SARS-CoV-2 Positive Hospitalized Cancer Patients during the Italian Outbreak: The Cohort Study in Reggio Emilia

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Definitions
2.3. Imaging Evaluation
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.C.; Chen, C.S.; Chan, Y.J. The outbreak of COVID-19: An overview. J. Chin. Med. Assoc. 2020, 83, 217–220. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Cowling, B.J.; Leung, G.M. Epidemiological research priorities for public health control of the ongoing global novel coronavirus (2019-nCoV) outbreak. Eurosurveillance 2020, 25, 2000110. [Google Scholar] [CrossRef] [PubMed]
- McCloskey, B.; Heymann, D.L. SARS to novel coronavirus—Old lessons and new lessons. Epidemiol. Infect. 2020, 148, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Remuzzi, A.; Remuzzi, G. COVID-19 and Italy: What next? Lancet 2020, 395, 1225–1228. [Google Scholar] [CrossRef]
- Holshue, M.L.; DeBolt, C.; Lindquist, S.; Lofy, K.H.; Wiesman, J.; Bruce, H.; Spiters, C.; Ericson, K.; Wilkerson, S.; Weldon, W.C.; et al. First Case of 2019 Novel Coronavirus in the United States. N. Engl. J. Med. 2020, 382, 929–936. [Google Scholar] [CrossRef]
- World Health Organization. Rolling Updates on Coronavirus Disease (COVID-19). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 30 March 2020).
- Italian Ministry of Health. Novel Coronavirus and COVID-19. Italy Situation. Available online: http://www.salute.gov.it/portale/nuovocoronavirus/dettaglioNotizieNuovoCoronavirus.jsp?lingua=italiano&menu=notizie&p=dalministero&id=4454 (accessed on 12 April 2020).
- Kamboj, M.; Sepkowitz, K.A. Nosocomial infections in patients with cancer. Lancet Oncol. 2009, 10, 589–597. [Google Scholar] [CrossRef]
- Bitterman, R.; Eliakim-Raz, N.; Vinograd, I.; Zalmanovici, T.A.; Leibovici, L.; Paul, M. Influenza vaccines in immunosuppressed adults with cancer. Cochrane Database Syst. Rev. 2018, 2, CD00898. [Google Scholar] [CrossRef]
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-Cov-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef]
- Yu, J.; Ouyang, W.; Chua, M.L.K.; Xie, C. SARS-CoV-2 Transmission in Patients with Cancer at a Tertiary Care Hospital in Wuhan, China. JAMA Oncol. 2020, 6, 1108–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Zhu, F.; Xie, L.; Wang, C.; Wang, J.; Chen, R.; Jia, P.; Guan, H.Q.; Peng, L.; Chen, Y.; et al. Clinical characteristics of COVID-19-infected cancer patients: A retrospective case study in three hospitals within Wuhan, China. Ann. Oncol. 2020, 31, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. The epidemiological characteristics of an outbreak of 2019 novel coronavirus disease (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi/Chin. J. Epidem. 2020, 41, 145–151. [Google Scholar]
- World Health Organization—China Joint Mission. Report on Coronavirus Disease. Available online: https://who.int/docs/default-source/coranaviruse/who-china-joint-mission-on-covid-19-final-report.pdf (accessed on 12 March 2020).
