
A Comparative Event-Related Potentials Study between Alcohol Use Disorder, Gambling Disorder and Healthy Control Subjects through a Contextual Go/NoGo Task
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
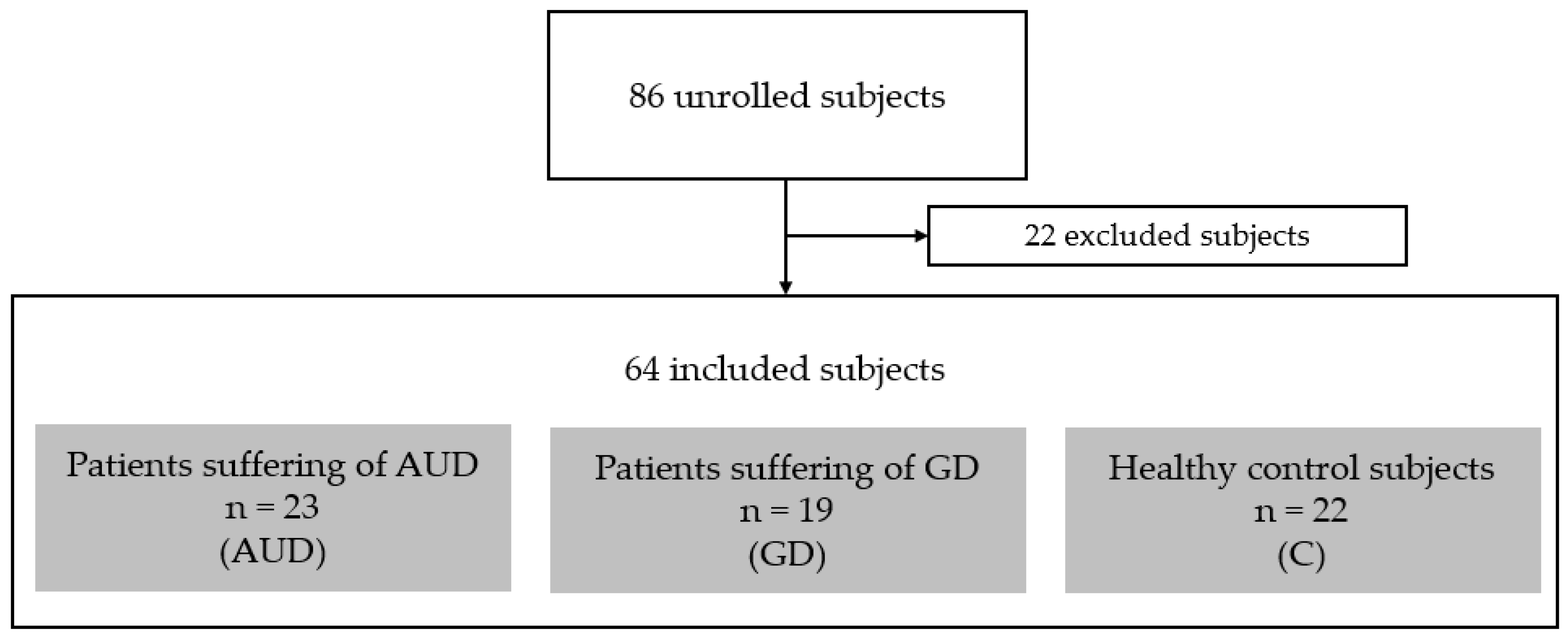
2.1. Participants and Ethics Statement
2.2. Procedure
- The Beck Depression Inventory (BDI-II) [35] to score the severity of depression symptoms (21 items; range, 0–63). A score of 10–18 indicates mild depression; a score of 19–29 indicates moderate depression; and a score of 30–63 indicates severe depression.
- The Alcohol Use Disorder Identification Test (AUDIT) [36] to score the severity of alcohol use (10 items; range, 0–40). Problematic alcohol use is assumed for a score higher than 12 for males and 11 for females.
- The South Oaks Gambling Screen (SOGS) [37] to score the severity of gambling use (20 items; range, 0–20). Problematic gambling practice is considered for a score of 5 or more.
