
The Core of Medical Imaging: State of the Art and Perspectives on the Detectors

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Ultrasound Imaging
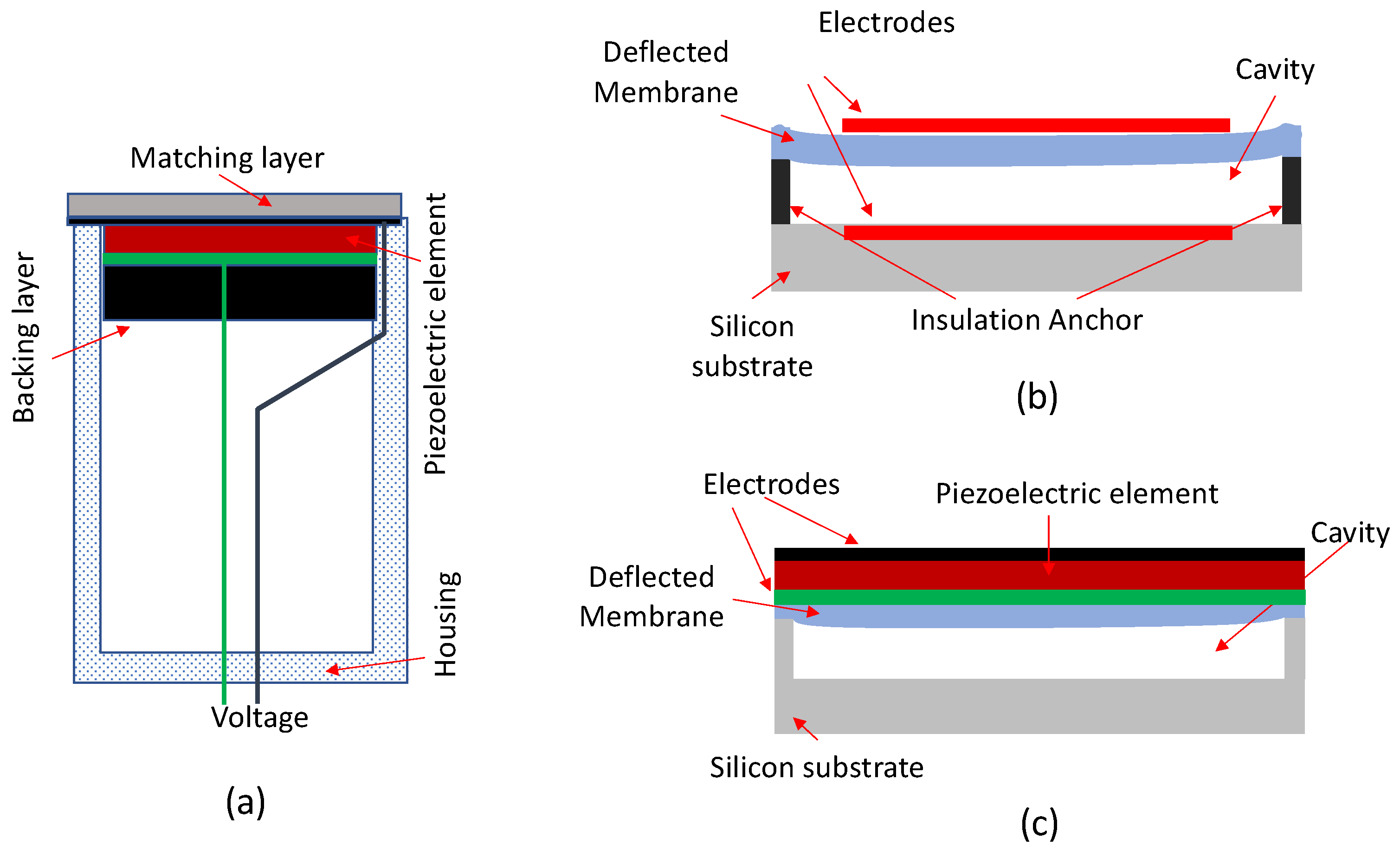
2.1. Piezoelectric Transducers Technology
2.2. Micromachined Ultrasonic Transducers
2.3. All-Optical Ultrasound Detection Technology
3. Optical and Thermal Imaging
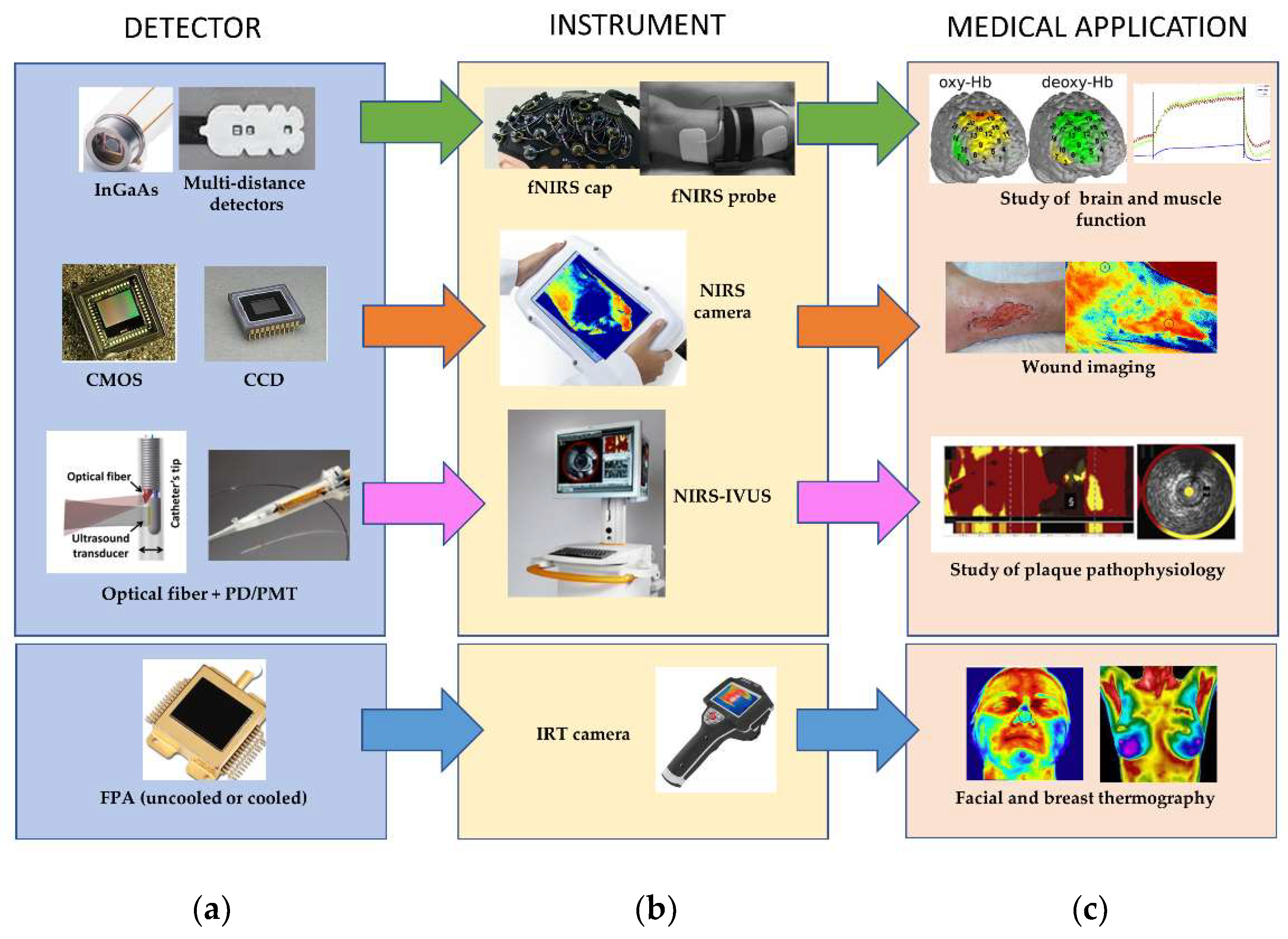
3.1. Near-Infrared Spectroscopy (NIRS)
3.1.1. Instruments
3.1.2. Image Sensors
3.1.3. Recent Technologies
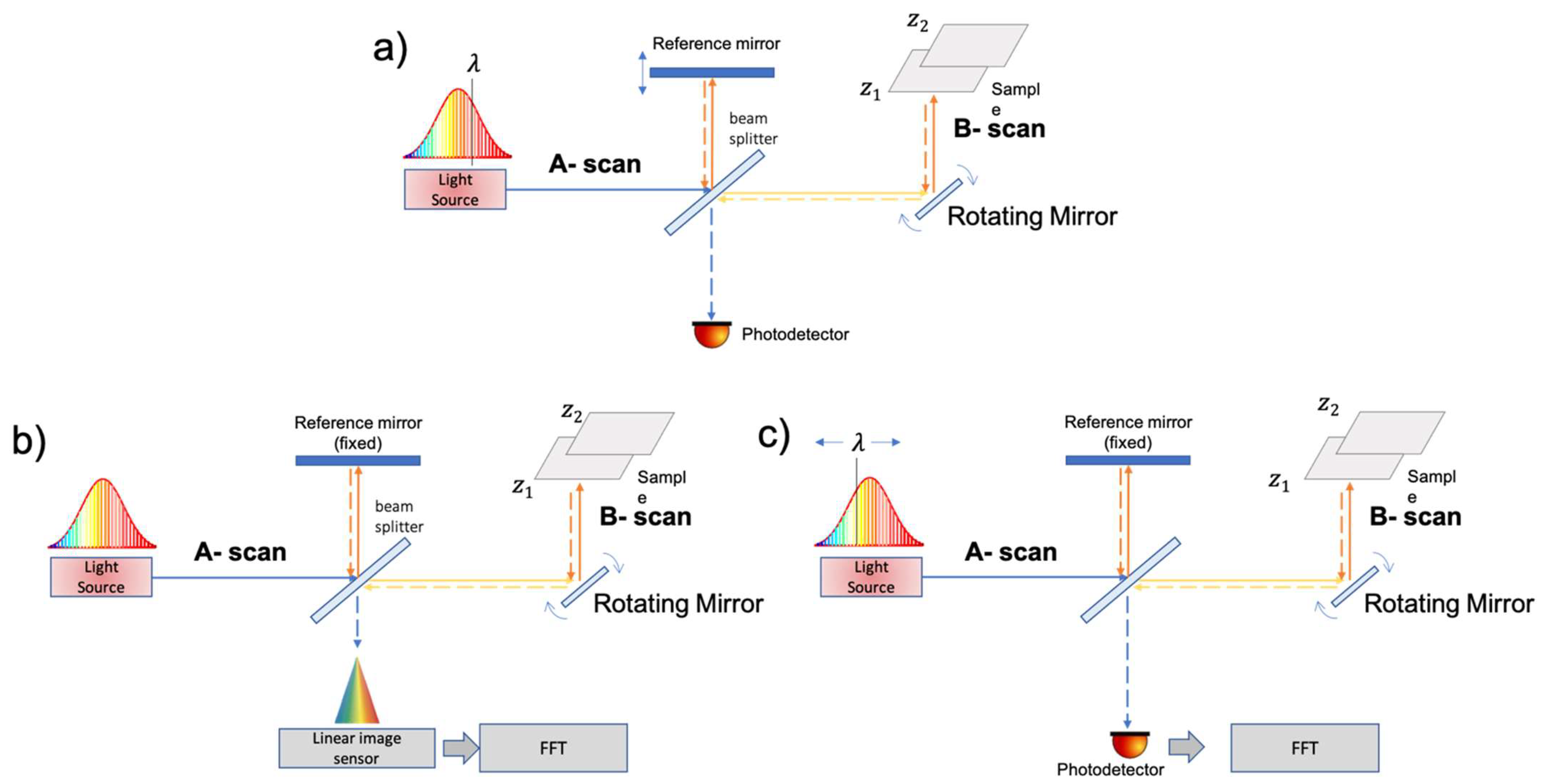
3.2. Optical Coherence Tomography (OCT)
3.3. Infrared Thermal (IRT)
3.3.1. Instruments
3.3.2. Image Sensors
4. Magnetic Resonance Imaging (MRI)
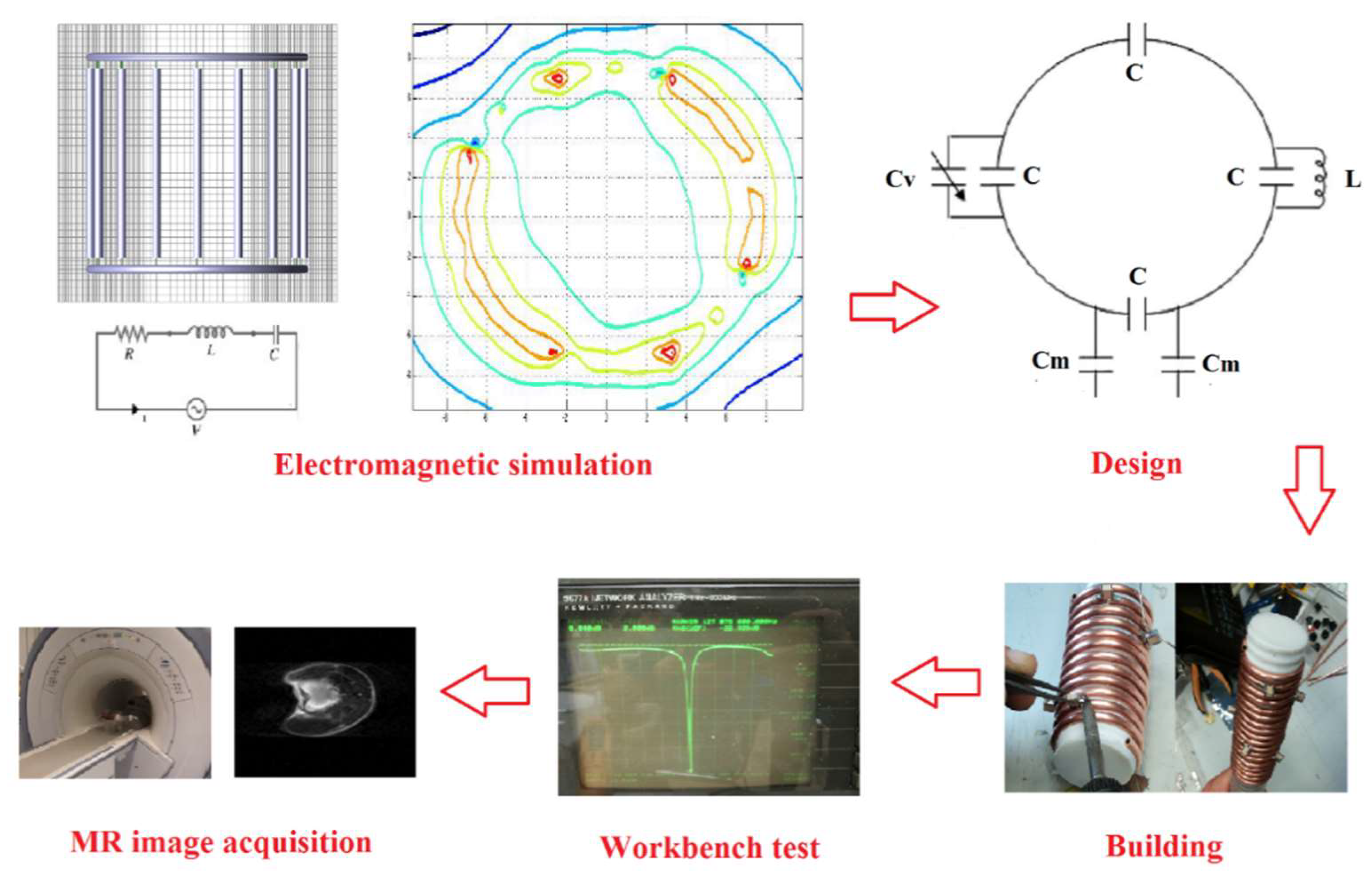
4.1. Radiofrequency (RF) Coils Design, Simulation, and Test
4.2. Recent Developments in RF Coil Technology
4.2.1. Phased Array Coils
4.2.2. Digital Coils
4.2.3. Catheter Coils
4.2.4. Reconfigurable Coils
4.2.5. Patient-Specific Coils
4.2.6. Metamaterials
5. Computed Tomography (CT)
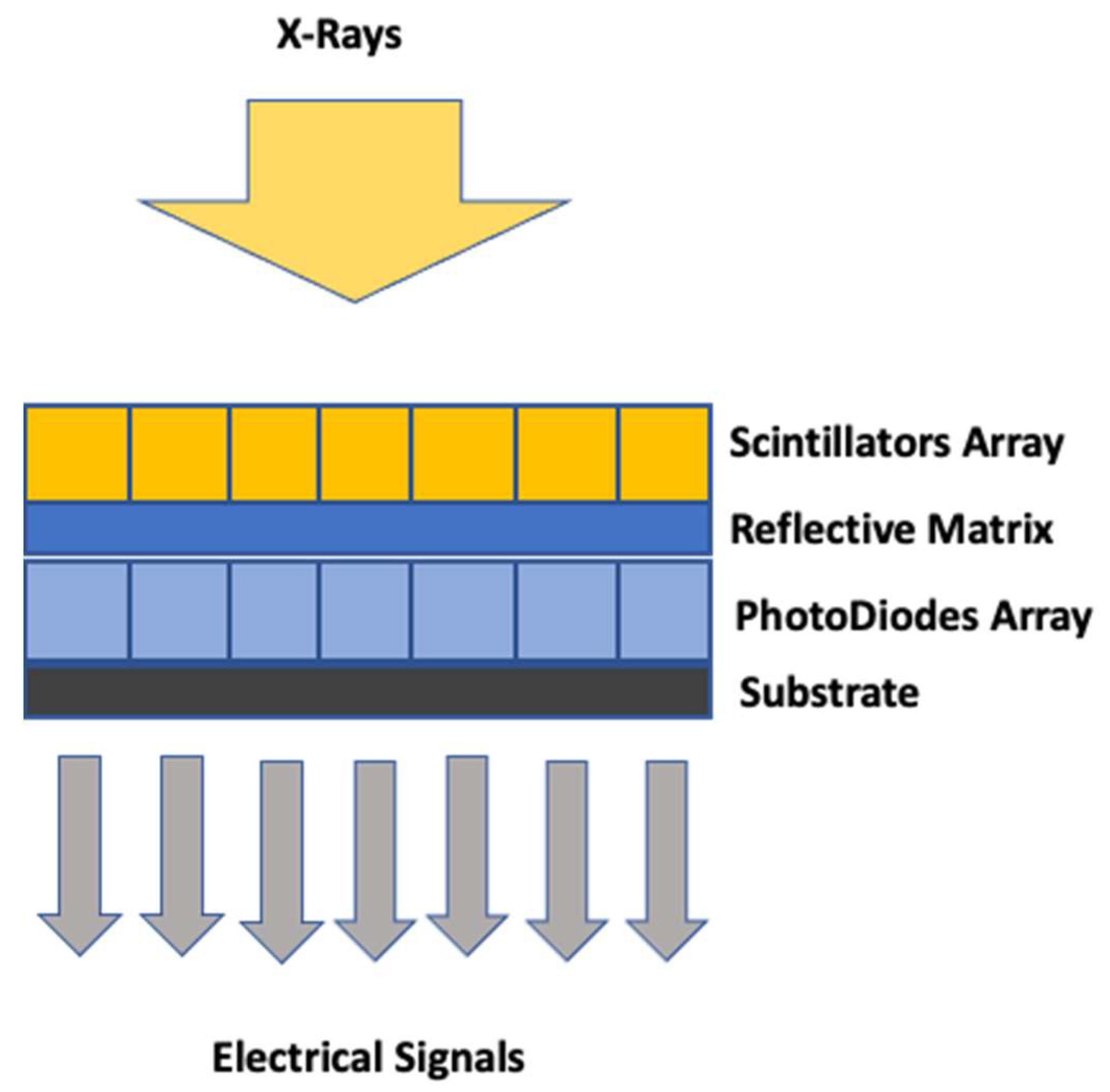
5.1. Indirect CT Detectors
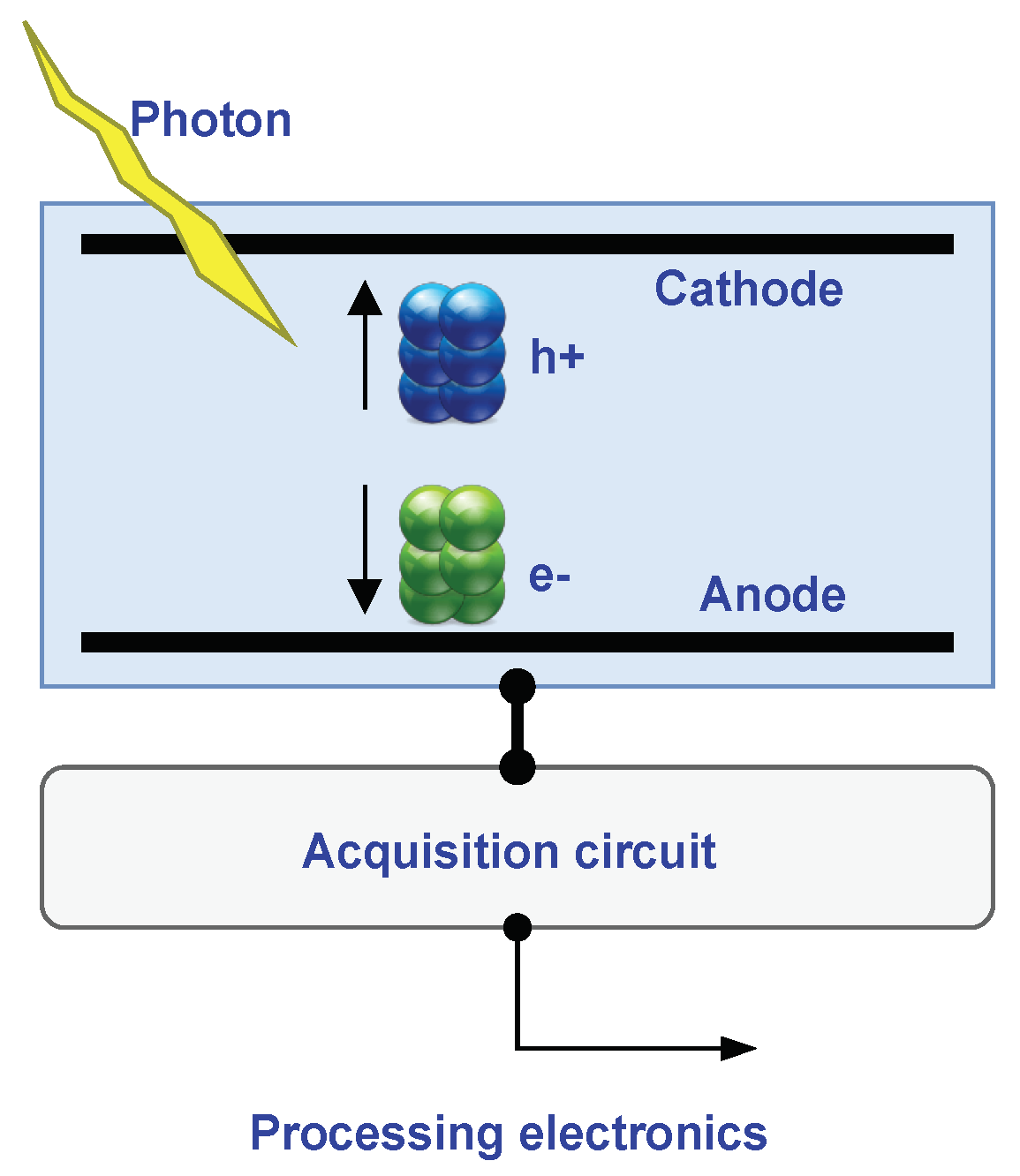
5.2. Direct CT Detectors
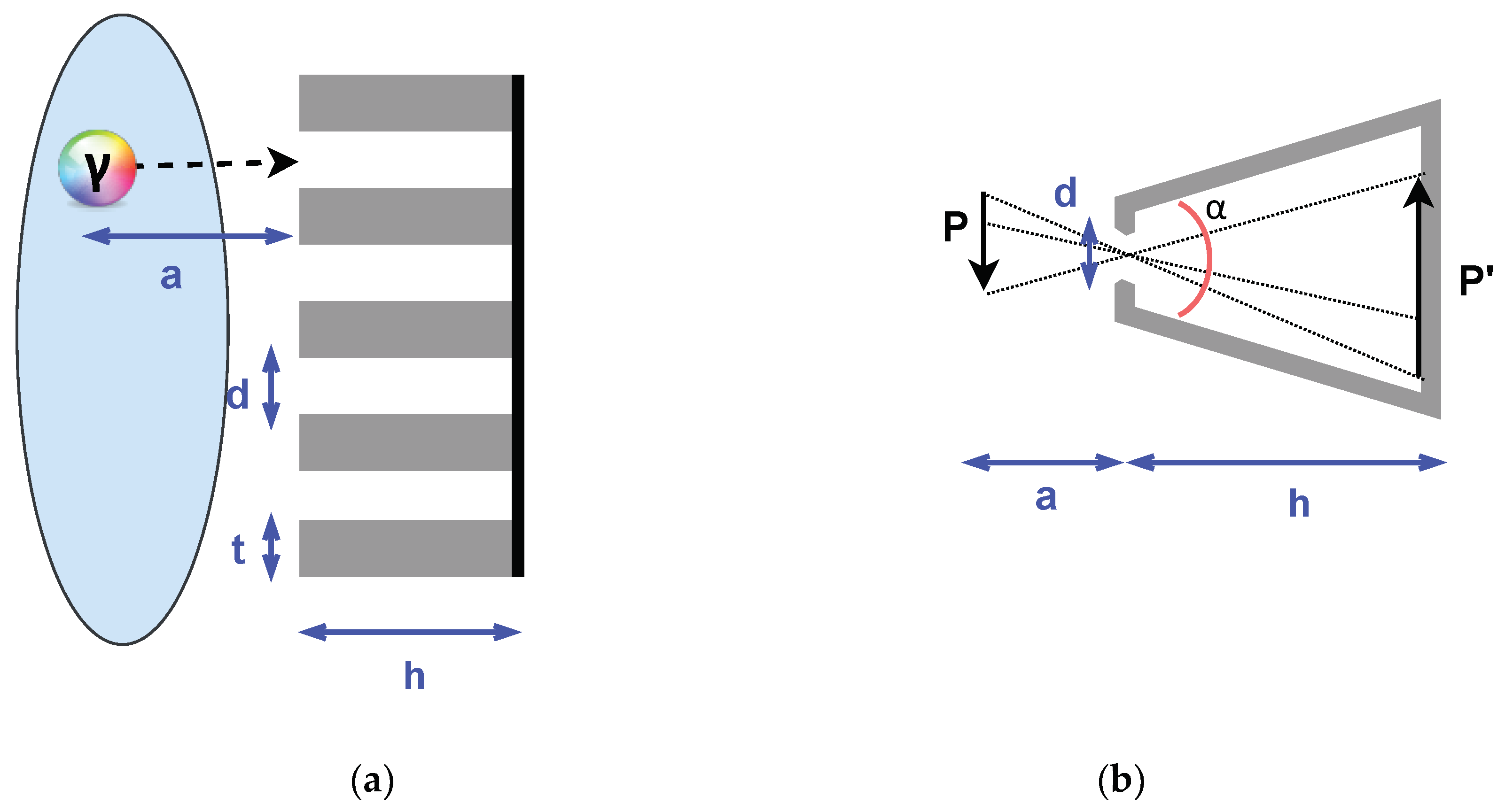
5.3. CT Collimators
6. Nuclear Medicine Imaging
6.1. New Generation Photon Detectors: CZT Technology
6.2. Single-Photon Emission Computed Tomography (SPECT)
6.2.1. CZT Detectors in SPECT
6.2.2. Collimators in SPECT
6.3. Positron Emission Tomography (PET) Imaging
PET Detectors
7. Discussion and Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Uchino, K. Piezoelectro composites. In Comprehensive Composite Materials II; Elsevier: Amsterdam, The Netherlands, 2017; pp. 613–624. [Google Scholar] [CrossRef]
- Harput, S.; Tortoli, P.; Eckersley, R.J.; Dunsby, C.; Tang, M.X.; Christensen-Jeffries, K.; Ramalli, A.; Brown, J.; Zhu, J.; Zhang, G.; et al. 3-D Super-Resolution Ultrasound Imaging with a 2-D Sparse Array. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2020, 67, 269–277. [Google Scholar] [CrossRef]
- Chen, Q.; Song, H.; Yu, J.; Kim, K. Current Development and Applications of Super-Resolution Ultrasound Imaging. Sensors 2021, 21, 2417. [Google Scholar] [CrossRef] [PubMed]
- Versluis, M.; Stride, E.; Lajoinie, G.; Dollet, B.; Segers, T. Ultrasound Contrast Agent Modeling: A Review. Ultrasound Med. Biol. 2020, 46, 2117–2144. [Google Scholar] [CrossRef]
- Sigrist, R.M.S.; Liau, J.; El Kaffas, A.; Chammas, M.C.; Willmann, J.K. Ultrasound elastography: Review of techniques and clinical applications. Theranostics 2017, 7, 1303–1329. [Google Scholar] [CrossRef] [PubMed]
- Marinozzi, F.; Bini, F.; Grandoni, A. Experimental Investigation of Inter-element Isolation in a Medical Array Transducer at Various Manufacturing Stages. Ultrason. Imaging 2017, 39, 62–74. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.J.; Wolf, P.D. 3-D Ultrasound Imaging Using Helicoid Array Transducers. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2021, 68, 697–706. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Gachagan, A.; Murray, P. Design of 2d sparse array transducers for anomaly detection in medical phantoms. Sensors 2020, 20, 5370. [Google Scholar] [CrossRef]
- Mozaffarzadeh, M.; Soozande, M.; Fool, F.; Pertijs, M.A.P.; Vos, H.J.; Verweij, M.D.; Bosch, J.G.; de Jong, N. Receive/transmit aperture selection for 3D ultrasound imaging with a 2D matrix transducer. Appl. Sci. 2020, 10, 5300. [Google Scholar] [CrossRef]
- Zubair, M.; Dickinson, R.J. 3D synthetic aperture imaging with a therapeutic spherical random phased array for transcostal applications. Phys. Med. Biol. 2021, 66, 035024. [Google Scholar] [CrossRef]
- Cabrera-Munoz, N.E.; Eliahoo, P.; Wodnicki, R.; Jung, H.; Chiu, C.T.; Williams, J.A.; Kim, H.H.; Zhou, Q.; Yang, G.Z.; Shung, K.K. Fabrication and characterization of a miniaturized 15-MHz side-looking phased-array transducer catheter. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2019, 66, 1079–1092. [Google Scholar] [CrossRef]
- Demi, L. Practical guide to ultrasound beam forming: Beam pattern and image reconstruction analysis. Appl. Sci. 2018, 8, 1544. [Google Scholar] [CrossRef] [Green Version]
- Luijten, B.; Cohen, R.; De Bruijn, F.J.; Schmeitz, H.A.W.; Mischi, M.; Eldar, Y.C.; Van Sloun, R.J.G. Adaptive Ultrasound Beamforming Using Deep Learning. IEEE Trans. Med. Imaging 2020, 39, 3967–3978. [Google Scholar] [CrossRef]
- Luchies, A.C.; Byram, B.C. Training improvements for ultrasound beamforming with deep neural networks. Phys. Med. Biol. 2019, 64. [Google Scholar] [CrossRef]
- Nazemi, H.; Antony Balasingam, J.; Swaminathan, S.; Ambrose, K.; Nathani, M.U.; Ahmadi, T.; Babu Lopez, Y.; Emadi, A. Mass Sensors Based on Capacitive and Piezoelectric Micromachined Ultrasonic Transducers—CMUT and PMUT. Sensors 2020, 20, 2010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dausch, D.E.; Castellucci, J.B.; Chou, D.R.; Von Ramm, O.T. Theory and operation of 2-D array piezoelectric micromachined ultrasound transducers. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2008, 55, 2484–2492. [Google Scholar] [CrossRef]
