
Ischemic Conditioning to Reduce Fatigue in Isometric Skeletal Muscle Contraction



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects and Study Design
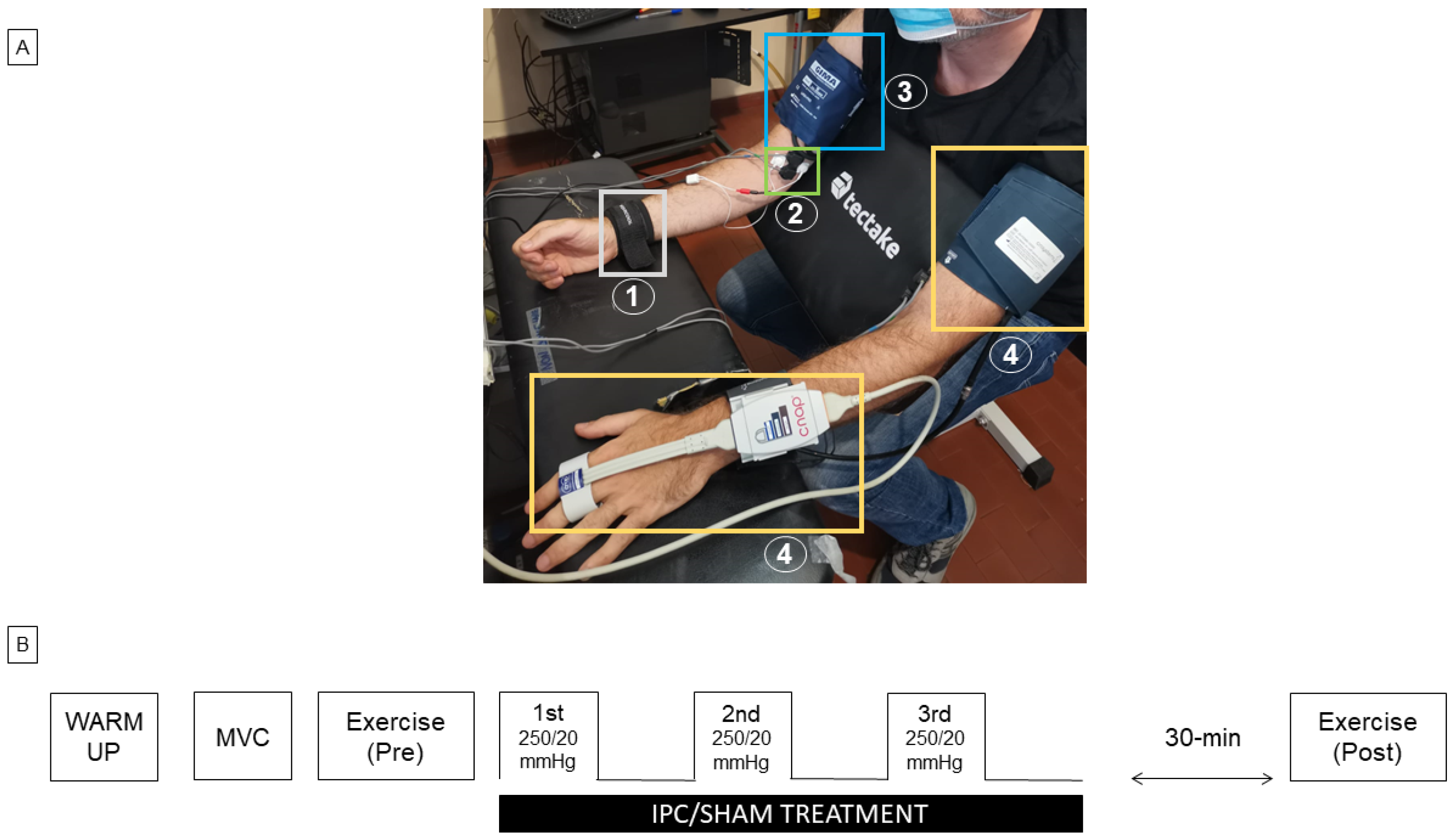
2.2. Experimental Set-Up
2.3. Experimental Protocol and Exhaustion Detection
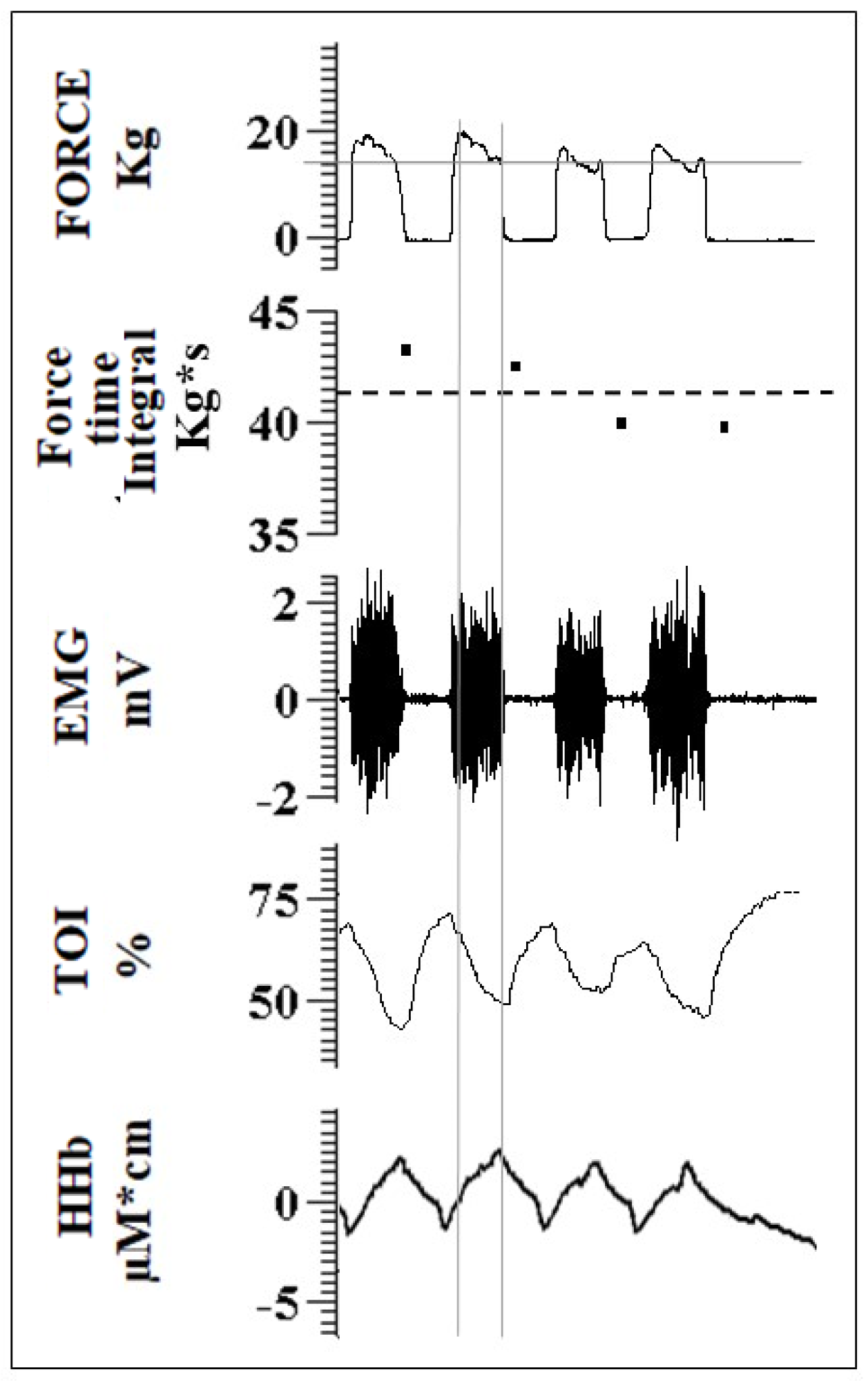
2.4. Data Analysis
2.5. Statical Analysis
3. Results
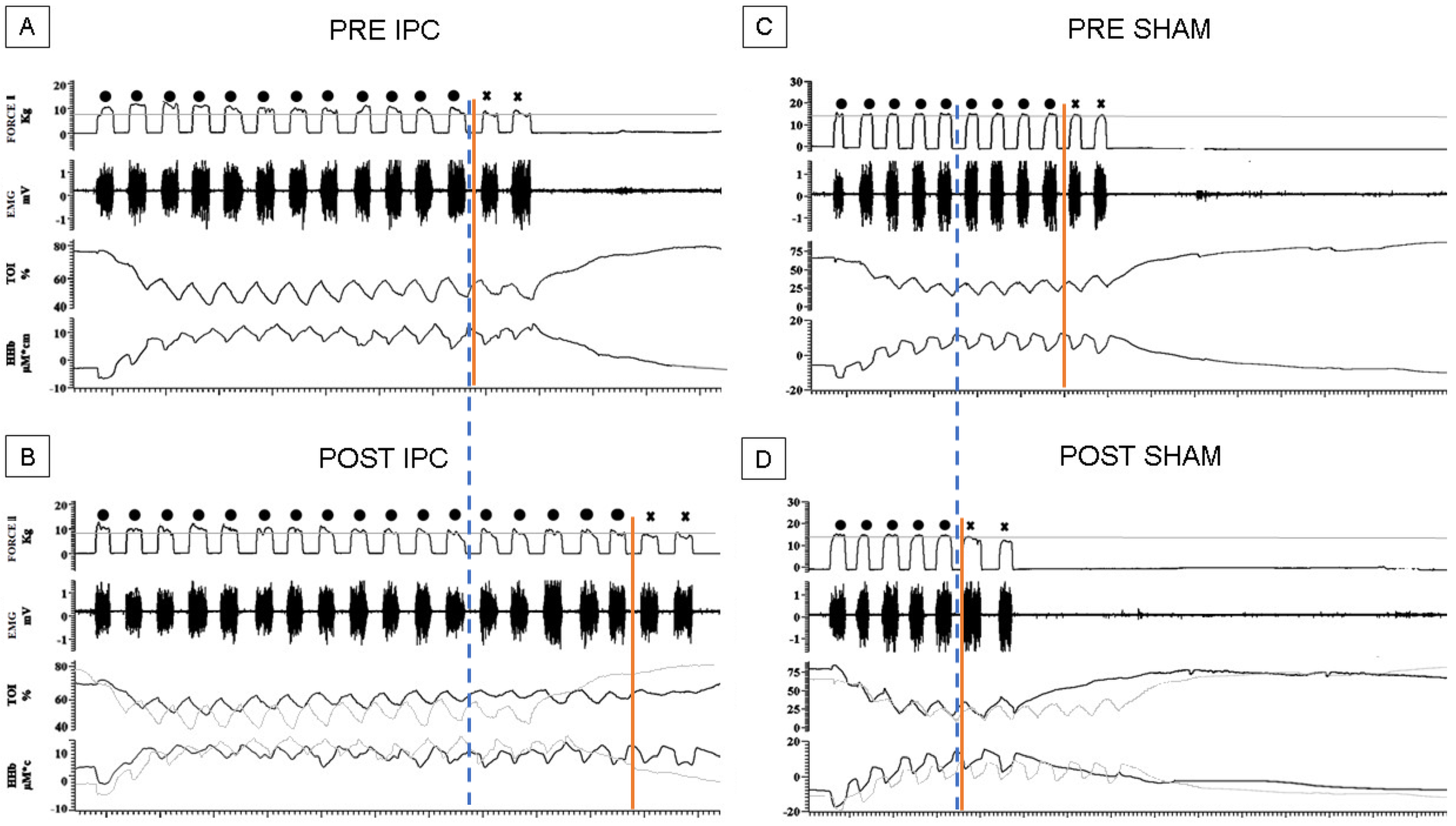
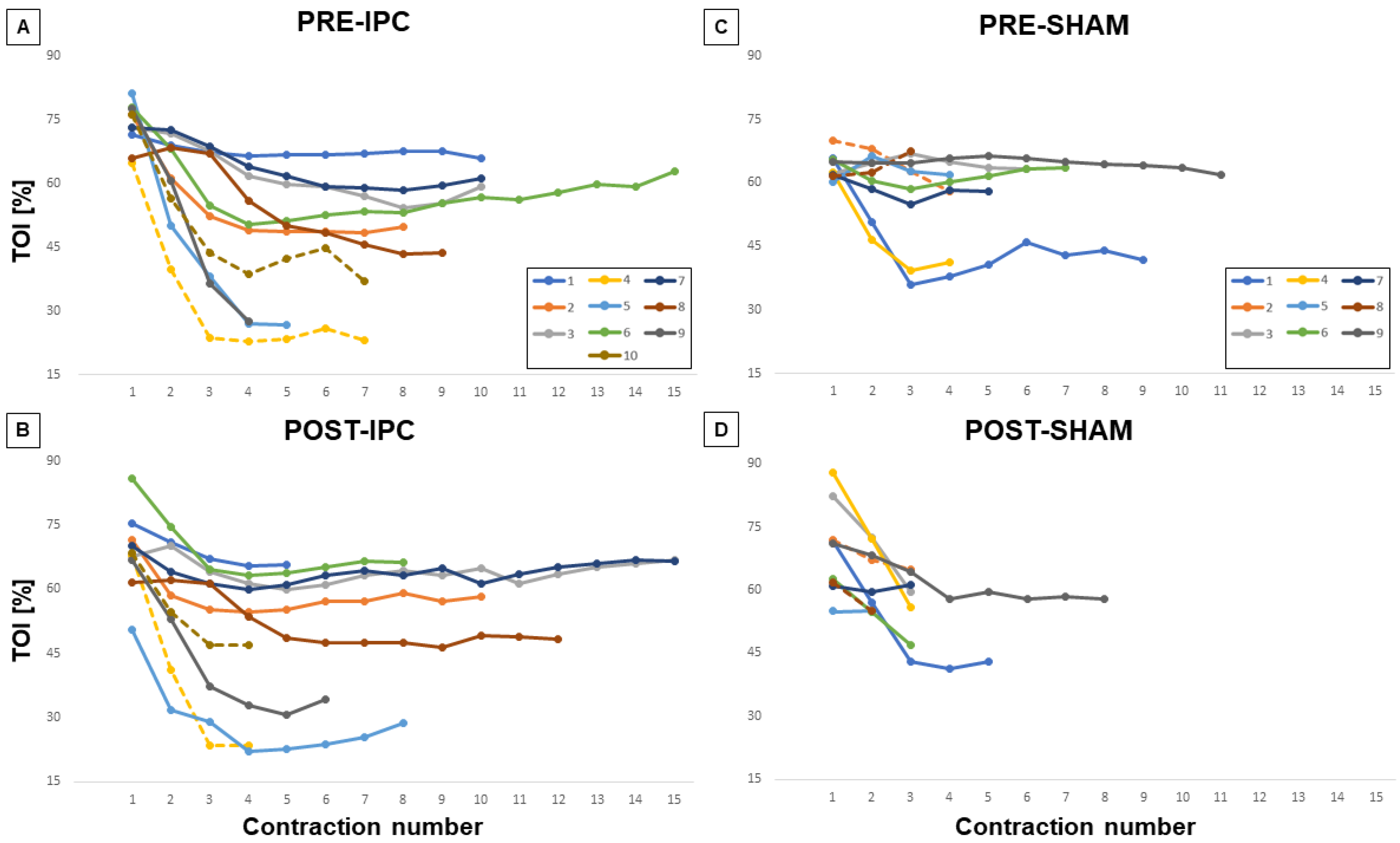
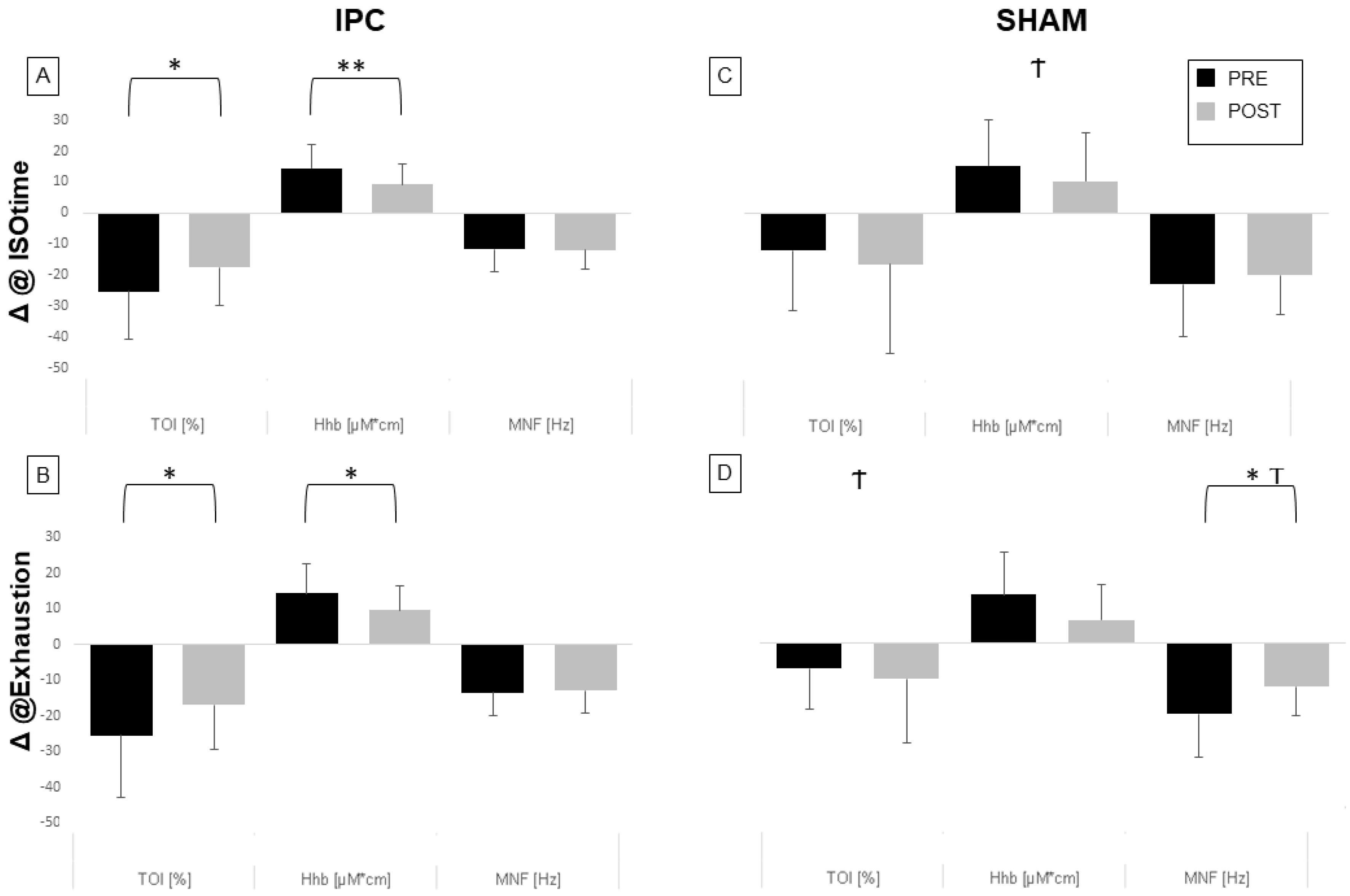
3.1. Hemodynamic Changes during Exercise
3.2. EMG Changes during Exercise
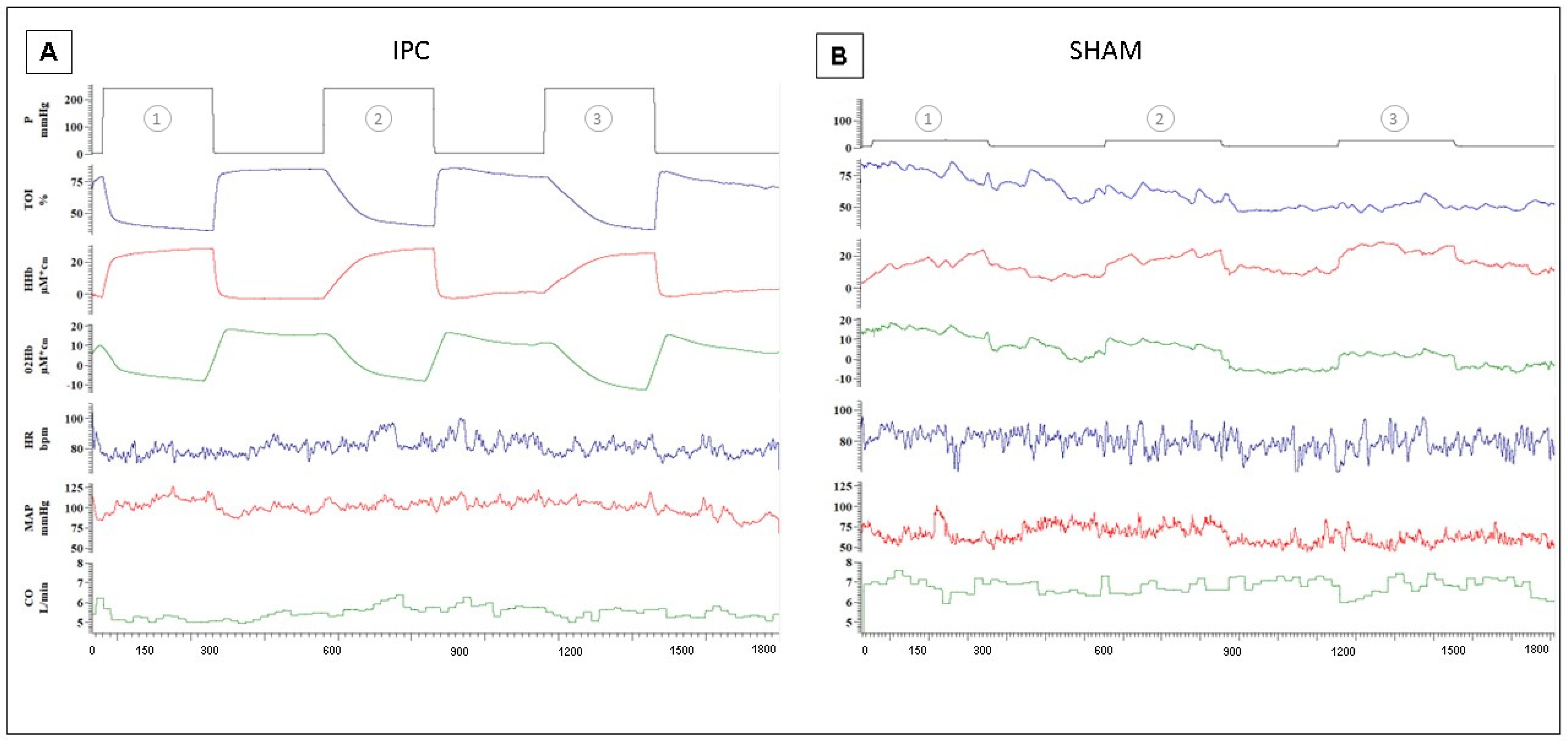
3.3. Hemodynamic Changes during Treatment
4. Discussion
4.1. Effects of IPC on Exercise
4.2. Response to the Subsequent Ischemic Stimuli of IPC
4.3. Experimental Set-Up Advantages and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thuret, R.; Saint Yves, T.; Tillou, X.; Chatauret, N.; Thuillier, R.; Barrou, B.; Billault, C. Ischemic Pre- and Post-Conditioning: Current Clinical Applications. Progrès Urol. 2014, 24, S56–S61. [Google Scholar] [CrossRef] [PubMed]
- Tullio, F.; Angotti, C.; Perrelli, M.-G.; Penna, C.; Pagliaro, P. Redox Balance and Cardioprotection. Basic Res. Cardiol. 2013, 108, 392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hausenloy, D.J.; Barrabes, J.A.; Bøtker, H.E.; Davidson, S.M.; Di Lisa, F.; Downey, J.; Engstrom, T.; Ferdinandy, P.; Carbrera-Fuentes, H.A.; Heusch, G.; et al. Ischaemic Conditioning and Targeting Reperfusion Injury: A 30 Year Voyage of Discovery. Basic Res. Cardiol. 