

Addressing Body Image Disturbance through Metaverse-Related Technologies: A Systematic Review

 and
and
Abstract
:1. Introduction
Metaverse-Related Technologies Use in ED
2. Materials and Methods
2.1. General Description
2.2. Selection Criteria
2.3. Outcomes
2.4. Search Methodology
2.5. Data Collection and Analysis
2.6. Data Extraction and Management
2.7. Quality of Studies Included
2.8. Statistical Analysis
3. Results
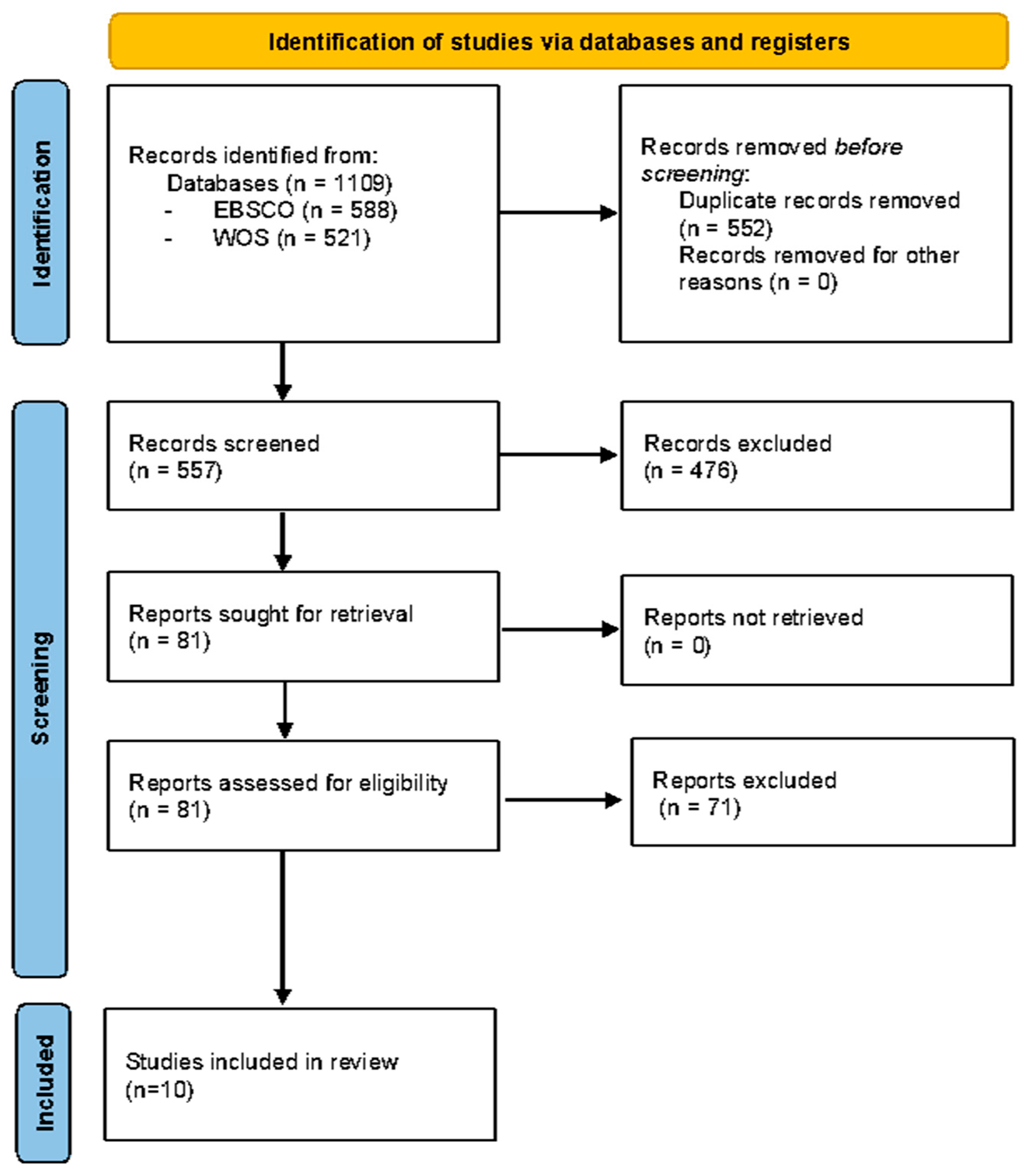
3.1. Study Selection and Inclusion
3.2. General Characteristics of the Studies Included
3.3. Assessment of Methodological Quality of Included Studies
3.4. Primary Outcomes
3.5. Secondary Outcomes
4. Discussion
4.1. Metaverse-Related Technologies Usefulness to Improve Body Image Disturbance for Patients Diagnosed with Anorexia or Bulimia Nervosa
4.2. Metaverse-Related Technologies Advantages to Improve Body Image Disturbance for Patients Diagnosed with Anorexia or Bulimia Nervosa
4.3. Patient’s Satisfaction after Using Metaverse-Related Technologies to Improve Body Image Disturbance
5. Conclusions
- (1)
- There is enough empirical evidence that supports the proposition that Metaverse-related technology is a promising tool to be used with patients diagnosed with AN and BN, in order to improve Body image distortion.
- (2)
- Considering the different Metaverse-related technology developed with AN and BN patients, it is crucial to address both the advantages and disadvantages highlighted earlier in order to successfully develop Metaverse strategies to improve body image disturbance.
- (3)
- Insufficient evidence exists in the literature regarding AN and BN patients’ satisfaction level, after using Metaverse-related technology to improve body image distortion.
