
Evolution of Machine Learning in Tuberculosis Diagnosis: A Review of Deep Learning-Based Medical Applications

 , ,
, ,  ,
,  ,
,
Abstract
:1. Introduction
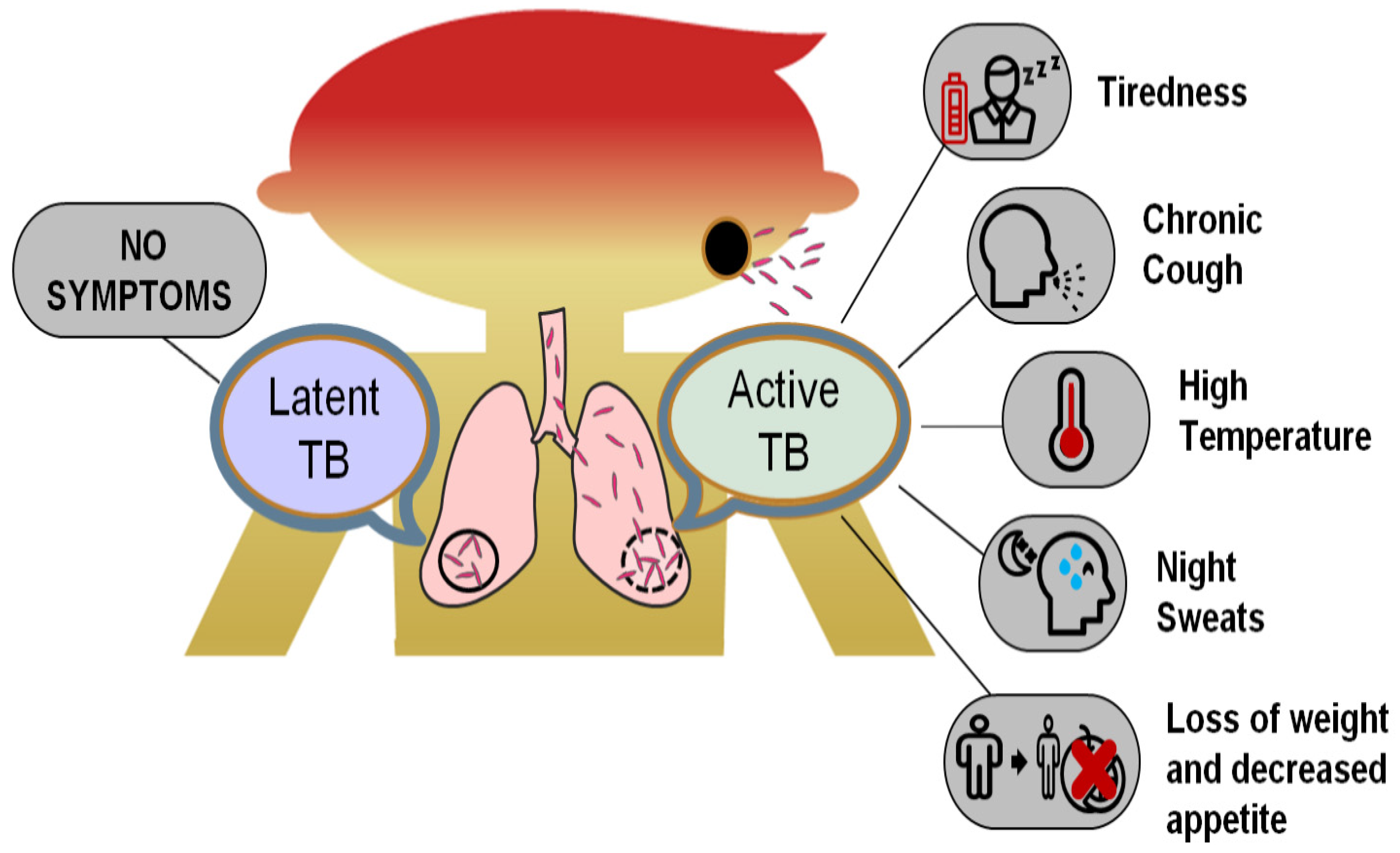
2. Tuberculosis (TB) and Its Occurrence
3. Conventional Diagnostic Techniques for Pulmonary TB
4. History of AI Applications in TB Diagnosis
5. Overview of AI Techniques Used in TB Diagnosis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S.No. | Learning Technique | Merits | Limitations | Refs. |
|---|---|---|---|---|
| 1. | Supervised Learning |
|
| [46] |
| 2. | Unsupervised Learning |
|
| [48] |
| 3. | Semi-supervised Learning |
|
| [54] |
| 4. | Transfer Learning |
|
| [58] |
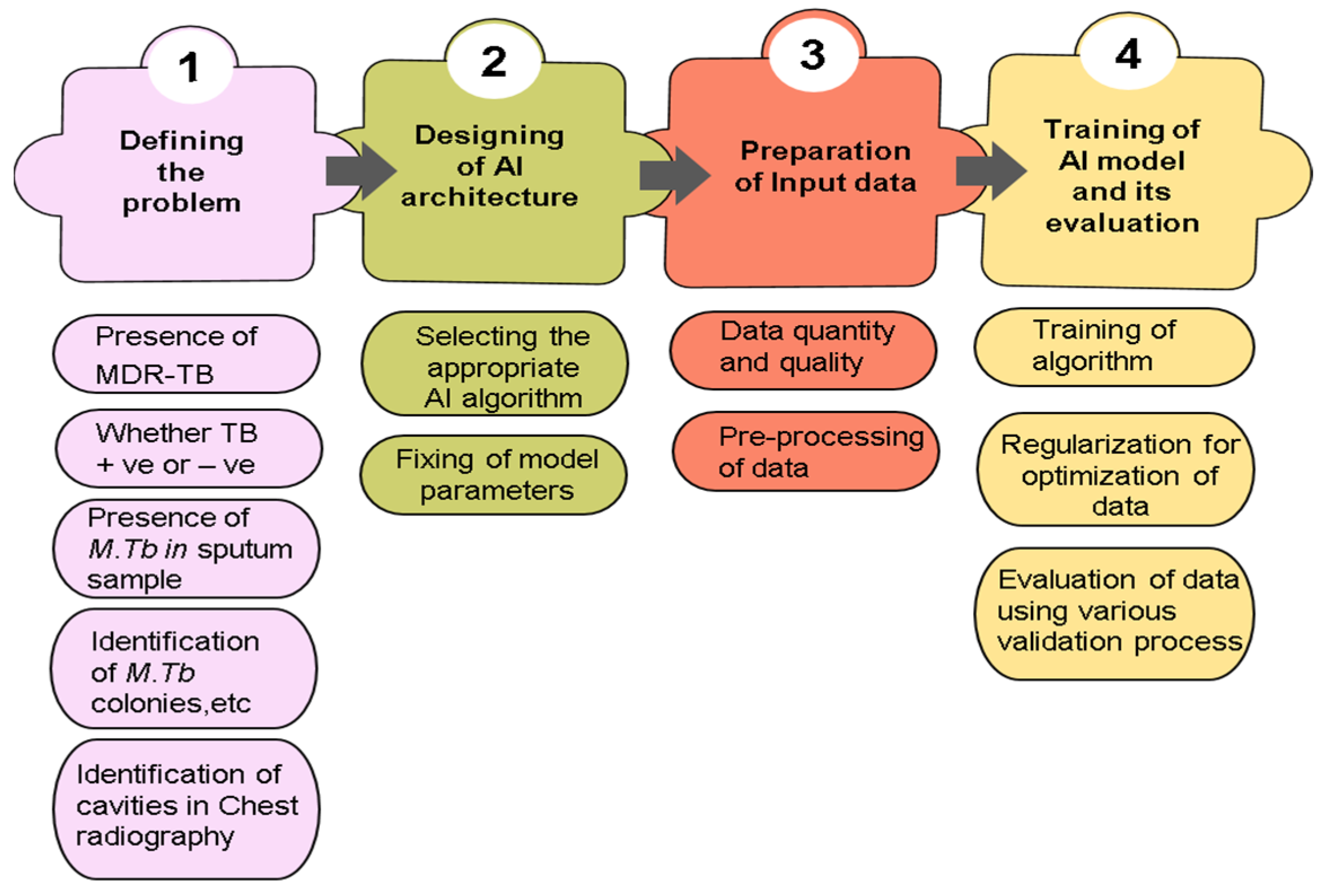
6. Construction of AI Model in TB Diagnosis
6.1. Preparation of Input Data
6.2. Input Databases Used in TB Diagnosis
| S. No. | Name of the Database | Developed by | Features of the Database | Ref. |
|---|---|---|---|---|
| Chest X-ray Dataset | ||||
| 1. | Shenzhen dataset | Partnership with Shenzhen No.3 People’s Hospital, Guangdong Medical College, Shenzhen, China |
| [72] |
| 2. | Montgomery County chest X-ray dataset (MC) | Partnership with the Department of Health and Human Services, Montgomery County, Maryland, USA |
| [72] |
| 3. | PadChest | Radiologist at San Juan Hospital, Spain |
| [73] |
| 4. | ChestX-ray8 dataset | Radiologist at NIH Clinic center, Bethesda, Maryland, USA, as a part of routine care |
| [9] |
| 5. | Belarus TB Portal dataset | TB specialist at Minsk city, capital of Belarus, Europe |
| [74] |
| 6. | TBX11K dataset | Media Computing Lab, Nankai University, China |
| [75] |
| 7. | 8-Bit dataset-A | Radiologist at National Institute of Tuberculosis and Respiratory Diseases, New Delhi, India |
| [76] |
| 8. | 14-Bit dataset-B | Radiologist at National Institute of Tuberculosis and Respiratory Diseases, New Delhi, India |