2.3. Contextual Go/NoGo Tasks
2.4. EEG Recording and Treatment
2.5. Statistics
3. Results
3.1. Clinical Data
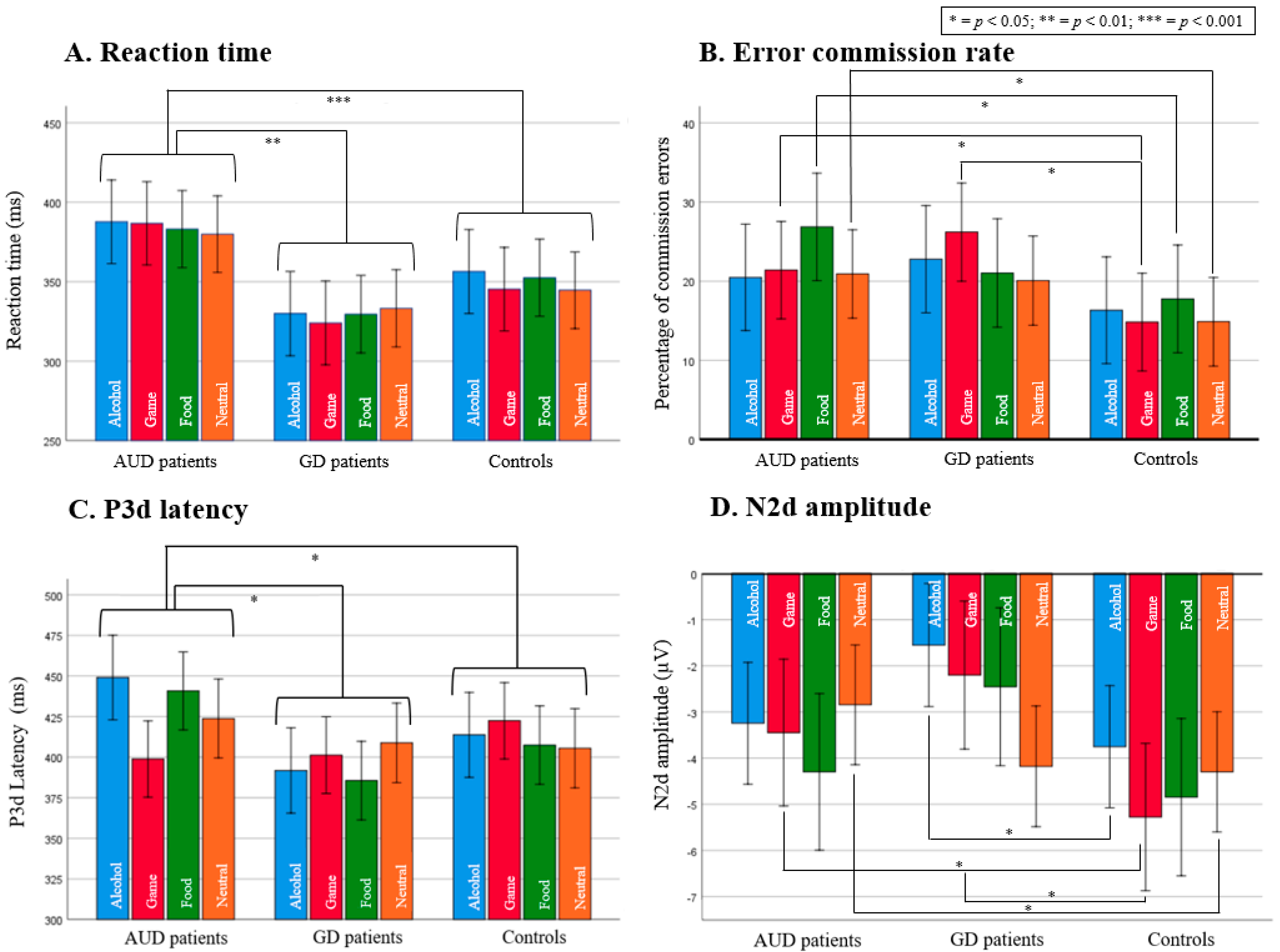
3.2. Reaction Time Results
3.3. Performance Results
3.3.1. AUD Patients Exhibit a Higher Commission Error Rate in the Food Context but Not in the Alcohol Context
3.3.2. GD Patients Exhibit a Higher Commission Error Rate in the Game Context
3.4. Correlations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Logan, G.D.; Cowan, W.B. On the ability to inhibit thought and action: A theory of an act of control. Psychol. Rev. 1984, 91, 295–327. [Google Scholar] [CrossRef]
- Noël, X.; Brevers, D.; Bechara, A. A neurocognitive approach to understanding the neurobiology of addiction. Curr. Opin. Neurobiol. 2013, 23, 632–638. [Google Scholar] [CrossRef] [PubMed]
- Noël, X.; Van der Linden, M.; Schmidt, N.; Sferrazza, R.; Hanak, C.; Le Bon, O.; De Mol, J.; Kornreich, C.; Pelc, I.; Verbanck, P. Supervisory Attentional System in Nonamnesic Alcoholic Men. Arch. Gen. Psychiatry 2001, 58, 1152–1158. [Google Scholar] [CrossRef] [PubMed]
- Brevers, D.; Noël, X. Pathological gambling and the loss of willpower: A neurocognitive perspective. Socioaffect Neurosci. Psychol. 2013, 3, 21592. [Google Scholar] [CrossRef] [PubMed]
- Wiers, R.W.; Bartholow, B.D.; Wildenberg, E.V.D.; Thush, C.; Engels, R.C.; Sher, K.J.; Grenard, J.; Ames, S.L.; Stacy, A.W. Automatic and controlled processes and the development of addictive behaviors in adolescents: A review and a model. Pharmacol. Biochem. Behav. 2007, 86, 263–283. [Google Scholar] [CrossRef] [PubMed]
- Volkow, N.D.; Fowler, J.S.; Wang, G.-J.; Swanson, J.M. Dopamine in drug abuse and addiction: Results from imaging studies and treatment implications. Mol. Psychiatry 2004, 9, 557–569. [Google Scholar] [CrossRef] [PubMed]
- Field, M.; Cox, W.M. Attentional bias in addictive behaviors: A review of its development, causes, and consequences. Drug Alcohol. Depend. 2008, 97, 1–20. [Google Scholar] [CrossRef]
- Robinson, T.E.; Berridge, K.C. The neural basis of drug craving: An incentive-sensitization theory of addiction. Brain Res. Brain Res. Rev. 1993, 18, 247–291. [Google Scholar] [CrossRef]
- Goldstein, R.Z.; Volkow, N.D. Dysfunction of the prefrontal cortex in addiction: Neuroimaging findings and clinical implications. Nat. Rev. Neurosci. 2011, 12, 652–669. [Google Scholar] [CrossRef]
- Goldstein, R.Z.; Volkow, N.D. Drug addiction and its underlying neurobiological basis: Neuroimaging evidence for the involvement of the frontal cortex. Am. J. Psychiatry 2002, 159, 1642–1652. [Google Scholar] [CrossRef]
- Zilverstand, A.; Huang, A.S.; Alia-Klein, N.; Goldstein, R.Z. Neuroimaging Impaired Response Inhibition and Salience Attribution in Human Drug Addiction. A systematic review. Neuron 2018, 98, 886–903. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, T.; Villebro, N.; Møller, A.M. Interventions for preoperative smoking cessation. Cochrane Database Syst. Rev. 2014, 3, CD002294. [Google Scholar] [CrossRef] [PubMed]