2016, 111, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagliaro, P.; Gattullo, D.; Rastaldo, R.; Losano, G. Ischemic Preconditioning: From the First to the Second Window of Protection. Life Sci. 2001, 69, 1–15. [Google Scholar] [CrossRef]
- Incognito, A.V.; Burr, J.F.; Millar, P.J. The Effects of Ischemic Preconditioning on Human Exercise Performance. Sports Med. 2016, 46, 531–544. [Google Scholar] [CrossRef]
- Hausenloy, D.; Lim, S. Remote Ischemic Conditioning: From Bench to Bedside. Front. Physiol. 2012, 3, 27. [Google Scholar] [CrossRef] [Green Version]
- Heusch, G. Myocardial Ischaemia–Reperfusion Injury and Cardioprotection in Perspective. Nat. Rev. Cardiol. 2020, 17, 773–789. [Google Scholar] [CrossRef]
- Gaspar, A.; Lourenço, A.P.; Pereira, M.Á.; Azevedo, P.; Roncon-Albuquerque, R.; Marques, J.; Leite-Moreira, A.F. Randomized Controlled Trial of Remote Ischaemic Conditioning in ST-Elevation Myocardial Infarction as Adjuvant to Primary Angioplasty (RIC-STEMI). Basic Res. Cardiol. 2018, 113, 14. [Google Scholar] [CrossRef]