5.1. Clinical and Researcher Implications
5.2. Limitations
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Méndez, J.P.; Vázquez-Velázquez, V.; García-García, E. Los trastornos de la conducta alimentaria. Medigraphic 2008, 65, 579–592. [Google Scholar]
- Lewinsohn, P.M.; Striegel-Moore, R.H.; Seeley, J.R. Epidemiology and natural course of eating disorders in young women from adolescence to young adulthood. J. Am. Acad. Child Adolesc. Psychiatry 2000, 39, 1284–1292. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Anorexia Nervosa. In Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; DSM-5; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar] [CrossRef]
- Sadock, B.J.; Ruiz, P.; Sadock, V.; Kaplan, H. Sinopsis de Psiquiatría: Ciencias de la Conducta, Psiquiatría Clínica; Wolter Kluwer: Alphen aan den Rijn, The Netherlands, 2015; pp. 962–980. [Google Scholar]
- Lindvall Dahlgren, C.; Wisting, L.; Rø, Ø. Feeding and eating disorders in the DSM-5 ERA: A systematic review of prevalence rates in non-clinical male and female samples. J. Eat. Disord. 2017, 5, 56. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.; Wu, Y.; Liu, F.; Zhu, Y.; Jin, H.; Zhang, H.; Wan, Y.; Li, C.; Yu, D. An update on the prevalence of eating disorders in the general population: A systematic review and meta-analysis. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2021, 27, 415–428. [Google Scholar] [CrossRef]
- Martínez-González, L.; Fernández-Villa, T.; Molina, A.J.; Delgado-Rodríguez, M.; Martín, V. Incidence of Anorexia nervosa in women: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 3824. [Google Scholar] [CrossRef] [PubMed]
- Garner, D.M. Body image and Anorexia nervosa. In Body Image: A Handbook of Theory, Research, and Clinical Practice; Cash, T.F., Pruzinsky, T., Eds.; Guilford Press: New York, NY, USA, 2002; pp. 295–303. [Google Scholar]
- Stice, E. Body image and Bulimia nervosa. In Body Image: A Handbook of Theory, Research, and Clinical Practice; Cash, T.F., Pruzinsky, T., Eds.; Guilford Press: New York, NY, USA, 2002; pp. 304–311. [Google Scholar]
- Schwartz, M.B.; Brownell, K.D. Obesity and body image. Body Image 2004, 1, 43–56. [Google Scholar] [CrossRef] [PubMed]
- Nye, S.; Cash, T.F. Outcomes of manualized cognitive-behavioral body image therapy with eating disordered women treated in a private clinical practice. Eat. Disord. 2006, 14, 31–40. [Google Scholar] [CrossRef]
- Rosen, J.C. Body-image disorder: Definition, development, and contribution to eating disorders. In The Etiology of Bulimia Nervosa: The Individual and Familial Context; Crowther, J.H., Ed.; Hemisphere: London, UK, 1992; pp. 157–172. [Google Scholar]
- Gleaves, D.H.; Williamson, D.A.; Barker, S.E. Confirmatory factor analysis of a multidimensional model of Bulimia nervosa. J. Abnorm. Psychol. 1993, 102, 173–176. [Google Scholar] [CrossRef]
- Stice, E.; E Shaw, H. Role of body dissatisfaction in the onset and maintenance of eating pathology. J. Psychosom. Res. 2002, 53, 985–993. [Google Scholar] [CrossRef]
- Pruzinsky, T.; Cash, T.F. Body Images: Development, Deviance, and Change; The Guilford Press: New York, NY, USA, 1991. [Google Scholar]
- Yamamotova, A.; Bulant, J.; Bocek, V.; Papezova, H. Dissatisfaction with own body makes patients with eating disorders more sensitive to pain. J. Pain Res. 2017, 10, 1667–1675. [Google Scholar] [CrossRef]
- Grogan, S. Body Image: Understanding Body Dissatisfaction in Men, Women and Children; Routledge, Taylor & Francis Group: Abingdon, UK, 2022. [Google Scholar]
- Garner, D.M.; Garfinkel, P.E. Body image in Anorexia nervosa: Measurement, theory and clinical implications. Int. J. Psychiatry Med. 1982, 11, 263–284. [Google Scholar] [CrossRef]
- Keeton, W.P.; Cash, T.; Brown, T. Body image or body images?: Comparative, Multidimensional Assessment among College Students. J. Personal. Assess. 1990, 54, 213–230. [Google Scholar] [CrossRef]
- Bergstrom, R.L.; Neighbors, C. Body image disturbance and the social norms approach: An Integrative Review of the literature. J. Soc. Clin. Psychol. 2006, 25, 975–1000. [Google Scholar] [CrossRef]
- Farrell, C.; Shafran, R.; Lee, M. Empirically evaluated treatments for Body image disturbance: A review. Eur. Eat. Disord. Rev. 2006, 14, 289–300. [Google Scholar] [CrossRef]
- Noles, S.W.; Cash, T.F.; Winstead, B.A. Body Image, Physical Attractiveness, and Depression. J. Consult. Clin. Psychol. 1985, 53, 88–94. [Google Scholar] [CrossRef]
- Rosen, J.C. Body image assessment and treatment in controlled studies of eating disorders. Int. J. Eat. Disord. 1996, 20, 331–343. [Google Scholar] [CrossRef]
- van Eeden, A.E.; van Hoeken, D.; Hoek, H.W. Incidence, prevalence and mortality of Anorexia nervosa and Bulimia nervosa. Curr. Opin. Psychiatry 2021, 34, 515–524. [Google Scholar] [CrossRef]
- Cieślik, B.; Mazurek, J.; Rutkowski, S.; Kiper, P.; Turolla, A.; Szczepańska-Gieracha, J. Virtual reality in psychiatric disorders: A systematic review of reviews. Complement. Ther. Med. 2020, 52, 102480. [Google Scholar] [CrossRef]
- Yang, Y.; Siau, K.; Xie, W.; Sun, Y. Smart health. J. Organ. End User Comput. 2022, 34, 1–14. [Google Scholar] [CrossRef]
- Almarzouqi, A.; Aburayya, A.; Salloum, S.A. Prediction of user’s intention to use metaverse system in medical education: A hybrid SEM-ml learning approach. IEEE Access 2022, 10, 43421–43434. [Google Scholar] [CrossRef]
- Tlili, A.; Huang, R.; Shehata, B.; Liu, D.; Zhao, J.; Metwally, A.H.S.; Wang, H.; Denden, M.; Bozkurt, A.; Lee, L.-H.; et al. Is metaverse in education a blessing or a curse: A combined content and bibliometric analysis. Smart Learn. Environ. 2022, 9, 24. [Google Scholar] [CrossRef]
- Kye, B.; Han, N.; Kim, E.; Park, Y.; Jo, S. Educational applications of metaverse: Possibilities and limitations. J. Educ. Eval. Health Prof. 2021, 18, 32. [Google Scholar] [CrossRef] [PubMed]
- An, A. Adopting metaverse-related mixed reality technologies to tackle Urban Development Challenges: An empirical study of an Australian municipal government. IET Smart Cities 2023, 5, 64–72. [Google Scholar] [CrossRef]
