
Machine Learning-Based Feature Selection and Classification for the Experimental Diagnosis of Trypanosoma cruzi


Abstract
:1. Introduction
1.1. Previous Work on Diagnosis Techniques and Clinical Findings for T. cruzi
1.2. Machine Learning in Chagas Disease Classification
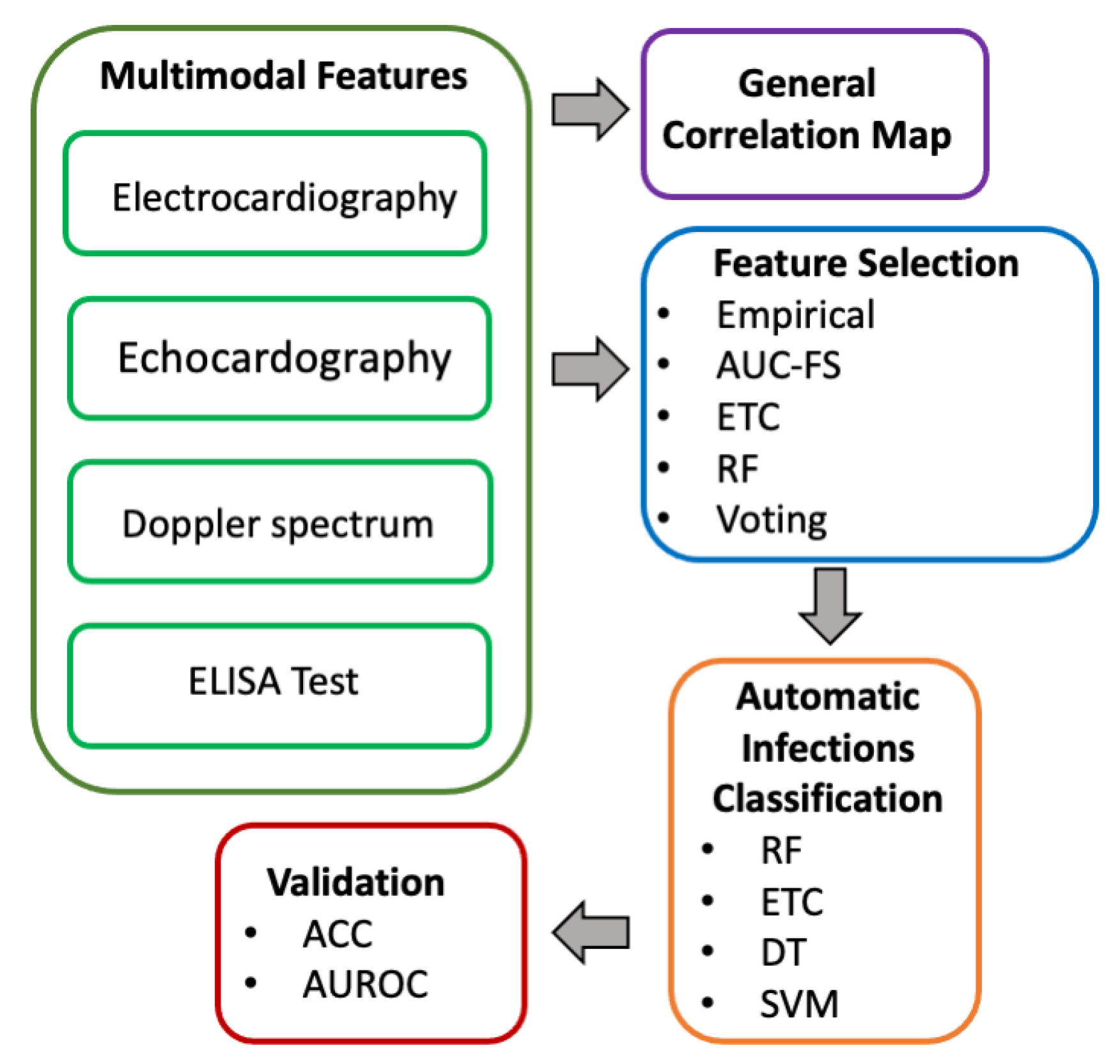
2. Data Acquisition and Methodology
2.1. Experiment Description
2.2. Data Acquisition
2.3. Multimodal Data Analysis
2.3.1. Statistic Analysis
2.3.2. Feature Selection
2.3.3. Automatic Classification
2.3.4. Validation
3. Results and Discussion
3.1. Pearson Correlation Maps—Statistic Analysis
3.2. Feature Selection
3.3. Classification and Validation
Comparison with Other Related Works and Clinical Diagnosis
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rahmani, A.; Yousefpoor, E.; Yousefpoor, M.S.; Mehmood, Z.; Haider Malik, A.; Hosseinzadeh, M.; Naqvi, R. Machine Learning (ML) in Medicine: Review, Applications, and Challenges. Mathematics 2021, 9, 2970. [Google Scholar] [CrossRef]
- Integrating Neglected Tropical Diseases into Global Health and Development: Fourth WHO Report on Neglected Tropical Diseases. Available online: https://apps.who.int/iris/bitstream/handle/10665/255011/9789241565448-eng.pdf (accessed on 8 January 2022).