| [76] |
| Sputum Smear Microscopy Image Dataset | ||||
| 9. | ZNSM iDB | Jaypee University of Information Technology, Solan, India |
| [77] |
6.3. Quantity and Quality of Input Data
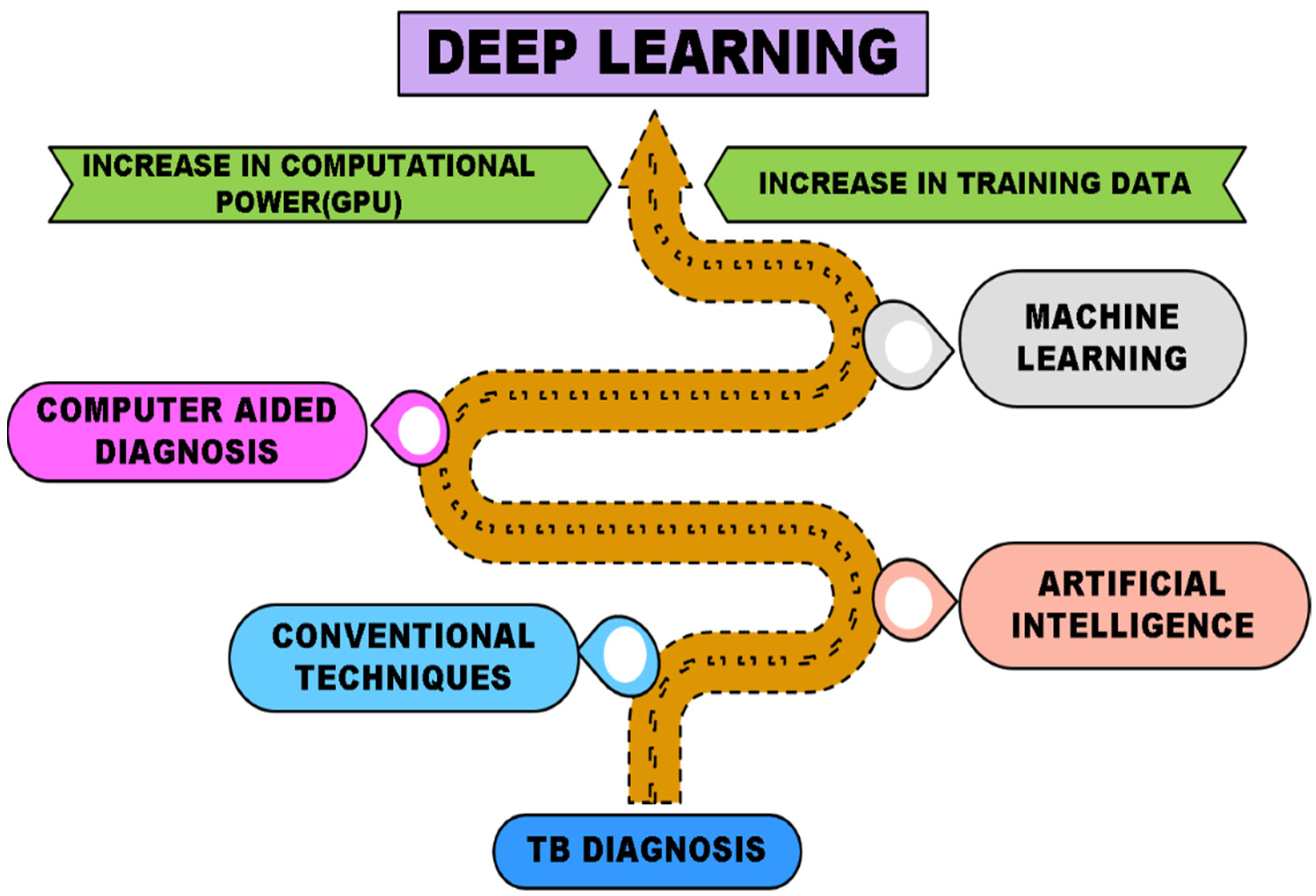
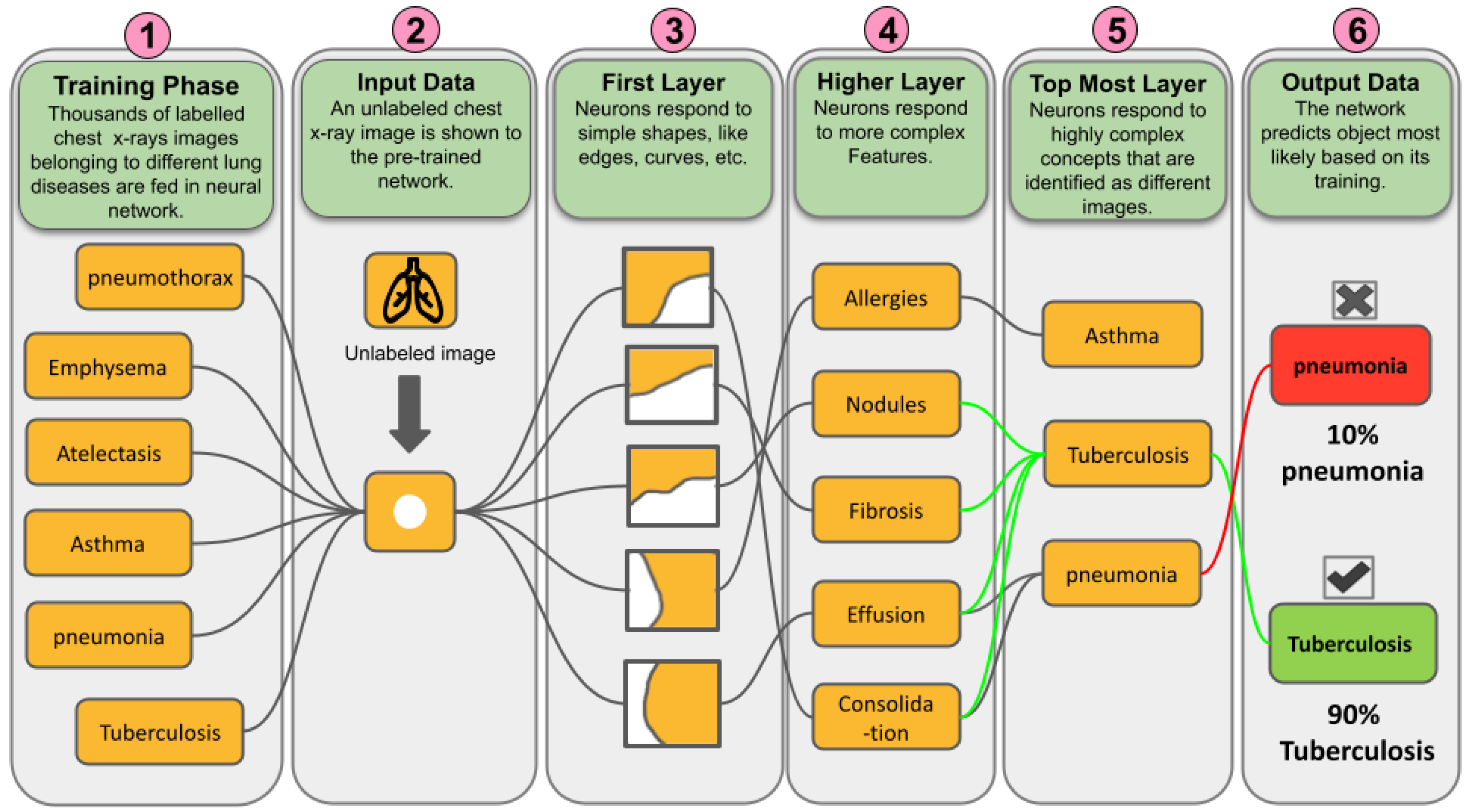
7. Advancing with Deep Learning
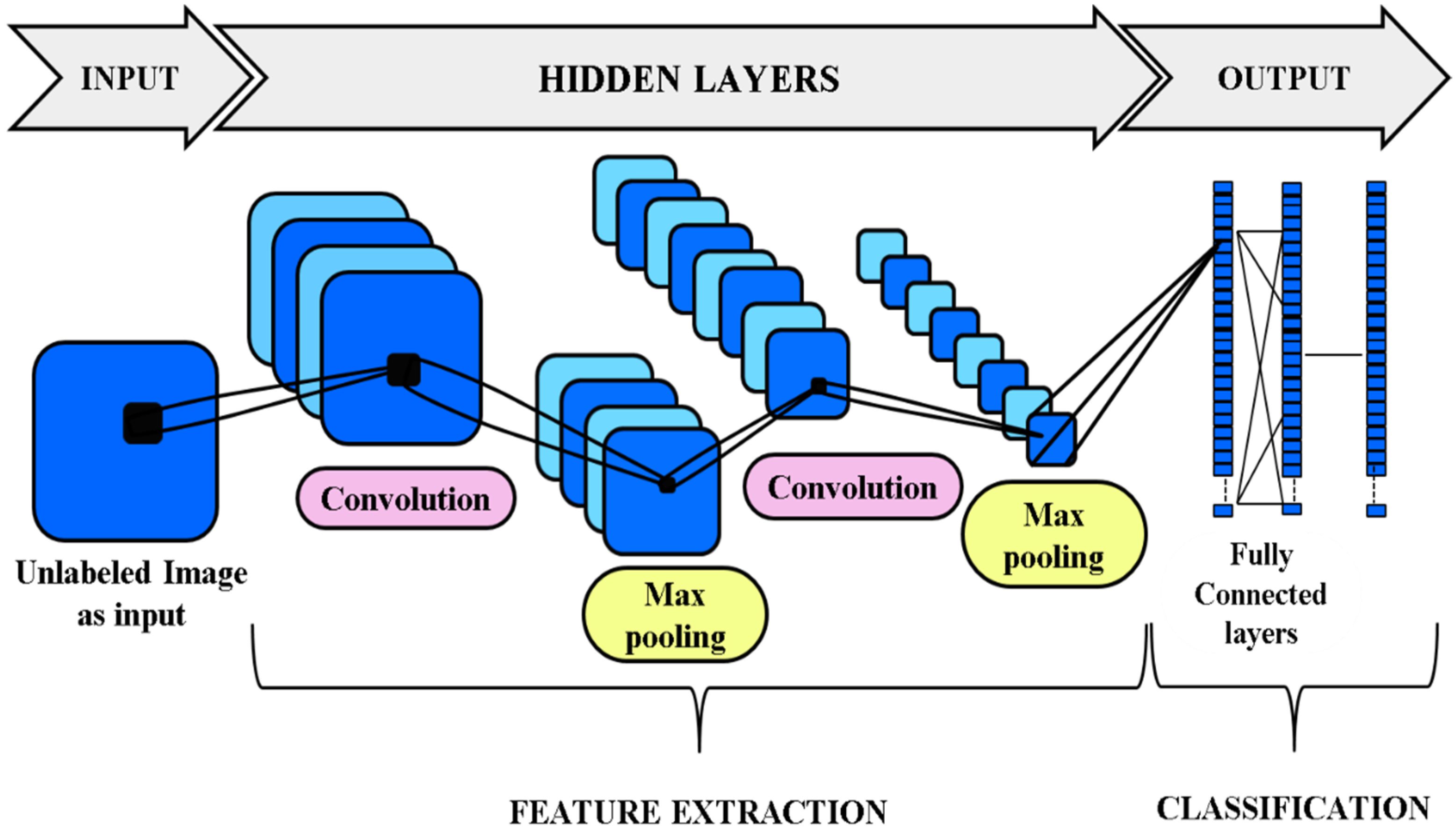
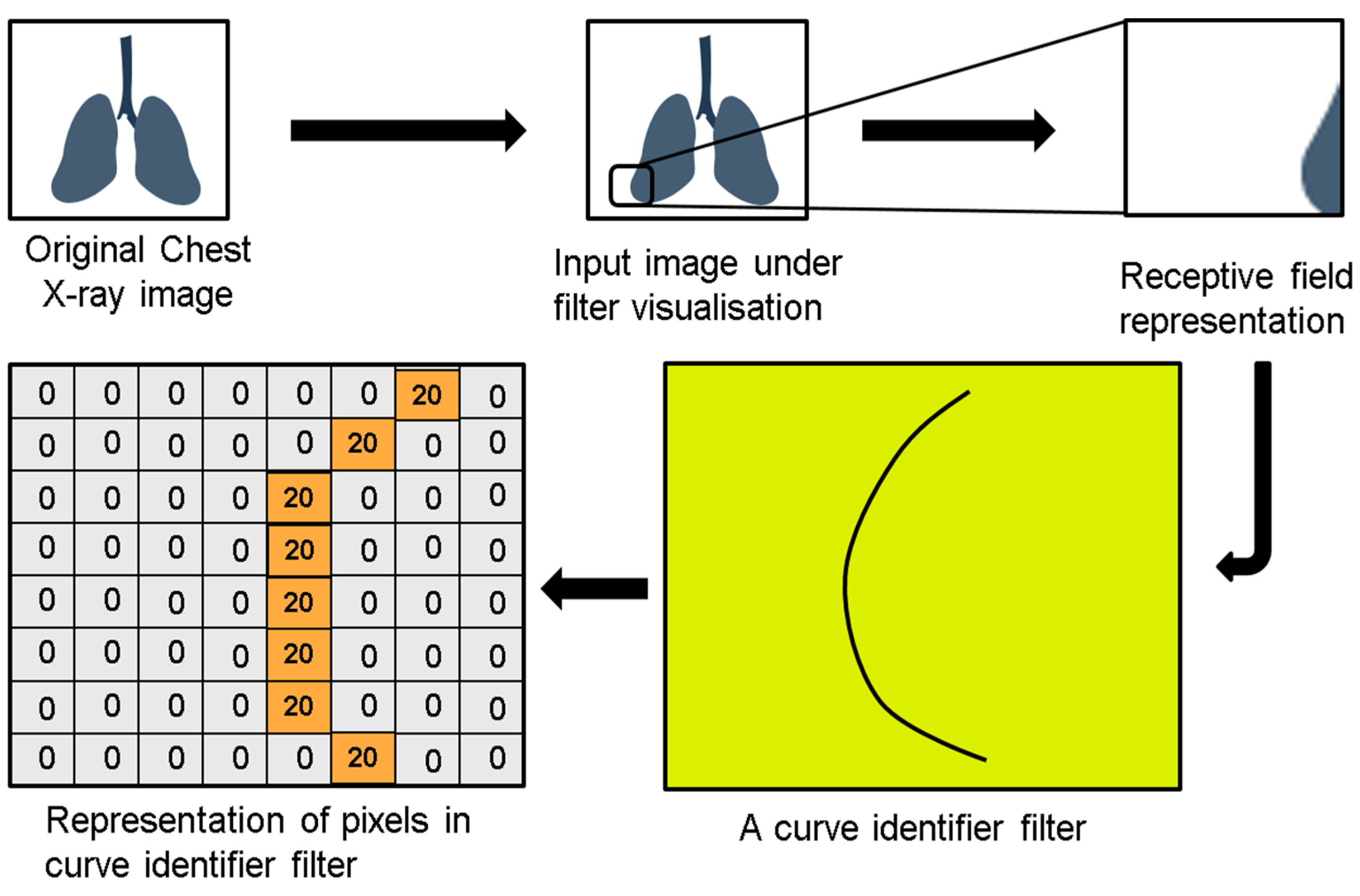
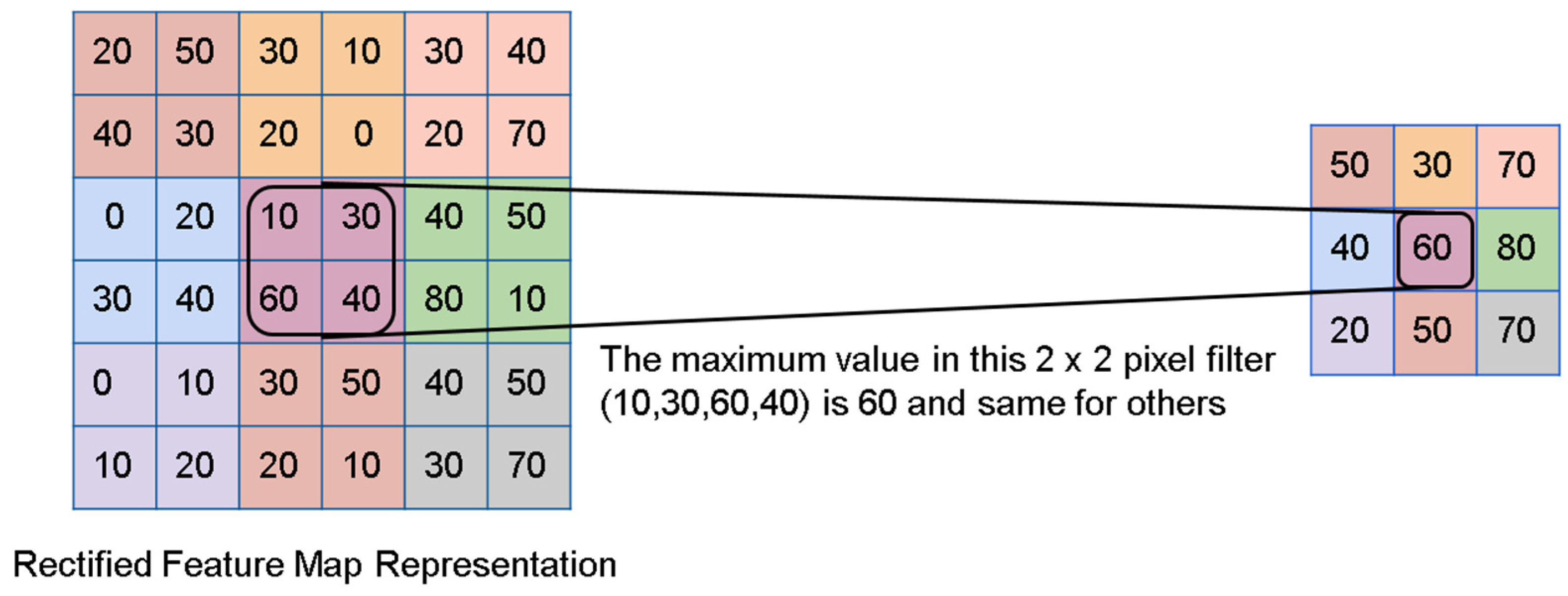
7.1. Convolutional Neural Networks (CNN)
7.2. Does CNN Make Our Job Easier in TB Diagnosis?
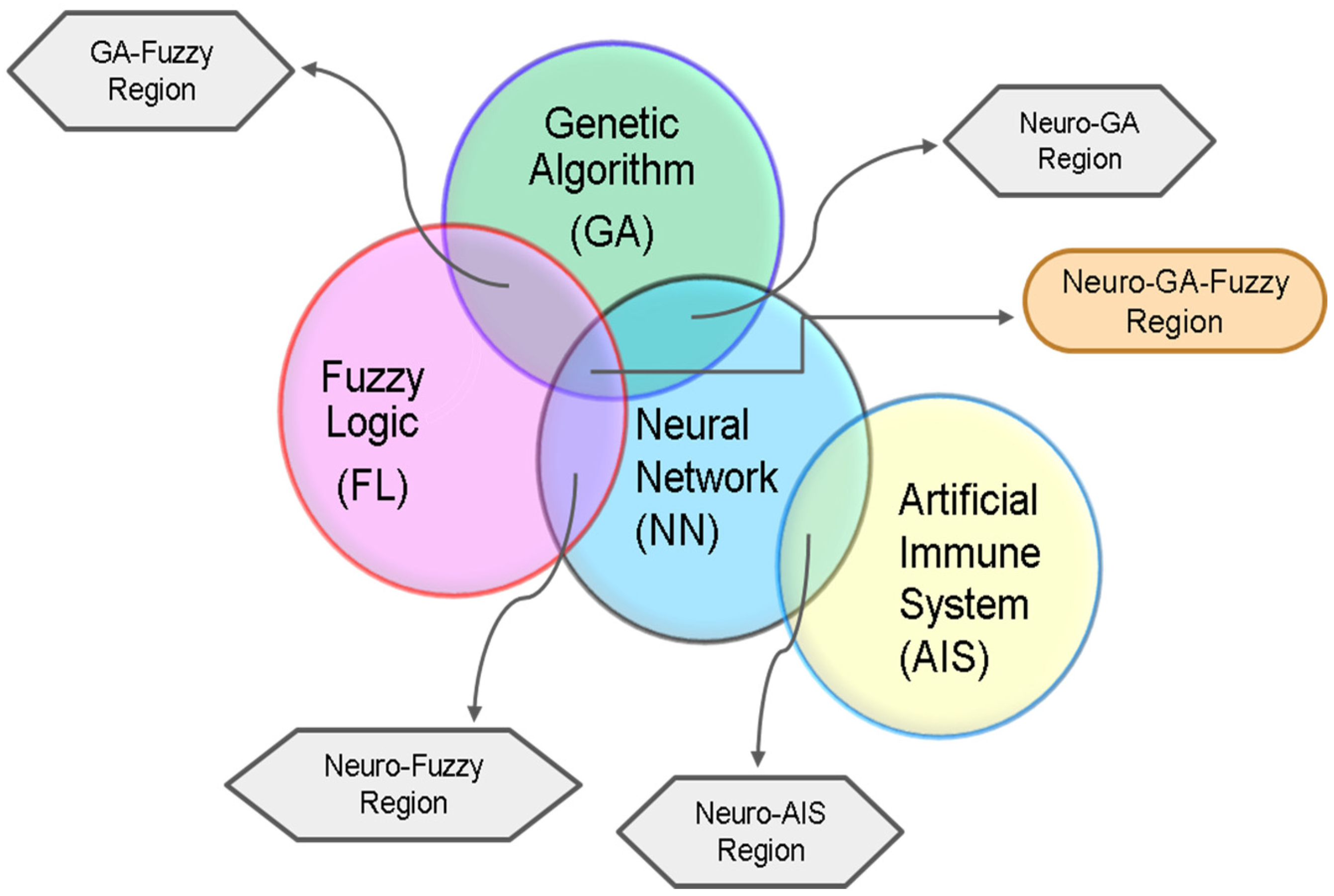
8. Integration of Deep Learning with Advanced Algorithms in TB Diagnosis
8.1. Adaptive Neuro-Fuzzy Inference System
8.2. Genetic Algorithm with Deep Learning
Genetic-Neuro-Fuzzy Inference System (GENFIS)
8.3. Artificial Immune System (AIS) with Deep Learning
9. Tools Built Using Deep Learning Techniques
10. Conclusions and Future Aspect
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. World Health Organization Global Tuberculosis Report 2020. 2020. Available online: http://apps.who.int/iris (accessed on 3 July 2022).
- Cole, S.T.; Riccardi, G. New tuberculosis drugs on the horizon. Curr. Opin. Microbiol. 2011, 14, 570–576. [Google Scholar] [CrossRef] [PubMed]
- Reid, M.J.A.; Arinaminpathy, N.; Bloom, A.; Bloom, B.R.; Boehme, C.; Chaisson, R.; Chin, D.P.; Churchyard, G.; Cox, H.; Ditiu, L.; et al. Building a tuberculosis-free world: The Lancet Commission on tuberculosis. Lancet 2019, 393, 1331–1384. [Google Scholar] [CrossRef] [Green Version]
- Melendez, J.; Sánchez, C.I.; Philipsen, R.H.H.M.; Maduskar, P.; Dawson, R.; Theron, G.; Dheda, K.; Van Ginneken, B. An automated tuberculosis screening strategy combining X-ray-based computer-aided detection and clinical information. Sci. Rep. 2016, 6, 25265. [Google Scholar] [CrossRef]