- Steuer, J. Defining virtual reality: Dimensions determining telepresence. J. Commun. 1992, 42, 73–93. [Google Scholar] [CrossRef]
- Al-Rasheed, A.; Alabdulkreem, E.; Alduailij, M.; Alduailij, M.; Alhalabi, W.; Alharbi, S.; Lytras, M.D. Virtual reality in the treatment of patients with overweight and obesity: A systematic review. Sustainability 2022, 14, 3324. [Google Scholar] [CrossRef]
- Riva, G.; Gaggioli, A. Virtual clinical therapy. In Digital Human Modeling; Springer: Berlin/Heidelberg, Germany, 2008; pp. 90–107. [Google Scholar]
- Pillai, A.S.; Mathew, P.S. Impact of Virtual Reality in Healthcare: A Review. In Virtual and Augmented Reality in Mental Health Treatment; IGI Global: Hershey, PA, USA, 2019; pp. 17–31. [Google Scholar] [CrossRef]
- Kohler, T.; Matzler, K.; Füller, J. Avatar-based Innovation: Using Virtual Worlds for real-world innovation. Technovation 2009, 29, 395–407. [Google Scholar] [CrossRef]
- Perpiñá, C.; Botella, C.; Baños, R.M. Virtual reality in eating disorders. Eur. Eat. Disord. Rev. 2003, 11, 261–278. [Google Scholar] [CrossRef]
- Ossolinski, G.; Jiwa, M.; McManus, A.; Parsons, R. Do images of a personalised future body shape help with weight loss? A randomised controlled study. Trials 2017, 18, 180. [Google Scholar] [CrossRef]
- Behm-Morawitz, E.; Lewallen, J.; Choi, G. A second chance at Health: How a 3D virtual world can improve health self-efficacy for weight loss management among adults. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 74–79. [Google Scholar] [CrossRef]
- Manzoni, G.M.; Cesa, G.L.; Bacchetta, M.; Castelnuovo, G.; Conti, S.; Gaggioli, A.; Mantovani, F.; Molinari, E.; Cárdenas-López, G.; Riva, G.; et al. Virtual reality–enhanced cognitive–behavioral therapy for morbid obesity: A randomized controlled study with 1 year follow-up. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 134–140. [Google Scholar] [CrossRef]
- Wiederhold, B.K. The Potential for Virtual Reality to Improve Health Care; The Virtual Reality Medical Centre (VRMC): San Diego, CA, USA, 2006. [Google Scholar]
- Baños, R.M.; Botella, C.; Tordera, C.P. Imagen Corporal en los Trastornos Alimentarios: Evaluación Y Tratamiento Mediante Realidad Virtual; Promolibro: Bogotá, Colombia, 2000. [Google Scholar]
- Preston, C.; Ehrsson, H.H. Implicit and explicit changes in body satisfaction evoked by body size illusions: Implications for eating disorder vulnerability in women. PLoS ONE 2018, 13, e0199426. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The Prisma 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Altman, D.G. Practical Statistics for Medical Research; CRC Press: Boca Raton, FL, USA, 1990. [Google Scholar]
- Pluye, P.; Gagnon, M.; Griffiths, F.; Johnson-Lafleur, J. A scoring system for appraising mixed methods research, and concomitantly appraising qualitative, quantitative and mixed methods primary studies in mixed studies reviews. Int. J. Nurs. Stud. 2009, 46, 529–546. [Google Scholar] [CrossRef] [PubMed]
- Hong, Q.N.; Pluye, P.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.; Griffiths, F.; Nicolau, B. Mixed Methods Appraisal Tool (MMAT), Version 2018. Registration of Copyright 2018. p. 1148552. Available online: http://mixedmethodsappraisaltoolpublic.pbworks.com/w/file/fetch/127916259/MMAT_2018_criteria-manual_2018-08-01_ENG.pdf (accessed on 30 July 2023).
- Porras-Garcia, B.; Ferrer-Garcia, M.; Serrano-Troncoso, E.; Carulla-Roig, M.; Soto-Usera, P.; Miquel-Nabau, H.; Shojaeian, N.; Santos-Carrasco, I.D.L.M.; Borszewski, B.; Díaz-Marsá, M.; et al. Validity of virtual reality body exposure to elicit fear of gaining weight, body anxiety and body-related attentional bias in patients with Anorexia nervosa. J. Clin. Med. 2020, 9, 3210. [Google Scholar] [CrossRef]
- Garcia, B.P.; Garcia, M.F.; Olszewska, A.; Yilmaz, L.; Ibañez, C.G.; Blanes, M.G.; Gültekin, G.; Troncoso, E.S.; Maldonado, J.G. Is this my own body? changing the perceptual and affective body image experience among college students using a new virtual reality embodiment-based technique. J. Clin. Med. 2019, 8, 925. [Google Scholar] [CrossRef] [PubMed]
- So, B.P.-H.; Lai, D.K.-H.; Cheung, D.S.-K.; Lam, W.-K.; Cheung, J.C.-W.; Wong, D.W.-C. Virtual reality-based immersive rehabilitation for cognitive- and behavioral-impairment-related eating disorders: A VREHAB framework scoping review. Int. J. Environ. Res. Public Health 2022, 19, 5821. [Google Scholar] [CrossRef]
- Buche, C.; Bigot, N.L. REVAM: A virtual reality application for inducing body size perception modifications. In Proceedings of the 2018 International Conference on Cyberworlds (CW), Singapore, 3–5 October 2018; pp. 229–236. [Google Scholar] [CrossRef]
- Butler, R.M.; Heimberg, R.G. Exposure therapy for eating disorders: A systematic review. Clin. Psychol. Rev. 2020, 78, 101851. [Google Scholar] [CrossRef]
- Ciążyńska, J.; Maciaszek, J. Various types of virtual reality-based therapy for eating disorders: A systematic review. J. Clin. Med. 2022, 11, 4956. [Google Scholar] [CrossRef]
- Purvis, C.K.; Jones, M.; Bailey, J.O.; Bailenson, J.; Taylor, C.B. Developing a novel measure of body satisfaction using virtual reality. PLoS ONE 2015, 10, e0140158. [Google Scholar] [CrossRef]
- Clus, D.; Larsen, M.E.; Lemey, C.; Berrouiguet, S. The use of virtual reality in patients with eating disorders: Systematic review. J. Med. Internet Res. 2018, 20, e157. [Google Scholar] [CrossRef]
- Corno, G.; Serino, S.; Cipresso, P.; Baños, R.M.; Riva, G. Assessing the relationship between attitudinal and perceptual component of body image disturbance using virtual reality. Cyberpsychol. Behav. Soc. Netw. 2018, 21, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Dascal, J.; Reid, M.; IsHak, W.W.; Spiegel, B.; Recacho, J.; Rosen, B.; Danovitch, I. Virtual reality and medical inpatients: A systematic review of randomized, controlled trials. Innov. Clin. Neurosci. 2017, 14, 14–21. [Google Scholar] [PubMed]
- De Carvalho, M.R.; Dias, T.R.d.S.; Duchesne, M.; Nardi, A.E.; Appolinario, J.C. Virtual reality as a promising strategy in the assessment and treatment of Bulimia nervosa and binge eating disorder: A systematic review. Behav. Sci. 2017, 7, 43. [Google Scholar] [CrossRef] [PubMed]