- Manwar, R.; Kratkiewicz, K.; Avanaki, K. Overview of ultrasound detection technologies for photoacoustic imaging. Micromachines 2020, 11, 692. [Google Scholar] [CrossRef]
- Wang, J.; Zheng, Z.; Chan, J.; Yeow, J.T.W. Capacitive micromachined ultrasound transducers for intravascular ultrasound imaging. Microsyst. Nanoeng. 2020, 6, 73. [Google Scholar] [CrossRef]
- Attia, A.B.E.; Balasundaram, G.; Moothanchery, M.; Dinish, U.S.; Bi, R.; Ntziachristos, V.; Olivo, M. A review of clinical photoacoustic imaging: Current and future trends. Photoacoustics 2019, 16, 100144. [Google Scholar] [CrossRef]
- Kratkiewicz, K.; Manwar, R.; Zhou, Y.; Mozaffarzadeh, M.; Avanaki, K. Technical considerations in the Verasonics research ultrasound platform for developing a photoacoustic imaging system. Biomed. Opt. Express 2021, 12, 1050. [Google Scholar] [CrossRef] [PubMed]
- Zhao, T.; Desjardins, A.E.; Ourselin, S.; Vercauteren, T.; Xia, W. Minimally invasive photoacoustic imaging: Current status and future perspectives. Photoacoustics 2019, 16, 100146. [Google Scholar] [CrossRef] [PubMed]
- Fang, C.; Hu, H.; Zou, J. A Focused Optically Transparent PVDF Transducer for Photoacoustic Microscopy. IEEE Sens. J. 2020, 20, 2313–2319. [Google Scholar] [CrossRef]
- Chen, R.; He, Y.; Shi, J.; Yung, C.; Hwang, J.; Wang, L.V.; Zhou, Q. Transparent High-Frequency Ultrasonic Transducer for Photoacoustic Microscopy Application. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2020, 67, 1848–1853. [Google Scholar] [CrossRef]
- Chen, S.; Guo, L.J.; Wang, X. Photoacoustics All-optical photoacoustic microscopy. Photoacoustics 2015, 3, 143–150. [Google Scholar] [CrossRef] [Green Version]
- Zhao, T.; Su, L.; Xia, W. Optical ultrasound generation and detection for intravascular imaging: A review. J. Healthc. Eng. 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Dong, B.; Sun, C.; Zhang, H.F. Optical Detection of Ultrasound in Photoacoustic Imaging. IEEE Trans. Biomed. Eng. 2017, 64, 4–15. [Google Scholar] [CrossRef]
- Finlay, M.C.; Mosse, C.A.; Colchester, R.J.; Noimark, S.; Zhang, E.Z.; Ourselin, S.; Beard, P.C.; Schillin, R.J.; Parkin, I.P.; Papakonstantinou, I.; et al. Through-needle all-optical ultrasound imaging in vivo: A preclinical swine study. Light Sci. Appl. 2017, 6, e17103-7. [Google Scholar] [CrossRef] [Green Version]
- Colchester, R.J.; Little, C.; Dwyer, G.; Noimark, S.; Alles, E.J.; Zhang, E.Z.; Loder, C.D.; Parkin, I.P.; Papakonstantinou, I.; Beard, P.C.; et al. All-Optical Rotational Ultrasound Imaging. Sci. Rep. 2019, 9, 5576. [Google Scholar] [CrossRef] [PubMed]
- Jöbsis, F.F. Noninvasive, infrared monitoring of cerebral and myocardial oxygen sufficiency and circulatory parameters. Science 1977, 198, 1264–1267. [Google Scholar] [CrossRef]
- Jue, T.; Masuda, K. Application of Near Infrared Spectroscopy in Biomedicine; Springer Science & Business Media: Berlin, Germany, 2013; ISBN 9781461462521. [Google Scholar]
- Vedantham, S.; Karellas, A. Emerging Breast Imaging Technologies on the Horizon. Semin. Ultrasound CT MRI 2018, 39, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Hartwig, V.; Marinelli, M.; Rocco, F.; L’Abbate, A. Assessment of microvascular function using near-infrared spectroscopic 2D imaging of whole hand combined with vascular occlusion test. J. Med. Biol. Eng. 2016, 36, 87–95. [Google Scholar] [CrossRef]
- Jalil, B.; Salvetti, O.; Potì, L.; Hartwig, V.; Marinelli, M.; L’Abbate, A. Near infrared image processing to quantitate and visualize oxygen saturation during vascular occlusion. Comput. Methods Programs Biomed. 2016, 126, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Gargani, L.; Bruni, C.; Barskova, T.; Hartwig, V.; Marinelli, M.; Trivella, M.G.; Matucci-Cerinic, M.; L’Abbate, A. Near-infrared spectroscopic imaging of the whole hand: A new tool to assess tissue perfusion and peripheral microcirculation in scleroderma. Semin. Arthritis Rheum. 2019, 48, 867–873. [Google Scholar] [CrossRef]
- Jalil, B.; Hartwig, V.; Salvetti, O.; Potì, L.; Gargani, L.; Barskova, T.; Matucci Cerinic, M.; L’Abbate, A. Assessment of hand superficial oxygenation during ischemia/reperfusion in healthy subjects versus systemic sclerosis patients by 2D near infrared spectroscopic imaging. Comput. Methods Programs Biomed. 2018, 155, 101–108. [Google Scholar] [CrossRef]
- Hartwig, V.; Marinelli, M.; Gargani, L.; Barskova, T.; Trivella, M.G.; Cerinic, M.M.; L’Abbate, A. Two-dimensional near infrared spectroscopic imaging of the hand to assess microvascular abnormalities in systemic sclerosis: A pilot study. J. Near Infrared Spectrosc. 2015, 23, 59–66. [Google Scholar] [CrossRef]