- Dye, C.; Williams, B.G. Criteria for the control of drug-resistant tuberculosis. Proc. Natl. Acad. Sci. USA 2000, 97, 8180–8185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, T.; Cheng, I.; Long, R.; Mandal, M. Novel coarse-to-fine dual scale technique for tuberculosis cavity detection in chest radiographs. Eurasip J. Image Video Process. 2013, 2013, 3. [Google Scholar] [CrossRef]
- Song, Y.L.; Yang, Y. Localization algorithm and implementation for focal of pulmonary tuberculosis chest image. In Proceedings of the 2010 International Conference on Machine Vision and Human-machine Interface, Kaifeng, China, 24–25 April 2010; pp. 361–364. [Google Scholar] [CrossRef]
- Jaeger, S.; Karargyris, A.; Antani, S.; Thoma, G. Detecting tuberculosis in radiographs using combined lung masks. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 4978–4981. [Google Scholar] [CrossRef] [Green Version]
- Sathitratanacheewin, S.; Sunanta, P.; Pongpirul, K. Deep learning for automated classification of tuberculosis-related chest X-Ray: Dataset distribution shift limits diagnostic performance generalizability. Heliyon 2020, 6, e04614. [Google Scholar] [CrossRef]
- Vajda, S.; Karargyris, A.; Jaeger, S.; Santosh, K.C.; Candemir, S.; Xue, Z.; Antani, S.K.; Thoma, G.R. Feature Selection for Automatic Tuberculosis Screening in Frontal Chest Radiographs. J. Med. Syst. 2018, 42, 146. [Google Scholar] [CrossRef]
- Cao, Y.; Liu, C.; Liu, B.; Brunette, M.J.; Zhang, N.; Sun, T.; Zhang, P.; Peinado, J.; Garavito, E.S.; Garcia, L.L.; et al. Improving Tuberculosis Diagnostics Using Deep Learning and Mobile Health Technologies among Resource-Poor and Marginalized Communities. In Proceedings of the 2016 IEEE First International Conference on Connected Health: Applications, Systems and Engineering Technologies (CHASE), Washington, DC, USA, 27–29 June 2016; pp. 274–281. [Google Scholar] [CrossRef]
- Hwang, S.; Kim, H.-E.; Jeong, J.; Kim, H.-J. A novel approach for tuberculosis screening based on deep convolutional neural networks. In Proceedings of the Medical Imaging 2016: Computer-Aided Diagnosis, San Diego, CA, USA, 27 February–3 March 2016; Volume 9785, p. 97852W. [Google Scholar] [CrossRef]