- Di Lernia, D.; Serino, S.; Tuena, C.; Cacciatore, C.; Polli, N.; Riva, G. Mental health meets computational neuroscience: A predictive bayesian account of the relationship between interoception and multisensory bodily illusions in Anorexia nervosa. Int. J. Clin. Health Psychol. 2023, 23, 100383. [Google Scholar] [CrossRef]
- Emmelkamp, P.M.; Meyerbröker, K. Virtual reality therapy in mental health. Annu. Rev. Clin. Psychol. 2021, 17, 495–519. [Google Scholar] [CrossRef] [PubMed]
- Feixas, G.; Alabèrnia-Segura, J. Technological contributions to psychotherapy: The potential of virtual reality. Rev. De Psicoter. 2021, 32, 81–93. [Google Scholar] [CrossRef]
- Ferrer-García, M.; Gutiérrez-Maldonado, J.; Pla-Sanjuanelo, J.; Vilalta-Abella, F.; Riva, G.; Clerici, M.; Ribas-Sabaté, J.; Andreu-Gracia, A.; Fernandez-Aranda, F.; Forcano, L.; et al. A randomised controlled comparison of second-level treatment approaches for treatment-resistant adults with Bulimia nervosa and binge eating disorder: Assessing the benefits of virtual reality cue exposure therapy. Eur. Eat. Disord. Rev. 2017, 25, 479–490. [Google Scholar] [CrossRef]
- Ferrer-Garcia, M.; Porras-Garcia, B.; Figueres-Puigderrajols, N.; Marnet, R.; Albarral, J.; Gutierrez-Maldonado, J. The BIAS-VR. assessing body image disturbance using a virtual reality software. preliminary results. Annu. Rev. Cybertherapy Telemed. 2020, 18, 257–260. [Google Scholar]
- Ferrer-Garcia, M.; Porras-Garcia, B.; Miquel, H.; Serrano-Troncoso, E.; Carulla-Roig, M.; Gutierrez-Maldonado, J. The way we look at our own body really matters! body-related attentional bias as a predictor of worse clinical outcomes after a virtual reality body exposure therapy. Annu. Rev. Cybertherapy Telemed. 2021, 19, 99–103. [Google Scholar]
- Ferrer-Garcia, M.; Porras-Garcia, B.; Moreno, M.; Bertomeu, P.; Maldonado, J.G. Embodiment in different size virtual bodies produces changes in women’s body image distortion and dissatisfaction. Annu. Rev. Cybertherapy Telemed. 2018, 16, 111–117. [Google Scholar]
- Ferrer-Garcia, M.; Gutiérrez-Maldonado, J.; Riva, G. Virtual reality based treatments in eating disorders and obesity: A review. J. Contemp. Psychother. 2013, 43, 207–221. [Google Scholar] [CrossRef]
- Ferrer-Garcia, M.; Pla-Sanjuanelo, J.; Dakanalis, A.; Vilalta-Abella, F.; Riva, G.; Fernandez-Aranda, F.; Forcano, L.; Riesco, N.; Sánchez, I.; Clerici, M.; et al. A randomized trial of virtual reality-based cue exposure second-level therapy and cognitive behavior second-level therapy for Bulimia nervosa and binge-eating disorder: Outcome at six-month followup. CyberPsychol. Behav. Soc. Netw. 2019, 22, 60–68. [Google Scholar] [CrossRef]
- Fisher, S.; Abdullah, A.; Charvin, I.; Da Fonseca, D.; Bat-Pitault, F. Comparison of body image evaluation by virtual reality and paper-based figure rating scales in adolescents with Anorexia nervosa: Retrospective study. Eat. Weight Disord. 2020, 25, 735–743. [Google Scholar] [CrossRef] [PubMed]
- Fonseca-Baeza, S.; Corno, G.; Banos, R.M. An intervention protocol proposal to modify the body image disturbance using virtual reality. Calid. De Vida Y Salud 2018, 11, 48–61. [Google Scholar]
- Meschberger-Annweiler, F.-A.; Ascione, M.; Porras-Garcia, B.; Ferrer-Garcia, M.; Moreno-Sanchez, M.; Miquel-Nabau, H.; Serrano-Troncoso, E.; Carulla-Roig, M.; Gutiérrez-Maldonado, J. An attentional bias modification task, through virtual reality and eye-tracking technologies, to enhance the treatment of Anorexia nervosa. J. Clin. Med. 2023, 12, 2185. [Google Scholar] [CrossRef]
- Freeman, D.; Reeve, S.; Robinson, A.; Ehlers, A.; Clark, D.; Spanlang, B.; Slater, M. Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol. Med. 2017, 47, 2393–2400. [Google Scholar] [CrossRef] [PubMed]
- Gadsby, S. Manipulating body representations with virtual reality: Clinical implications for Anorexia nervosa. Philos. Psychol. 2019, 32, 900–924. [Google Scholar] [CrossRef]
- Grochowska, A.; Wichniak, A.; Jarema, M. Virtual reality—A valuable tool to advance treatment of mental disorders. Arch. Psychiatry Psychother. 2019, 21, 65–73. [Google Scholar] [CrossRef]
- Gutiérrez-Maldonado, J. The use of virtual reality technology in the treatment of psychopathological disorders. J. Clin. Med. 2022, 11, 5358. [Google Scholar] [CrossRef]
- Gutiérrez-Maldonado, J.; Ferrer-García, M.; Riva, G. VR cue-exposure treatment for Bulimia nervosa. Stud. Health Technol. Inform. 2013, 191, 21–25. [Google Scholar] [CrossRef]
- Gutiérrez-Maldonado, J.; Pla-Sanjuanelo, J.; Ferrer-García, M. Cue-exposure software for the treatment of Bulimia nervosa and binge eating disorder. Psicothema 2016, 28, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Maldonado, J.; Wiederhold, B.K.; Riva, G. Future directions: How virtual reality can further improve the assessment and treatment of eating disorders and obesity. CyberPsychol. Behav. Soc. Netw. 2016, 19, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Miquel-Nabau, H.; Briseño-Oloriz, N.; Porras-Garcia, B.; Ascione, M.; Meschberger-Annweiler, F.-A.; Ferrer-Garcia, M.; Moreno-Sanchez, M.; Serrano-Troncoso, E.; Carulla-Roig, M.; Maldonado, J.G. Modification of body-related attentional bias through virtual reality and eye-tracking in healthy participants: Implications for Anorexia nervosa treatments. Brain Sci. 2023, 13, 764. [Google Scholar] [CrossRef]
- Hudson, G.M.; Lu, Y.; Zhang, X.; Hahn, J.; Zabal, J.E.; Latif, F.; Philbeck, J. The development of a BMI-guided shape morphing technique and the effects of an individualized figure rating scale on self-perception of body size. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 579–594. [Google Scholar] [CrossRef]
- Kim, S.; Kim, E. The use of virtual reality in psychiatry: A review. J. Korean Acad. Child Adolesc. Psychiatry 2020, 31, 26–32. [Google Scholar] [CrossRef]
- Koskina, A.; Campbell, I.C.; Schmidt, U. Exposure therapy in eating disorders revisited. Neurosci. Biobehav. Rev. 2013, 37, 193–208. [Google Scholar] [CrossRef]