- Rassi, A., Jr.; Rassi, A.; Marin-Neto, J.A. Chagas disease. Lancet 2010, 375, 1388–1402. [Google Scholar] [CrossRef]
- Rivero-Gairaud, I. Enfermedad de Chagas. Revista Médica de Costa Rica y Centroamérica 2016, 73, 297–301. [Google Scholar]
- La Enfermedad de Chagas (Tripanosomiasis Americana). Available online: https://www.who.int/es/news-room/fact-sheets/detail/chagas-disease-(american-trypanosomiasis) (accessed on 4 September 2021).
- Cevallos, A.M.; Hernández, R. Chagas’ Disease: Pregnancy and Congenital Transmission. Biomed Res. Int. 2014, 2014, 401864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Technical Report of the TDR Disease Reference Group on Chagas Disease, Human African Trypanosomiasis and Leishmaniasis. Research priorities for Chagas disease, human African trypanosomiasis and leishmaniasis. World Health Organ Tech. Rep. Ser. 2012, 975, 1–26.
- World Health Organization. Chagas disease in Latin America: An epidemiological update based on 2010 estimates. Wkly. Epidemiol. Rec. 2015, 90, 33–44. [Google Scholar]
- Chaves, K.D.H.; Vásquez, R.Z.; Corrales, V.C. Enfermedad de Chagas: Afección cardiaca. Rev. Médica Sinerg. 2019, 4, 101–110. [Google Scholar] [CrossRef] [Green Version]
- Duffy, T. Desarrollo y Aplicación de Estrategias de PCR para la Genotipificación y Cuantificación de Trypanosoma cruzi. Ph.D. Thesis, Universidad de Buenos Aires, Buenos Aires, Argentina, 2010. [Google Scholar]
- Joshi, M.; Deshpande, J. Polymerase chain reaction: Methods, principles and application. Int. J. Biomed. Res. 2011, 2, 81–97. [Google Scholar] [CrossRef]
- Werner, B.A.; Heitmann, G.I.; Jercic, L.M.I.; Jofré, M.L.; Muñoz, C.d.V.P.; Noemí, H.I.; San Martin, V.A.M.; Sapunar, P.J.; Torres, H.M.; Zulantay, A.I. Guía clínica de la enfermedad de Chagas 2006: Parte V. Diagnóstico de Laboratorio. Rev. Chil. Infectol. 2008, 25, 379–383. [Google Scholar]
- Gan, S.D.; Patel, K.R. Enzyme immunoassay and enzymelinked immunosorbent assay. J. Investig. Dermatol. 2013, 133, e12. [Google Scholar] [CrossRef] [Green Version]
- Acquatella, H.; Asch, F.; Barbosa, M.; Barros, M.; Bern, C.; Cavalcante, J.; Echeverria-Correa, L.E.; Lima, J.; Marcus, R.; Marín-Neto, J.; et al. Recommendations for multimodality cardiac imaging in patients with Chagas disease: A report from the American Society of Echocardiography in collaboration with the InterAmerican Association of Echocardiography (ECOSIAC) and the Cardiovascular Imaging Department of the Brazilian Society of Cardiology. J. Am. Soc. Echocardiogr. 2018, 31, 3–25. [Google Scholar]
- Romano, M.M.D.; Moreira, H.T.; Schmidt, A.; Carlos-Maciel, B.; Marin-Neto, J.A. Imaging Diagnosis of Right Ventricle Involvement in Chagas Cardiomyopathy. Biomed Res. Int. 2017, 2017, 3820191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lancellotti, P.; Zamorano, J.L.; Habib, G.; Badano, L. The EACVI Textbook of Echocardiography, 2nd ed.; Oxford University Press: Oxford, MO, USA, 2017. [Google Scholar]