- Longobardi, P.; Hartwig, V.; Santarella, L.; Hoxha, K.; Campos, J.; Laurino, M.; Salvo, P.; Trivella, M.G.; Coceani, F.; Rocco, M.; et al. Potential markers of healing from near infrared spectroscopy imaging of venous leg ulcer. A randomized controlled clinical trial comparing conventional with hyperbaric oxygen treatment. Wound Repair Regen. 2020, 28, 856–866. [Google Scholar] [CrossRef]
- Hartwig, V.; Guiducci, L.; Marinelli, M.; Pistoia, L.; Tegrimi, T.M.; Iervasi, G.; Quinones-Galvan, A.; L’Abbate, A. Multimodal Imaging for the Detection of Brown Adipose Tissue Activation in Women: A Pilot Study Using NIRS and Infrared Thermography. J. Healthc. Eng. 2017, 2017. [Google Scholar] [CrossRef]
- Althobaiti, M.; Al-Naib, I. Recent developments in instrumentation of functional near-infrared spectroscopy systems. Appl. Sci. 2020, 10, 6522. [Google Scholar] [CrossRef]
- Ozaki, Y.; Huck, C.; Satoru, T.; Søren, B.E. Near-Infrared Spectroscopy Theory, Spectral Analysis, Instrumentation, and Applications; Springer: Berlin/Heidelberg, Germany, 2021; ISBN 978-981-15-8648-4. [Google Scholar]
- Feng, K.D.; Wang, Z.; Yang, Y. Development of medical imaging sensors. Int. J. Distrib. Sens. Netw. 2020, 16, 1550147720903607. [Google Scholar] [CrossRef]
- Fereyre, P.; Powell, G. CMOS Image Sensors Are Entering a New Age. Mater. Sci. 2016. Available online: https://www.siue.edu/~sumbaug/e2v_CMOS_Image_Sensors_are_entering_a_new_age_V4.pdf (accessed on 1 July 2021).
- Rogalski, A.; Kopytko, M.; Martyniuk, P. Infrared Detector Characterization. In Antimonide-Based Infrared Detect. A New Perspect. 2018. Available online: https://www.spiedigitallibrary.org/ebooks/PM/Antimonide-based-Infrared-Detectors-A-New-Perspective/1/Infrared-Detector-Characterization/10.1117/3.2278814.ch1 (accessed on 3 June 2021).
- Gondek History of infrared detectors A. Opto-Electron. Rev. 2010, 22, 77–85. [CrossRef]
- Bourantas, C.V.; Jaffer, F.A.; Gijsen, F.J.; Van Soest, G.; Madden, S.P.; Courtney, B.K.; Fard, A.M.; Tenekecioglu, E.; Zeng, Y.; Van Der Steen, A.F.W.; et al. Hybrid intravascular imaging: Recent advances, technical considerations, and current applications in the study of plaque pathophysiology. Eur. Heart J. 2017, 38, 400–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkinson, S.E.; Madder, R.D. Intracoronary near-infrared spectroscopy—role and clinical applications. Cardiovasc. Diagn. Ther. 2020, 10, 1508–1516. [Google Scholar] [CrossRef]
- Li, C.; Chen, G.; Zhang, Y.; Wu, F.; Wang, Q. Advanced fluorescence imaging technology in the near-infrared-II window for biomedical applications. J. Am. Chem. Soc. 2020, 142, 14789–14804. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Swanson, E.; Lin, C.; Schuman, J.; Stinson, W.; Chang, W.; Hee, M.; Flotte, T.; Gregory, K.; Puliafito, C.; et al. Optical coherence tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef] [Green Version]
- Tomlins, P.H.; Wang, R.K. Theory, developments and applications of optical coherence tomography. J. Phys. D. Appl. Phys. 2005, 38, 2519–2535. [Google Scholar] [CrossRef]
- Fujimoto, J.G.; Pitris, C.; Boppart, S.A.; Brezinski, M.E. Optical coherence tomography: An emerging technology for biomedical imaging and optical biopsy. Neoplasia 2000, 2, 9–25. [Google Scholar] [CrossRef] [Green Version]
- Maciel, M.J.; Rosa, C.C.; Wolffenbuttel, R.F.; Correia, J.H. Optical coherence tomography within a single microsystem. J. Phys. D. Appl. Phys. 2018, 51, 365401. [Google Scholar] [CrossRef]
- Hamdan, R.; Gonzalez, R.G.; Ghostine, S.; Caussin, C. Optical coherence tomography: From physical principles to clinical applications. Arch. Cardiovasc. Dis. 2012, 105, 529–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Boer, J.F.; Cense, B.; Park, B.H.; Pierce, M.C.; Tearney, G.J.; Bouma, B.E. Improved signal-to-noise ratio in spectral-domain compared with time-domain optical coherence tomography. Opt. Lett. 2003, 28, 2067. [Google Scholar] [CrossRef]
- Leitgeb, R.; Hitzenberger, C.; Fercher, A. Performance of fourier domain vs time domain optical coherence tomography. Opt. Express 2003, 11, 889. [Google Scholar] [CrossRef]
- Choma, M.; Sarunic, M.; Yang, C.; Izatt, J. Sensitivity advantage of swept source and Fourier domain optical coherence tomography. Opt. Express 2003, 11, 2183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, A.R.; Roisman, L.; Zhang, Q.; Zheng, F.; Rafael de Oliveira Dias, J.; Yehoshua, Z.; Schaal, K.B.; Feuer, W.; Gregori, G.; Chu, Z.; et al. Comparison between spectral-domain and swept-source optical coherence tomography angiographic imaging of choroidal neovascularization. Investig. Ophthalmol. Vis. Sci. 2017, 58, 1499–1505. [Google Scholar] [CrossRef] [PubMed]
- Etehadtavakol, M.; Ng, E.Y.K. Application of Infrared to Biomedical Sciences; Springer: Singapore, 2017; ISBN 978-981-10-3146-5. [Google Scholar]