- Griffin, J.; Ferguson, R.; Gissane, C.; Bailey, S.; Patterson, S. Ischemic Preconditioning Enhances Critical Power during a 3 Minute All-out Cycling Test. J. Sport. Sci. 2017, 36, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Seeger, J.P.H.; Timmers, S.; Ploegmakers, D.J.M.; Cable, N.T.; Hopman, M.T.E.; Thijssen, D.H.J. Is Delayed Ischemic Preconditioning as Effective on Running Performance during a 5 km Time Trial as Acute IPC? J. Sci. Med. Sport. 2017, 20, 208–212. [Google Scholar] [CrossRef] [Green Version]
- Cocking, S.; Wilson, M.G.; Nichols, D.; Cable, N.T.; Green, D.J.; Thijssen, D.H.J.; Jones, H. Is There an Optimal Ischemic-Preconditioning Dose to Improve Cycling Performance? Int. J. Sport. Physiol. Perform. 2018, 13, 274–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, A.; Goyal, R. Experimental Brain Ischemic Preconditioning: A Concept to Putative Targets. CNS Neurol. Disord. Drug Targets 2016, 15, 489–495. [Google Scholar] [CrossRef]
- Penna, C.; Alloatti, G.; Crisafulli, A. Mechanisms Involved in Cardioprotection Induced by Physical Exercise. Antioxid. Redox Signal. 2020, 32, 1115–1134. [Google Scholar] [CrossRef]
- de Groot, P.C.E.; Thijssen, D.H.J.; Sanchez, M.; Ellenkamp, R.; Hopman, M.T.E. Ischemic Preconditioning Improves Maximal Performance in Humans. Eur. J. Appl. Physiol. 2009, 108, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvador, A.; Aguiar, R.; Lisbôa, F.; Pereira, K.; Cruz, R.; Caputo, F. Ischemic Preconditioning and Exercise Performance: A Systematic Review and Meta-Analysis. Int. J. Sport. Physiol. Perform. 