- Haro, P.; Hevia-Montiel, N.; López-Blanco, X.; Rosado-Vallado, M.; López-Valencia, G.; Waleckx, E. Aplicaciones y potencial de las técnicas de diagnóstico por imagen en la investigación biomédica de la enfermedad de Chagas. Rev. Bioméd. 2021, 32, 45–54. [Google Scholar] [CrossRef]
- Yacoub, S.; Birks, E.J.; Slavik, Z.; Henein, M. Early detection of myocardial dysfunction in Chagas disease using novel echocardiographic indices. Trans. R. Soc. Trop. Med. Hyg. 2003, 97, 528–534. [Google Scholar] [CrossRef]
- Viotti, R.; Vigliano, C.; Laucella, S.; Lococo, B.; Petti, M.; Bertocchi, G.; Vera, B.R.; Armenti, H. Value of echocardiography for diagnosis and prognosis of chronic Chagas disease cardiomyopathy without heart failure. Heart 2004, 90, 655–660. [Google Scholar] [CrossRef] [Green Version]
- Valerio, L.; Roure, S.; Sabria, M.; Balanzo, X.; Vallès, X.; Serés, L. Clinical, electrocardiographic and echocardiographic abnormalities in Latin American migrants with newly diagnosed Chagas disease 2005-2009, Barcelona, Spain. Eurosurveillance 2011, 16, 19971. [Google Scholar] [CrossRef] [Green Version]
- Ferrer, E.; Lares, M.; Viettri, M.; Medina, M. Comparación entre técnicas inmunológicas y moleculares para el diagnóstico de la enfermedad de Chagas. Enfermedades Infecciosas y Microbiología Clínica 2013, 31, 277–282. [Google Scholar] [CrossRef]
- De Oliveira, L.F.; Romano, M.M.; de Carvalho, E.E.; Cabeza, J.M.; Salgado, H.C.; Fazan, R., Jr.; Costa, R.S.; da Silva, J.S.; Higuchi, M.d.L.; Maciel, B.C.; et al. Histopathological correlates of global and segmental left ventricular systolic dysfunction in experimental chronic Chagas cardiomyopathy. J. Am. Heart Assoc. 2016, 5, e002786. [Google Scholar] [CrossRef] [Green Version]
- Santos, F.M.; Mazzeti, A.L.; Caldas, S.; Goncalves, K.R.; Lima, W.G.; Torres, R.M.; Bahia, M.T. Chagas cardiomyopathy: The potential effect of benznidazole treatment on diastolic dysfunction and cardiac damage in dogs chronically infected with Trypanosoma cruzi. Acta Trop. 2016, 161, 44–54. [Google Scholar] [CrossRef]
- Teles, W.d.S.; Machado, A.P.; Cantos, P.C.C., Jr.; de Melo, C.M.; Silva, M.H.S.; da Silva, R.N.; Jeraldo, V.d.L.S. Machine learning and automatic selection of attributes for the identification of Chagas disease from clinical and sociodemographic data. Res. Soc. Dev. 2021, 10, e19310413879. [Google Scholar] [CrossRef]
- Silva, L.E.V.; Moreira, H.T.; Bernardo, M.M.M.; Schmidt, A.; Romano, M.M.D.; Salgado, H.C.; Fazan, R., Jr.; Tinós, R.; Marin-Neto, J.A. Prediction of echocardiographic parameters in Chagas disease using heart rate variability and machine learning. Biomed. Signal Process. Control. 2021, 67, 102513. [Google Scholar] [CrossRef]
- Escalera, S.; Pujol, O.; Laciar, E.; Vitria, J.; Pueyo, E.; Radeva, P. Coronary damage classification of patients with the Chagas disease with error-correcting output codes. In Proceedings of the 2008 4th International IEEE Conference Intelligent Systems, Varna, Bulgaria, 6–8 September 2008; pp. 12–22. [Google Scholar]