- Dai, M.; Liu, D.; Liu, M.; Zhou, F.; Li, G.; Chen, Z.; Zhang, Z.; You, H.; Wu, M.; Zheng, Q.; et al. Patients with cancer appear more vulnerable to SARS-CoV-2: A multi-center study during the COVID-19 outbreak. Cancer Discov. 2020, 10, 783–791. [Google Scholar]
- Mehta, V.; Goel, S.; Kabarttiti, R.; Cole, D.; Goldfinger, M.; Acuna-Villaorduna, A.; Pradhan, K.; Thota, R.; Reissman, S.; Sparano, J.A.; et al. Case fatality rate of cancer patients with COVID-19 in a New York Hospital system. Cancer Discov. 2020, 10, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Rizvi, H.; Egger, V.; Preeshagull, I.R.; Wolchok, J.D.; Hellmann, M.D. Impact of PD-1 blockade on severity of COVID-19 in patients with lung cancers. Cancer Discov. 2020. [Google Scholar] [CrossRef]
- Ueda, M.; Martinis, R.; Hendrie, P.C.; McDonnell, T.; Crews, J.R.; Wong, T.L.; McCreery, T.; Jagels, B.; Crane, A.; Byrd, D.R.; et al. Managing Cancer Care During the COVID-19 Pandemic: Agility and Collaboration Toward a Common Goal. J. Natl. Compr. Cancer Netw. 2020, 1, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Al-Shamsi, H.O.; Alhazzani, W.; Alhuraiji, A.; Coomes, E.A.; Chemaly, R.F.; Almuhanna, M.; Wolff, R.A.; Ibrahim, N.K.; Chua, M.L.K.; Hotte, S.J.; et al. A Practical Approach to the Management of Cancer Patients During the Novel Coronavirus Disease 2019 (COVID-19) Pandemic: An International Collaborative Group. Oncologist 2020, 25, 936–945. [Google Scholar] [CrossRef] [Green Version]
- Kutikov, A.; Weinberg, D.S.; Edelman, M.J.; Horwitz, E.M.; Uzzo, R.G.; Fisher, R.I. A war on two fronts: Cancer care in the time of COVID-19. Ann. Int. Med. 2020, 172, 756–758. [Google Scholar] [CrossRef] [Green Version]
- Pinto, C.; Cagnazzo, C. Indications regarding the management of interventional clinical trials with drugs during the current COVID-19 (Coronavirus Disease-19) emergency in Italy. ESMO Open 2020. [Google Scholar] [CrossRef]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection When Novel Coronavirus (nCov) Infection is Suspected. Interim Guidance. Available online: https://www.who.int/publications/i/item/clinical-management-of-covid-19 (accessed on 27 March 2020).
- Colombi, D.; Bodini, F.C.; Petrini, M.; Maffi, G.; Morelli, N.; Milanese, G.; Silva, M.; Sverzellati, N.; Michieletti, E. Well-aerated lung on admitting chest CT to predict adverse outcome in COVID-19 pneumonia. Radiology 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guzzinati, S.; Virdone, S.; De Angelis, R.; Panato, C.; Gatta, G.; Trama, A.; Rugge, M.; Tagliabue, G.; Casella, C.; Caruso, B.; et al. Characteristics of people living in Italy after a cancer diagnosis in 2010 and projections to 2020. BMC Cancer 2018, 18, 169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giorgi Rossi, P.; Marino, M.; Formisano, D.; Venturelli, F.; Vicentini, M.; Grilli, R. Characteristics and outcomes of a cohort of SARS-CoV-2 patients in the Province of Reggio Emilia, Italy. medRxiv 2020. [Google Scholar] [CrossRef]
- McMichael, T.M.; Currie, D.W.; Clark, S.; Pogosjans, S.; Kay, M.; Shwartz, M.G.; Lewis, J.; Baer, A.; Kawakami, V.; Lukoff, M.D.; et al. Epidemiology of Covid-19 in a Long-Term Care Facility in King County, Washington. N. Engl. J. Med. 2020, 382, 2005–2011. [Google Scholar] [CrossRef]
- Goyal, P.; Choi, J.J.; Pinheiro, L.C.; Schenck, E.J.; Chen, R.; Satlin, M.J.; Campion, T.R.; Nahid, M.; Ringel, J.B.; Hoffman, K.L.; et al. Clinical Characteristics of Covid-19 in New York City. N. Engl. J. Med. 2020, 382, 2372–2374. [Google Scholar] [CrossRef]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [CrossRef]
- Zheng, R.S.; Sun, K.X.; Zhang, S.V.; Zeng, H.M.; Zou, X.N.; Chen, R.; Gu, X.Y.; Wei, W.W.; He, J. Report of cancer epidemiology in China, 2015. Chin. J. Oncol. 2019, 41, 19–28. [Google Scholar]
- Italian Tumor Registry. Available online: https://www.registri-tumori.it/cms/pagine/i-numeri-del-cancro (accessed on 2 March 2020).