- Berthel, S.J.; Cooper, C.B.; Fotouhi, N. Chapter One—Tuberculosis. In Medicinal Chemistry Approaches to Tuberculosis and Trypanosomiasis; Annual Reports in Medicinal Chemistry Series; Elsevier: Amsterdam, The Netherlands, 2019; Volume 52, pp. 1–25. [Google Scholar]
- Richeldi, L. An Update on the Diagnosis of Tuberculosis Infection. Am. J. Respir. Crit. Care Med. 2006, 174, 736–742. [Google Scholar] [CrossRef] [Green Version]
- Subbaraman, R.; Nathavitharana, R.R.; Mayer, K.H.; Satyanarayana, S.; Chadha, V.K.; Arinaminpathy, N.; Pai, M. Constructing care cascades for active tuberculosis: A strategy for program monitoring and identifying gaps in quality of care. PLoS Med. 2019, 16, e1002754. [Google Scholar] [CrossRef]
- Jasmer, R.M.; Nahid, P.; Hopewell, P.C. Latent Tuberculosis Infection. J. Gastroenterol. Hepatol. 2015, 30, 13–26. [Google Scholar] [CrossRef]
- Noubissi, E.C.; Katte, J.-C.; Sobngwi, E. Diabetes and HIV. Curr. Diabetes Rep. 2018, 18, 125. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.K.; Mohan, A. Miliary Tuberculosis. ASM J. Microbiol. Spectr. 2017, 5, 491–513. [Google Scholar] [CrossRef]
- Mbuagbaw, L.; Guglielmetti, L.; Hewison, C.; Bakare, N.; Bastard, M.; Caumes, E.; Jachym, M.F.; Robert, J.; Veziris, N.; Khachatryan, N.; et al. Outcomes of bedaquiline treatment in patients with multidrug-resistant tuberculosis. Emerg. Infect. Dis. 2019, 25, 936–943. [Google Scholar] [CrossRef] [Green Version]
- Bhirud, P.; Joshi, A.; Hirani, N.; Chowdhary, A. Rapid Laboratory Diagnosis of Pulmonary Tuberculosis. Int. J. Mycobacteriol. 2017, 6, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Miotto, P.; Zhang, Y.; Cirillo, D.M.; Yam, W.C. Drug resistance mechanisms and drug susceptibility testing for tuberculosis. Respirology 2018, 23, 1098–1113. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Chest Radiography in Tuberculosis. 2016. Available online: http://www.who.int (accessed on 3 July 2022).