- Jalil, B.; Hartwig, V.; Moroni, D.; Salvetti, O.; Benassi, A.; Jalil, Z.; Pistoia, L.; Minutoli Tegrimi, T.; Quinones-Galvan, A.; Iervasi, G.; et al. A Pilot Study of Infrared Thermography Based Assessment of Local Skin Temperature Response in Overweight and Lean Women during Oral Glucose Tolerance Test. J. Clin. Med. 2019, 8, 260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahiri, B.B.; Bagavathiappan, S.; Jayakumar, T.; Philip, J. Medical applications of infrared thermography: A review. Infrared Phys. Technol. 2012, 55, 221–235. [Google Scholar] [CrossRef] [PubMed]
- Cardone, D.; Merla, A. New frontiers for applications of thermal infrared imaging devices: Computational psychopshysiology in the neurosciences. Sensors 2017, 17, 1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, J. Electromagnetic Analysis and Design in Magnetic Resonance Imaging; CRC Press: Boca Raton, FL, USA, 1999; ISBN 9780849396939. [Google Scholar]
- Haase, A.; Odoj, F.; Von Kienlin, M.; Warnking, J.; Fidler, F.; Weisser, A.; Nittka, M.; Rommel, E.; Lanz, T.; Kalusche, B.; et al. NMR probeheads for in vivo applications. Concepts Magn. Reson. 2000, 12, 361–388. [Google Scholar] [CrossRef]
- Roemer, P.B.; Edelstein, W.A.; Hayes, C.E.; Souza, S.P.; Mueller, O.M. The NMR phased array. Magn. Reson. Med. 1990, 16, 192–225. [Google Scholar] [CrossRef]
- Giovannetti, G.; Viti, V.; Positano, V.; Santarelli, M.F.; Landini, L.; Benassi, A. Coil sensitivity map-based filter for phased-array image reconstruction in Magnetic Resonance Imaging. Int. J. Biomed. Eng. Technol. 2007, 1, 4–17. [Google Scholar] [CrossRef]
- Giovannetti, G.; Viti, V.; Positano, V.; Santarelli, M.F.; Landini, L.; Benassi, A. Magnetostatic simulation for accurate design of low field MRI phased-array coils. Concepts Magn. Reson. Part. B Magn. Reson. Eng. 2007, 31. [Google Scholar] [CrossRef]
- Giovannetti, G.; Hartwig, V.; Positano, V.; Vanello, N. Radiofrequency coils for magnetic resonance applications: Theory, design, and evaluation. Crit. Rev. Biomed. Eng. 2014, 42, 109–135. [Google Scholar] [CrossRef] [PubMed]
- Giovannetti, G.; Hartwig, V.; Viti, V.; Zadaricchio, P.; Meini, L.; Landini, L.; Benassi, A. Low Field Elliptical MR Coil Array Designed by FDTD. Concepts Magn. Reson. Part B Magn. Reson. Eng. Educ. J. 2008, 33, 32–38. [Google Scholar] [CrossRef]
- Giovannetti, G.; Fontana, N.; Monorchio, A.; Tosetti, M.; Tiberi, G. Estimation of losses in strip and circular wire conductors of radiofrequency planar surface coil by using the finite element method. Concepts Magn. Reson. Part. B Magn. Reson. Eng. 2017, 47, e21358. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Bottomley, P.A. Optimized quadrature surface coil designs. Magn. Reson. Mater. Phys. Biol. Med. 2008, 21, 41–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blamire, A.M. The technology of MRI—The next 10 years? Br. J. Radiol. 2008, 81, 601–617. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, M.; Potthast, A.; Sosnovik, D.E.; Polimeni, J.R.; Wiggins, G.C.; Triantafyllou, C.; Wald, L.L. A 128-channel receive-only cardiac coil for highly accelerated cardiac MRI at 3 tesla. Magn. Reson. Med. 2008, 59, 1431–1439. [Google Scholar] [CrossRef] [Green Version]
- Childs, A.S.; Malik, S.J.; O’Regan, D.P.; Hajnal, J.V. Impact of number of channels on RF shimming at 3T. Magn. Reson. Mater. Phys. Biol. Med. 2013, 26, 401–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jogiya, R.; Schuster, A.; Zaman, A.; Motwani, M.; Kouwenhoven, M.; Nagel, E.; Kozerke, S.; Plein, S. Three-dimensional balanced steady state free precession myocardial perfusion cardiovascular magnetic resonance at 3T using dual-source parallel RF transmission: Initial experience. J. Cardiovasc. Magn. Reson. 2014, 16, 90. [Google Scholar] [CrossRef] [Green Version]
- Winte, L.; Kellman, P.; Renz, W.; Gräl, A.; Hezel, F.; Thalhammer, C.; Von Knobelsdorff-Brenkenhoff, F.; Tkachenko, V.; Schulz-Menger, J.; Niendorf, T. Comparison of three multichannel transmit/receive radiofrequency coil configurations for anatomic and functional cardiac MRI at 7.0T: Implications for clinical imaging. Eur. Radiol. 2012, 22, 2211–2220. [Google Scholar] [CrossRef] [PubMed]
- Collick, B.D.; Behzadnezhad, B.; Hurley, S.A.; Mathew, N.K.; Behdad, N.; Lindsay, S.A.; Robb, F.; Stormont, R.S.; McMillan, A.B. Rapid development of application-specific flexible MRI receive coils. Phys. Med. Biol. 2020, 65, 19NT01. [Google Scholar] [CrossRef]
- Yeh, J.N.T.; Lin, J.F.L.; Li, Y.T.; Lin, F.H. A flexible and modular receiver coil array for magnetic resonance imaging. IEEE Trans. Med. Imaging 2019, 38, 824–833. [Google Scholar] [CrossRef]
- Gruber, B.; Froeling, M.; Leiner, T.; Klomp, D.W.J. RF coils: A practical guide for nonphysicists. J. Magn. Reson. Imaging 2018, 48, 590–604. [Google Scholar] [CrossRef]