- Verdejo-Garcia, A.; Rezapour, T.; Giddens, E.; Zonoozi, A.K.; Rafei, P.; Berry, J.; Caracuel, A.; Copersino, M.L.; Field, M.; Garland, E.L.; et al. Cognitive training and remediation interventions for substance use disorders: A Delphi consensus study. Addiction 2022. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.L.; Mattick, R.P.; Jamadar, S.D.; Iredale, J.M. Deficits in behavioural inhibition in substance abuse and addiction: A meta-analysis. Drug Alcohol. Depend. 2014, 145, 1–33. [Google Scholar] [CrossRef] [PubMed]
- Harper, S.R. Using qualitative methods to assess student trajectories and college impact. New Dir. Inst. Res. 2007, 136, 55–68. [Google Scholar] [CrossRef]
- Goudriaan, A.E.; Oosterlaan, J.; de Beurs, E.; Brink, W.V.D. Neurocognitive functions in pathological gambling: A comparison with alcohol dependence, Tourette syndrome and normal controls. Addiction 2006, 101, 534–547. [Google Scholar] [CrossRef]
- Lawrence, A.; Luty, J.; Bogdan, N.A.; Sahakian, B.; Clark, L. Problem gamblers share deficits in impulsive decision-making with alcohol-dependent individuals. Addiction 2009, 104, 1006–1015. [Google Scholar] [CrossRef]
- Comings, D.E.; Blum, K. Reward deficiency syndrome: Genetic aspects of behavioral disorders. Prog. Brain Res. 2000, 126, 325–341. [Google Scholar] [CrossRef]
- Goldstein, R.; Goldstein, R.Z.; Alia-Klein, N.; Tomasi, D.; Zhang, L.; Cottone, L.A.; Maloney, T.; Telang, F.; Caparelli, E.C.; Chang, L.; et al. Is decreased prefrontal cortical sensitivity to monetary reward associated with impaired motivation and self-control in cocaine addiction? Am. J. Psychiatry 2007, 164, 43–51. [Google Scholar] [CrossRef]
- Vanes, L.; Van Holst, R.J.; Jansen, J.M.; Brink, W.V.D.; Oosterlaan, J.; Goudriaan, A.E. Contingency Learning in Alcohol Dependence and Pathological Gambling: Learning and Unlearning Reward Contingencies. Alcohol. Clin. Exp. Res. 2014, 38, 1602–1610. [Google Scholar] [CrossRef]
- Sescousse, G.; Caldú, X.; Segura, B.; Dreher, J.-C. Processing of primary and secondary rewards: A quantitative meta-analysis and review of human functional neuroimaging studies. Neurosci. Biobehav. Rev. 2013, 37, 681–696. [Google Scholar] [CrossRef] [PubMed]
- Martins, J.S.; Joyner, K.J.; McCarthy, D.M.; Morris, D.H.; Patrick, C.J.; Bartholow, B.D. Differential brain responses to alcohol-related and natural rewards are associated with alcohol use and problems: Evidence for reward dysregulation. Addict. Biol. 2022, 27, e13118. [Google Scholar] [CrossRef] [PubMed]
- Romanczuk-Seiferth, N.; Koehler, S.; Dreesen, C.; Wüstenberg, T.; Heinz, A. Pathological gambling and alcohol dependence: Neural disturbances in reward and loss avoidance processing. Addict. Biol. 2015, 20, 557–569. [Google Scholar] [CrossRef] [PubMed]