- Steingart, K.R.; Steingart, M.; Ng, V.; Hopewell, P.C.; Ramsay, A.; Cunningham, J.; Urbanczik, R.; Perkins, M.; Aziz, M.A.; Pai, M. Fluorescence versus conventional sputum smear microscopy for tuberculosis: A systematic review. Lancet Infect. Dis. 2006, 6, 570–581. [Google Scholar] [CrossRef]
- Ojha, A.; Banik, S.; Melanthota, S.K.; Mazumder, N. Light emitting diode (LED) based fluorescence microscopy for tuberculosis detection: A review. Lasers Med. Sci. 2020, 35, 1431–1437. [Google Scholar] [CrossRef]
- Cruciani, M.; Scarparo, C.; Malena, M.; Bosco, O.; Serpelloni, G.; Mengoli, C. Meta-Analysis of BACTEC MGIT 960 and BACTEC 460 TB, with or without Solid Media, for Detection of Mycobacteria. J. Clin. Microbiol. 2004, 42, 2321–2325. [Google Scholar] [CrossRef] [Green Version]
- Uplekar, M.; Weil, D.; Lonnroth, K.; Jaramillo, E.; Lienhardt, C.; Dias, H.M.; Falzon, D.; Floyd, K.; Gargioni, G.; Getahun, H.; et al. WHO’s new End TB Strategy. Lancet 2015, 385, 1799–1801. [Google Scholar] [CrossRef]
- Steingart, K.R.; Sohn, H.; Schiller, I.; Kloda, L.A.; Boehme, C.C.; Pai, M.; Dendukuri, N. Xpert® MTB/RIF assay for pulmonary tuberculosis and rifampicin resistance in adults. Cochrane Database Syst. Rev. 2013, 1, CD009593. [Google Scholar] [CrossRef] [Green Version]
- Ling, D.I.; Zwerling, A.A.; Pai, M. GenoType MTBDR assays for the diagnosis of multidrug-resistant tuberculosis: A meta-analysis. Eur. Respir. J. 2008, 32, 1165–1174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation. The Use of Molecular Line Probe Assays for the Detection of Resistance to Second-Line Anti-Tuberculosis Drugs: Policy Guidance. 2019. Available online: https://apps.who.int/iris/handle/10665/246131 (accessed on 3 July 2022).
- World Health Organisation. The Use of Loop-Mediated Isothermal Amplification (TB-LAMP) for the Diagnosis of Pulmonary Tuberculosis: Policy Guidance. 2016. Available online: https://apps.who.int/iris/handle/10665/249154 (accessed on 3 July 2022).
- Virenfeldt, J.; Rudolf, F.; Camara, C.; Furtado, A.; Gomes, V.; Aaby, P.; Petersen, E.; Wejse, C. Treatment delay affects clinical severity of tuberculosis: A longitudinal cohort study. BMJ Open 2014, 4, e004818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, L.; He, X.; He, D.; Wang, K.; Qin, D. Biosensing Technologies for Mycobacterium tuberculosis Detection: Status and New Developments. Clin. Dev. Immunol. 2011, 2011, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, S.; Kakkar, V. Recent technological advancements in tuberculosis diagnostics—A review. Biosens. Bioelectron. 2018, 115, 14–29. [Google Scholar] [CrossRef] [PubMed]
- Rosenblatt, F. The perceptron: A probabilistic model for information storage and organization in the brain. Psychol. Rev. 1958, 65, 386–408. [Google Scholar] [CrossRef] [Green Version]
- Abe, H.; Kumazawa, S.; Taji, T.; Sasaki, S.I. Applications of computerized pattern recognition: A survey of correlations between pharmacological activities and mass spectra. Biol. Mass Spectrom. 1976, 3, 151–154. [Google Scholar] [CrossRef]
- Maliwan, N.; Reid, R.W.; Pliska, S.R.; Bird, T.J.; Zvetina, J.R. Direct diagnosis of tuberculosis by computer assisted pattern recognition gas chromatographic analysis of sputum. Biomed. Chromatogr. 1991, 5, 165–170. [Google Scholar] [CrossRef]
- Asada, N.; Doi, K.; MacMahon, H.; Montner, S.M.; Giger, M.L.; Abé, C.; Wu, Y. Potential usefulness of an artificial neural network for differential diagnosis of interstitial lung diseases: Pilot study. Radiology 1990, 177, 857–860. [Google Scholar] [CrossRef]
- Veropoulos, K.; Campbell, C.; Learmonth, G.; Knight, B.; Simpson, J. The Automated Identification of Tubercle Bacilli using Image Processing and Neural Computing Techniques. In ICANN 1998. Perspectives in Neural Computing; Niklasson, L., Bodén, M., Ziemke, T., Eds.; Springer: London, UK, 1998; pp. 797–802. [Google Scholar] [CrossRef]
- El-Solh, A.A.; Hsiao, C.-B.; Goodnough, S.; Serghani, J.; Grant, B.J. Predicting Active Pulmonary Tuberculosis Using an Artificial Neural Network. Chest 1999, 116, 968–973. [Google Scholar] [CrossRef] [Green Version]
- Hearst, M.A.; Dumais, S.T.; Osuna, E.; Platt, J.; Scholkopf, B. Support Vector Machines. IEEE Intell. Syst. Their Appl. 1998, 13, 18–28. [Google Scholar] [CrossRef] [Green Version]
- El-Solh, A.; Mylotte, J.; Sherif, S.; Serghani, J.; Grant, B.J. Validity of a decision tree for predicting active pulmonary tuberculosis. Am. J. Respir. Crit. Care Med. 1997, 155, 1711–1716. [Google Scholar] [CrossRef] [PubMed]
- Ho, T.K. Random Decision Forests. In Proceedings of the 3rd International Conference on Document Analysis and Recognition, Montreal, QC, Canada, 14–16 August 1995; pp. 278–282. [Google Scholar] [CrossRef]
- Osman, M.K.; Ahmad, F.; Saad, Z.; Mashor, M.Y.; Jaafar, H. A genetic algorithm-neural network approach for Mycobacterium tuberculosis detection in Ziehl-Neelsen stained tissue slide images. In Proceedings of the 2010 10th International Conference on Intelligent Systems Design and Applications, Cairo, Egypt, 29 November–1 December 2010; pp. 1229–1234. [Google Scholar] [CrossRef]
- Semogan, A.R.C.; Gerardo, B.D.; Tanguilig, B.T.; De Castro, J.T.; Cervantes, L.F. A rule-based fuzzy diagnostics decision support system for tuberculosis. In Proceedings of the 2011 Ninth International Conference on Software Engineering Research, Management and Applications, Baltimore, MD, USA, 10–12 August 2011; pp. 60–63. [Google Scholar] [CrossRef]
- Gao, X.W.; Qian, Y. Prediction of Multidrug-Resistant TB from CT Pulmonary Images Based on Deep Learning Techniques. Mol. Pharm. 2018, 15, 4326–4335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raymond, J.L.; Medina, J.F. Computational Principles of Supervised Learning in the Cerebellum. Annu. Rev. Neurosci. 2018, 41, 233–253. [Google Scholar] [CrossRef] [PubMed]
- Ayaz, M.; Shaukat, F.; Raja, G. Ensemble learning based automatic detection of tuberculosis in chest X-ray images using hybrid feature descriptors. Phys. Eng. Sci. Med. 2021, 44, 183–194. [Google Scholar] [CrossRef]
- Weber, M.; Welling, M.; Perona, P. Unsupervised learning of models for recognition. In Computer Vision—ECCV 2000. ECCV 2000. Lecture Notes in Computer Science; Springer: Berlin, Heidelberg, 2000; Volume 1842, pp. 18–32. [Google Scholar] [CrossRef]
- Meier, N.R.; Sutter, T.M.; Jacobsen, M.; Ottenhoff, T.H.M.; Vogt, J.E.; Ritz, N. Machine Learning Algorithms Evaluate Immune Response to Novel Mycobacterium tuberculosis Antigens for Diagnosis of Tuberculosis. Front. Cell. Infect. Microbiol. 2021, 10, 594030. [Google Scholar] [CrossRef]
- Karmani, P.; Chandio, A.A.; Karmani, V.; Soomro, J.A.; Korejo, I.A.; Chandio, M.S. Taxonomy on Healthcare System Based on Machine Learning Approaches: Tuberculosis Disease Diagnosis. Int. J. Comput. Digit. Syst. 2020, 9, 1199–1212. [Google Scholar] [CrossRef]
- Orjuela-Cañón, A.D.; Mendoza, J.E.C.; García, C.E.A.; Vela, E.P.V. Tuberculosis diagnosis support analysis for precarious health information systems. Comput. Methods Programs Biomed. 2018, 157, 11–17. [Google Scholar] [CrossRef]
- Aguiar, F.S.; Torres, R.C.; Pinto, J.V.F.; Kritski, A.L.; Seixas, J.M.; Mello, F.C.Q. Development of two artificial neural network models to support the diagnosis of pulmonary tuberculosis in hospitalized patients in Rio de Janeiro, Brazil. Med. Biol. Eng. Comput. 2016, 54, 1751–1759. [Google Scholar] [CrossRef]
- Kumar, A.; Padhy, S.K.; Takkar, B.; Chawla, R. Artificial intelligence in diabetic retinopathy: A natural step to the future. Indian J. Ophthalmol. 2019, 67, 1004–1009. [Google Scholar] [CrossRef]
- Van Engelen, J.E.; Hoos, H.H. A survey on semi-supervised learning. Mach. Learn. 2019, 109, 373–440. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.K.; Yi, P.H.; Hager, G.D.; Lin, C.T. Refining dataset curation methods for deep learning-based automated tuberculosis screening. J. Thorac. Dis. 2020, 12, 5078–5085. [Google Scholar] [CrossRef] [PubMed]