- Serai, S.D.; Merrow, A.C.; Kline-Fath, B.M. Fetal MRI on a multi-element digital coil platform. Pediatr. Radiol. 2013, 43, 1213–1217. [Google Scholar] [CrossRef] [PubMed]
- Nohava, L.; Ginefri, J.C.; Willoquet, G.; Laistler, E.; Frass-Kriegl, R. Perspectives in Wireless Radio Frequency Coil Development for Magnetic Resonance Imaging. Front. Phys. 2020, 8, 11. [Google Scholar] [CrossRef]
- Homagk, A.K.; Umathum, R.; Korn, M.; Weber, M.A.; Hallscheidt, P.; Semmler, W.; Bock, M. An expandable catheter loop coil for intravascular MRI in larger blood vessels. Magn. Reson. Med. 2010, 63, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Serfaty, J.M.; Yang, X.; Aksit, P.; Quick, H.H.; Solaiyappan, M.; Atalar, E. Toward MRI-guided coronary catheterization: Visualization of guiding catheters, guidewires, and anatomy in real time. J. Magn. Reson. Imaging 2000, 12, 590–594. [Google Scholar] [CrossRef]
- Bernhardt, A.; Wilson, M.W.; Settecase, F.; Evans, L.; Malba, V.; Martin, A.J.; Saeed, M.; Roberts, T.P.L.; Arenson, R.L.; Hetts, S.W. Steerable Catheter Microcoils for Interventional MRI. Acad. Radiol. 2011, 18, 270–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulumulla, S.B.; Park, K.J.; Fiveland, E.; Iannotti, J.; Robb, F. MEMS switch integrated radio frequency coils and arrays for magnetic resonance imaging. Rev. Sci. Instrum. 2017, 88, 025003. [Google Scholar] [CrossRef]
- Zamarayeva, A.M.; Gopalan, K.; Corea, J.R.; Liu, M.Z.; Pang, K.; Lustig, M.; Arias, A.C. Custom, spray coated receive coils for magnetic resonance imaging. Sci. Rep. 2021, 11, 2635. [Google Scholar] [CrossRef]
- Duan, G.; Zhao, X.; Anderson, S.W.; Zhang, X. Boosting magnetic resonance imaging signal-to-noise ratio using magnetic metamaterials. Commun. Phys. 2019, 2, 35. [Google Scholar] [CrossRef]
- Qing, X.; Chen, Z.N.; Yeap, S.B.; Sun, M.; Goh, C.K.; Xinyi, T. MRI coils using metamaterials. In Proceedings of the 2015 IEEE International Symposium on Antennas and Propagation & USNC/URSI National Radio Science Meeting, Vancouver, BC, Canada, 19–25 July 2015; pp. 1348–1349. [Google Scholar]
- Hurshkainen, A.A.; Derzhavskaya, T.A.; Glybovski, S.B.; Voogt, I.J.; Melchakova, I.V.; Van Den Berg, C.A.T.; Raaijmakers, A.J.E. Element decoupling of 7 T dipole body arrays by EBG metasurface structures: Experimental verification. J. Magn. Reson. 2016, 269, 87–96. [Google Scholar] [CrossRef] [Green Version]
- Goldman, L.W. Principles of CT: Multislice CT. J. Nucl. Med. Technol. 2008, 36, 57–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shefer, E.; Altman, A.; Behling, R.; Goshen, R.; Gregorian, L.; Roterman, Y.; Uman, I.; Wainer, N.; Yagil, Y.; Zarchin, O. State of the Art of CT Detectors and Sources: A Literature Review. Curr. Radiol. Rep. 2013, 1, 76–91. [Google Scholar] [CrossRef]
- Tabari, A.; Lo Gullo, R.; Murugan, V.; Otrakji, A.; Digumarthy, S.; Kalra, M. Recent Advances in Computed Tomographic Technology. J. Thorac. Imaging 2017, 32, 89–100. [Google Scholar] [CrossRef]
- Yester, M.V.; Barnes, G.T. Geometrical Limitations Of Computed Tomography (CT) Scanner Resolution. In Application of Optical Instrumentation in Medicine VI; International Society for Optics and Photonics: Washington, DC, USA, 1977; Volume 127, pp. 296–303. [Google Scholar] [CrossRef]
- Jiang, H. Computed Tomography: Principles, Design, Artifacts, and Recent Advances; SPIE Press: Washington, DC, USA, 2009; Volume 114, ISBN 978-0-470-56353-3. [Google Scholar]
- Lecoq, P. Detectors in Medicine and Biology. In Particle Physics Reference Library; Fabjan, C., Schopper, H., Eds.; Springer: Cham, Switzerland, 2011. [Google Scholar] [CrossRef]
- Melcher, C.L. Perspectives on the future development of new scintillators. Nucl. Instrum. Methods Phys. Res. Sect. A Accel. Spectrometers Detect. Assoc. Equip. 2005, 537, 6–14. [Google Scholar] [CrossRef]
- Kanai, T.; Satoh, M.; Miura, I. Characteristics of a nonstoichiometric Gd3+δ(Al,Ga) 5-δO12:Ce garnet scintillator. J. Am. Ceram. Soc. 2008, 91, 456–462. [Google Scholar] [CrossRef]
- Jagtap, S.; Chopade, P.; Tadepalli, S.; Bhalerao, A.; Gosavi, S. A review on the progress of ZnSe as inorganic scintillator. Opto-Electron. Rev. 2019, 27, 90–103. [Google Scholar] [CrossRef]
- Lell, M.M.; Wildberger, J.E.; Alkadhi, H.; Damilakis, J.; Kachelriess, M. Evolution in computed tomography: The battle for speed and dose. Invest. Radiol. 2015, 50, 629–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danielsson, M.; Mats, P.; Sjolin, M. Photon-counting x-ray detectors for CT. Phys. Med. Biol. 2021, 66. [Google Scholar] [CrossRef] [PubMed]
- Flohr, T.; Petersilka, M.; Henning, A.; Ulzheimer, S.; Ferda, J.; Schmidt, B. Photon-counting CT review. Phys. Med. 2020, 79, 126–136. [Google Scholar] [CrossRef]