- Kothgassner, O.D.; Reichmann, A.; Bock, M.M. Virtual reality interventions for mental health. In Current Topics in Behavioral Neuroscience; Springer: Berlin/Heidelberg, Germany, 2023. [Google Scholar] [CrossRef]
- Lafond, E.; Riva, G.; Gutierrez-Maldonado, J.; Wiederhold, B.K. Eating disorders and obesity in virtual reality: A comprehensive research chart. CyberPsychol. Behav. Soc. Netw. 2016, 19, 141–147. [Google Scholar] [CrossRef]
- Langer, Á.I.; Aguilar-Parra, J.; Ulloa, V.G.; Carmona-Torres, J.; Cangas, A.J. Substance use, bullying, and body image disturbances in adolescents and young adults under the prism of a 3D simulation program: Validation of MySchool4web. Telemed. E-Health 2016, 22, 18–30. [Google Scholar] [CrossRef] [PubMed]
- Langlet, B.S.; Odegi, D.; Zandian, M.; Nolstam, J.; Södersten, P.; Bergh, C. Virtual reality app for treating eating behavior in eating disorders: Development and usability study. JMIR Serious Games 2021, 9, e24998. [Google Scholar] [CrossRef] [PubMed]
- Lanning, M.; Shen, J.; Wasser, D.; Riddle, S.; Agustin, B.; Hood, K.; Naranjo, D. Exposure to closed loop barriers using virtual reality. J. Diabetes Sci. Technol. 2020, 14, 837–843. [Google Scholar] [CrossRef] [PubMed]
- Lemieux, V.; Monthuy-Blanc, J.; Corno, G. Application of virtual reality in an ED primary prevention context: An exploratory study. Annu. Rev. Cybertherapy Telemed. 2020, 18, 207–211. [Google Scholar]
- Liu, T.; Pietschmann, D.; Ohler, P. Affecting explicit and implicit body image with thin-idealized avatars in virtual reality: The role of sense of embodiment. CyberPsychology Behav. Soc. Netw. 2022, 25, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Magrini, M.; Curzio, O.; Tampucci, M.; Donzelli, G.; Cori, L.; Imiotti, M.C.; Maestro, S.; Moroni, D. Anorexia nervosa, body image perception and virtual reality therapeutic applications: State of the art and operational proposal. Int. J. Environ. Res. Public Health 2022, 19, 2533. [Google Scholar] [CrossRef] [PubMed]
- Malighetti, C.; Sansoni, M.; Gaudio, S.; Matamala-Gomez, M.; Di Lernia, D.; Serino, S.; Riva, G. From virtual reality to regenerative virtual therapy: Some insights from a systematic review exploring inner body perception in anorexia and Bulimia nervosa. J. Clin. Med. 2022, 11, 7134. [Google Scholar] [CrossRef]
- Malighetti, C.; Schnitzer, C.; Potter, G.; Nameth, K.; Brown, T.; Vogel, E.; Riva, G.; Runfola, C.; Safer, D. Rescripting emotional eating with virtual reality: A case study. Annu. Rev. Cybertherapy Telemed. 2021, 19, 117–121. [Google Scholar]
- Mölbert, S.C.; Thaler, A.; Mohler, B.J.; Streuber, S.; Romero, J.; Black, M.J.; Zipfel, S.; Karnath, H.-O.; Giel, K.E. Assessing body image in Anorexia nervosa using biometric self-avatars in virtual reality: Attitudinal components rather than visual body size estimation are distorted. Psychol. Med. 2018, 48, 642–653. [Google Scholar] [CrossRef]
- Monthuy-Blanc, J.; Bouchard, S.; Ouellet, M.; Corno, G.; Iceta, S.; Rousseau, M. “eLoriCorps immersive body rating scale”: Exploring the assessment of body image disturbances from allocentric and egocentric perspectives. J. Clin. Med. 2020, 9, 2926. [Google Scholar] [CrossRef] [PubMed]
- Mountford, V.A.; Tchanturia, K.; Valmaggia, L. “What are you thinking when you look at me?” A pilot study of the use of virtual reality in body image. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 93–99. [Google Scholar] [CrossRef]
- Döllinger, N.; Wolf, E.; Mal, D.; Wenninger, S.; Botsch, M.; Latoschik, M.E.; Wienrich, C. Resize me! exploring the user experience of embodied realistic modulatable avatars for body image intervention in virtual reality. Front. Virtual Real. 2022, 3, 935449. [Google Scholar] [CrossRef]
- Osumi, M.; Imai, R.; Ueta, K.; Nobusako, S.; Morioka, S. Negative body image associated with changes in the visual body appearance increases pain perception. PLoS ONE 2014, 9, e107376. [Google Scholar] [CrossRef]
- Péresmitré, G.G.; Hernández, R.L.; Acevedo, S.P.; Hernández, M.L.; Cruz, D.; Alcántara, A.H. Virtual reality and psychoeducation. selective prevention formats in eating disorders. Rev. Mex. Trastor. Aliment. 2013, 4, 23–30. [Google Scholar] [CrossRef]
- Perpiñá, C.; Roncero, M. Similarities and differences between eating disorders and obese patients in a virtual environment for normalizing eating patterns. Compr. Psychiatry 2016, 67, 39–45. [Google Scholar] [CrossRef]
- Perpiñá, C.; Roncero, M.; Fernández-Aranda, F.; Jiménez-Murcia, S.; Forcano, L.; Sánchez, I. Clinical validation of a virtual environment for normalizing eating patterns in eating disorders. Compr. Psychiatry 2013, 54, 680–686. [Google Scholar] [CrossRef]
- Piryankova, I.V.; Stefanucci, J.K.; Romero, J.; De La Rosa, S.; Black, M.J.; Mohler, B.J. Can I recognize my body’s weight? the influence of shape and texture on the perception of self. ACM Trans. Appl. Percept. 2014, 11, 1–18. [Google Scholar] [CrossRef]
- Piryankova, I.V.; Wong, H.Y.; Linkenauger, S.A.; Stinson, C.; Longo, M.R.; Bülthoff, H.H.; Mohler, B.J. Owning an overweight or underweight body: Distinguishing the physical, experienced and virtual body. PLoS ONE 2014, 9, e103428. [Google Scholar] [CrossRef]
- Pla-Sanjuanelo, J.; Ferrer-Garcia, M.; Vilalta-Abella, F.; Gutierrez-Maldonado, J.; Andreu-Gracia, A.; Dakanalis, A.; Escandon-Nagel, N.; Fernandez-Aranda, F.; Gomez-Tricio, O.; Ribas-Sabate, J.; et al. Using virtual reality for cue-exposure therapy in a case of Bulimia nervosa. Annu. Rev. Cybertherapy Telemed. 2016, 14, 155–160. [Google Scholar]
- Pla-Sanjuanelo, J.; Ferrer-García, M.; Vilalta-Abella, F.; Riva, G.; Dakanalis, A.; Ribas-Sabaté, J.; Andreu-Gracia, A.; Fernandez-Aranda, F.; Sanchez-Diaz, I.; Escandón-Nagel, N.; et al. Testing virtual reality-based cue-exposure software: Which cue-elicited responses best discriminate between patients with eating disorders and healthy controls? Eat. Weight Disord. 2019, 24, 757–765. [Google Scholar] [CrossRef]
- Popescu, L. Image editing tools for visually appealing self-presentations: Digitally mediated social presence, body dissatisfaction and shame, and ideal beauty standards. J. Res. Gend. Stud. 2022, 12, 48–62. [Google Scholar] [CrossRef]