- Asl, B.M.; Setarehdan, S.K.; Mohebbi, M. Support vector machine-based arrhythmia classification using reduced features of heart rate variability signal. Artif. Intell. Med. 2008, 44, 51–64. [Google Scholar] [CrossRef] [PubMed]
- Dumonteil, E.; Escobedo-Ortegon, J.; Reyes-Rodriguez, N.; Arjona-Torres, A.; Ramirez-Sierra, M.J. Immunotherapy of Trypanosoma cruzi infection with DNA vaccines in mice. Infect. Immun. 2004, 72, 46–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De la Cruz, J.J.; Villanueva-Lizama, L.; Dzul-Huchim, V.; Ramirez-Sierra, M.J.; Martinez-Vega, P.; Rosado-Valledo, M.; Ortega-Lopez, J.; Flores-Pucheta, C.I.; Portia, G.; Zhan, B.; et al. Production of recombinant TSA-1 and evaluation of its potential for the immuno-therapeutic control of Trypanosoma cruzi infection in mice. Hum. Vaccin. Immunother. 2019, 15, 210–219. [Google Scholar] [CrossRef] [Green Version]
- Hernández-Cuevas, N.; Marín-Cervera, A.; Garcia-Polanco, S.; Martínez-Vega, P.; Rosado-Vallado, M.; Dumonteil, E. Fibronectin degradation as biomarker for Trypanosoma cruzi infection and treatment monitoring in mice. Parasitology 2021, 148, 1067–1073. [Google Scholar] [CrossRef]
- National Research Council. Guide for the Care and Use of Laboratory Animals, 8th ed.; National Academies Press: Washington, DC, USA, 2011; pp. 11–40. [Google Scholar]
- Xing, S.; Tsaih, S.W.; Yuan, R.; Svenson, K.L.; Jorgenson, L.M.; So, M.; Paigen, B.J.; Korstanje, R. Genetic influence on electrocardiogram time intervals and heart rate in aging mice. Am. J. Physiol. Heart Circ. Physiol. 2009, 296, H1907–H1913. [Google Scholar] [CrossRef]
- Mitchell, G.F.; Jeron, A.; Koren, G. Measurement of heart rate and Q-T interval in the conscious mouse. Am. J. Physiol. 1998, 274, H747–H751. [Google Scholar] [CrossRef]
- Teichholz, L.E.; Kreulen, T.; Herman, M.V.; Gorlin, R.B.M. Problems in echocardiographic volume determinations: Echocardiographic-angiographic correlations in the presence or absence of asynergy. Am. J. Cardiol. 1976, 37, 7–11. [Google Scholar] [CrossRef]
- Stypmann, J.; Engelen, M.A.; Troatz, C.; Rothenburger, M.; Eckardt, L.; Tiemann, K. Echocardiographic assessment of global left ventricular function in mice. Lab. Anim. 2009, 43, 127–137. [Google Scholar] [CrossRef]
- Redd, A.K.; Taffet, G.E.; Li, Y.H.; Lim, S.W.; Pham, T.T.; Pocius, J.S.; Entman, M.L.; Michael, L.H.; Hartley, C.J. Pulsed Doppler signal processing for use in mice: Applications. IEEE Trans. Biomed. Eng. 2005, 52, 1771–1783. [Google Scholar] [CrossRef]
- Spinella, S.; Liegeard, P.; Hontebeyrie-Joskowicz, M. Trypanosoma cruzi: Predominance of IgG2a in nonspecific humoral response during experimental Chagas’ disease. Exp. Parasitol. 1992, 74, 46–56. [Google Scholar] [CrossRef]
- Mamitsuka, H. Selecting features in microarray classification using ROC curves. Pattern Recognit. 2006, 39, 2393–2404. [Google Scholar] [CrossRef]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Breiman, L.; (Statistics Department, Berkeley University, Berkeley, CA, USA). Manual on setting up, using, and understanding random forests V.3.1. 2002; unpublished work. [Google Scholar]
