
Integrated Equipment for Parkinson’s Disease Early Detection Using Graph Convolution Network



Abstract
:
1. Introduction
- We present the world’s first Parkinson patients’ gait dataset PD-Walk, which consists of 191 people’s walking videos (with extracted skeletons). It is worth mentioning that all the data were annotated by doctors from top hospitals.
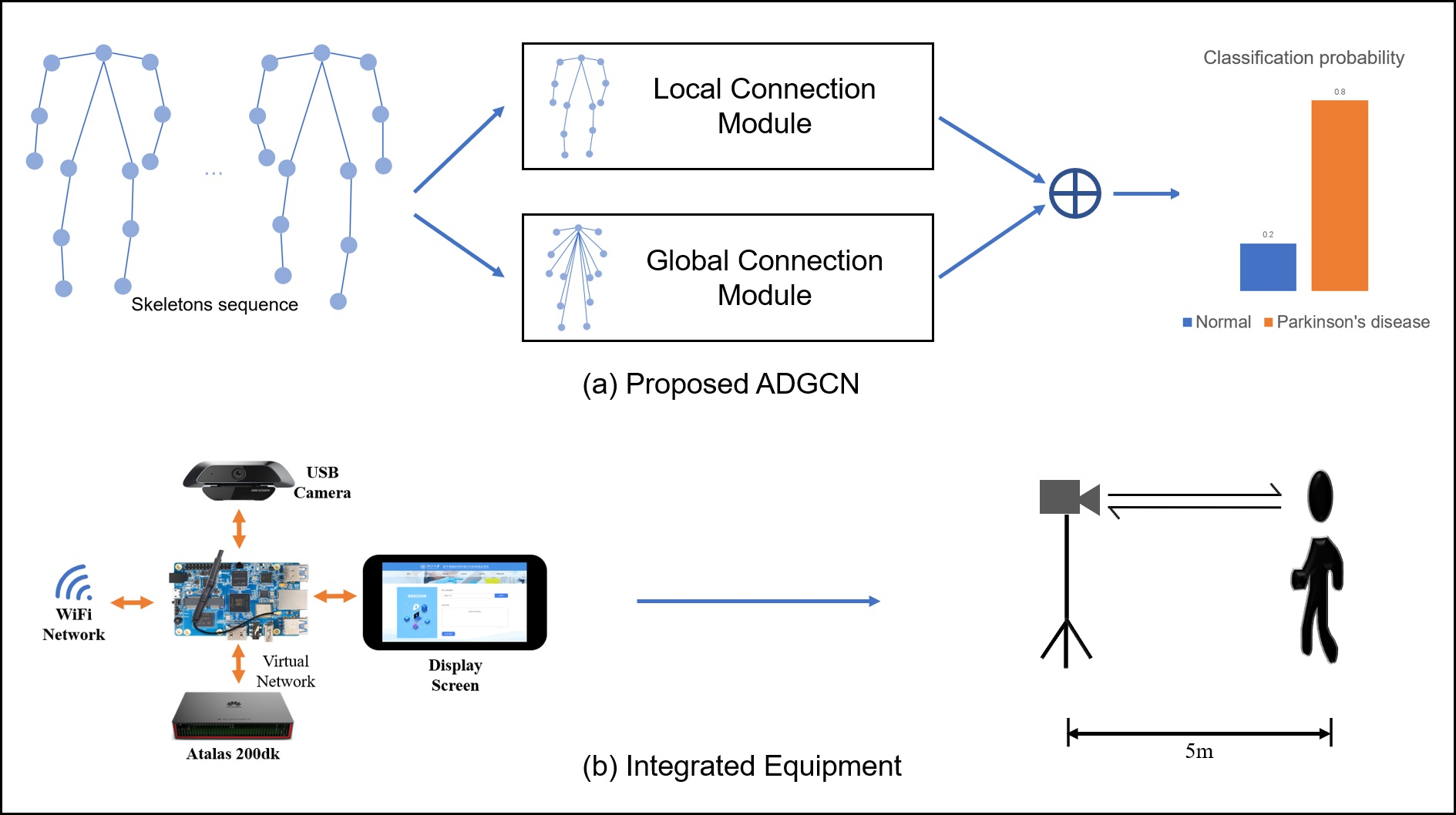
- A strengthened asymmetric dual-stream graph convolution network (ADGCN) is proposed, which can catch the slight difference in gait between Parkinson’s disease patients and healthy people.