- Porras-Garcia, B.; Singh, A.; Miquel, H.; Tana-Velasco, G.; Briseno-Oloriz, N.; Fleta-Diaz, J.; Iglesias, E.; Ferrer-Garcia, M.; Gutierrez-Maldonado, J. Going beyond body exposure therapy. presenting an innovative virtual reality and EyeTracking body-related attentional bias task. Annu. Rev. Cybertherapy Telemed. 2021, 19, 93–97. [Google Scholar]
- Porras-Garcia, B.; Ferrer-Garcia, M.; Yilmaz, L.; Sen, Y.O.; Olszewska, A.; Ghita, A.; Serrano-Troncoso, E.; Treasure, J.; Gutiérrez-Maldonado, J. Body-related attentional bias as mediator of the relationship between body mass index and body dissatisfaction. Eur. Eat. Disord. Rev. J. Eat. Disord. Assoc. 2020, 28, 454–464. [Google Scholar] [CrossRef]
- Riva, G.; Dakanalis, A. Altered processing and integration of multisensory bodily representations and signals in eating disorders: A possible path toward the understanding of their underlying causes. Front. Hum. Neurosci. 2018, 12, 49. [Google Scholar] [CrossRef]
- Serino, S.; Dakanalis, A.; Gaudio, S.; Carrà, G.; Cipresso, P.; Clerici, M.; Riva, G. Out of body, out of space: Impaired reference frame processing in eating disorders. Psychiatry Res. 2015, 230, 732–734. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, L.; Roy-Vaillancourt, M.; Chebbi, B.; Bouchard, S.; Daoust, M.; Dénommée, J.; Thorpe, M. Body image and anti-fat attitudes: An experimental study using a haptic virtual reality environment to replicate human touch. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 100–106. [Google Scholar] [CrossRef]
- Tremblay, L.; Chebbi, B.; Bouchard, S. The predictive role of body image and anti-fat attitudes on attentional bias toward body area in haptic virtual reality environment. Virtual Real. 2022, 26, 333–342. [Google Scholar] [CrossRef]
- Turbyne, C.; Goedhart, A.; de Koning, P.; Schirmbeck, F.; Denys, D. Systematic review and meta-analysis of virtual reality in mental healthcare: Effects of full body illusions on body image disturbance. Front. Virtual Real. 2021, 2, 657638. [Google Scholar] [CrossRef]
- Turnbull, G.; Alexi, J.; Mann, G.; Li, Y.; Engel, M.; Bayliss, D.M.; Farrell, S.; Bell, J. The influence of three-dimensional cues on body size judgements. Q. J. Exp. Psychol. 2022, 75, 2318–2331. [Google Scholar] [CrossRef]
- Turnbull, G.; Lego, S.; Kennedy, B.L.; Alexi, J.; Li, Y.R.; Engel, M.M.; Mann, G.; Bayliss, D.M.; Farrell, S.; Bell, J. Sizing up the crowd: Assessing spatial integration difficulties in body size judgements across eating disorder symptomatology. Front. Psychol. 2023, 13, 1003250. [Google Scholar] [CrossRef]
- Varlamov, A.V.; Yakovleva, N.V. Distortions of body perception during immersion in computer virtual reality using full-body tracking. RUDN J. Psychol. Pedagog. 2022, 19, 670–688. [Google Scholar] [CrossRef]
- Weber, S.; Mast, F.W.; Weibel, D. Body size illusions influence perceived size of objects: A validation of previous research in virtual reality. Virtual Real. 2020, 24, 385–397. [Google Scholar] [CrossRef]
- Ziser, K.; Mölbert, S.C.; Stuber, F.; Giel, K.E.; Zipfel, S.; Junne, F. Effectiveness of body image directed interventions in patients with Anorexia nervosa: A systematic review. Int. J. Eat. Disord. 2018, 51, 1121–1127. [Google Scholar] [CrossRef]
- Behrens, S.C.; Tesch, J.; Sun, P.J.; Starke, S.; Black, M.J.; Schneider, H.; Pruccoli, J.; Zipfel, S.; Giel, K.E. Virtual reality exposure to a healthy weight body is a promising adjunct treatment for Anorexia nervosa. Psychother. Psychosom. 2023, 92, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Porras-Garcia, B.; Serrano-Troncoso, E.; Carulla-Roig, M.; Soto-Usera, P.; Ferrer-Garcia, M.; Figueras-Puigderrajols, N.; Yilmaz, L.; Sen, Y.O.; Shojaeian, N.; Gutiérrez-Maldonado, J. Virtual reality body exposure therapy for Anorexia nervosa. A case report with follow-up results. Front. Psychol. 2020, 11, 956. [Google Scholar] [CrossRef] [PubMed]
- Porras-Garcia, B.; Ferrer-Garcia, M.; Serrano-Troncoso, E.; Carulla-Roig, M.; Soto-Usera, P.; Miquel-Nabau, H.; Olivares, L.F.-D.C.; Marnet-Fiol, R.; Santos-Carrasco, I.d.l.M.; Borszewski, B.; et al. An-VR-be. A randomized controlled trial for reducing fear of gaining weight and other eating disorder symptoms in Anorexia nervosa through virtual reality-based body exposure. J. Clin. Med. 2021, 10, 682. [Google Scholar] [CrossRef]
- Keizer, A.; van Elburg, A.; Helms, R.; Dijkerman, H.C. A virtual reality full body illusion improves body image disturbance in Anorexia nervosa. PLoS ONE 2016, 11, e0163921. [Google Scholar] [CrossRef]
- Malighetti, C.; Chirico, A.; Serino, S.; Cavedoni, S.; Matamala-Gomez, M.; Stramba-Badiale, C.; Mancuso, V.; Corno, G.; Polli, N.; Cacciatore, C.; et al. Manipulating body size distortions and negative body-related memories in patients with Anorexia nervosa: A virtual reality-based pilot study. Annu. Rev. Cybertherapy Telemed. 2020, 18, 177–181. [Google Scholar]
- Marco, J.H.; Perpiñá, C.; Botella, C. Effectiveness of cognitive behavioral therapy supported by virtual reality in the treatment of body image in eating disorders: One year follow-up. Psychiatry Res. 2013, 209, 619–625. [Google Scholar] [CrossRef]
- Porras-Garcia, B.; Serrano-Troncoso, E.; Carulla-Roig, M.; Soto-Usera, P.; Ferrer-Garcia, M.; Olivares, L.; Figueras-Puigderrajols, N.; Santos-Carrasco, I.D.; Borszewski, B.; Diaz-Marsa, M.; et al. Targeting the fear of gaining weight and body-related concerns in Anorexia nervosa. preliminary findings from a virtual reality randomized clinical trial. Annu. Rev. Cybertherapy Telemed. 2020, 18, 223–227. [Google Scholar]
- Porras-Garcia, B.; Ferrer-García, M.; Serrano-Troncoso, E.; Carulla-Roig, M.; Soto-Usera, P.; Fernández-Del Castillo Olivares, L.; Figueras-Puigderajols, N.; Gutiérrez-Maldonado, J.; Virtual reality body exposure therapy for Anorexia nervosa. A single case study. In Proceedings of the HCI International 2020-Posters: 22nd International Conference, HCII 2020, Copenhagen, Denmark, 19–24 July 2020; Proceedings, Part II 22. Springer International Publishing: Berlin/Heidelberg, Germany, 2020; pp. 108–115. [Google Scholar]