- Alam, M.Z.; Rahman, M.S.; Rahman, M.S. A Random Forest based predictor for medical data classification using feature ranking. Inform. Med. Unlocked 2019, 15, 100180. [Google Scholar] [CrossRef]
- Vapnik, V.N. The Nature of Statistical Learning Theory; Springer: New York, NY, USA, 1995; pp. 267–290. [Google Scholar]
- Pech-Aguilar, A.G.; Haro-Álvarez, A.P.; Rosado-Vallado, M.E. Updated review on the pathophysiology of Chagas cardiomyopathy. Rev. Medica Inst. Mex. Seguro Soc. 2020, 58, 328–334. [Google Scholar]
- Huikuri, H.V.; Stein, P.K. Heart rate variability in risk stratification of cardiac patients. Prog. Cardiovasc. Dis. 2013, 56, 153–159. [Google Scholar] [CrossRef]
- Speerschneider, T.; Thomsen, M.B. Physiology and analysis of the electrocardiographic T wave in mice. Acta Physiol. 2013, 209, 262–271. [Google Scholar] [CrossRef]
- Kim, E.S.H.; Sharma, A.M.; Scissons, R.; Dawson, D.; Eberhardt, R.T.; Gerhard-Herman, M.; Hughes, J.P.; Knight, S.; Kupinski, A.M.; Shugart, R.; et al. Interpretation of pheripheral arterial and venous Doppler waveforms: A consensus statement from society for vascular Medicine and Society for Vascular Ultrasound. Vasc. Med. 2020, 1, 484–506. [Google Scholar] [CrossRef]
- Bouhdi, D.E.; Truyens, C.; Rivera, M.T.; Bazin, H.; Carlier, I. Trypanosoma cruzi infection in mice induces a polyisotypic hypergammaglobulinaemia and parasite-specific response involving high IgC2a concentrations and highly avid IgC1 antibodies. Parasite Immunol. 1994, 16, 1669–1676. [Google Scholar]
- Caldas, I.S.; Diniz, L.F.; Guedes, P.M.D.M.; Nascimento, Á.F.D.S.D.; Galvão, L.M.D.C.; Lima, W.G.; Caldas, S.; Bahia, M.T. Myocarditis in different experimental models infected by Trypanosoma cruzi is correlated with the production of IgG1 isotype. Acta Trop. 2017, 40–49. [Google Scholar] [CrossRef]
- Eickhoff, S.C.; Lawrence, C.T.; Sagartz, J.E.; Bryant, L.A.; Labovitz, A.J.; Gala, S.S.; Hoft, D.F. ECG Detection of Murine Chagasic Cardiomyopathy. J. Parasitol. 2010, 96, 758–764. [Google Scholar] [CrossRef] [PubMed]
- ECGenie Indices; Mouse Especific Inc.: Framingham, MA, USA, 2018; unpublished manuscript.
- Tovar Perez, J.E.; Ortiz-Urbina, J.; Heredia, C.P.; Pham, T.T.; Madala, S.; Hartley, C.J.; Entman, M.L.; Taffet, G.E.; Reddy, A.K. Aortic acceleration as a noninvasive index of left ventricular contractility in the mouse. Sci. Rep. 2021, 11, 536. [Google Scholar] [CrossRef] [PubMed]
- McSweeney, J.; Dobson, L.; Macnab, A. Acceleration time and ratio of acceleration time and ejection time in bicuspid aortic stenosis; a valid clinical measure? Heart 2020, 106, A7–A8. [Google Scholar]
- Talley, R.C.; Meyer, J.F.; McNay, J.L. Evaluation of the pre-ejection period as an estimate of myocardial contractility in dogs. Am. J. Cardiol. 1971, 27, 384–391. [Google Scholar] [CrossRef]