- Shapiro, C.L. Cancer survivorship. N. Engl. J. Med. 2018, 379, 2438–2450. [Google Scholar] [CrossRef]
- Cummings, M.J.; Baldwin, M.R.; Abrams, D.; Jacobson, S.D.; Meyer, B.J.; Balough, E.M.; Aaron, J.G.; Classen, J.; Rabbani, L.E.; Hastie, J.; et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City. A prospective cohort study. Lancet 2020, 395, 1763–1770. [Google Scholar] [CrossRef]
- Tumor Registry of Reggio Emilia. Available online: https://www.ausl.re.it/sites/default/files/Pubblicazione_Tumori_Area_Vasta_Emilia_Nord.pdf (accessed on 8 March 2020).
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersali, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Bersanelli, M. Controversies about COVID-19 and anticancer treatment with immune checkpoint inhibitors. Immunotherapy 2020, 12, 269–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damato, A.; Spallanzani, A.; Berselli, A.; Rovesti, G.; Bennatti, S.; Luppi, G.; Pinto, C. Impact of PD-1/PD-L1 blockade therapy in COVID-19 infected cancer patients hospitalization. Results of an Italian Study in the Province of Modena and Reggio Emilia during SARS-CoV-2 outbreak. Proc. ESMO 2020. Abstract, submitted. [Google Scholar]
- Calabrò, L.; Peters, S.; Soria, J.C.; Di Giacomo, A.M.; Barlesi, F.; Covre, A.; Altomonte, M.; Vegni, V.; Gridelli, C.; Reck, M. Challenges in lung cancer therapy during the COVID-19 pandemic. Lancet Respir. Med. 2020, 8, 542–544. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hiu, D.S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Garassino, M.C.; Whisenant, J.G.; Huang, L.C.; Trama, A.; Torri, V.; Agustoni, F.; Baena, J.; Banna, G.; Berardi, R.; Bettini, A.C.; et al. COVID-19 in patients with thoracic malignancies (TERAVOLT): First results of an international, registry-based, cohort study. Lancet Oncol. 2020. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Total Patients (No. 1226) | Cancer Patients (No. 138) | Non-Cancer Patients (No. 1088) | Adj OR |
|---|---|---|---|---|
| Sex, No. (%) | ||||
| Female | 493 (40.2%) | 52 (37.7%) | 441 (40.5%) | |
| Male | 733 (59.8%) | 86 (62.3%) | 647 (59.5%) | |
| Mean age, years (SD) | 71.7 (14.5) | 76.8 (10.4) | 71.0 (14.8) | |