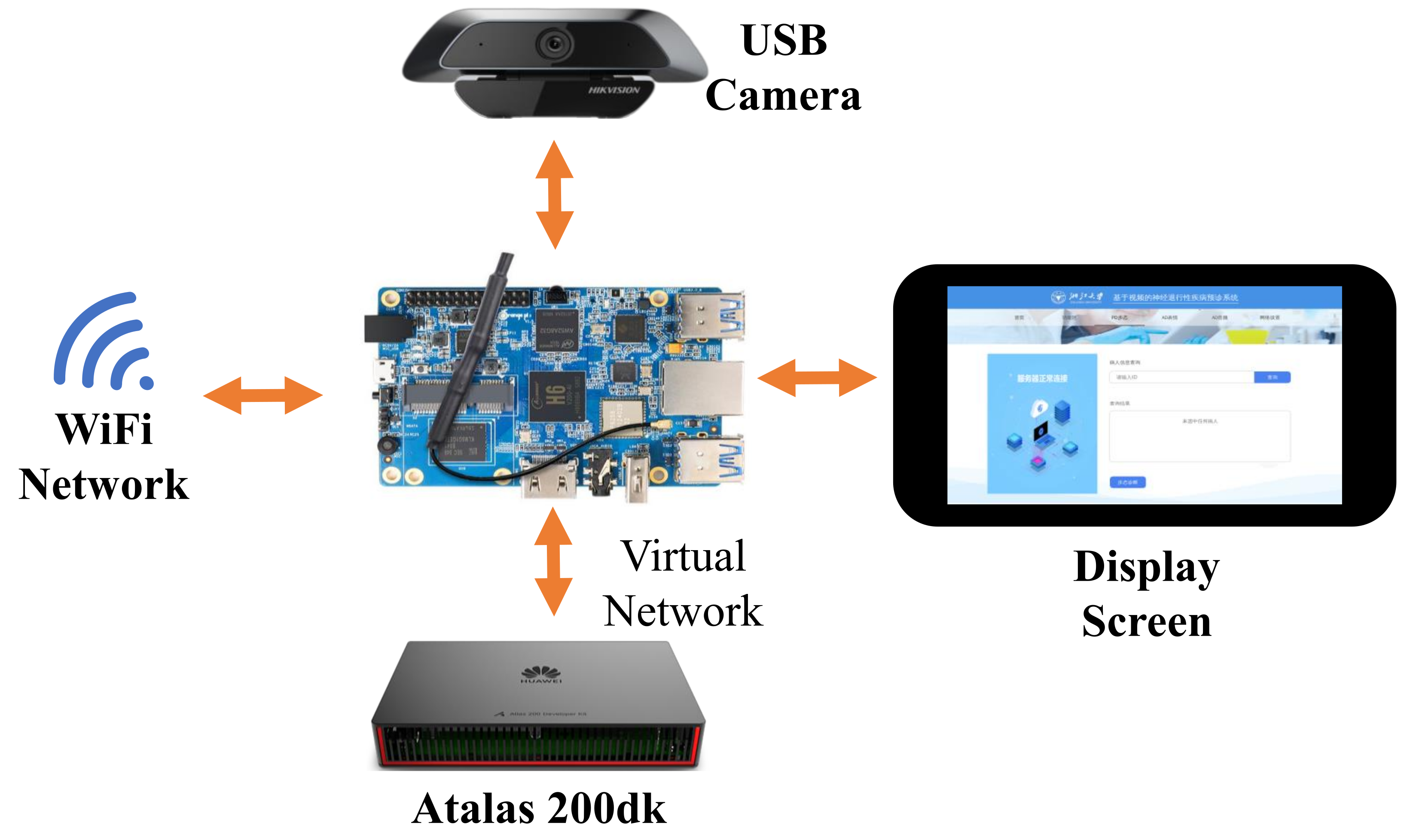
- For the first time, we deploy our method on low-power integrated equipment and test it in a real-world environment in hospital.
2. Related Work
2.1. Graph Neural Networks
2.2. Parkinson’s Disease Detection
3. Dataset
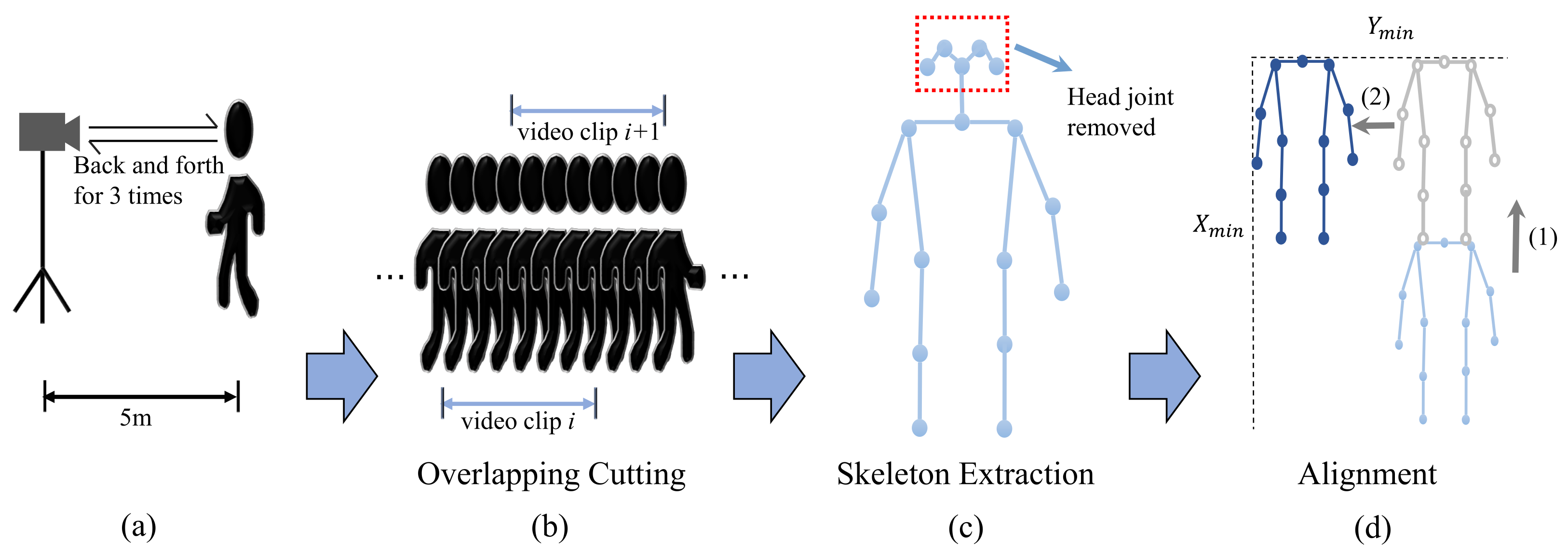
3.1. Data Collection
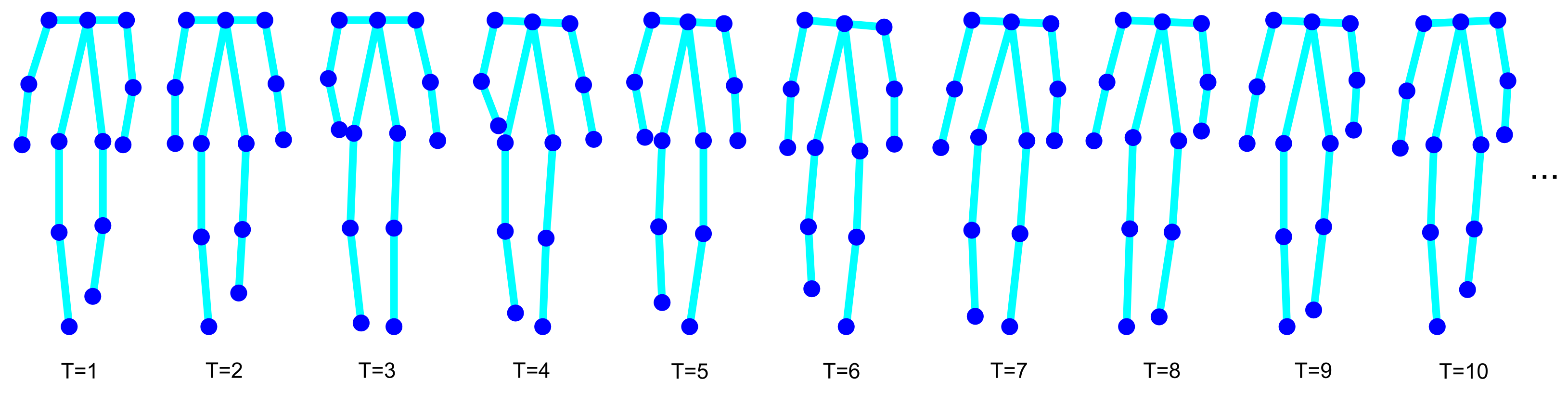
3.2. Data Preprocess
3.3. Simple Baseline
- Angle: For some PD patients, it is hard to swing the arm. In this work, the angles around the elbow and shoulder are calculated in each frame. The mean and variance of the same angle in time domain are used to measure the difficulty of swinging arms.
- Bone length: In the 2D space, the calculated bone length is the result after projection. The different postures of a walker will generate different bone lengths. The bone length feature is considered to model the walker’s posture information.
- Symmetry: The gait of a healthy person is symmetrical. For PD patients, due to the rigidity of muscles, it is hard to walk symmetrically. As shown in Equation (2), the symmetry features are computed by comparing the angles and bone lengths on the left and right sides of the human body.where l means left, r means right, and denote computing expectation and variance along the time domain.
- Speed: We calculate the first order difference of the body joints and average it in the time domain.
- Acceleration: Acceleration contains rich motion information. The joints’ acceleration is computed by the first order difference of the joints’ speed.