2015, 11, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.Z.; Baynosa, R.C.; Zamboni, W.A. Therapeutic Interventions Against Reperfusion Injury in Skeletal Muscle. J. Surg. Res. 2011, 171, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Bailey, T.G.; Jones, H.; Gregson, W.; Atkinson, G.; Cable, N.T.; Thijssen, D.H.J. Effect of Ischemic Preconditioning on Lactate Accumulation and Running Performance. Med. Sci. Sports Exerc. 2012, 44, 2084–2089. [Google Scholar] [CrossRef] [Green Version]
- Kjeld, T.; Rasmussen, M.R.; Jattu, T.; Nielsen, H.B.; Secher, N.H. Ischemic Preconditioning of One Forearm Enhances Static and Dynamic Apnea. Med. Sci. Sports Exerc. 2014, 46, 151–155. [Google Scholar] [CrossRef] [Green Version]
- Marocolo, M.; Simim, M.A.M.; Bernardino, A.; Monteiro, I.R.; Patterson, S.D.; da Mota, G.R. Ischemic Preconditioning and Exercise Performance: Shedding Light through Smallest Worthwhile Change. Eur. J. Appl. Physiol. 2019, 119, 2123–2149. [Google Scholar] [CrossRef]
- Fox, C.; Walsh, P.; Mulhall, K.J. Molecular Mechanism of Ischaemic Preconditioning of Skeletal Muscle In Vitro. Cureus 2018, 10, e3763. [Google Scholar] [CrossRef] [Green Version]
- Caru, M.; Levesque, A.; Lalonde, F.; Curnier, D. An Overview of Ischemic Preconditioning in Exercise Performance: A Systematic Review. J. Sport. Health Sci. 2019, 8, 355–369. [Google Scholar] [CrossRef] [PubMed]