- Reker, D.; Schneider, P.; Schneider, G.; Brown, J.B. Active learning for computational chemogenomics. Future Med. Chem. 2017, 9, 381–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melendez, J.; van Ginneken, B.; Maduskar, P.; Philipsen, R.H.H.M.; Ayles, H.; Sanchez, C.I. On Combining Multiple-Instance Learning and Active Learning for Computer-Aided Detection of Tuberculosis. IEEE Trans. Med. Imaging 2015, 35, 1013–1024. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, B.G. Expert systems: Working systems and the research literature. Expert Syst. 1986, 3, 32–50. [Google Scholar] [CrossRef]
- Rahman, T.; Khandakar, A.; Kadir, M.A.; Islam, K.R.; Islam, K.F.; Mazhar, R.; Hamid, T.; Islam, M.T.; Kashem, S.; Bin Mahbub, Z.; et al. Reliable Tuberculosis Detection Using Chest X-ray with Deep Learning, Segmentation and Visualization. IEEE Access 2020, 8, 191586–191601. [Google Scholar] [CrossRef]
- Rashid, R.; Khawaja, S.G.; Akram, M.U.; Khan, A.M. Hybrid RID Network for Efficient Diagnosis of Tuberculosis from Chest X-rays. In Proceedings of the 2018 9th Cairo International Biomedical Engineering Conference (CIBEC), Cairo, Egypt, 20–22 December 2018; pp. 167–170. [Google Scholar] [CrossRef]
- Kuddus, A.; Meehan, M.T.; White, L.J.; McBryde, E.S.; Adekunle, A.I. Modeling drug-resistant tuberculosis amplification rates and intervention strategies in Bangladesh. PLoS ONE 2020, 15, e0236112. [Google Scholar] [CrossRef]
- Xu, J.; Xue, K.; Zhang, K. Current status and future trends of clinical diagnoses via image-based deep learning. Theranostics 2019, 9, 7556–7565. [Google Scholar] [CrossRef]
- Ko, C.-H.; Cheng, M.-Y. Hybrid use of AI techniques in developing construction management tools. Autom. Constr. 2003, 12, 271–281. [Google Scholar] [CrossRef]
- Riad, N.; Arditi, D.; Mohammadi, J. A conceptual model for claim management in construction: An ai approach. Comput. Struct. 1991, 40, 67–74. [Google Scholar] [CrossRef]
- Miller, D.D. The medical AI insurgency: What physicians must know about data to practice with intelligent machines. NPJ Digit. Med. 2019, 2, 62. [Google Scholar] [CrossRef] [Green Version]
- Mittelstadt, B.; Russell, C.; Wachter, S. Explaining explanations in AI. In Proceedings of the Conference on Fairness, Accountability, and Transparency (FAT* ’19), Atlanta, GA, USA, 29–31 January 2019; pp. 279–288. [Google Scholar] [CrossRef]
- Hase, P.; Bansal, M. Evaluating Explainable AI: Which Algorithmic Explanations Help Users Predict Model Behavior? In Proceedings of the 58th Annual Meeting of the Association for Computational Linguistics, Online, 4 May 2020; pp. 5540–5552. [Google Scholar] [CrossRef]
- Liu, S.; Deng, W. Very deep convolutional neural network based image classification using small training sample size. In Proceedings of the 2015 3rd IAPR Asian Conference on Pattern Recognition (ACPR), Kuala Lumpur, Malaysia, 3–6 November 2015; pp. 730–734. [Google Scholar] [CrossRef]
- Lakhani, P.; Sundaram, B. Deep Learning at Chest Radiography: Automated Classification of Pulmonary Tuberculosis by Using Convolutional Neural Networks. Radiology 2017, 284, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Che, J.; Ding, H.; Zhou, X. Chejiao at ImageCLEFmed Tuberculosis 2020: CT Report Generation Based on Transfer learning. In Proceedings of the CLEF2020 Working Notes. CEUR Workshop Proceedings, Thessaloniki, Greece, 22–25 September 2020; pp. 22–25. [Google Scholar]
- Gentili, A. ImageCLEF2018: Transfer learning for deep learning with CNN for tuberculosis classification. CEUR Workshop Proc. 2018, 2125, 6–12. [Google Scholar]
- Jaeger, S.; Candemir, S.; Antani, S.; Wáng, Y.-X.J.; Lu, P.-X.; Thoma, G. Two public chest X-ray datasets for computer-aided screening of pulmonary diseases. Quant. Imaging Med. Surg. 2014, 4, 475–477. [Google Scholar] [CrossRef] [PubMed]
- Filho, M.E.C.; Galliez, R.M.; Bernardi, F.A.; de Oliveira, L.L.; Kritski, A.; Santos, M.K.; Alves, D. Preliminary Results on Pulmonary Tuberculosis Detection in Chest X-Ray Using Convolutional Neural Networks. In Computational Science—ICCS 2020. ICCS 2020; Lecture Notes in Computer Science Series; Springer: Cham, Switzerland, 2020; Volume 12140, pp. 563–576. [Google Scholar] [CrossRef]
- Belarus Tuberculosis Database and TB Portal. Available online: http://tuberculosis.by/ (accessed on 3 July 2022).
- Liu, Y.; Wu, Y.-H.; Ban, Y.; Wang, H.; Cheng, M.-M. Rethinking computer-aided tuberculosis diagnosis. In Proceedings of the IEEE Computer Society Conference on Computer Vision and Pattern Recognition, Seattle, WA, USA, 13–19 June 2020; pp. 2643–2652. [Google Scholar] [CrossRef]
- Chauhan, A.; Chauhan, D.; Rout, C. Role of Gist and PHOG Features in Computer-Aided Diagnosis of Tuberculosis without Segmentation. PLoS ONE 2014, 9, e112980. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.I.; Mishra, S.; Yadav, V.K.; Chauhan, A.; Sarkar, M.; Sharma, S.K.; Rout, C. Ziehl–Neelsen sputum smear microscopy image database: A resource to facilitate automated bacilli detection for tuberculosis diagnosis. J. Med. Imaging 2017, 4, 027503. [Google Scholar] [CrossRef]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A simple way to prevent neural networks from overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar]
- Denil, M.; Shakibi, B.; Dinh, L.; Ranzato, M.; de Freitas, N. Predicting parameters in deep learning. Adv. Neural Inf. Process. Syst. 2013, 26, 1–9. [Google Scholar]
- Gregory, R.W.; Henfridsson, O.; Kaganer, E.; Kyriakou, S.H. The Role of Artificial Intelligence and Data Network Effects for Creating User Value. Acad. Manag. Rev. 2021, 46, 534–551. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Schmidhuber, J. Deep Learning in Neural Networks: An Overview. Neural Netw. 2015, 61, 85–117. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.; Zhang, M.; Chen, T.; Sun, Z.; Ma, Y.; Yu, B. Recent advances in convolutional neural network acceleration. Neurocomputing 2018, 323, 37–51. [Google Scholar] [CrossRef] [Green Version]
- Shin, H.-C.; Roth, H.R.; Gao, M.; Lu, L.; Xu, Z.; Nogues, I.; Yao, J.; Mollura, D.; Summers, R.M. Deep Convolutional Neural Networks for Computer-Aided Detection: CNN Architectures, Dataset Characteristics and Transfer Learning. IEEE Trans. Med. Imaging 2016, 35, 1285–1298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chauhan, R.; Ghanshala, K.K.; Joshi, R.C. Convolutional Neural Network (CNN) for Image Detection and Recognition. In Proceedings of the 2018 First International Conference on Secure Cyber Computing and Communication (ICSCCC), Jalandhar, India, 15–17 December 2018; IEEE: Piscataway, NJ, USA; pp. 278–282. [Google Scholar] [CrossRef]
- Abbas, A.; Abdelsamea, M.M. Learning Transformation for Automated classification of manifestation of Tuberculosis using Convolutional Neural Network. In Proceedings of the 2018 13th International Conference on Computer Engineering and Systems (ICCES), Cairo, Egypt, 18–19 December 2018; pp. 122–126. [Google Scholar] [CrossRef]
- Ahsan, M.; Gomes, R.; Denton, A. Application of a convolutional neural network using transfer learning for tuberculosis detection. In Proceedings of the 2019 IEEE International Conference on Electro Information Technology (EIT), Brookings, SD, USA, 20–22 May 2019; pp. 427–433. [Google Scholar] [CrossRef]
- Andika, L.A.; Pratiwi, H.; Handajani, S.S. Convolutional neural network modeling for classification of pulmonary tuberculosis disease. J. Physics: Conf. Ser. 2020, 1490, 012020. [Google Scholar] [CrossRef]
- Lopez-Garnier, S.; Sheen, P.; Zimic, M. Automatic diagnostics of tuberculosis using convolutional neural networks analysis of MODS digital images. PLoS ONE 2019, 14, e0212094. [Google Scholar] [CrossRef]
