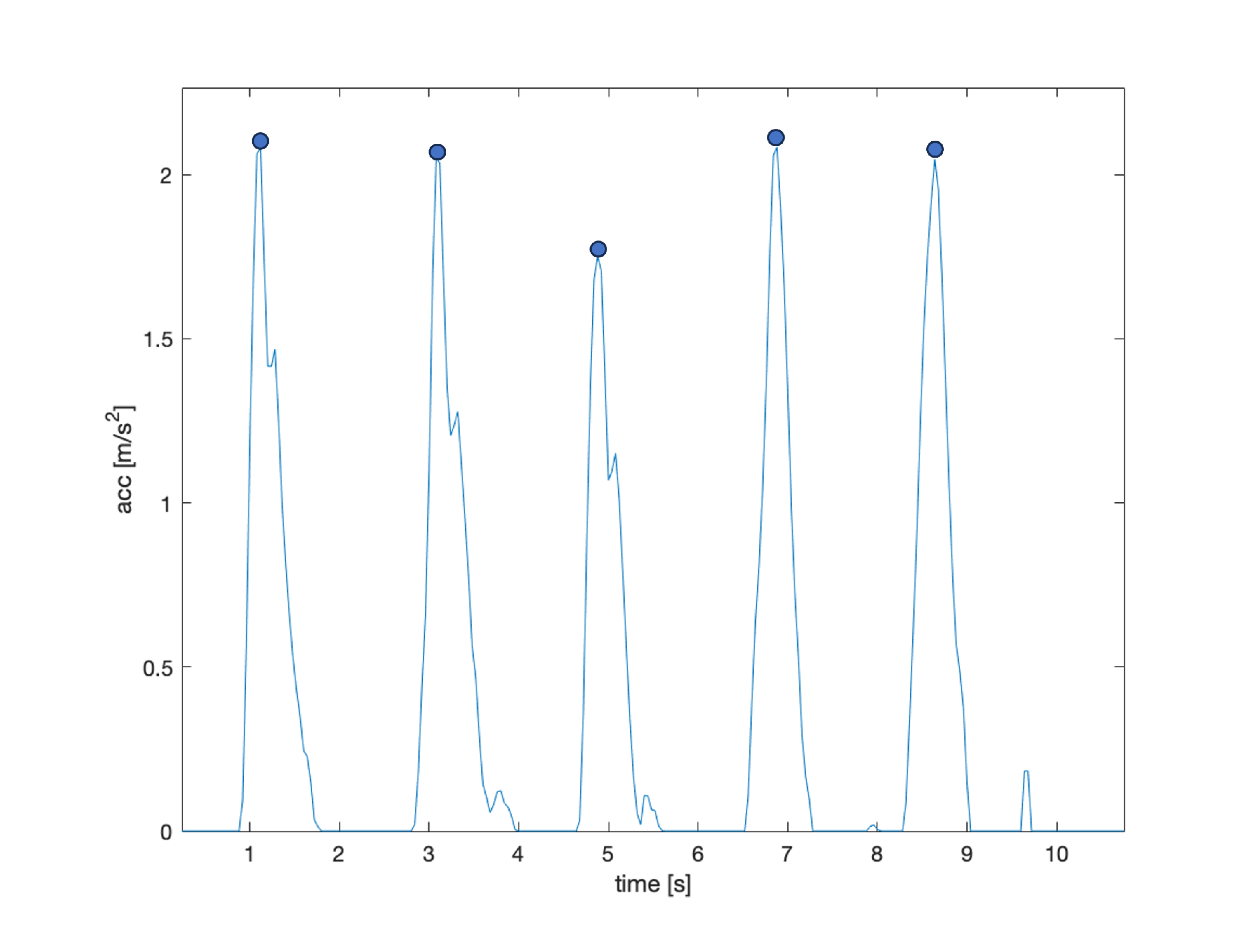
2.3. Algorithms
3. Augmented Reality Application
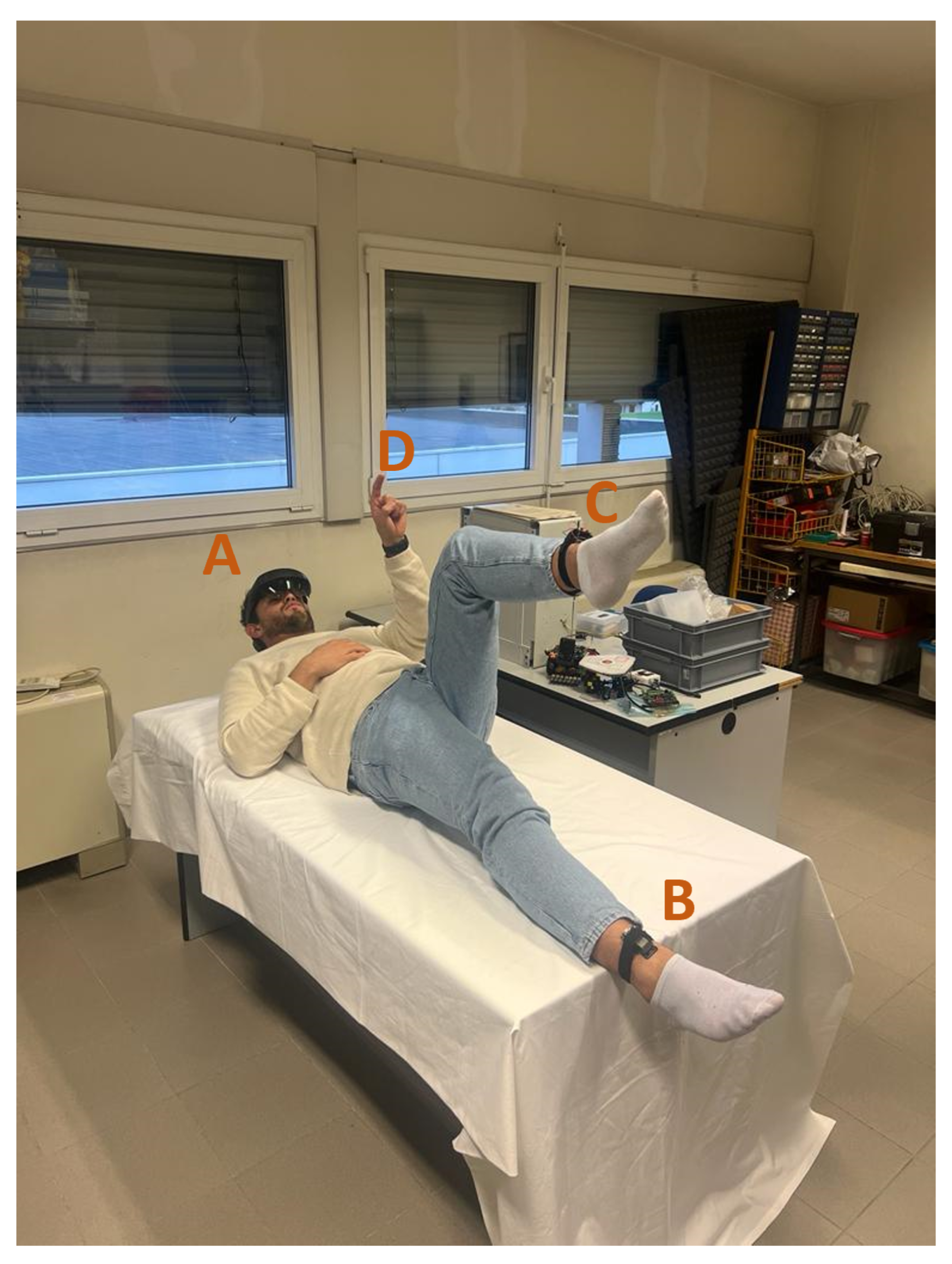
4. System Integration and Experiments
5. Validation
6. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cardoso, R.; Parola, V.; Neves, H.; Bernardes, R.A.; Duque, F.M.; Mendes, C.A.; Pimentel, M.; Caetano, P.; Petronilho, F.; Albuquerque, C.; et al. Physical rehabilitation programs for bedridden patients with prolonged immobility: A scoping review. Int. J. Environ. Res. Public Health 2022, 19, 6420. [Google Scholar] [CrossRef] [PubMed]
- Parola, V.; Neves, H.; Duque, F.M.; Bernardes, R.A.; Cardoso, R.; Mendes, C.A.; Sousa, L.B.; Santos-Costa, P.; Malça, C.; Durães, R.; et al. Rehabilitation Programs for Bedridden Patients with Prolonged Immobility: A Scoping Review Protocol. Int. J. Environ. Res. Public Health 2021, 18, 12033. [Google Scholar] [CrossRef] [PubMed]
- Holst, M.; Hansen, P.; Pedersen, L.; Paulsen, S.; Valentinsen, C.; Kohler, M. Physical activity in hospitalized old medical patients; how active are they, and what. J. Aging Res. Clin. Pract. 2015, 4, 116–123. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Ferrucci, L.; Simonsick, E.M.; Salive, M.E.; Wallace, R.B. Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. N. Engl. J. Med. 1995, 332, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, D.; Zhao, L.; Li, D.; Huang, M.; Wang, Y. Life satisfaction and its influencing factors for bedridden patients with stroke. J. Stroke Cerebrovasc. Dis. 2023, 32, 107254. [Google Scholar] [CrossRef]
- Martínez-Velilla, N.; Casas-Herrero, A.; Zambom-Ferraresi, F.; de Asteasu, M.L.S.; Lucia, A.; Galbete, A.; García-Baztán, A.; Alonso-Renedo, J.; González-Glaría, B.; Gonzalo-Lázaro, M.; et al. Effect of exercise intervention on functional decline in very elderly patients during acute hospitalization: A randomized clinical trial. JAMA Intern. Med. 2019, 179, 28–36. [Google Scholar] [CrossRef]
- Ellis, G.; Whitehead, M.A.; Robinson, D.; O’Neill, D.; Langhorne, P. Comprehensive geriatric assessment for older adults admitted to hospital: Meta-analysis of randomised controlled trials. BMJ 2011, 343, d6553. [Google Scholar] [CrossRef]