- Kido, K.; Suga, T.; Tanaka, D.; Honjo, T.; Homma, T.; Fujita, S.; Hamaoka, T.; Isaka, T. Ischemic Preconditioning Accelerates Muscle Deoxygenation Dynamics and Enhances Exercise Endurance during the Work-to-Work Test. Physiol. Rep. 2015, 3, e12395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanaka, D.; Suga, T.; Tanaka, T.; Kido, K.; Honjo, T.; Fujita, S.; Hamaoka, T.; Isaka, T. Ischemic Preconditioning Enhances Muscle Endurance during Sustained Isometric Exercise. Int. J. Sports Med. 2016, 37, 614–618. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Cruz, R.S.; de Aguiar, R.A.; Turnes, T.; Salvador, A.F.; Caputo, F. Effects of Ischemic Preconditioning on Short-Duration Cycling Performance. Appl. Physiol. Nutr. Metab. 2016, 41, 825–831. [Google Scholar] [CrossRef]
- da Mota, G.R.; Willis, S.J.; Sobral, N.D.S.; Borrani, F.; Billaut, F.; Millet, G.P. Ischemic Preconditioning Maintains Performance on Two 5-Km Time Trials in Hypoxia. Med. Sci. Sports Exerc. 2019, 51, 2309–2317. [Google Scholar] [CrossRef]
- Ferraresi, C.; De Benedictis, C.; Maffiodo, D.; Franco, W.; Messere, A.; Pertusio, R.; Roatta, S. Design and Simulation of a Novel Pneumotronic System Aimed to the Investigation of Vascular Phenomena Induced by Limb Compression. J. Bionic Eng. 2019, 16, 550–562. [Google Scholar] [CrossRef]