- Balconi, M.; Venturella, I.; Finocchiaro, R. Evidences from Rewarding System, FRN and P300 Effect in Internet-Addiction in Young People. Brain Sci. 2017, 7, 81. [Google Scholar] [CrossRef] [PubMed]
- Balconi, M.; Angioletti, L. Neurophysiology of Gambling Behavior and Internet Use Vulnerability: A Comparison Between Behavioral and EEG Measures. Clin. EEG Neurosci. 2022, 53, 268–277. [Google Scholar] [CrossRef]
- Detandt, S.; Bazan, A.; Schröder, E.; Olyff, G.; Kajosch, H.; Verbanck, P.; Campanella, S. A smoking-related background helps moderate smokers to focus: An event-related potential study using a Go-NoGo task. Clin. Neurophysiol. 2017, 128, 1872–1885. [Google Scholar] [CrossRef]
- Dong, G.; Lu, Q.; Zhou, H.; Zhao, X. Impulse inhibition in people with Internet addiction disorder: Electrophysiological evidence from a Go/NoGo study. Neurosci. Lett. 2010, 485, 138–142. [Google Scholar] [CrossRef]
- Dousset, C.; Chenut, C.; Kajosch, H.; Kornreich, C.; Campanella, S. Comparison of Neural Correlates of Reactive Inhibition in Cocaine, Heroin, and Polydrug Users through a Contextual Go/No-Go Task Using Event-Related Potentials. Biology 2022, 11, 1029. [Google Scholar] [CrossRef]
- Littel, M.; Euser, A.S.; Munafò, M.R.; Franken, I.H. Electrophysiological indices of biased cognitive processing of substance-related cues: A meta-analysis. Neurosci. Biobehav. Rev. 2012, 36, 1803–1816. [Google Scholar] [CrossRef]
- Petit, G.; Kornreich, C.; Noël, X.; Verbanck, P.; Campanella, S. Alcohol-Related Context Modulates Performance of Social Drinkers in a Visual Go/No-Go Task: A Preliminary Assessment of Event-Related Potentials. PLoS ONE 2012, 7, e37466. [Google Scholar] [CrossRef]
- Rugg, M.D.; Coles, M.G.H. Electrophysiology of Mind; Oxford University Press: Oxford, UK, 1996. [Google Scholar] [CrossRef]
- Albert, J.; López-Martín, S.; Carretié, L. Emotional context modulates response inhibition: Neural and behavioral data. Neuroimage 2010, 49, 914–921. [Google Scholar] [CrossRef] [PubMed]
- Petit, G.; Kornreich, C.; Dan, B.; Verbanck, P.; Campanella, S. Electrophysiological correlates of alcohol- and non-alcohol-related stimuli processing in binge drinkers: A follow-up study. J. Psychopharmacol. 2014, 28, 1041–1052. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Balker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59 (Suppl. 20), 22–33; quiz 34–57. [Google Scholar] [PubMed]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Saunders, J.B.; Aasland, O.G.; Babor, T.F.; De La Fuente, J.R.; Grant, M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption-II. Addiction 1993, 88, 791–804. [Google Scholar] [CrossRef] [PubMed]
- Lesieur, H.R.; Blume, S.B. The South Oaks Gambling Screen (SOGS): A new instrument for the identification of pathological gamblers. Am. J. Psychiatry 1987, 144, 1184–1188. [Google Scholar] [CrossRef]