- Greysen, S.R. Activating hospitalized older patients to confront the epidemic of low mobility. JAMA Intern. Med. 2016, 176, 928–929. [Google Scholar] [CrossRef] [PubMed]
- Gill, T.M.; Allore, H.G.; Gahbauer, E.A.; Murphy, T.E. Change in disability after hospitalization or restricted activity in older persons. JAMA 2010, 304, 1919–1928. [Google Scholar] [CrossRef]
- Brown, C.J.; Redden, D.T.; Flood, K.L.; Allman, R.M. The underrecognized epidemic of low mobility during hospitalization of older adults. J. Am. Geriatr. Soc. 2009, 57, 1660–1665. [Google Scholar] [CrossRef]
- Tasheva, P.; Vollenweider, P.; Kraege, V.; Roulet, G.; Lamy, O.; Marques-Vidal, P.; Méan, M. Association between physical activity levels in the hospital setting and hospital-acquired functional decline in elderly patients. JAMA Netw. Open 2020, 3, e1920185. [Google Scholar] [CrossRef]
- Kortebein, P.; Ferrando, A.; Lombeida, J.; Wolfe, R.; Evans, W.J. Effect of 10 days of bed rest on skeletal muscle in healthy older adults. JAMA 2007, 297, 1769–1774. [Google Scholar] [CrossRef]
- Liu, B.; Moore, J.E.; Almaawiy, U.; Chan, W.H.; Khan, S.; Ewusie, J.; Hamid, J.S.; Straus, S.E.; Collaboration, M.O. Outcomes of Mobilisation of Vulnerable Elders in Ontario (MOVE ON): A multisite interrupted time series evaluation of an implementation intervention to increase patient mobilisation. Age Ageing 2018, 47, 112–119. [Google Scholar] [CrossRef] [PubMed]
- de Morton, N.A.; Keating, J.L.; Jeffs, K. The effect of exercise on outcomes for older acute medical inpatients compared with control or alternative treatments: A systematic review of randomized controlled trials. Clin. Rehabil. 2007, 21, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.J.; Foley, K.T.; Lowman, J.D.; MacLennan, P.A.; Razjouyan, J.; Najafi, B.; Locher, J.; Allman, R.M. Comparison of posthospitalization function and community mobility in hospital mobility program and usual care patients: A randomized clinical trial. JAMA Intern. Med. 2016, 176, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Bekdemir, A.; Ilhan, N. Predictors of caregiver burden in caregivers of bedridden patients. J. Nurs. Res. 2019, 27, e24. [Google Scholar] [CrossRef] [PubMed]