| Median age, years (range) | 73 (23–100) | 76 (45–98) | 73 (23–100) | |
| ICU hospitalized, No. (%) | 92 (7.5%) | 14 (10.1%) | 73 (6.7%) | 1.23, 95% CI 0.63–2.41 |
| Deaths, No. (%) | 330 (26.9%) | 47 (34.1%) | 283 (26.0%) | 1.07, 95% CI 0.71–1.61 |
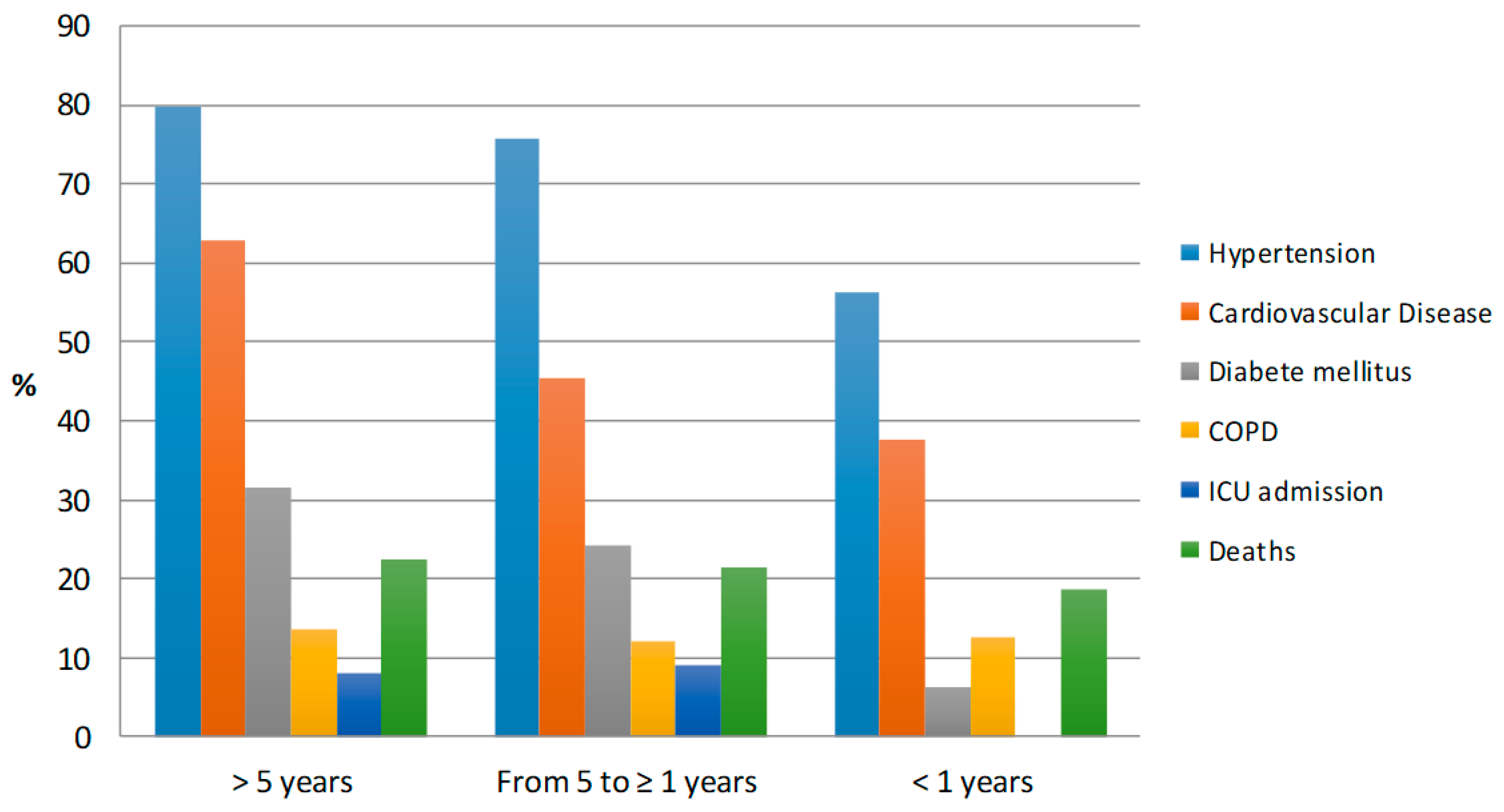
| >5 Years | From 5 to ≥1 Years | <1 Year | |
|---|---|---|---|
| Patients, No. (%) | 89 (64.5%) | 33 (23.9%) | 16 (11.6%) |
| Gender, No. (%) | |||
| Female | 39 (43.8%) | 11 (33.3%) | 3 (18.8%) |
| Male | 50 (56.2%) | 22 (66.7%) | 13 (81.3%) |
| Mean age years | 78.3 | 75.3 | 72.5 |
| Median, years (range) age | 79 (57- 98) | 75 (49–92) | 74 (45–89) |
| Smoking status, No. (%) | |||
| Never | 53 (59.6%) | 16 (48.5%) | 7 (43.8%) |
| Former/Current | 29 (32.5%) | 15 (45.4%) | 8 (50.0%) |
| Missing | 7 (7.9%) | 2 (6.1%) | 1 (6.2%) |
| Tumor site, No. (%) | Breast 20 (22.5%) | ||
| Colorectal 18 (20.2%) | |||
| Prostate 16 (18.0%) | |||
| Bladder 6 (6.7%) | |||
| Lung 5 (5.6%) | Colorectal 5 (15.2%) | Bladder 4 (25%) | |
| Kidney 4 (4.5%) | Prostate 10 (30.3%) | Prostate 4 (25%) | |
| Stomach 4 (4.5%) | Breast 7 (21.2%) | Lung 2 (12.5%) | |
| Thyroid 4 (4.5%) | Bladder 2 (6.1%) | Colorectal 2 (12.5%) | |
| Uterus 3 (3.4%) | Lung 2 (6.1%) | Mesothelioma 1 (6.2%) | |
| Other 9 (10.0%) | Other 7 (21.2%) | Other 3 (15.8%) | |
| Comorbidities, No. (%) | |||
| 12 (13.5%) | 4 (12.1%) | 2 (12.5%) |
| 71 (79.8%) | 25 (75.8%) | 9 (56.3%) |
| 56 (62.9%) | 15 (45.5%) | 6 (37.5%) |
| 28 (31.5%) | 8 (24.2%) | 1 (6.3%) |
| ICU admission, No. (%) | 11 (12.4%) | 3 (9.1%) | 0 |
| Deaths, No. (%) | 35 (39.3%) | 9 (27.3%) | 3 (18.8%) |
| Lung CT Scan Finding | Total Patients (No. 1015) | Cancer Patients (No. 105) | Non-Cancer Patients (No. 910) | p | OR (95% CI) | |
|---|---|---|---|---|---|---|
| Ground-glass opacities | Presence | 98 (95.1%) | 98 (95.1%) | 851 (94.0%) | 0.649 | 1.44 (0.56–3.71) |
| Absence | 5 (4.9%) | 5 (4.9%) | 54 (6.0%) | |||
| Missing | 2 | 2 | 5 | |||
| Consolidation | Presence | 76 (74.5%) | 76 (74.5%) | 619 (68.3%) | 0.200 | 1.38 (0.86–0.20) |
| Absence | 26 (25.5%) | 26 (25.5%) | 287 (31.7%) | |||
| Missing | 3 | 3 | 4 | |||