4. Proposed Methods
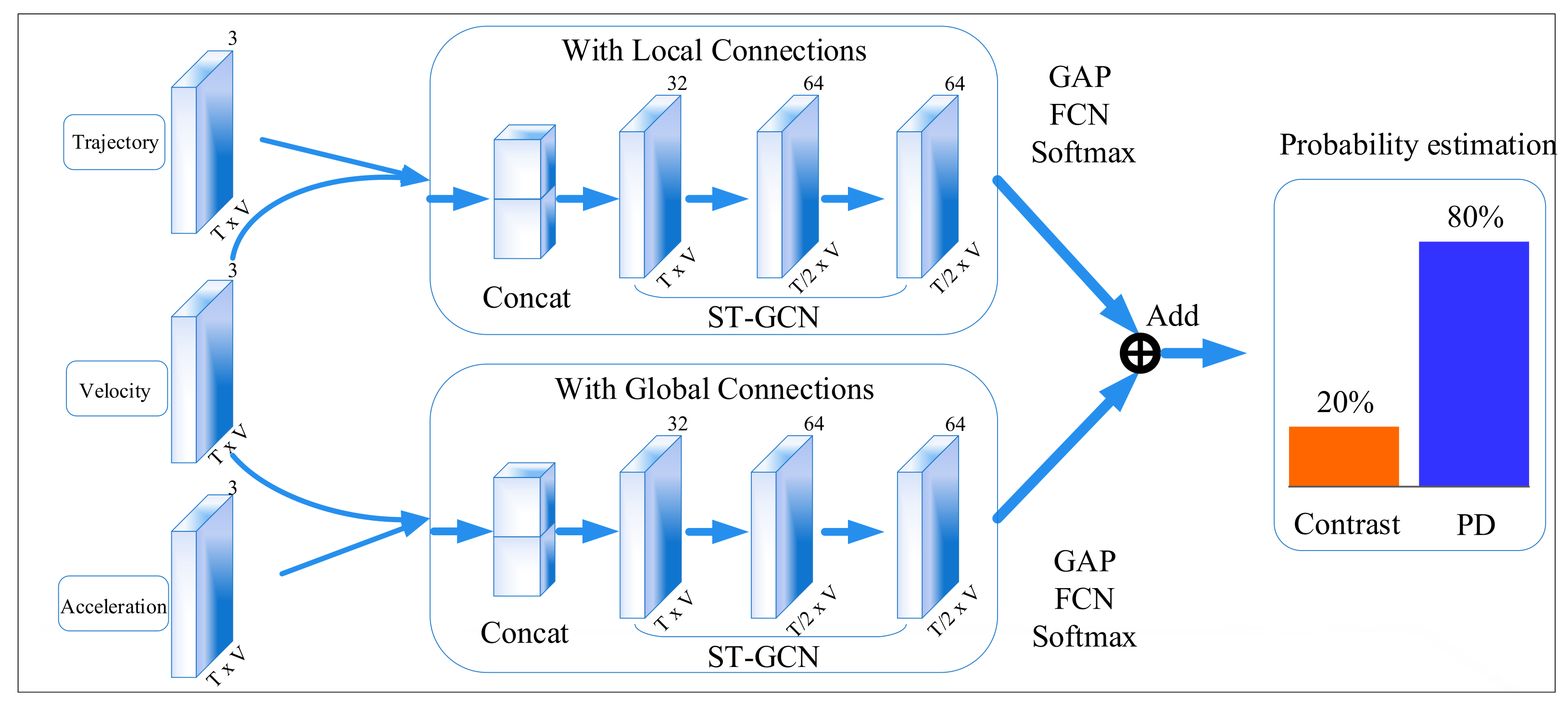
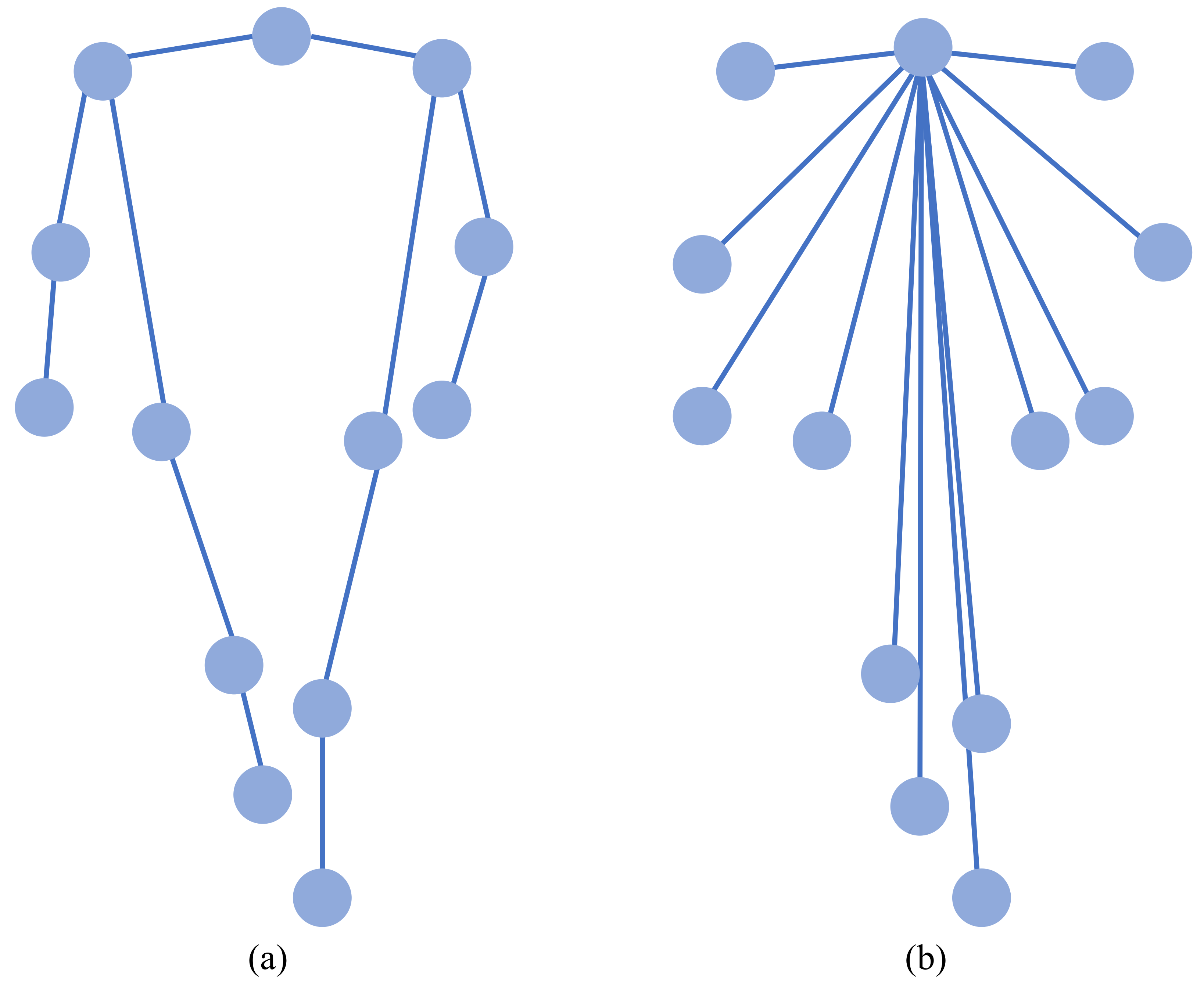
4.1. Local and Global Connections
4.2. Position and Motion Information
4.3. Loss Function
4.4. Integrated Equipment
5. Experiment
5.1. Implementation Details
5.2. Main Results
5.3. Ablation Study
5.3.1. Loss Function
5.3.2. Data Augmentation and Joints Selection
5.3.3. Dual Branch
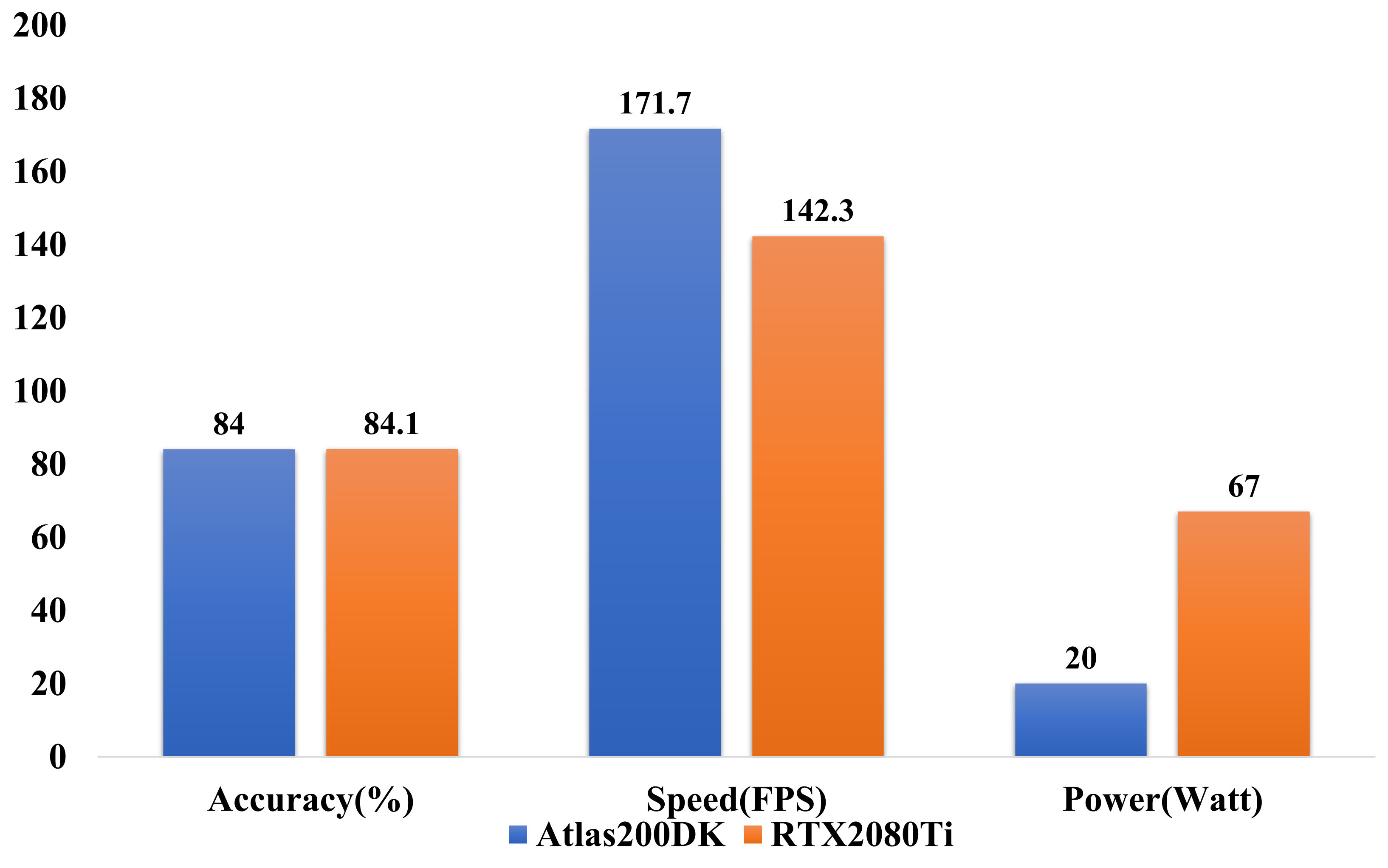
5.4. Deployment Efficiency
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, G.; Ma, J.; Cui, S.; He, Y.; Xiao, Q.; Liu, J.; Chen, S. Parkinson’s disease in China: A forty-year growing track of bedside work. Transl. Neurodegener. 2019, 1, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Radaideh, A.M.; Rababah, E.M. The role of magnetic resonance imaging in the diagnosis of Parkinson’s disease: A review. Clin. Imaging 2016, 40, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J. Parkinson’s disease: Clinical features and diagnosis. J. Neurol. Neurosurg. Psychiatry 2008, 79, 368–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinmetzer, T.; Maasch, M.; Bönninger, I.; Travieso, C.M. Analysis and Classification of Motor Dysfunctions in Arm Swing in Parkinson’s Disease. Electronics 2019, 8, 1471. [Google Scholar] [CrossRef] [Green Version]
- Pistacchi, M.; Gioulis, M.; Sanson, F.; De Giovannini, E.; Filippi, G.; Rossetto, F.; Zambito Marsala, S. Gait analysis and clinical correlations in early Parkinson’s disease. Funct. Neurol. 2017, 1, 28–34. [Google Scholar] [CrossRef]
- Salarian, A.; Russmann, H.; Vingerhoets, F.J.G.; Burkhard, P.R.; Aminian, K. Ambulatory Monitoring of Physical Activities in Patients With Parkinson’s Disease. IEEE Trans. Biomed. Eng. 2007, 54, 2296–2299. [Google Scholar] [CrossRef]
- Medeiros, L.; Almeida, H.; Dias, L.; Perkusich, M.; Fischer, R. A Gait Analysis Approach to Track Parkinson’s Disease Evolution Using Principal Component Analysis. In Proceedings of the 2016 IEEE 29th International Symposium on Computer-Based Medical Systems (CBMS), Dublin, Ireland, 20–24 June 2016; pp. 48–53. [Google Scholar] [CrossRef]
- Veeraragavan, S.; Gopalai, A.A.; Gouwanda, D.; Ahmad, S.A. Parkinson’s Disease Diagnosis and Severity Assessment Using Ground Reaction Forces and Neural Networks. Front. Physiol. 2020, 11, 1409. [Google Scholar] [CrossRef]