- Provenzano, L.; Porciello, G.; Ciccarone, S.; Lenggenhager, B.; Tieri, G.; Marucci, M.; Dazzi, F.; Loriedo, C.; Bufalari, I. Characterizing body image distortion and bodily self-plasticity in Anorexia nervosa via visuo-tactile stimulation in virtual reality. J. Clin. Med. 2020, 9, 98. [Google Scholar] [CrossRef]
- Serino, S.; Polli, N.; Riva, G. From avatars to body swapping: The use of virtual reality for assessing and treating body-size distortion in individuals with anorexia. J. Clin. Psychol. 2019, 75, 313–322. [Google Scholar] [CrossRef]
- Mountford, V.; Haase, A.; Waller, G. Body checking in the eating disorders: Associations between cognitions and behaviors. Int. J. Eat. Disord. 2006, 39, 708–715. [Google Scholar] [CrossRef]
- Clement, U.; Löwe, B. Body Image Questionnaire (BIQ-20), Manual with Questionnaire and Assessment Tools; GöttingenHogrefe: Göttingen, Germany, 1996. [Google Scholar]
- Cruz, S.; Maganto, C. El test de las siluetas: Un estudio exploratorio de la distorsión e insatisfacción con la imagen corporal en adolescentes. Rev. Inst. Investig. Fac. Psicol. 2003, 8, 79–99. [Google Scholar]
- Reed, D.L.; Thompson, J.K.; Brannick, M.T.; Sacoo, W.P. Development and validation of the physical appearance state and trait anxiety Scale (PASTAS). J. Anxiety Disord. 1991, 5, 323–332. [Google Scholar] [CrossRef]
- Lobera, I.J.; Ríos, P.B. Spanish Version of the Body Appreciation Scale (BAS) for Adolescents. Span. J. Psychol. 2011, 14, 411–420. [Google Scholar] [CrossRef]
- Garner, D. Eating Disorder Inventory-3: Professional Manual; Psychological Assessment Resources: Lutz, FL, USA, 2004. [Google Scholar]
- Gardner, R.M.; Jappe, L.M.; Gardner, L. Development and validation of a new figural drawing scale for body-image assessment: The BIAS-BD. J. Clin. Psychol. 2009, 65, 113–122. [Google Scholar] [CrossRef]
- Stefanile, C.; Matera, C.; Pisani, E. Pisani, Body Shape Questionnaire (BSQ-14): An Italian version. J. Eat. Disord. 2009, 6, 485–494. [Google Scholar]
- Slade, P.D.; Dewey, M.E.; Newton, T.; Brodie, D.; Kiemle, G. Development and preliminary validation of the Body Satisfaction Scale (BSS). Psychol. Health 1990, 4, 213–220. [Google Scholar] [CrossRef]
- Cash, T.F.; Lewis, R.J.; Keeton, P. Development and validation of the Body-Image Automatic Thoughts Questionnaire: A measure of body-related cognitions. In Proceedings of the Meeting of the Southeastern Psychological Association, Atlanta, GA, USA, 25–28 March 1987. [Google Scholar]
- Probst, M.; Vandereycken, W.; Coppenolle, H.V.; Vanderlinden, J. The Body Attitude Test for patients with an eating disorder: Psychometric characteristics of a new questionnaire. Eat. Disord. 1995, 3, 133–144. [Google Scholar]
- Cash, T.F. Body Image Therapy: A Program for Selfdirected Change; Guilford Press: New York, NY, USA, 1991. [Google Scholar]
- Cash, T.F. The situational inventory of body- image dysphoria: Contextual assessment of a negative body image. Behav. Ther. 1994, 17, 133–134. [Google Scholar]
- Perpiñá, C.; Baños, R.; Botella, C.; Marco, J.H. La realidad virtual como herramienta terapéutica: Un estudio de caso en las alteraciones de la imagen corporal en los trastornos alimentarios. Rev. Argent. De Clínica Psicológica 2001, 10, 227–241. [Google Scholar]
- Perpiñá, C.; Botella, C.; Baños, R.; Marco, J.H.; Alcañiz, M.; Quero, S. Body Image and virtual reality in eating disorders: Exposure by virtual reality is more effective than the classical body image treatment? Cyberpsychol. Behav. 1999, 2, 149–159. [Google Scholar] [CrossRef]
- Perpiñá, C.; Marco, J.H.; Botella, C.; Baños, R. Tratamiento de la Imagen Corporal en los trastornos alimentarios mediante tratamiento cognitivocomportamental apoyado con realidad virtual: Resultados al año de seguimiento. Psicol. Conduct. 2004, 12, 519–537. [Google Scholar]
- Riva, G.; Bacchetta, M.; Baruffi, M.; Rinaldi, S.; Vincelli, F.Y.; Molinari, E. Virtual reality-based experiential cognitive treatment of obesity and binge-eating disorders. Clin. Psychol. Psychother. 2000, 7, 209–219. [Google Scholar] [CrossRef]
- Ferrer-García, M.; Gutiérrez-Maldonado, J. The use of virtual reality in the study, assessment, and treatment of body image in eating disorders and nonclinical samples: A review of the literature. Body Image 2012, 9, 1–11. [Google Scholar] [CrossRef]
- Nichols, S.; Patel, H. Health and safety implications of virtual reality: A review of empirical evidence. Appl. Ergon. 2002, 33, 251–271. [Google Scholar] [CrossRef] [PubMed]
- Woolley, F.; Kane, R.L.; Hughes, C.C.; Wright, D.D. The effects of doctor-patient communication on satisfac-tion and outcome of care. Soc. Sci. Med. Part A Med. Psychol. Med. Sociol. 1978, 12, 123–128. [Google Scholar] [CrossRef]
- Matsangidou, M.; Otkhmezuri, B.; Ang, C.S.; Avraamides, M.; Riva, G.; Gaggioli, A.; Iosif, D.; Karekla, M. “Now i can see me” designing a multi-user virtual reality remote psychotherapy for body weight and shape concerns. Hum.–Comput. Interact. 2022, 37, 314–340. [Google Scholar] [CrossRef]
- Ma, L.; Mor, S.; Anderson, P.L.; Baños, R.M.; Botella, C.; Bouchard, S.; Cárdenas-López, G.; Donker, T.; Fernández-Álvarez, J.; Lindner, P. Integrating virtual realities and psychotherapy: SWOT analysis on VR and MR based treatments of anxiety and stress-related disorders. Cogn. Behav. Ther. 2021, 50, 509–526. [Google Scholar] [CrossRef] [PubMed]
- Booth, A.; Clarke, M.; Dooley, G.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. The nuts and bolts of PROSPERO: An international prospective register of systematic reviews. Syst. Rev. 2012, 1, 2. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Publication Year | Country | Study Design |
|---|---|---|---|
| Behrens et al. [116] | 2023 | Germany | Quantitative |
| Porras-Garcia et al. [117] | 2020 | Spain | Quantitative |
| Porras-Garcia et al. [118] | 2021 | Spain | Quantitative |
| Keizer et al. [119] | 2016 | Netherlands | Quantitative |
| Malighetti et al. [120] | 2021 | Italy | Quantitative |
| Marco et al. [121] | 2013 | Spain | Quantitative |
| Porras-Garcia et al. [122] | 2020 | Spain | Quantitative |
| Porras-Garcia et al. [123] | 2020 | Spain | Quantitative |