- Symons, R.; Cork, T.E.; Sahbaee, P.; Fuld, M.K.; Kappler, S.; Folio, L.R.; Bluemke, D.A.; Pourmorteza, A. Low-dose lung cancer screening with photon-counting CT: A feasibility study. Phys. Med. Biol. 2017, 62, 202–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tao, A.; Huang, R.; Tao, S.; Michalak, G.J.; McCollough, C.H.; Leng, S. Dual-source photon counting detector CT with a tin filter: A phantom study on iodine quantification performance. Phys. Med. Biol. 2019, 64, 115019. [Google Scholar] [CrossRef] [PubMed]
- Epple, F.M.; Ehn, S.; Thibault, P.; Koehler, T.; Potdevin, G.; Herzen, J.; Pennicard, D.; Graafsma, H.; Noël, P.B.; Pfeiffer, F. Phase unwrapping in spectral X-ray differential phase-contrast imaging with an energy-resolving photon-counting pixel detector. IEEE Trans. Med. Imaging 2015, 34, 816–823. [Google Scholar] [CrossRef] [PubMed]
- Engel, K.J.; Bäumer, C.; Wiegert, J.; Zeitler, G. Spectral analysis of scattered radiation in CT. In Medical Imaging 2008: Physics of Medical Imaging; International Society for Optics and Photonics: Washington, DC, USA, 2008; Volume 6913, p. 69131R. [Google Scholar] [CrossRef]
- Vogtmeier, G.; Dorscheid, R.; Engel, K.J.; Luhta, R.; Mattson, R.; Harwood, B.; Appleby, M.; Randolph, B.; Klinger, J. Two-dimensional anti-scatter grids for computed tomography detectors. In Medical Imaging 2008: Physics of Medical Imaging; International Society for Optics and Photonics: Washington, DC, USA, 2008; Volume 6913, p. 691359. [Google Scholar] [CrossRef]
- Del Sordo, S.; Abbene, L.; Caroli, E.; Mancini, A.M.; Zappettini, A.; Ubertini, P. Progress in the development of CdTe and CdZnTe semiconductor radiation detectors for astrophysical and medical applications. Sensors 2009, 9, 3491–3526. [Google Scholar] [CrossRef]
- Peterson, T.E.; Furenlid, L.R. SPECT detectors: The Anger Camera and beyond. Phys. Med. Biol. 2011, 56, R145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, W.; Chalich, Y.; Deen, M.J. Sensors for positron emission tomography applications. Sensors 2019, 19, 5019. [Google Scholar] [CrossRef] [Green Version]
- Iniewski, K. CZT detector technology for medical imaging. J. Instrum. 2014, 9, C11001. [Google Scholar] [CrossRef]
- Erlandsson, K.; Kacperski, K.; Van Gramberg, D.; Hutton, B.F. Performance evaluation of D-SPECT: A novel SPECT system for nuclear cardiology. Phys. Med. Biol. 2009, 54, 2635–2649. [Google Scholar] [CrossRef]
- Scheiber, C. CdTe and CdZnTe detectors in nuclear medicine. Nucl. Instrum. Methods Phys. Res. Sect. A Accel. Spectrometers Detect. Assoc. Equip. 2000, 448, 513–524. [Google Scholar] [CrossRef]
- Keidar, Z.; Raysberg, I.; Lugassi, R.; Frenkel, A.; Israel, O. Novel Cadmium Zinc Telluride Based detector General Purpose Gamma Camera: Initial Evaluation and Comparison with a Standard Camera. J. Nucl. Med. 2016, 57, 295. [Google Scholar]
- Takahashi, M.; Miyazaki, Y.; Kondo, A.; Ehara, T.; Kenji Koga, I.M. Performance Evaluation of the Discovery NM/CT 670 CZT. J. Nucl Med. 2019, 59, 1835. [Google Scholar]
- Gimelli, A.; Liga, R.; Bertasi, M.; Kusch, A.; Marzullo, P. Head-to-head comparison of a CZT-based all-purpose SPECT camera and a dedicated CZT cardiac device for myocardial perfusion and functional analysis. J. Nucl. Cardiol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Iniewski, K. CZT sensors for Computed Tomography: From crystal growth to image quality. J. Instrum. 2016, 11, C12034. [Google Scholar] [CrossRef]
- Cates, J.W.; Gu, Y.; Levin, C.S. Direct conversion semiconductor detectors in positron emission tomography. Mod. Phys. Lett. A 2015, 30, 1530011. [Google Scholar] [CrossRef]
- Akutagawa, W.; Zanio, K. Gamma Response of Semi-insulating Material. J. Appl. Phys. 1969, 40, 3838–3854. [Google Scholar] [CrossRef]
- Zheng, X.; Cheng, Z.; Deen, M.J.; Peng, H. Improving the spatial resolution in CZT detectors using charge sharing effect and transient signal analysis: Simulation study. Nucl. Instrum. Methods Phys. Res. Sect. A Accel. Spectrometers Detect. Assoc. Equip. 2016, 808, 60–70. [Google Scholar] [CrossRef]
- Niimi, T.; Nanasato, M.; Sugimoto, M.; Maeda, H. Evaluation of Cadmium-Zinc-Telluride Detector-based Single-Photon Emission Computed Tomography for Nuclear Cardiology: A Comparison with Conventional Anger Single-Photon Emission Computed Tomography. Nucl. Med. Mol. Imaging 2017, 51, 331–337. [Google Scholar] [CrossRef]
- Gambhir, S.S.; Berman, D.S.; Ziffer, J.; Nagler, M.; Sandler, M.; Patton, J.; Hutton, B.; Sharir, T.; Haim, S.B.; Haim, S.B. A novel high-sensitivity rapid-acquisition single-photon cardiac imaging camera. J. Nucl. Med. 2009, 50, 635–643. [Google Scholar] [CrossRef] [Green Version]
- Van Audenhaege, K.; Van Holen, R.; Vandenberghe, S.; Vanhove, C.; Metzler, S.D.; Moore, S.C. Review of SPECT collimator selection, optimization, and fabrication for clinical and preclinical imaging. Med. Phys. 2015, 42, 4796–4813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorenson, J.A.; Phelps, M.E. Physics in Nuclear Medicine, 2nd ed.; Elsevier Health Sciences: Amsterdam, The Netherlands, 1990. [Google Scholar]