- El Maachi, I.; Bilodeau, G.A.; Bouachir, W. Deep 1D-Convnet for accurate Parkinson disease detection and severity prediction from gait. Expert Syst. Appl. 2020, 143, 113075. [Google Scholar] [CrossRef]
- Cantürk, İ. A computerized method to assess Parkinson’s disease severity from gait variability based on gender. Biomed. Signal Process. Control 2021, 66, 102497. [Google Scholar] [CrossRef]
- Liu, X.; Li, W.; Liu, Z.; Du, F.; Zou, Q. A dual-branch model for diagnosis of Parkinson’s disease based on the independent and joint features of the left and right gait. Appl. Intell. 2021, 10, 7221–7232. [Google Scholar] [CrossRef]
- Hsieh, Y.L.; Abbod, M.F. Gait Analyses of Parkinson’s Disease Patients Using Multiscale Entropy. Electronics 2021, 10, 2604. [Google Scholar] [CrossRef]
- Pereira dos Santos, D.M.; Ferreira Neto, M.; Lemos, M.R.; da Silva, V.J.; da Silva Federal, W.A.; de Lucena Junior, V.F. Wearable System for Early Identification of Parkinson’s Disease Symptoms Through the Evaluation of the Gait Training. In Proceedings of the 2019 IEEE 9th International Conference on Consumer Electronics (ICCE-Berlin), Berlin, Germany, 8–11 September 2019; pp. 51–56. [Google Scholar] [CrossRef]
- Li, B.; Yao, Z.; Wang, J.; Wang, S.; Yang, X.; Sun, Y. Improved Deep Learning Technique to Detect Freezing of Gait in Parkinson’s Disease Based on Wearable Sensors. Electronics 2020, 9, 1919. [Google Scholar] [CrossRef]
- Locatelli, P.; Alimonti, D.; Traversi, G.; Re, V. Classification of Essential Tremor and Parkinson’s Tremor Based on a Low-Power Wearable Device. Electronics 2020, 9, 1695. [Google Scholar] [CrossRef]
- Cao, Z.; Simon, T.; Wei, S.E.; Sheikh, Y. Realtime Multi-Person 2D Pose Estimation Using Part Affinity Fields. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017. [Google Scholar]
- Fang, H.S.; Xie, S.; Tai, Y.W.; Lu, C. RMPE: Regional Multi-Person Pose Estimation. In Proceedings of the IEEE International Conference on Computer Vision (ICCV), Venice, Italy, 22–29 October 2017. [Google Scholar]
- Sun, K.; Xiao, B.; Liu, D.; Wang, J. Deep High-Resolution Representation Learning for Human Pose Estimation. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), Long Beach, CA, USA, 15–20 June 2019. [Google Scholar]