- Guidelines for the Diagnosis and Treatment of Chagas Disease. Available online: http://iris.paho.org/xmlui/handle/10665.2/49653 (accessed on 21 September 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnostic Modality | ID Extracted Feature | |||
|---|---|---|---|---|
| ECG | 1. HR 2. HRV 3. CV 4. RR Interval | 5. PQ Interval 6. R Interval 7. QRS 8. QT Interval | 9. ST Interval 10. QTc Interval 11. QTc 12. QTc dispersion | 13. SR mean 14. R Amplitude mean |
| ECHO | 15. HR SHORTH AXIS 16. LVd | 17. LVs 18. FS | 19. EF | |
| Doppler | 20. AbAO HR Avg 21. AbAO HR SD 22. AbAO RR internal Avg 23. AbAO RR interval SD 24. AbAO Peak velocity Avg 25. AbAO Peak velocity SD 26. AbAO Minimum Flow Velocity Avg 27. AbAO Minimum Velocity SD 28. AbAO Mean Flow velocity Avg 29. AbAO Mean Flow velocity SD 30. AbAO Pulsability Index Avg 31. AbAO Pulsability Index SD | 32. AbAO Resistivity Index Avg 33. AbAO Resistivity Index SD 34. AO HR Avg 35. AO HR SD 36. AO RR Interval Avg 37. AO RR Interval SD 38. AO Pre-ejection time Avg 39. AO Pre-ejection time SD 40. AO Peak velocity Avg 41. AO Peak velocity SD 42. AO Stroke Distance Avg | 43. AO Stroke Distance SD 44. AO Ejection time Avg 45. AO Ejection Time SD 46. AO Rise Time Avg 47. AO Rise Time SD 48. AO Mean velocity Avg 49. AO Mean velocity SD 50. AO Mean Acceleration Time Avg 51. AO Mean Acceleration Time SD 52. AO Peak Acceleration Avg 53. AO Peak Acceleration SD | 54. MV HR Avg 55. MV HR SD 56. MV RR Interval Avg 57. MV RR Interval SD 58. MV E Peak velocity Avg 59. MV E Peak velocity SD 60. MV E Acceleration time Avg 61. MV E Acceleration time SD 62. MV E Peak to Peak time SD 63. MV E Deceleration time SD 64. MV E Deceleration Rate SD |
| ELISA | 65. IgGT | 66. IgG1 | 67. IgG2a | |
| Classifier | ECG | ECHO | Doppler | ELISA | ||||
|---|---|---|---|---|---|---|---|---|
| ACC | AUROC | ACC | AUROC | ACC | AUROC | ACC | AUROC | |
| Control vs. Acute, 5-Fold Cross-Validation (N = 30) | ||||||||
| RF | 53.3 ± 22.1 | 71.1 ± 24.9 | 70.0 ± 12.5 | 66.7 ± 14.1 | 50.0 ± 10.5 | 68.9 ± 11.4 | 90.0 ± 13.3 | 92.2 ± 15.6 |
| ETC | 63.3 ± 16.3 | 73.3 ± 20.6 | 66.7 ± 10.5 | 66.7 ± 12.2 | 60.0 ± 22.6 | 66.7 ± 18.9 | 90.0 ± 13.3 | 94.4 ± 11.1 |
| DT | 66.7 ± 10.5 | 60.0 ± 17.0 | 70.0 ± 12.5 | 73.3 ± 8.2 | 53.3 ± 6.7 | 53.3 ± 6.7 | 86.7 ± 12.5 | 93.3 ± 13.3 |
| SVM | 66.7 ± 25.8 | 71.1 ± 23.9 | 63.3 ± 6.7 | 82.2 ± 8.9 | 50.0 ± 23.6 | 51.1 ± 15.1 | 90.0 ± 8.2 | 95.6 ± 5.2 |
| Control vs. Acute, Final Test (N = 6) | ||||||||
| RF | 66.7 | 68.4 | 66.7 | 69.3 | 66.7 | 65.2 | 100 | 98.5 |
| ETC | 66.7 | 67.3 | 50.0 | 52.1 | 66.7 | 67.4 | 100 | 98.4 |
| DT | 50.0 | 53.2 | 66.7 | 65.2 | 33.3 | 40.3 | 100 | 97.3 |
| SVM | 50.0 | 52.4 | 50.0 | 54.4 | 66.7 | 70.2 | 83.3 | 90.7 |
| Control vs. Chronic, 5-Fold Cross-Validation (N = 30) | ||||||||
| RF | 60.0 ± 17.0 | 75.6 ± 16.3 | 56.7 ± 22.6 | 64.4 ± 27.6 | 73.3 ± 13.3 | 77.8 ± 22.5 | 100 ± 0 | 100 ± 0 |
| ETC | 63.3 ± 16.3 | 68.9 ± 19.1 | 56.7 ± 22.6 | 52.2 ± 17.8 | 80.0 ± 6.7 | 85.6 ± 10.9 | 100 ± 0 | 100 ± 0 |