| Visual extension | 0 | 0 (0.0%) | 0 (0.0%) | 12 (1.5%) | 0.190 | 1.48 (0.95–2.33) * 1.39 (0.84–2.29) ** |
| 1–19% | 12 (13.5%) | 12 (13.5%) | 163 (20.9%) | |||
| 20–39% | 28 (31.4%) | 28 (31.4%) | 262 (33.6%) | |||
| 40–59% | 24 (27.0%) | 24 (27.0%) | 181 (23.2%) | |||
| ≥60% | 25 (28.1%) | 25 (28.1%) | 162 (20.8%) | |||
| Missing | 16 | 16 | 130 | |||
| Death (No. 52) | ICU Admission or Death (No. 58) | ICU Admission (No. 12) | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Age (>74 vs. ≤74 years) * | 2.95 | 1.29–6.78 | 1.53 | 0.73–3.23 | 0.11 | 0.03–0.41 |
| Age (per 10 year increase) * | 2.20 | 1.41–3.42 | 1.60 | 1.09–2.35 | 0.28 | 0.13–0.57 |
| Gender (male vs. female) ^ | 1.98 | 0.87–4.51 | 1.66 | 0.77–3.55 | 1.85 | 0.46–7.47 |
| Metastatic disease ^^ | 3.84 | 0.80–17.51 | 2.14 | 0.50–9.16 | - | ** |
| Cancer diagnosis ≤5 years “ | 0.31 | 0.11–0.84 | 0.38 | 0.15–0.95 | 0.2 | 0.03–1.30 |
| Cancer diagnosis <1 years § | 0.13 | 0.02–1.04 | 0.14 | 0.02–0.92 | 1 | - |
| Breast cancer *** | 0.74 | 0.21–2.63 | 0.90 | 0.28–2.88 | 1.41 | 0.16–12.65 |
| Colorectal cancer *** | 0.94 | 0.34–2.61 | 1.25 | 0.48–3.23 | 1.44 | 0.31–6.51 |
| Bladder cancer *** | 1.80 | 0.48–4.75 | 1.52 | 0.42–5.47 | 1.52 | 0.15–15.21 |
| Lung cancer *** | 0.78 | 0.16–3.74 | 0.66 | 0.14–3.03 | 0.95 | 0.08–11.25 |
| Former smokers *** | 1 | 1 | 1 | |||
| Never smokers * | 0.47 | 0.19–1.25 | 0.48 | 0.20–1.18 | 0.21 | 0.04–1.07 |
| Smokers * | 0.38 | 0.08–1.32 | 0.55 | 0.13–2.30 | 0.44 | 0.04–4.52 |
| COPD *** | 0.38 | 0.11–1.28 | 0.46 | 0.15–1.42 | 2.43 | 0.39–15.18 |
| Hypertension *** | 1.74 | 0.67–4.54 | 1.21 | 0.51–2.88 | 0.96 | 0.22–4.22 |
| Diabetes mellitus *** | 0.56 | 0.23–1.38 | 0.75 | 0.33–1.71 | 0.62 | 0.14–2.78 |
| Cardiovasc. disease *** | 1.58 | 0.68–3.68 | 1.14 | 0.52–2.49 | 0.68 | 0.16–2.86 |
| Characteristics | All Patients | Deaths |
|---|---|---|
| Gender, No. (%) | ||
| Female | 5 (35.7%) | 0 |
| Male | 9 (64.3%) | 5 |
| Median age, years (range) | 79 (49–90) | 79 (65–81) |
| Stage of disease, No. (%) | ||
| Localized | 3 (21.4%) | 1 |
| Metastatic | 11 (78.6%) | 4 |
| Setting of therapy, No. (%) | ||
| Adjuvant | 3 (21.4%) | 1 |