- Dey, J. Improvement of performance of cardiac SPECT camera using curved detectors with pinholes. IEEE Trans. Nucl. Sci. 2012, 59, 334–347. [Google Scholar] [CrossRef] [PubMed]
- Funk, T.; Kirch, D.L.; Koss, J.E.; Botvinick, E.; Hasegawa, B.H. A novel approach to multipinhole SPECT for myocardial perfusion imaging. J. Nucl. Med. 2006, 47, 595–602. [Google Scholar]
- Gallamini, A.; Zwarthoed, C.; Borra, A. Positron emission tomography (PET) in oncology. Cancers 2014, 6, 1821–1889. [Google Scholar] [CrossRef] [Green Version]
- Herholz, K.; Heiss, W.D. Positron emission tomography in clinical neurology. Mol. Imaging Biol. 2004, 6, 239–269. [Google Scholar] [CrossRef] [PubMed]
- Politis, M.; Piccini, P. Positron emission tomography imaging in neurological disorders. J. Neurol. 2012, 259, 1769–1780. [Google Scholar] [CrossRef] [PubMed]
- Tarkin, J.M.; Ä †orović, A.; Wall, C.; Gopalan, D.; Rudd, J.H.F. Positron emission tomography imaging in cardiovascular disease. Heart 2020, 106, 1712–1718. [Google Scholar] [CrossRef]
- Santarelli, M.F.; Vanello, N.; Scipioni, M.; Valvano, G.; Landini, L. New Imaging Frontiers in Cardiology: Fast and Quantitative Maps from Raw Data. Curr. Pharm. Des. 2017, 23, 3268–3284. [Google Scholar] [CrossRef] [PubMed]
- Santarelli, M.F.; Scipioni, M.; Genovesi, D.; Giorgetti, A.; Marzullo, P.; Landini, L. Imaging Techniques As An Aid In The Early Detection Of Cardiac Amyloidosis. Curr. Pharm. Des. 2020, 26, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Cantone, M.C.; Hoeschen, C. Radiation Physics for Nuclear Medicine; Springer-Verlag: Berlin/Heidelberg, Germany, 2011. [Google Scholar]
- Defrise, M.; Kinahan, P.E.; Michel, C.J. Image Reconstruction Algorithms in PET. In Positron Emission Tomography: Basic Sciences; Bailey, D.L., Townsend, D.W., Valk, P.E., Maisey, M.N., Eds.; Springer: London, UK, 2005; pp. 63–91. ISBN 978-1-84628-007-8. [Google Scholar]
- Scipioni, M.; Santarelli, M.F.; Giorgetti, A.; Positano, V.; Landini, L. Negative binomial maximum likelihood expectation maximization (NB-MLEM) algorithm for reconstruction of pre-corrected PET data. Comput. Biol. Med. 2019, 115, 103481. [Google Scholar] [CrossRef]
- Scipioni, M.; Pedemonte, S.; Santarelli, M.F.; Landini, L. Probabilistic Graphical Models for Dynamic PET: A Novel Approach to Direct Parametric Map Estimation and Image Reconstruction. IEEE Trans. Med. Imaging 2020, 39, 152–160. [Google Scholar] [CrossRef]
- Scipioni, M.; Giorgetti, A.; Della Latta, D.; Fucci, S.; Positano, V.; Landini, L.; Santarelli, M.F. Direct Parametric Maps Estimation from Dynamic PET Data: An Iterated Conditional Modes Approach. J. Healthc. Eng. 2018, 5942873. [Google Scholar] [CrossRef]
- Xie, S.; Zhang, X.; Zhang, Y.; Ying, G.; Huang, Q.; Xu, J.; Peng, Q. Crystals Evaluation of Various Scintillator Materials in Radiation Detector Design for Positron Emission Tomography (PET). Crystals 2020, 10, 869. [Google Scholar] [CrossRef]
- Spanoudaki, V.C.; Levin, C.S. Photo-detectors for time of flight positron emission tomography (ToF-PET). Sensors 2010, 10, 10484–10505. [Google Scholar] [CrossRef]
- Nassalski, A.; Kapusta, M.; Batsch, T.; Wolski, D.; Möckel, D.; Enghardt, W.; Moszyński, M. Comparative study of scintillators for PET/CT detectors. IEEE Trans. Nucl. Sci. 2007, 54, 3–10. [Google Scholar] [CrossRef]
- Lewellen, T.K. Recent developments in PET detector technology Positron emission tomography—Some of the basics. Phys. Med. Biol 2010, 53, 1–46. [Google Scholar] [CrossRef]
- Hayashi, T. Haiashi_PMT_IEEET1989.pdf. IEEE Trans. Nucl. Sci. 1989, 36, 1078–1083. [Google Scholar] [CrossRef]
- Cadorette, G.; Rodrigue, S.; Lecomte, R. Tuning of Avalanche Photodiode PET Camera. IEEE Trans. Med. Imaging 1993, 36, 1078–1083. [Google Scholar] [CrossRef]
- Otte, N.; Dolgoshein, B.; Hose, J.; Klemin, S.; Lorenz, E.; Mirzoyan, R.; Popova, E.; Teshima, M. The SiPM—A new photon detector for PET. Nucl. Phys. B Proc. Suppl. 2006, 150, 417–420. [Google Scholar] [CrossRef]
- Gu, Y.; Matteson, J.L.; Skelton, R.T.; Deal, A.C.; Stephan, E.A.; Duttweiler, F.; Gasaway, T.M.; Levin, C.S. Study of a high-resolution, 3-D positioning cadmium zinc telluride detector for PET. Phys. Med. Biol. 2011, 56, 1563–1584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, Y.; Levin, C.S. Study of electrode pattern design for a CZT-based PET detector. Phys. Med. Biol. 2014, 59, 2599–2621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drezet, A.; Monnet, O.; Montémont, G.; Rustique, J.; Sanchez, G.; Verger, L. CdZnTe detectors for the positron emission tomographic imaging of small animals. In Proceedings of the IEEE Symposium Conference Record Nuclear Science 2004, Rome, Italy, 16–22 October 2004; Volume 7, pp. 4564–4568. [Google Scholar] [CrossRef]