- Messere, A.; Pertusio, R.; Macrì, C.; Maffiodo, D.; Franco, W.; De Benedictis, C.; Ferraresi, C.; Roatta, S. Delivery of Customizable Compressive Patterns to Human Limbs to Investigate Vascular Reactivity. Biomed. Phys. Eng. Express 2018, 4, 067003. [Google Scholar] [CrossRef]
- Messere, A.; Roatta, S. Influence of Cutaneous and Muscular Circulation on Spatially Resolved versus Standard Beer-Lambert near-Infrared Spectroscopy. Physiol. Rep. 2013, 1, e00179. [Google Scholar] [CrossRef]
- Messere, A.; Roatta, S. Local and Remote Thermoregulatory Changes Affect NIRS Measurement in Forearm Muscles. Eur. J. Appl. Physiol. 2015, 115, 2281–2291. [Google Scholar] [CrossRef]
- Scano, A.; Pirovano, I.; Manunza, M.E.; Spinelli, L.; Contini, D.; Torricelli, A.; Re, R. Sustained Fatigue Assessment during Isometric Exercises with Time-Domain near Infrared Spectroscopy and Surface Electromyography Signals. Biomed. Opt. Express 2020, 11, 7357–7375. [Google Scholar] [CrossRef]
- Barbosa, T.C.; Machado, A.C.; Braz, I.D.; Fernandes, I.A.; Vianna, L.C.; Nobrega, A.C.L.; Silva, B.M. Remote Ischemic Preconditioning Delays Fatigue Development during Handgrip Exercise. Scand. J. Med. Sci. Sports 2015, 25, 356–364. [Google Scholar] [CrossRef]
- Souza, H.; Arriel, R.; Hohl, R.; Mota, G.; Marocolo, M. Is Ischemic Preconditioning Intervention Occlusion-Dependent to Enhance Resistance Exercise Performance? J. Strength Cond. Res. 2019, 35, 2706–2712. [Google Scholar] [CrossRef]