- Msonda, P.; Uymaz, S.A.; Karaağaç, S.S. Spatial Pyramid Pooling in Deep Convolutional Networks for Automatic Tuberculosis Diagnosis. Trait. Du Signal 2020, 37, 1075–1084. [Google Scholar] [CrossRef]
- Zhang, Y.-D.; Nayak, D.R.; Zhang, X.; Wang, S.-H. Diagnosis of secondary pulmonary tuberculosis by an eight-layer improved convolutional neural network with stochastic pooling and hyperparameter optimization. J. Ambient Intell. Humaniz. Comput. 2020, 1–18. [Google Scholar] [CrossRef]
- Liu, C.; Cao, Y.; Alcantara, M.; Liu, B.; Brunette, M.; Peinado, J.; Curioso, W. TX-CNN: Detecting tuberculosis in chest X-ray images using convolutional neural network. In Proceedings of the 2017 IEEE International Conference on Image Processing (ICIP), Beijing, China, 17–20 September 2017; pp. 2314–2318. [Google Scholar] [CrossRef]
- Rohilla, A.; Hooda, R.; Mittal, A. TB Detection in Chest Radiograph Using Deep Learning Architecture. Int. J. Adv. Res. Sci. Eng. 2017, 6, 1073–1084. [Google Scholar]
- Vilone, G.; Luca, L. Notions of explainability and evaluation approaches for explainable artificial intelligence. Inf. Fusion 2021, 76, 89–106. [Google Scholar] [CrossRef]
- Adadi, A.; Berrada, M. Explainable AI for Healthcare: From Black Box to Interpretable Models. In Advances in Intelligent Systems and Computing; Springer: Singapore, 2020; Volume 1076, pp. 327–337. [Google Scholar] [CrossRef]
- Barredo Arrieta, A.; Díaz-Rodríguez, N.; Del Ser, J.; Bennetot, A.; Tabik, S.; Barbado, A.; Garcia, S.; Gil-Lopez, S.; Molina, D.; Benjamins, R.; et al. Explainable Explainable Artificial Intelligence (XAI): Concepts, taxonomies, opportunities and chal-lenges toward responsible AI. Inf. Fusion 2020, 58, 82–115. [Google Scholar] [CrossRef] [Green Version]
- Doshi-Velez, F.; Been, K. Towards a rigorous science of interpretable machine learning. arXiv 2017, arXiv:1702.08608. [Google Scholar]
- Asay, B.C.; Edwards, B.B.; Andrews, J.; Ramey, M.E.; Richard, J.D.; Podell, B.K.; Gutiérrez, J.F.M.; Frank, C.B.; Magunda, F.; Robertson, G.T.; et al. Digital Image Analysis of Heterogeneous Tuberculosis Pulmonary Pathology in Non-Clinical Animal Models using Deep Convolutional Neural Networks. Sci. Rep. 2020, 10, 6047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chithra, R.S.; Jagatheeswari, P. Severity detection and infection level identification of tuberculosis using deep learning. Int. J. Imaging Syst. Technol. 2020, 30, 994–1011. [Google Scholar] [CrossRef]
- Chang, R.I.; Chiu, Y.H.; Lin, J.W. Two-stage classification of tuberculosis culture diagnosis using convolutional neural network with transfer learning. J. Supercomput. 2020, 76, 8641–8656. [Google Scholar] [CrossRef]
- Nafisah, S.I.; Ghula, M. Tuberculosis detection in chest radiograph using convolutional neural network architecture and explainable artificial intelligence. Neural Comput. Appl. 2022, 1–21. [Google Scholar] [CrossRef]
- Pasa, F.; Golkov, V.; Pfeiffer, F.; Cremers, D.; Pfeiffer, D. Efficient deep network architectures for fast chest X-ray tuberculosis screening and visualization. Sci. Rep. 2019, 9, 6268. [Google Scholar] [CrossRef] [Green Version]
- Ahmadi, H.; Gholamzadeh, M.; Shahmoradi, L.; Nilashi, M.; Rashvand, P. Diseases diagnosis using fuzzy logic methods: A systematic and meta-analysis review. Comput. Methods Programs Biomed. 2018, 161, 145–172. [Google Scholar] [CrossRef]
- Sharma, T.; Singh, V.; Sudhakaran, S.; Verma, N. Fuzzy based Pooling in Convolutional Neural Network for Image Classification. In Proceedings of the IEEE International Conference on Fuzzy Systems, New Orleans, LA, USA, 23–26 June 2019; pp. 1–6. [Google Scholar] [CrossRef]
- Kang, C.; Yu, X.; Wang, S.H.; Guttery, D.S.; Pandey, H.M.; Tian, Y.; Zhang, Y. A Heuristic Neural Network Structure Relying on Fuzzy Logic for Images Scoring. IEEE Trans. Fuzzy Syst. 2021, 29, 34–45. [Google Scholar] [CrossRef] [Green Version]
- Shrivastava, A.K.; Rajak, A. Modeling Pulmonary Tuberculosis using Adaptive Neuro Fuzzy Inference System. Int. J. Innov. Res. Comput. Sci. Technol. 2016, 4, 24–27. [Google Scholar] [CrossRef]
- Shrivastava, A.K.; Rajak, A.; Bhardwaj, S. Detection of tuberculosis based on multiple parameters using ANFIS. In Proceedings of the 3rd International Conference on Innovative Applications of Computational Intelligence on Power, Energy and Controls with their Impact on Humanity, CIPECH 2018, Ghaziabad, India, 1–2 November 2018; pp. 120–124. [Google Scholar] [CrossRef]
- Goni, I.; Ngene, C.U.; Manga, I.; Nata’ala, A. Intelligent System for Diagnosing Tuberculosis Using Adaptive Neuro-Fuzzy. Asian J. Res. Comput. Sci. 2018, 2, 1–9. [Google Scholar] [CrossRef]
- Oreski, S.; Oreski, G. Genetic algorithm-based heuristic for feature selection in credit risk assessment. Expert Syst. Appl. 2014, 41, 2052–2064. [Google Scholar] [CrossRef]
- Brabazon, A.; O’Neill, M.; McGarraghy, S. Genetic algorithm. Nat. Comput. Algorithms 2015, 28, 21–42. [Google Scholar] [CrossRef]
- Maulik, U.; Bandyopadhyay, S. Genetic algorithm-based clustering technique. Pattern Recognit. 2000, 33, 1455–1465. [Google Scholar] [CrossRef]
- Geetha, P.V.; Lukshmi, R.A.; Venkatesan, P. Tuberculosis Disease Classification using Genetic-neuro Expert System. Indian J. Sci. Technol. 2014, 7, 421–425. [Google Scholar] [CrossRef]
- Vally, D.; Sarma, C.H.V. Diagnosis Chest Diseases Using Neural Network and Genetic Hybrid Algorithm. Int. J. Eng. Res. Appl. 2015, 5, 20–26. [Google Scholar]
- Omisore, M.O.; Samuel, O.W.; Atajeromavwo, E.J. A Genetic-Neuro-Fuzzy inferential model for diagnosis of tuberculosis. Appl. Comput. Informatics. 2017, 13, 27–37. [Google Scholar] [CrossRef] [Green Version]
- Vathana, R.B.; Balasubramanian, R. Genetic-Neuro-Fuzzy Inferential Model for Tuberculosis Detection. Int. J. Appl. Eng. Res. 2018, 13, 13308–13312. [Google Scholar]
- Greensmith, J.; Whitbrook, A. Aickelin Artificial Immune Systems. Int. J. Recent Res. Appl. Stud. 2010, 3, 21–448. [Google Scholar] [CrossRef] [Green Version]
- Dasgupta, D.; Yu, S.; Nino, F. Recent advances in artificial immune systems: Models and applications. Appl. Soft Comput. J. 2011, 11, 1574–1587. [Google Scholar] [CrossRef]
- Er, O.; Yumusak, N.; Temurtas, F. Diagnosis of chest diseases using artificial immune system. Expert Syst. Appl. 2012, 39, 1862–1868. [Google Scholar] [CrossRef]
- Shamshirband, S.; Hessam, S.; Javidnia, H.; Amiribesheli, M.; Vahdat, S.; Petković, D.; Gani, A.; Kiah, L. Tuberculosis disease diagnosis using artificial immune recognition system. Int. J. Med. Sci. 2014, 11, 508–514. [Google Scholar] [CrossRef] [Green Version]
- Saybani, M.R.; Shamshirband, S.; Hormozi, S.G.; Wah, T.Y.; Aghabozorgi, S.; Pourhoseingholi, M.A.; Olariu, T. Diagnosing tuberculosis with a novel support vector machine-based artificial immune recognition system, Iran. Red Crescent Med. J. 2015, 17, e24557. [Google Scholar] [CrossRef] [Green Version]
- Saybani, M.R.; Shamshirband, S.; Golzari, S.; Wah, T.Y.; Saeed, A.; Kiah, L.M.; Balas, V.E. RAIRS2 a new expert system for diagnosing tuberculosis with real-world tournament selection mechanism inside artificial immune recognition system. Med. Biol. Eng. Comput. 2016, 54, 385–399. [Google Scholar] [CrossRef] [PubMed]
- Pappalardo, F.; Russo, G.; Pennisi, M.; Sgroi, G.; Palumbo, G.A.P.; Motta, S.; Fichera, E. An agent based modeling approach for the analysis of tuberculosis-Immune system dynamics. In Proceedings of the 2018 IEEE International Conference on Bioinformatics and Biomedicine, BIBM, Madrid, Spain, 3–6 December 2019; pp. 1386–1392. [Google Scholar] [CrossRef]
- World Health Organization (WHO). The End TB Strategy. 2013. Available online: http://www.who.int (accessed on 3 July 2022).