- Zhou, T.; Wang, W.; Liu, S.; Yang, Y.; Van Gool, L. Differentiable Multi-Granularity Human Representation Learning for Instance-Aware Human Semantic Parsing. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), Nashville, TN, USA, 20–25 June 2021; pp. 1622–1631. [Google Scholar]
- Randhavane, T.; Bhattacharya, U.; Kapsaskis, K.; Gray, K.; Bera, A.; Manocha, D. Learning Perceived Emotion Using Affective and Deep Features for Mental Health Applications. In Proceedings of the 2019 IEEE International Symposium on Mixed and Augmented Reality Adjunct (ISMAR-Adjunct), Beijing, China, 10–18 October 2020. [Google Scholar]
- Bhattacharya, U.; Mittal, T.; Chandra, R.; Randhavane, T.; Bera, A.; Manocha, D. STEP: Spatial Temporal Graph Convolutional Networks for Emotion Perception from Gaits. In Proceedings of the AAAI Conference on Artificial Intelligence, New York, NY, USA, 7–12 February 2020; Volume 34, pp. 1342–1350. [Google Scholar] [CrossRef]
- Bhattacharya, U.; Roncal, C.; Mittal, T.; Chandra, R.; Kapsaskis, K.; Gray, K.; Bera, A.; Manocha, D. Take an Emotion Walk: Perceiving Emotions from Gaits Using Hierarchical Attention Pooling and Affective Mapping. In Computer Vision—ECCV 2020; Springer International Publishing: Berlin/Heidelberg, Germany, 2020; pp. 145–163. [Google Scholar]
- Zhuang, Y.; Lin, L.; Tong, R.; Liu, J.; Iwamoto, Y.; Chen, Y.W. G-GCSN: Global Graph Convolution Shrinkage Network for Emotion Perception from Gait. In Computer Vision—ACCV 2020 Workshops; Sato, I., Han, B., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 46–57. [Google Scholar]
- Yan, S.; Xiong, Y.; Lin, D. Spatial Temporal Graph Convolutional Networks for Skeleton-Based Action Recognition. In Proceedings of the AAAI, New Orleans, LA, USA, 2–7 February 2018. [Google Scholar]
- Shi, L.; Zhang, Y.; Cheng, J.; Lu, H. Two-Stream Adaptive Graph Convolutional Networks for Skeleton-Based Action Recognition. In Proceedings of the 2019 IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), Long Beach, CA, USA, 15–20 June 2019; pp. 12018–12027. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Chen, S.; Chen, X.; Zhang, Y.; Wang, Y.; Tian, Q. Actional-Structural Graph Convolutional Networks for Skeleton-Based Action Recognition. In Proceedings of the 2019 IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), Long Beach, CA, USA, 15–20 June 2019; pp. 3590–3598. [Google Scholar] [CrossRef] [Green Version]