| Metastatic 1st line | 4 (28.6%) | 1 |
| Metastatic > 1st line | 7 (50.0%) | 3 |
| Tumor site, No. (%) | Lung 3 (21.4%) | |
| Bladder 3 (21.4%) | Lung 1 | |
| Ovary 3 (21.4%) | Bladder 2 | |
| Colorectal 2 (14.3%) | ||
| Breast 1 (7.1%) | Colorectal 2 | |
| Pleura 1 (7.1%) | ||
| Prostate 1 (7.1%) | ||
| Lung metastasis, No. (%) | 6 (42.8%) | 1 |
| Cancer treatments within 60 days, No. (%) | ||
| CHT alone * | 8 (57.1%) | 3 |
| CHT plus antiangiogenic drugs ** | 3 (21.4%) | 2 |
| CHT plus immunotherapy *** | ||
| Hormone therapy § | 1 (7.1%) | 0 |
| 2 (14.3%) | 0 | |
| Smoking status, No. (%) | ||
| Never | 8 (5.71%) | 3 |
| Former/Current | 4 (28.6%) | 2 |
| Missing | 2 (14.3%) | 0 |
| Hypertension, No. (%) | 10 (71.4%) | 3 |
| Diabetes mellitus, No. (%) | 2 (14.3%) | 1 |
| COPD, No. (%) | 2 (14.3%) | 0 |
| Cardiovasc. disease, No. (%) | 4 (28.6%) | 3 |
| Flu vaccination, No. (%) | 6 (42.8%) | 1 |
| COVID-19 treatments, No. (%) | ||
| Hydroxychloroquine and/or | 13 (92.8%) | 5 |
| Azithromycin | ||
| Antiviral drugs ^ | 7 (50%) | 4 |
| Glucocorticoids | 12 (85.7%) | 4 |
| Heparin | 12 (85.7%) | 4 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinto, C.; Berselli, A.; Mangone, L.; Damato, A.; Iachetta, F.; Foracchia, M.; Zanelli, F.; Gervasi, E.; Romagnani, A.; Prati, G.; et al. SARS-CoV-2 Positive Hospitalized Cancer Patients during the Italian Outbreak: The Cohort Study in Reggio Emilia. Biology 2020, 9, 181. https://doi.org/10.3390/biology9080181
Pinto C, Berselli A, Mangone L, Damato A, Iachetta F, Foracchia M, Zanelli F, Gervasi E, Romagnani A, Prati G, et al. SARS-CoV-2 Positive Hospitalized Cancer Patients during the Italian Outbreak: The Cohort Study in Reggio Emilia. Biology. 2020; 9(8):181. https://doi.org/10.3390/biology9080181
Chicago/Turabian StylePinto, Carmine, Annalisa Berselli, Lucia Mangone, Angela Damato, Francesco Iachetta, Marco Foracchia, Francesca Zanelli, Erika Gervasi, Alessandra Romagnani, Giuseppe Prati, and et al. 2020. "SARS-CoV-2 Positive Hospitalized Cancer Patients during the Italian Outbreak: The Cohort Study in Reggio Emilia" Biology 9, no. 8: 181. https://doi.org/10.3390/biology9080181