| Provenzano et al. [124] | 2020 | Italy | Quantitative |
| Serino et al. [125] | 2019 | Italy | Quantitative |
| Study | Study Aim | Sample Size (Mean Age) | Eating Disorder | Body Image Disturbance Tested |
|---|---|---|---|---|
| Behrens et al. [116] | To evaluate the usefulness of VR exposure to a healthy body | CG: 20(26.36) EG: 20(30.1) | EG: AN; GC: No AN | Cognitive/Perceptual/Affective |
| Porras-Garcia et al. [117] | To evaluate the effectiveness of VR body exposure therapy as adjunct treatment | 1(15) | AN | Cognitive/Perceptual/Affective |
| Porras-Garcia et al. [118] | To evaluate the effectiveness of VR body exposure therapy to reduce fear of weight gain and other ED symptoms | 35(NP) | EG: AN; GC: No AN | Cognitive/Perceptual/Affective |
| Keizer et al. [119] | To investigate whether a Full-Body Illusion (FBI) in VR affects body size estimation | 59(NP) | EG: AN; GC: No AN | Perceptive |
| Malighetti et al. [120] | To use VR to modify body image distortions and negative body-related memories | 7(17) | AN | Cognitive/Perceptual/Affective |
| Marco et al. [121] | To evaluate the effectiveness of cognitive behavioral therapy (CBT) supported by VR in body image treatment | 32(21.82) | AN/BN | Cognitive/Affective |
| Porras-Garcia et al. [122] | To evaluate the usefulness of VR body exposure therapy in AN treatment | 17(NP) | EG:AN; GC: No AN | Perceptual/Affective |
| Porras-Garcia et al. [123] | To evaluate the usefulness of VR body exposure therapy in AN treatment | 1(14) | AN | Cognitive/Perceptual/Affective |
| Provenzano et al. [124] | To use VR to characterize and reduce body image distortion | 40(23.6) | EG:AN; GC: No AN | Affective |
| Serino et al. [125] | To report on the use of VR using Full-Body Illusion as part of a multidisciplinary treatment | 1(NP) | AN | Perceptual |
| Study | Training Using Metaverse-Related Technologies | Metaverse-Related Technology Used | Useful to Improve Body Image Disturbance | Questionnaire Used |
|---|---|---|---|---|
| Behrens et al. [116] | In four VR sessions, participants were exposed to a healthy BMI, measuring different aspects of Body Image Distortion before and after each session. | VR (Valve Index—VIVE) | No | BCCS y FKB-20 [126,127] |
| Porras-Garcia et al. [117] | A virtual avatar was created, that gradually increased its BMI over five sessions, discontinuing when the patient’s body anxiety decreased by 40% during a measurement 5 months later. | VR (HMD-HTC-VIVE) | Yes | HMD Fove Eye Tracking, TSA-D, PASTAS y VAS-A [128,129] |
| Porras-Garcia et al. [118] | Patients were evaluated before, 5 weeks after and at a 3-month follow-up. The experimental group received VR body exposure along with CBT, assessing anxiety during the sessions. | VR (HTC-VIVE HMD) | Yes | FOVE VR-HMD, BAS, EDI-BD, PASTAS & BIAS-BD [129,130,131,132] |
| Keizer et al. [119] | In a split-group trial, the VR Full-Body Illusion was applied, and the body perception and estimation were assessed before, during and after exposure to an avatar. | VR (Oculus Rift DK2) | Yes | Analog measurements |
| Malighetti et al. [120] | Full Body Illusion was induced with VR, assessing body image and estimates of actual and ideal size before and after exposure. | VR (NP) | Yes | BSQ, BSS and VR Body Size Estimation Task [133,134] |
| Marco et al. [121] | CBT was combined with VR intervention, assessing different aspects of Body Image Distortion before and after treatment, and one year later. | VR (V6 de Virtual Research) | Yes | BIATQ, BAT, BASS & SIBID [135,136,137,138] |
| Porras-Garcia et al. [122] | In a controlled trial, CBT was combined with five sessions of VR body exposure therapy, assessing multiple components of body image before and after treatment. | VR (HTC-VIVE) | Yes | VR HMD FOVE, BIAS-BD, BIAS-X, EDI-BD, PASTAS &BIAS-O [129,131,132] |
| Porras-Garcia et al. [123] | During five sessions, a patient was exposed to an avatar with VR that gradually increased her BMI, evaluating different aspects of body image and reducing anxiety by 40%. | VR (HMD-HTC-VIVE) | Yes | TSA-BD, TSA-D, EDI-BD & PASTAS [128,129,131] |
| Provenzano et al. [124] | Using VR and the Full Body Image Illusion, participants were exposed to avatars of different sizes and their emotional responses and degree of attraction to these avatars were assessed. | VR (Oculus Rift Developers Kit Dk1) | No | Not Provided (indirect measurements used) |
| Serino et al. [125] | The ability of VR to improve a patient’s body perception was evaluated by comparing actual measurements with estimations in three sessions using different visuotactile stimulation conditions in Full Body Illusion. | VR (HMD-Oculus Rift DK2) | Yes | Not Provided (analog measurements used) |
| Study | Main Advantages and Disadvantages | Patient’s Satisfaction |
|---|---|---|
| Behrens et al. [116] | Yes | Yes |
| Porras-Garcia et al. [117] | Yes | Yes |
| Porras-Garcia et al. [118] | Yes | Not provided |
| Keizer et al. [119] | Yes | Not provided |
| Malighetti et al. [120] | Yes | Not provided |
| Marco et al. [121] | Yes | Not provided |
| Porras-Garcia et al. [122] | Yes | Not provided |
| Porras-Garcia et al. [123] | Yes | Not provided |
| Provenzano et al. [124] | Yes | Not provided |
| Serino et al. [125] | Yes | Not provided |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perez, M.; Pineda-Rafols, A.; Egea-Romero, M.P.; Gonzalez-Moreno, M.; Rincon, E. Addressing Body Image Disturbance through Metaverse-Related Technologies: A Systematic Review. Electronics 2023, 12, 4580. https://doi.org/10.3390/electronics12224580
Perez M, Pineda-Rafols A, Egea-Romero MP, Gonzalez-Moreno M, Rincon E. Addressing Body Image Disturbance through Metaverse-Related Technologies: A Systematic Review. Electronics. 2023; 12(22):4580. https://doi.org/10.3390/electronics12224580
Chicago/Turabian StylePerez, Moises, Adriana Pineda-Rafols, Maria Pilar Egea-Romero, Maria Gonzalez-Moreno, and Esther Rincon. 2023. "Addressing Body Image Disturbance through Metaverse-Related Technologies: A Systematic Review" Electronics 12, no. 22: 4580. https://doi.org/10.3390/electronics12224580