- Xiong, X.; Min, W.; Zheng, W.S.; Liao, P.; Yang, H.; Wang, S. S3D-CNN: Skeleton-based 3D consecutive-low-pooling neural network for fall detection. Appl. Intell. 2020, 50, 3521–3534. [Google Scholar] [CrossRef]
- Ding, C.; Liu, K.; Cheng, F.; Belyaev, E. Spatio-temporal attention on manifold space for 3D human action recognition. Appl. Intell. 2021, 51, 560–570. [Google Scholar] [CrossRef]
- Mehrizi, R.; Peng, X.; Zhang, S.; Liao, R.; Li, K. Automatic Health Problem Detection from Gait Videos Using Deep Neural Networks. arXiv 2020, arXiv:cs.CV/1906.01480. [Google Scholar]
- Wang, Y.; Wang, J.; Liu, X.; Zhu, T. Detecting Depression Through Gait Data: Examining the Contribution of Gait Features in Recognizing Depression. Front. Psychiatry 2021, 12, 633. [Google Scholar] [CrossRef]
- Fan, W.; Ma, Y.; Li, Q.; He, Y.; Zhao, E.; Tang, J.; Yin, D. Graph Neural Networks for Social Recommendation. In The World Wide Web Conference; Association for Computing Machinery: New York, NY, USA, 2019; pp. 417–426. [Google Scholar] [CrossRef] [Green Version]
- Do, K.; Tran, T.; Venkatesh, S. Graph Transformation Policy Network for Chemical Reaction Prediction. In Proceedings of the 25th ACM SIGKDD International Conference on Knowledge Discovery & Data Mining, Anchorage, AK, USA, 4–8 August 2019; Association for Computing Machinery: New York, NY, USA, 2019; pp. 750–760. [Google Scholar] [CrossRef] [Green Version]
- Zhou, T.; Wang, W.; Qi, S.; Ling, H.; Shen, J. Cascaded Human-Object Interaction Recognition. In Proceedings of the 2020 IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), Seattle, WA, USA, 13–19 June 2020; pp. 4262–4271. [Google Scholar] [CrossRef]
- Zhou, T.; Li, L.; Li, X.; Feng, C.M.; Li, J.; Shao, L. Group-Wise Learning for Weakly Supervised Semantic Segmentation. IEEE Trans. Image Process. 2022, 31, 799–811. [Google Scholar] [CrossRef]
- Yu, F.; Koltun, V. Multi-Scale Context Aggregation by Dilated Convolutions. In Proceedings of the ICLR, San Juan, PR, USA, 2–4 May 2016. [Google Scholar]
- Mc Ardle, R.; Del Din, S.; Galna, B.; Thomas, A.; Rochester, L. Differentiating dementia disease subtypes with gait analysis: Feasibility of wearable sensors? Gait Posture 2020, 76, 372–376. [Google Scholar] [CrossRef]