- Brown, B.H. Electrical impedance tomography (EIT): A review. J. Med. Eng. Technol. 2003, 27, 97–108. [Google Scholar] [CrossRef] [PubMed]
- Leitzke, J.P.; Zangl, H. A review on electrical impedance tomography spectroscopy. Sensors 2020, 20, 5160. [Google Scholar] [CrossRef]
- Aldhaeebi, M.A.; Alzoubi, K.; Almoneef, T.S.; Bamatra, S.M.; Attia, H.; Ramahi, O.M. Review of microwaves techniques for breast cancer detection. Sensors 2020, 20, 2390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pisa, S.; Pittella, E.; Piuzzi, E. A survey of radar systems for medical applications. IEEE Aerosp. Electron. Syst. Mag. 2016, 31, 64–81. [Google Scholar] [CrossRef]
- Mostov, K.; Liptsen, E.; Boutchko, R. Medical applications of shortwave FM radar: Remote monitoring of cardiac and respiratory motion. Med. Phys. 2010, 37, 1332–1338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fenici, R.; Brisinda, D.; Meloni, A.M. Clinical application of magnetocardiography. Expert Rev. Mol. Diagn. 2005, 5, 291–313. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Imaging Methodology | Source | Energy, Frequency or Wavelength | Advanced Detectors | Detector’s Geometry | Spatial Resolution | Penetration Depth | Typical Field of View Size | Type of Diagnosis | Advantages | Limits |
|---|---|---|---|---|---|---|---|---|---|---|
| Ultrasound | Acoustic waves | 2.25–15 MHz; (1) 30–50 MHz | Piezoelectric; Micromachined (pMUTs; cMUTs); All-Optical | linear or sector array | (2) Axial: 500 μm; (3) Lateral: 1 mm | (4) 1–20 cm; (1) 2–3 mm | 10–15 cm | Whole body, hearth, abdominal organs | High spatial and temporal resolution, low cost, high dynamic range, non-ionizing | Operator-dependent images |
| NIRS | Non-ionizing EM waves | 700–1000 nm | InGaAs, CCD, CMOS | 2D array | about 1 cm | up to few cm | 1–20 cm | Peripheral muscle, blood vessels, brain, connective tissues, heart (exposed), breast, arms and legs | temporal sensitivity, low cost, portability, robustness to motion artifacts, noninvasive, non-ionizing | Poor spatial resolution |
| OCT | Non-ionizing EM waves | 1.3 μm | Photodiode Array | 1D array | 10–20 μm (Axial)/20–40 μm (Lateral) | 1–2.5 mm | 1 cm | Intravascular cardiology (coronary vessel, carotid) ophthalmology and dental (non invasive modality) | High spatial and temporal resolution, non-ionizing | Invasive (intravascular cardiology and gastrointestinal) |
| IRT | Non-ionizing EM waves | 8–12 μm | FPA, InGaAs, HgCdTe, layered GaAs/AlGaAs, QWIP, Vox microbolometer | 2D array | 2 mm | superficial | 20–50 cm | neurology, vascular disorders, rheumatic diseases, tissue viability, oncology, dermatological disorders, neonatal, ophthalmology, surgery, microvascular imaging, detection of BAT activation | Portability, compactnes, non-ionizing, noninvasive, dynamic measurements, low cost | Poor spatial resolution, cooling requirement |
| MRI | Non-ionizing EM waves | 20–300 MHz | RF surface, volume and phased-array coils | single element or array in planar or volumetric arrangement | 0.5 mm | 40 cm | 12–50 cm | Brain, heart, abdominal organs, arms and legs | Non-invasive, non-ionizing, good spatial and temporal resolution | High cost |
| CT | Ionizing EM waves | 70–150 keV | CdWO4, Gd2O2S:Pr, Ce(Y,Gd)2O3:Eu, GEGemstoneTM, ZnSe:Te (5) CdTe/CZT (6) | cylinder array arrangement | 0.5 mm | >100 cm | 50–65 cm | Almost all anatomical districts | High spatial resolution, short acquisition time | ionizing technique, use of contrast in most cases |
| SPECT | Ionizing EM waves | 100–300 KeV | collimator—scintillator—photodetector arrangement -CZT crystals | sets of 2D array | 2 mm | >40 cm | 15–40 cm | Whole body, Brain, hearth, abdominal organs | Non-invasive, functional imaging, molecular imaging | ionizing technique, medium-high costs |
| PET | Ionizing EM waves | 511 KeV | collimator—scintillator—photodetector arrangement | one or more cylinders array arrangement | 4 mm | >40 cm | 15–40 cm | Whole body, Brain, hearth, abdominal organs | Non-invasive, molecular imaging allowed, gives metabolic information, absolute quantitative information. | ionizing technique, high costs |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santarelli, M.F.; Giovannetti, G.; Hartwig, V.; Celi, S.; Positano, V.; Landini, L. The Core of Medical Imaging: State of the Art and Perspectives on the Detectors. Electronics 2021, 10, 1642. https://doi.org/10.3390/electronics10141642
Santarelli MF, Giovannetti G, Hartwig V, Celi S, Positano V, Landini L. The Core of Medical Imaging: State of the Art and Perspectives on the Detectors. Electronics. 2021; 10(14):1642. https://doi.org/10.3390/electronics10141642
Chicago/Turabian StyleSantarelli, Maria Filomena, Giulio Giovannetti, Valentina Hartwig, Simona Celi, Vincenzo Positano, and Luigi Landini. 2021. "The Core of Medical Imaging: State of the Art and Perspectives on the Detectors" Electronics 10, no. 14: 1642. https://doi.org/10.3390/electronics10141642