| DT | 60.0 ± 17.0 | 56.7 ± 17.0 | 53.3 ± 12.5 | 46.7 ± 12.5 | 63.3 ± 16.3 | 66.7 ± 18.3 | 100 ± 0 | 100 ± 0 |
| SVM | 70.0 ± 12.5 | 71.1 ± 11.3 | 66.7 ± 14.9 | 75.6 ± 13.0 | 76.7 ± 13.3 | 75.6 ± 10.9 | 95.7 ± 6.3 | 97.4 ± 3.5 |
| Control vs. Chronic, Final Test (N = 6) | ||||||||
| RF | 100 | 100 | 50.0 | 66.7 | 66.7 | 68.9 | 100 | 100 |
| ETC | 100 | 100 | 50.0 | 58.9 | 66.7 | 67.5 | 100 | 100 |
| DT | 66.7 | 67.8 | 50.0 | 52.4 | 50.0 | 54.4 | 100 | 100 |
| SVM | 83.3 | 88.9 | 50.0 | 53.4 | 66.7 | 64.3 | 100 | 100 |
| Control vs. General Infection, 5-Fold Cross-Validation (N = 60) | ||||||||
| RF | 66.7 ± 10.5 | 72.9 ± 8.9 | 73.3 ± 9.7 | 72.1 ± 9.0 | 60.0 ± 9.7 | 64.6 ± 17.9 | 95.0 ± 4.1 | 98.3 ± 2.3 |
| ETC | 66.7 ± 10.5 | 69.9 ± 12.7 | 65.0 ± 6.2 | 67.7 ± 9.7 | 50.0 ± 16.7 | 54.6 ± 16.2 | 95.0 ± 4.1 | 98.3 ± 2.3 |
| DT | 66.7 ± 9.1 | 64.6 ± 9.3 | 70.0 ± 4.1 | 69.6 ± 6.4 | 46.7 ± 12.5 | 45.0 ± 8.5 | 93.3 ± 6.2 | 93.0 ± 6.4 |
| SVM | 63.3 ± 11.3 | 69.4 ± 18.2 | 68.3 ± 6.2 | 76.0 ± 5.9 | 50.0 ± 9.1 | 49.1 ± 20.4 | 86.7 ± 8.5 | 97.7 ± 3.3 |
| Control vs. General Infection, Final Test (N = 12) | ||||||||
| RF | 83.3 | 75.7 | 58.3 | 45.7 | 58.3 | 42.9 | 83.3 | 85.7 |
| ETC | 58.3 | 71.4 | 50.0 | 47.2 | 50.0 | 41.4 | 83.3 | 87.1 |
| DT | 50.0 | 51.4 | 50.0 | 51.4 | 50.0 | 41.7 | 83.3 | 82.9 |
| SVM | 50.0 | 52.3 | 50.0 | 51.3 | 50.0 | 45.7 | 80.6 | 85.7 |
| Classifier | All Features | Empirical Selection | AUC-FS Selection | ETC Selection | RF Selection | Voting Selection | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ACC | AUROC | ACC | AUROC | ACC | AUROC | ACC | AUROC | ACC | AUROC | ACC | AUROC | |
| 5-Fold Cross-Validation (N = 30) | ||||||||||||
| RF | 90.0 ± 13.3 | 88.9 ± 22.2 | 93.3 ± 13.3 | 93.3 ± 13.3 | 90.0 ± 13.3 | 92.2 ± 15.6 | 90.0 ± 13.3 | 95.6 ± 8.9 | 90.0 ± 13.3 | 94.4 ± 11.1 | 93.3 ± 13.3 | 91.1 ± 17.8 |
| ETC | 86.7 ± 12.5 | 86.7 ± 21.5 | 90.0 ± 13.3 | 93.3 ± 13.3 | 86.7 ± 12.5 | 91.1 ± 17.8 | 93.3 ± 13.3 | 94.4 ± 11.1 | 93.3 ± 13.3 | 95.6 ± 8.9 | 93.3 ± 13.3 | 93.3 ± 13.3 |
| DT | 80.0 ± 12.5 | 73.3 ± 8.2 | 83.3 ± 14.9 | 76.7 ± 8.2 | 90.0 ± 13.3 | 86.7 ± 12.5 | 90.0 ± 13.3 | 86.7 ± 12.5 | 90.0 ± 13.3 | 83.3 ± 10.5 | 86.7 ± 12.5 | 90.0 ± 13.3 |
| SVM | 63.3 ± 24.5 | 75.6 ± 22.7 | 73.3 ± 22.6 | 80.0 ± 23.7 | 70.0 ± 28.7 | 82.2 ± 24.9 | 83.3 ± 18.3 | 91.1 ± 17.8 | 80.0 ± 24.5 | 84.4 ± 20.6 | 80.0 ± 24.5 | 82.2 ± 24.9 |
| Final Test (N = 6) | ||||||||||||
| RF | 83.3 | 85.8 | 100 | 100 | 100 | 100 | 83.3 | 92.8 | 100 | 100 | 83.3 | 92.3 |
| ETC | 83.3 | 94.3 | 83.3 | 89.4 | 83.3 | 93.7 | 83.3 | 89.5 | 83.3 | 92.4 | 83.3 | 93.5 |
| DT | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| SVM | 100 | 100 | 83.3 | 91.3 | 83.3 | 92.4 | 100 | 100 | 100 | 100 | 66.7 | 72.5 |
| Classifier | All Features | Empirical Selection | AUC-FS Selection | ETC Selection | RF Selection | Voting Selection | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ACC | AUROC | ACC | AUROC | ACC | AUROC | ACC | AUROC | ACC | AUROC | ACC | AUROC | |