- World Health Organization (WHO). Operational Handbook on Tuberculosis. 2020. Available online: http://www.who.int (accessed on 3 July 2022).
- Qin, Z.Z.; Naheyan, T.; Ruhwald, M.; Denkinger, C.M.; Gelaw, S.; Nash, M.; Creswell, J.; Kik, S.V. A new resource on artificial intelligence powered computer automated detection software products for tuberculosis programmes and implementers. Tuberculosis 2021, 127, 102049. [Google Scholar] [CrossRef]
- AI4HLTH Resource Database. Product Profile: Delft Imaging. 2020. Available online: http://www.delft.care (accessed on 3 July 2022).
- AI4HLTH Resource Database. Product Profile: Infervision. 2020. Available online: http://www.infervision.com (accessed on 3 July 2022).
- AI4HLTH Resource Database. Product Profile: JLK. 2020. Available online: http://www.jlkgroup.com (accessed on 3 July 2022).
- AI4HLTH Resource Database. Product Profile: Lunit. 2020. Available online: http://www.lunit.io (accessed on 3 July 2022).
- AI4HLTH Resource Database. Product Profile: Qure. ai. 2020. Available online: http://www.qure.ai (accessed on 3 July 2022).
- AI4HLTH Resource Database. Product Profile: Radisen. 2020. Available online: http://www.radisentech.com (accessed on 3 July 2022).
- AI4HLTH Resource Database. Product Profile: Artelus. 2020. Available online: https://www.artelus.com/ (accessed on 3 July 2022).
- AI4HLTH Resource Database. Product Profile: DeepTek Inc. 2020. Available online: https://www.deeptek.ai (accessed on 3 July 2022).
- AI4HLTH Resource Database. Product Profile: Dr CADx. 2020. Available online: https://www.drcadx.com (accessed on 3 July 2022).
- AI4HLTH Resource Database. Product Profile: EPCON. 2021. Available online: https://www.epcon.ai (accessed on 3 July 2022).
- AI4HLTH Resource Database. Product Profile: JF Healthcare. 2021. Available online: http://www.jfhealthcare.com/ (accessed on 3 July 2022).
- Lee, S.; Hyun, J.S.; Sungwon, K.; Eun-Kyung, K. Successful Implementation of an Artificial Intelligence-Based Computer-Aided Detection System for Chest Radiography in Daily Clinical Practice. Korean J. Radiol. 2022, 23, e52. [Google Scholar] [CrossRef] [PubMed]
- Qin, Z.Z.; Shahriar, A.; Mohammad, S.S.; Kishor, P.; Ahammad SS, A.; Tasneem, N.; Rachael, B.; Sayera, B.; Jacob, C. Tuberculosis detection from chest x-rays for triaging in a high tuberculosis-burden setting: An evaluation of five artificial intelligence algorithms. Lancet Digit. Health 2021, 3, e543–e554. [Google Scholar] [CrossRef]
- Khan, F.A.; Arman, M.; Gamuchirai, T.; Ahsana, N.; Syed, K.A.; Andrea, B.; Dick, M.; James, C.J.; Aamir, J.K.; Saima, S. Chest x-ray analysis with deep learning-based software as a triage test for pulmonary tuberculosis: A prospective study of diagnostic accuracy for culture-confirmed disease. Lancet Digit. Health 2020, 2, e573–e581. [Google Scholar] [CrossRef]
- Gawehn, E.; Hiss, J.A.; Brown, J.B.; Schneider, G. Advancing drug discovery via GPU-based deep learning. Expert Opinion on Drug Discovery. Expert Opin. Drug Discov. 2018, 13, 579–582. [Google Scholar] [CrossRef] [Green Version]
- ImageCLEF-The CLEF Cross Language Image Retrieval Track | ImageCLEF/LifeCLEF-Multimedia Retrieval in CLEF. 2003. Available online: https://www.imageclef.org/ (accessed on 3 July 2022).
- Alcantara, M.F.; Cao, Y.; Liu, C.; Liu, B.; Brunette, M.; Zhang, N.; Sun, T.; Zhang, P.; Chen, Q.; Li, Y.; et al. Improving Tuberculosis Diagnostics using Deep Learning and Mobile Health Technologies among Resource-poor Communities in Perú. Smart Health 2017, 1, 66–76. [Google Scholar] [CrossRef] [Green Version]
- Hartigan, M.A.; Wong, J.A. Algorithm AS 136: A k-Means Clustering Algorithm. J. R. Stat. Soc. C Appl. 2017, 28, 100–108. [Google Scholar] [CrossRef]








| S.No | Test | Principle | Detects | Drawbacks | Refs. |
|---|---|---|---|---|---|
| 1 | Chest X-ray | Imaging of inflammations in the lungs | Active tuberculosis |
| [22] |
| 2 | Conventional light microscopy | Light microscopy is used to visualize the Mycobacterium in the sputum smear | Active tuberculosis |
| [23] |
| 3 | Fluorescent LED microscopy | Fluorescence microscopy is used to visualize the Mycobacterium in the sputum sample | Active tuberculosis |
| [23,24] |
| 4 | Liquid culturing with drug susceptibility testing | Liquid media is used to culture Mycobacterium | Active tuberculosis and drug resistance |
| [25] |
| 5 | Lipoarabinomannan lateral flow assay | Detects antigen | Active tuberculosis in HIV-positive patients |
| [26] |
| 6 | Xpert MTB/RIF | Nucleic acid amplification test using quantitative PCR | Active tuberculosis and drug resistance mainly for rifampicin |
| [27] |
| 7 | Line probe assay for drug resistance to first-line anti-TB drugs (FL-LPA) | Nucleic acid amplification test using the line probe assay | Active tuberculosis and drug resistance to first-line anti-TB drugs |
| [28] |
| 8 | Line probe assay for drug resistance to second-line anti-TB drugs (SL-LPA) | Nucleic acid amplification test using the line probe assay | Active tuberculosis and drug resistance to second-line anti-TB drugs including injectable |
| [29] |
| 9 | Loopamp M. tuberculosis complex assay | Nucleic acid amplification test using loop-mediated isothermal amplification | Active tuberculosis |
| [30] |
| Sl.No | Name of the Tool | Design Stage | Advised Age Group | Process Time | Product Development Method | Refs. |
|---|---|---|---|---|---|---|
| Tools with CE-marked Certification * | ||||||
| 1. | CAD4TB (Delft Imaging, the Netherlands) | Available for sale | 4+ years | Less than 20 s |
| [126] |
| 2. | Infer Read DR Chest (InferVISION, Beijing, China) | Available for sale | 16+ years (approved), 12–18 years recommended | Less than 5 s |
| [127] |
| 3. | JLD02K (JVIEWER-X) (JLK, Seoul, South Korea) | Available for sale | 10+ years | 15–20 s |
| [128] |
| 4. | Lunit INSIGHT CXR (Lunit, Seoul, South Korea) | Available for sale | 14+ years | ≈20 s per on X-ray |
| [129] |
| 5. | qXR (Qure.ai, Mumbai, India) | Available for sale | 6+ years (approved), 2+ years recommended | Less than a minute |
| [130] |
| Tools with pending Certification | ||||||
| 1. | AXIR (Radisen, Seoul, South Korea) | Validation | 16+ years | Less than 20 s |
| [131] |
| 2. | T-Xnet (Artelus, Bangalore, India) | Validation | 18+ years | Max. 10 s |
| [132] |
| 3. | DxTB (DeepTek, Delaware, USA) | Available for sale | 14+ years | ≈2 s |
| [133] |
| 4. | Dr. CADx (Dr CADx, Bulawayo, Zimbabwe) | Validation | 16+ years | Less than a minute |
| [134] |
| 5. | XrayAME (Epcon, Antwerp, Belgium) | Available for sale | 18+ years | 20 s |
| [135] |
| 6. | JF CXR-1 (JF Healthcare, Nanchang, China) | Available for sale | 15+ years | ≈1–5 s |
| [136] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singh, M.; Pujar, G.V.; Kumar, S.A.; Bhagyalalitha, M.; Akshatha, H.S.; Abuhaija, B.; Alsoud, A.R.; Abualigah, L.; Beeraka, N.M.; Gandomi, A.H. Evolution of Machine Learning in Tuberculosis Diagnosis: A Review of Deep Learning-Based Medical Applications. Electronics 2022, 11, 2634. https://doi.org/10.3390/electronics11172634
Singh M, Pujar GV, Kumar SA, Bhagyalalitha M, Akshatha HS, Abuhaija B, Alsoud AR, Abualigah L, Beeraka NM, Gandomi AH. Evolution of Machine Learning in Tuberculosis Diagnosis: A Review of Deep Learning-Based Medical Applications. Electronics. 2022; 11(17):2634. https://doi.org/10.3390/electronics11172634
Chicago/Turabian StyleSingh, Manisha, Gurubasavaraj Veeranna Pujar, Sethu Arun Kumar, Meduri Bhagyalalitha, Handattu Shankaranarayana Akshatha, Belal Abuhaija, Anas Ratib Alsoud, Laith Abualigah, Narasimha M. Beeraka, and Amir H. Gandomi. 2022. "Evolution of Machine Learning in Tuberculosis Diagnosis: A Review of Deep Learning-Based Medical Applications" Electronics 11, no. 17: 2634. https://doi.org/10.3390/electronics11172634