- Gil, M.J.V.; Gonzalez-Medina, G.; Lucena-Anton, D.; Perez-Cabezas, V.; Ruiz-Molinero, M.D.C.; Martín-Valero, R. Augmented reality in physical therapy: Systematic review and meta-analysis. JMIR Serious Games 2021, 9, e30985. [Google Scholar]
- Toledo-Peral, C.L.; Vega-Martínez, G.; Mercado-Gutiérrez, J.A.; Rodríguez-Reyes, G.; Vera-Hernández, A.; Leija-Salas, L.; Gutiérrez-Martínez, J. Virtual/Augmented reality for rehabilitation applications using electromyography as control/biofeedback: Systematic literature review. Electronics 2022, 11, 2271. [Google Scholar] [CrossRef]
- Condino, S.; Turini, G.; Viglialoro, R.; Gesi, M.; Ferrari, V. Wearable augmented reality application for shoulder rehabilitation. Electronics 2019, 8, 1178. [Google Scholar] [CrossRef]
- Byra, J.; Czernicki, K. The effectiveness of virtual reality rehabilitation in patients with knee and hip osteoarthritis. J. Clin. Med. 2020, 9, 2639. [Google Scholar] [CrossRef]
- Ball, C.; Huang, K.T.; Francis, J. Virtual reality adoption during the COVID-19 pandemic: A uses and gratifications perspective. Telemat. Inform. 2021, 65, 101728. [Google Scholar] [CrossRef]
- Kamińska, D.; Zwoliński, G.; Laska-Leśniewicz, A.; Raposo, R.; Vairinhos, M.; Pereira, E.; Urem, F.; Ljubić Hinić, M.; Haamer, R.E.; Anbarjafari, G. Augmented Reality: Current and New Trends in Education. Electronics 2023, 12, 3531. [Google Scholar] [CrossRef]
- Ferraguti, F.; Minelli, M.; Farsoni, S.; Bazzani, S.; Bonfè, M.; Vandanjon, A.; Puliatti, S.; Bianchi, G.; Secchi, C. Augmented reality and robotic-assistance for percutaneous nephrolithotomy. IEEE Robot. Autom. Lett. 2020, 5, 4556–4563. [Google Scholar] [CrossRef]
- Ferraguti, F.; Farsoni, S.; Bonfè, M. Augmented reality and robotic systems for assistance in percutaneous nephrolithotomy procedures: Recent advances and future perspectives. Electronics 2022, 11, 2984. [Google Scholar] [CrossRef]
- Godfrey, A.; Hetherington, V.; Shum, H.; Bonato, P.; Lovell, N.; Stuart, S. From A to Z: Wearable technology explained. Maturitas 2018, 113, 40–47. [Google Scholar] [CrossRef]
- Capalbo, I.; Penhaker, M.; Peter, L.; Proto, A. Consumer perceptions on smart wearable devices for medical and wellness purposes. In Proceedings of the 2019 IEEE Technology & Engineering Management Conference (TEMSCON), Atlanta, GA, USA, 12–14 June 2019; pp. 1–6. [Google Scholar]