- Cornil, A.; Long, J.; Rothen, S.; Perales, J.C.; de Timary, P.; Billieux, J. The gambling craving experience questionnaire: Psychometric properties of a new scale based on the elaborated intrusion theory of desire. Addict. Behav. 2019, 95, 110–117. [Google Scholar] [CrossRef]
- May, J.; Andrade, J.; Kavanagh, D.; Feeney, G.F.X.; Gullo, M.; Statham, D.J.; Skorka-Brown, J.; Connolly, J.M.; Cassimatis, M.; Young, R.; et al. The Craving Experience Questionnaire: A brief, theory-based measure of consummatory desire and craving: CEQ: Craving Experience Questionnaire. Addiction 2014, 109, 728–735. [Google Scholar] [CrossRef]
- Drollette, E.S.; Scudder, M.R.; Raine, L.B.; Moore, R.D.; Saliba, B.J.; Pontifex, M.B.; Hillman, C.H. Acute exercise facilitates brain function and cognition in children who need it most: An ERP study of individual differences in inhibitory control capacity. Dev. Cogn. Neurosci. 2014, 7, 53–64. [Google Scholar] [CrossRef]
- Pires, L.; Leitão, J.; Guerrini, C.; Simoes, M. Event-related brain potentials in the study of inhibition: Cognitive control, source localization and age-related modulations. Neuropsychol. Rev. 2014, 24, 461–490. [Google Scholar] [CrossRef]
- Yuan, J.; He, Y.; Qinglin, Z.; Chen, A.; Li, H. Gender differences in behavioral inhibitory control: ERP evidence from a two-choice oddball task. Psychophysiology 2008, 45, 986–993. [Google Scholar] [CrossRef] [PubMed]
- Verbruggen, F.; Logan, G.D.; Stevens, M.A. STOP-IT: Windows executable software for the stop-signal paradigm. Behav. Res. Methods 2008, 40, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Krull, K.R.; Smith, L.T.; Parsons, O.A. Simple reaction time event-related potentials: Effects of alcohol and diazepam. Progress. Neuro-Psychopharmacol. Biol. Psychiatry 1994, 18, 1247–1260. [Google Scholar] [CrossRef] [PubMed]
- Noël, X.; Van der Linden, M.; D’acremont, M.; Bechara, A.; Dan, B.; Hanak, C.; Verbanck, P. Alcohol cues increase cognitive impulsivity in individuals with alcoholism. Psychopharmacology 2007, 192, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Flaudias, V.; Brousse, G.; de Chazeron, I.; Planche, F.; Brun, J.; Llorca, P.-M. Treatment in hospital for alcohol-dependent patients decreases attentional bias. Neuropsychiatr. Dis. Treat. 2013, 9, 773–779. [Google Scholar] [CrossRef]
- Gough, T.; Christiansen, P.; Rose, A.K.; Hardman, C.A. The effect of alcohol on food-related attentional bias, food reward and intake: Two experimental studies. Appetite 2021, 162, 105173. [Google Scholar] [CrossRef]
- Gordon, E.L.; Ariel-Donges, A.H.; Bauman, V.; Merlo, L.J. What Is the Evidence for ‘Food Addiction? A Systematic Review. Nutrients 2018, 10, 477. [Google Scholar] [CrossRef]