- Mota, G.R.; Rightmire, Z.B.; Martin, J.S.; McDonald, J.R.; Kavazis, A.N.; Pascoe, D.D.; Gladden, L.B. Ischemic Preconditioning Has No Effect on Maximal Arm Cycling Exercise in Women. Eur. J. Appl. Physiol. 2020, 120, 369–380. [Google Scholar] [CrossRef] [PubMed]
- Rashid, A.; Roatta, S. Differential Control of Blood Flow in Masseter and Biceps Brachii Muscles during Stress. Arch. Oral Biol. 2022, 141, 105490. [Google Scholar] [CrossRef] [PubMed]
- Orbegozo Cortés, D.; Puflea, F.; De Backer, D.; Creteur, J.; Vincent, J.-L. Near Infrared Spectroscopy (NIRS) to Assess the Effects of Local Ischemic Preconditioning in the Muscle of Healthy Volunteers and Critically Ill Patients. Microvasc. Res. 2015, 102, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Grassi, B.; Quaresima, V. Near-Infrared Spectroscopy and Skeletal Muscle Oxidative Function in Vivo in Health and Disease: A Review from an Exercise Physiology Perspective. J. Biomed. Opt. 2016, 21, 091313. [Google Scholar] [CrossRef] [Green Version]
- Andreas, M.; Schmid, A.I.; Keilani, M.; Doberer, D.; Bartko, J.; Crevenna, R.; Moser, E.; Wolzt, M. Effect of Ischemic Preconditioning in Skeletal Muscle Measured by Functional Magnetic Resonance Imaging and Spectroscopy: A Randomized Crossover Trial. J. Cardiovasc. Magn. Reson. 2011, 13, 32. [Google Scholar] [CrossRef] [Green Version]