- Kaewkannate, K.; Kim, S. A comparison of wearable fitness devices. BMC Public Health 2016, 16, 433. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, S.M.; Nair, N.; Chen, P.; Dikker, S. Introducing EmotiBit, an open-source multi-modal sensor for measuring research-grade physiological signals. Sci. Talks 2023, 6, 100181. [Google Scholar] [CrossRef]
- Farsoni, S.; Rizzi, J.; Ufondu, G.N.; Bonfè, M. Planning Collision-Free Robot Motions in a Human-Robot Shared Workspace via Mixed Reality and Sensor-Fusion Skeleton Tracking. Electronics 2022, 11, 2407. [Google Scholar] [CrossRef]
- Mesquita, J.; Guimarães, D.; Pereira, C.; Santos, F.; Almeida, L. Assessing the ESP8266 WiFi module for the Internet of Things. In Proceedings of the 2018 IEEE 23rd International Conference on Emerging Technologies and Factory Automation (ETFA), Turin, Italy, 4–7 September 2018; Volume 1, pp. 784–791. [Google Scholar]
- Palumbo, A. Microsoft HoloLens 2 in medical and healthcare context: State of the art and future prospects. Sensors 2022, 22, 7709. [Google Scholar] [CrossRef]
- Linowes, J.; Babilinski, K. Augmented Reality for Developers: Build Practical Augmented Reality Applications with Unity, ARCore, ARKit, and Vuforia; Packt Publishing Ltd.: Birmingham, UK, 2017. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Emotibit | |
| Mean | Variance |
| 0.21 | 1.3359 × 10 |
| 0.58 | 1.1789 × 10 |
| 9.67 | 1.8610 × 10 |
| Custom IMU | |
| Mean | Variance |
| 0.1572 | 0.0022 |
| 0.6449 | 0.0039 |
| 9.6389 | 0.0022 |
| Questionnaire | |
|---|---|
| Categories | Questions |
| Level of expertise | (Q1) previous experience in using virtual/augmented reality devices. |
| Workload | (Q2) Evaluate the comfort of wearing the headset and wearable sensors during the exercise. (Q3) Rate the perceived well-being while using the AR app, i.e., lack of sensations of nausea, discomfort, or unease. |
| App usability | (Q4) Rate the usability of the APP. (Q5) Assess the interaction with AR element in the app. (Q6) Were the AR element easy to understand? (Q7) Evaluate the system performance in guiding the exercises. |
| Design | (Q8)Evaluate the AR app user interface design. (Q9) Evaluate the clarity of the feedback and notifications in the execution of the exercise. |