- Brevers, D.; He, Q.; Keller, B.; Noël, X.; Bechara, A. Neural correlates of proactive and reactive motor response inhibition of gambling stimuli in frequent gamblers. Sci. Rep. 2017, 7, 7394. [Google Scholar] [CrossRef]
- Yau, Y.H.C.; Potenza, M.N. Gambling Disorder and Other Behavioral Addictions: Recognition and Treatment. Harv. Rev. Psychiatry 2015, 23, 134–146. [Google Scholar] [CrossRef]
- Hatoum, A.S.; Colbert, S.M.; Johnson, E.C.; Huggett, S.B.; Deak, J.D.; Pathak, A.G.; Jennings, M.V.; Paul, E.S.; Karcher, N.R.; Hansen, I.; et al. Multivariate genome-wide association meta-analysis of over 1 million subjects identifies loci underlying multiple substance use disorders. Addict. Med. 2022. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AUD Patients n = 23 | GD Patients n = 19 | Controls n = 23 | F/χ2 | p | Post-Hoc Analyses | ||||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | ||||
| Age | 47.52 | 8.37 | 39.68 | 8.79 | 32.45 | 8.46 | 17.582 | <0.001 | AUD > GD > C |
| Education (number of years) | 13.74 | 3.08 | 12.11 | 2.45 | 14.32 | 2.36 | 3.724 | 0.030 | C > GD |
| Female/Male | 8/15 | 1/18 | 9/13 | 7.195 | 0.027 | AUD > G, C > GD | |||
| BDI-II | 18.35 | 10.36 | 19.58 | 11.14 | 6.36 | 6.70 | 12.702 | <0.001 | AUD > C, GD > C |
| AUDIT | 31.65 | 5.58 | 6.32 | 5.50 | 4.68 | 3.87 | 200.522 | <0.001 | AUD > GD, AUD > C |
| SOGS | 0.26 | 0.62 | 12.42 | 3.47 | 0.09 | 0.29 | 258.244 | <0.001 | GD > AUD, GD > C |
| Alcohol CEQ | |||||||||
| intensity | 24.39 | 12.59 | / | / | / | / | / | / | / |
| frequency | 24.57 | 13.23 | / | / | / | / | / | / | / |
| Gambling CEQ | |||||||||
| intensity | / | / | 40.80 | 17.70 | / | / | / | / | / |
| frequency | / | / | 35.53 | 14.64 | / | / | / | / | / |
| Number of years of dependence | 11.93 | 10.08 | 14.68 | 14.45 | / | / | 0.525 | 0.473 | / |
| Number of previous alcohol detoxification | 1.17 | 1.34 | 0.00 | 0.00 | 0.00 | 0.00 | 1.153 | <0.001 | AUD > GD = C |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dubuson, M.; Noël, X.; Kornreich, C.; Hanak, C.; Saeremans, M.; Campanella, S. A Comparative Event-Related Potentials Study between Alcohol Use Disorder, Gambling Disorder and Healthy Control Subjects through a Contextual Go/NoGo Task. Biology 2023, 12, 643. https://doi.org/10.3390/biology12050643
Dubuson M, Noël X, Kornreich C, Hanak C, Saeremans M, Campanella S. A Comparative Event-Related Potentials Study between Alcohol Use Disorder, Gambling Disorder and Healthy Control Subjects through a Contextual Go/NoGo Task. Biology. 2023; 12(5):643. https://doi.org/10.3390/biology12050643
Chicago/Turabian StyleDubuson, Macha, Xavier Noël, Charles Kornreich, Catherine Hanak, Mélanie Saeremans, and Salvatore Campanella. 2023. "A Comparative Event-Related Potentials Study between Alcohol Use Disorder, Gambling Disorder and Healthy Control Subjects through a Contextual Go/NoGo Task" Biology 12, no. 5: 643. https://doi.org/10.3390/biology12050643