- Paradis-Deschênes, P.; Joanisse, D.R.; Billaut, F. Sex-Specific Impact of Ischemic Preconditioning on Tissue Oxygenation and Maximal Concentric Force. Front. Physiol. 2017, 7, 674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canova, D.; Roatta, S.; Bosone, D.; Micieli, G. Inconsistent Detection of Changes in Cerebral Blood Volume by near Infrared Spectroscopy in Standard Clinical Tests. J. Appl. Physiol. (1985) 2011, 110, 1646–1655. [Google Scholar] [CrossRef] [PubMed]
- Messere, A.; Turturici, M.; Millo, G.; Roatta, S. Repetitive muscle compression reduces vascular mechano-sensitivity and the hyperemic response to muscle contraction. J. Physiol. Pharmacol. 2017, 68, 427–437. Available online: http://www.jpp.krakow.pl/journal/archive/06_17/pdf/427_06_17_article.pdf (accessed on 8 February 2023).






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allois, R.; Pagliaro, P.; Roatta, S. Ischemic Conditioning to Reduce Fatigue in Isometric Skeletal Muscle Contraction. Biology 2023, 12, 460. https://doi.org/10.3390/biology12030460
Allois R, Pagliaro P, Roatta S. Ischemic Conditioning to Reduce Fatigue in Isometric Skeletal Muscle Contraction. Biology. 2023; 12(3):460. https://doi.org/10.3390/biology12030460
Chicago/Turabian StyleAllois, Ruben, Pasquale Pagliaro, and Silvestro Roatta. 2023. "Ischemic Conditioning to Reduce Fatigue in Isometric Skeletal Muscle Contraction" Biology 12, no. 3: 460. https://doi.org/10.3390/biology12030460