| Need for Instruction | (Q10) Did you require instructions or tutorials to use the app? |
| Overall satisfaction | (Q11) Rate your overall satisfaction with the proposed framework. |
| Questions | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Evaluations | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | |
| 1 | 4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| 2 | 3 | 0 | 1 | 3 | 5 | 0 | 0 | 0 | 0 | 2 | 0 | |
| 3 | 0 | 1 | 0 | 3 | 1 | 0 | 4 | 0 | 2 | 0 | 2 | |
| 4 | 3 | 8 | 2 | 3 | 2 | 4 | 6 | 8 | 4 | 3 | 7 | |
| 5 | 0 | 1 | 7 | 1 | 2 | 6 | 0 | 2 | 4 | 5 | 1 | |
| Comments and Suggestions | ||||||||||||
| (1) Improve the graphical interface; | ||||||||||||
| (2) Improve the repetition counter; | ||||||||||||
| (3) Improve the position of the avatar; | ||||||||||||
| (4) Making text larger for people with vision problems. | ||||||||||||
| Category | Question | Mean | Std Deviation |
|---|---|---|---|
| Expertise | Q1 | 2.2 | 1.31 |
| Workload | Q2 | 4.0 | 0.47 |
| Q3 | 4.5 | 0.97 | |
| Usability | Q4 | 3.2 | 1.04 |
| Q5 | 3.1 | 1.28 | |
| Q6 | 4.6 | 0.51 | |
| Q7 | 3.6 | 0.51 | |
| Design | Q8 | 4.2 | 0.42 |
| Q9 | 4.2 | 0.78 | |
| Instructions | Q10 | 4.1 | 1.19 |
| Satisfaction | Q11 | 3.9 | 0.56 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rizzi, J.; D’Antona, A.; Proto, A.; Piva, G.; Lamberti, N.; Bonfè, M.; Farsoni, S. A Framework Integrating Augmented Reality and Wearable Sensors for the Autonomous Execution of Rehabilitation Exercises. Electronics 2023, 12, 4958. https://doi.org/10.3390/electronics12244958
Rizzi J, D’Antona A, Proto A, Piva G, Lamberti N, Bonfè M, Farsoni S. A Framework Integrating Augmented Reality and Wearable Sensors for the Autonomous Execution of Rehabilitation Exercises. Electronics. 2023; 12(24):4958. https://doi.org/10.3390/electronics12244958
Chicago/Turabian StyleRizzi, Jacopo, Andrea D’Antona, Antonino Proto, Giovanni Piva, Nicola Lamberti, Marcello Bonfè, and Saverio Farsoni. 2023. "A Framework Integrating Augmented Reality and Wearable Sensors for the Autonomous Execution of Rehabilitation Exercises" Electronics 12, no. 24: 4958. https://doi.org/10.3390/electronics12244958