| 5-Fold Cross-Validation (N = 30) | ||||||||||||
| RF | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 |
| ETC | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 96.7 ± 6.7 | 98.4 ± 2.1 | 100 ± 0 | 100 ± 0 |
| DT | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 | 100 ± 0 |
| SVM | 90.0 ± 8.2 | 95.4 ± 2.5 | 96.7 ± 6.7 | 97.5 ± 7.4 | 93.3 ± 8.2 | 97.8 ± 4.4 | 90.0 ± 8.2 | 94.3 ± 4.6 | 93.3 ± 8.2 | 95.6 ± 3.2 | 96.7 ± 6.7 | 98.5 ± 3.4 |
| Final Test (N = 6) | ||||||||||||
| RF | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| ETC | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| DT | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| SVM | 66.7 | 75.4 | 83.3 | 91.4 | 83.3 | 95.3 | 83.3 | 88.4 | 83.3 | 95.1 | 100 | 100 |
| Classifier | All Features | Empirical Selection | AUC-FS Selection | ETC Selection | RF Selection | Voting Selection | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ACC | AUROC | ACC | AUROC | ACC | AUROC | ACC | AUROC | ACC | AUROC | ACC | AUROC | |
| 5-Fold Cross-Validation (N = 60) | ||||||||||||
| RF | 96.7 ± 4.1 | 98.0 ± 2.8 | 96.7 ± 4.1 | 98.3 ± 2.3 | 96.7 ± 4.1 | 98.3 ± 2.3 | 95.0 ± 4.1 | 98.6 ± 1.8 | 95.0 ± 4.1 | 98.9 ± 2.3 | 96.7 ± 4.1 | 98.3 ± 2.2 |
| ETC | 90.0 ± 9.7 | 95.5 ± 5.3 | 96.7 ± 4.1 | 96.3 ± 5.5 | 95.0 ± 4.1 | 98.9 ± 1.4 | 96.7 ± 4.1 | 97.7 ± 3.3 | 96.7 ± 4.1 | 99.7 ± 0.6 | 96.7 ± 4.1 | 98.3 ± 2.3 |
| DT | 95.0 ± 4.1 | 93.0 ± 6.4 | 91.7 ± 7.5 | 91.3 ± 7.5 | 91.7 ± 5.3 | 93.0 ± 3.6 | 93.3 ± 3.3 | 93.0 ± 3.6 | 93.3 ± 3.3 | 93.0 ± 3.6 | 93.3 ± 6.2 | 91.3 ± 5.3 |
| SVM | 76.7 ± 12.2 | 93.8 ± 7.7 | 86.7 ± 8.5 | 94.4 ± 6.9 | 88.3 ± 8.5 | 95.5 ± 4.6 | 88.3 ± 6.7 | 96.6 ± 3.3 | 86.7 ± 8.5 | 97.7 ± 2.1 | 85.0 ± 9.7 | 98.3 ± 2.2 |
| Final Test (N = 12) | ||||||||||||
| RF | 83.3 | 82.9 | 83.3 | 85.7 | 83.3 | 94.3 | 83.3 | 88.6 | 83.3 | 85.7 | 83.3 | 90 |
| ETC | 83.3 | 84.3 | 75 | 88.6 | 83.3 | 88.6 | 75 | 97.1 | 75 | 85.7 | 75 | 94.3 |
| DT | 83.3 | 85.7 | 83.3 | 85.7 | 83.3 | 85.7 | 83.3 | 85.7 | 83.3 | 85.7 | 83.3 | 85.7 |
| SVM | 66.7 | 74.3 | 66.7 | 74.3 | 66.7 | 82.9 | 66.7 | 71.4 | 58.3 | 71.4 | 75 | 82.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hevia-Montiel, N.; Perez-Gonzalez, J.; Neme, A.; Haro, P. Machine Learning-Based Feature Selection and Classification for the Experimental Diagnosis of Trypanosoma cruzi. Electronics 2022, 11, 785. https://doi.org/10.3390/electronics11050785
Hevia-Montiel N, Perez-Gonzalez J, Neme A, Haro P. Machine Learning-Based Feature Selection and Classification for the Experimental Diagnosis of Trypanosoma cruzi. Electronics. 2022; 11(5):785. https://doi.org/10.3390/electronics11050785
Chicago/Turabian StyleHevia-Montiel, Nidiyare, Jorge Perez-Gonzalez, Antonio Neme, and Paulina Haro. 2022. "Machine Learning-Based Feature Selection and Classification for the Experimental Diagnosis of Trypanosoma cruzi" Electronics 11, no. 5: 785. https://doi.org/10.3390/electronics11050785