- Lin, T.Y.; Goyal, P.; Girshick, R.; He, K.; Dollár, P. Focal Loss for Dense Object Detection. IEEE Trans. Pattern Anal. Mach. Intell. 2020, 42, 318–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, T.; Moreau, T.; Jiang, Z.; Zheng, L.; Yan, E. TVM: An Automated End-to-End Optimizing Compiler for Deep Learning. In Proceedings of the 13th USENIX Symposium on Operating Systems Design and Implementation (OSDI 18), Carlsbad, CA, USA, 8–10 October 2018. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | Accuracy | Recall | F1 Score |
|---|---|---|---|
| Hand-crafted Feature + SVM (Baseline) | 76.5% | 77.3% | 0.761 |
| ST-GCN | 78.5% | 79.2% | 0.801 |
| Ours | 82.6% | 84.0% | 0.842 |
| Ours | 84.1% | 85.8% | 0.852 |
| Head Joints | Augmentation | Accuracy | Recall | F1 Score |
|---|---|---|---|---|
| ✓ | ✕ | 74.8% | 72.3% | 0.744 |
| ✓ | ✓ | 76.2% | 73.6% | 0.771 |
| ✕ | ✓ | 78.5% | 79.2% | 0.801 |
| Model | Branch1 | Branch2 | Result | ||||
|---|---|---|---|---|---|---|---|
| Connection | Input | Connection | Input | Accuracy | Recall | F1 Score | |
| ST-GCN | Local | Trajectory | / | / | 78.5% | 79.2% | 0.801 |
| Dual branch | Local | Trajectory | Local | Velocity | 80.0% | 82.1% | 0.817 |
| Dual branch | Local | Trajectory + velocity | Local | Velocity + Acceleration | 80.5% | 82.6% | 0.822 |
| Dual branch | Global | Trajectory + velocity | Global | Velocity + Acceleration | 80.0% | 83.3% | 0.820 |
| Dual branch | Local | Trajectory + velocity | Global | Velocity + Acceleration | 84.1% | 85.8% | 0.852 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
He, Y.; Yang, T.; Yang, C.; Zhou, H. Integrated Equipment for Parkinson’s Disease Early Detection Using Graph Convolution Network. Electronics 2022, 11, 1154. https://doi.org/10.3390/electronics11071154
He Y, Yang T, Yang C, Zhou H. Integrated Equipment for Parkinson’s Disease Early Detection Using Graph Convolution Network. Electronics. 2022; 11(7):1154. https://doi.org/10.3390/electronics11071154
Chicago/Turabian StyleHe, Yefei, Tao Yang, Cheng Yang, and Hong Zhou. 2022. "Integrated Equipment for Parkinson’s Disease Early Detection Using Graph Convolution Network" Electronics 11, no. 7: 1154. https://doi.org/10.3390/electronics11071154