

Tissue and Serum Biomarkers in Degenerative Aortic Stenosis-Insights into Pathogenesis, Prevention and Therapy

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
1.1. Irisin Levels
1.2. Periostin
1.3. Osteoglycin
1.4. Interleukin 18
1.5. HMGB1
1.6. PCSK9
2. Material and Methods
2.1. Ethics Statement
2.2. Study Population
2.3. Blood Analysis
2.4. Valve Cusp Immunohistochemistry and Quantitative Morphometrical Analysis
2.5. RNA Isolation and qRT PCR Analysis
2.6. Statistical Analysis
3. Results
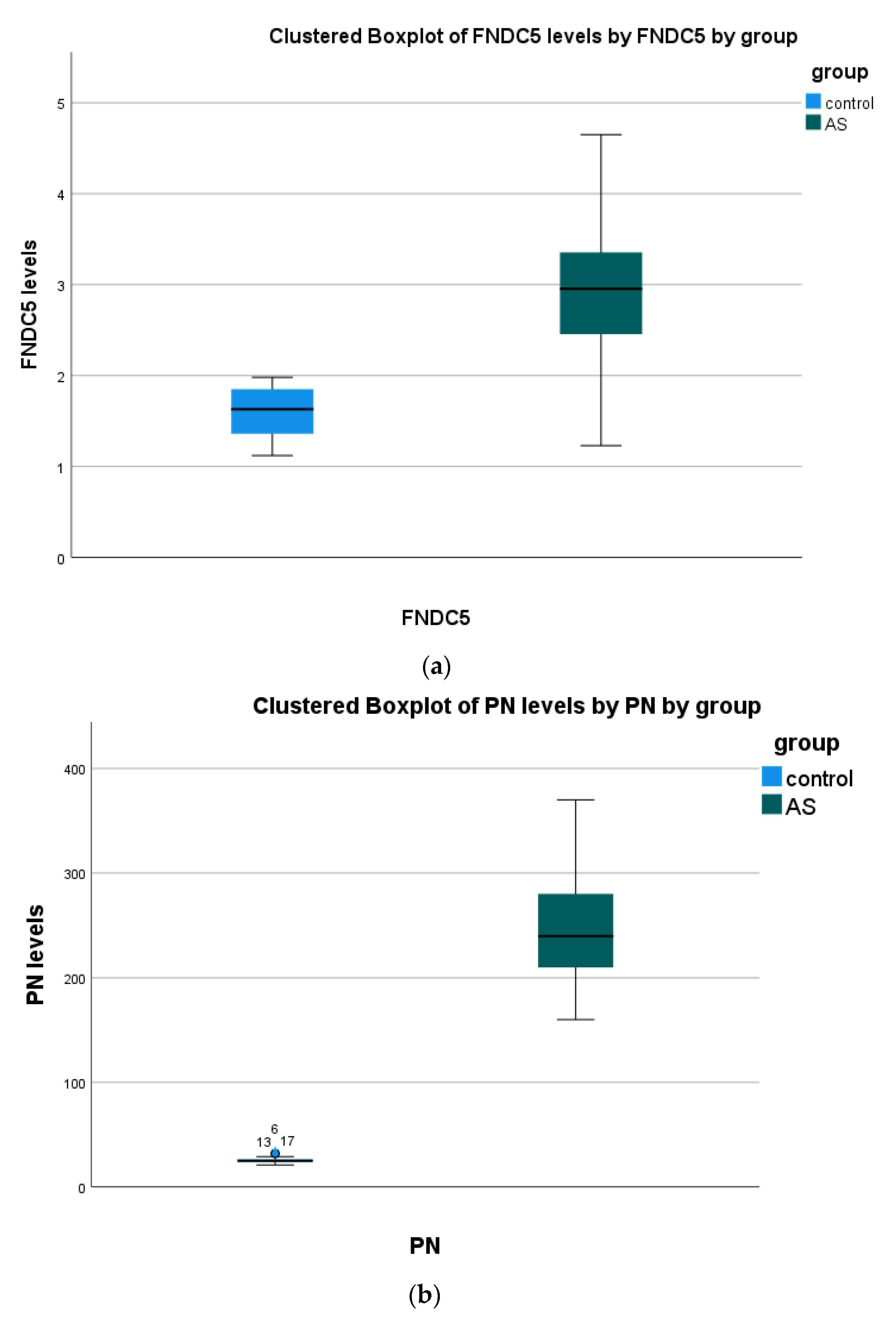
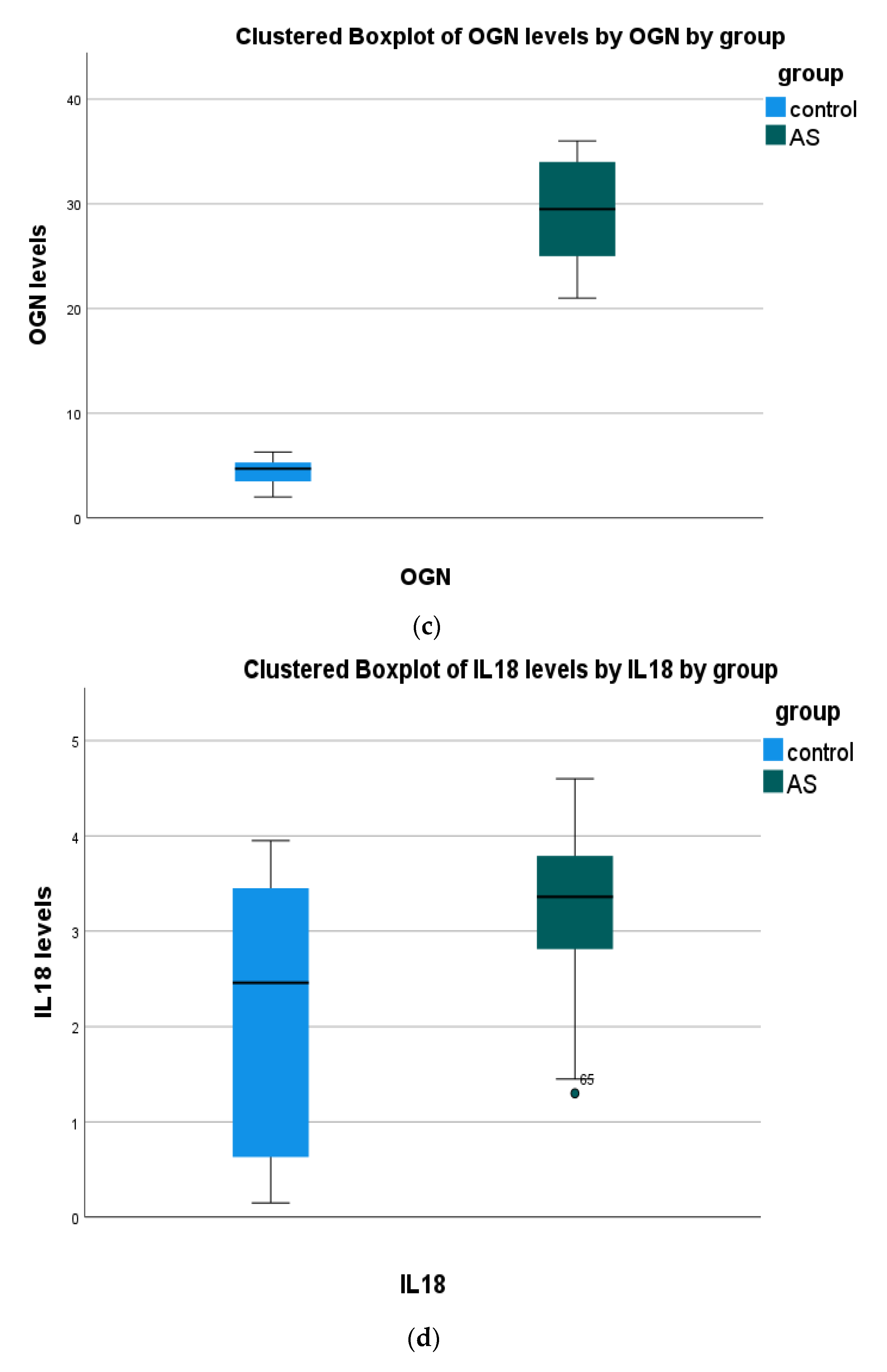
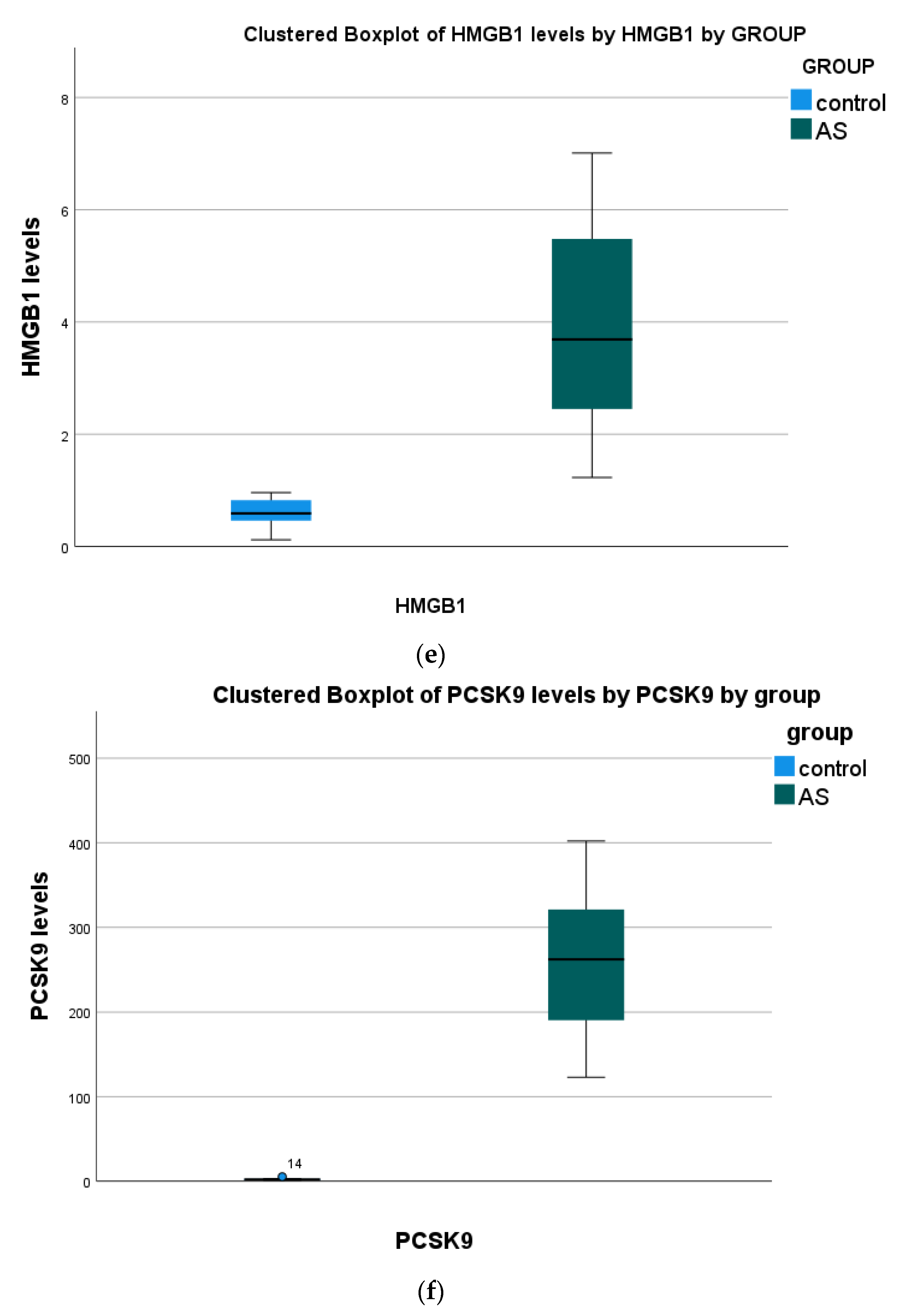
3.1. Serum Findings
3.2. Tissue vs. Serum
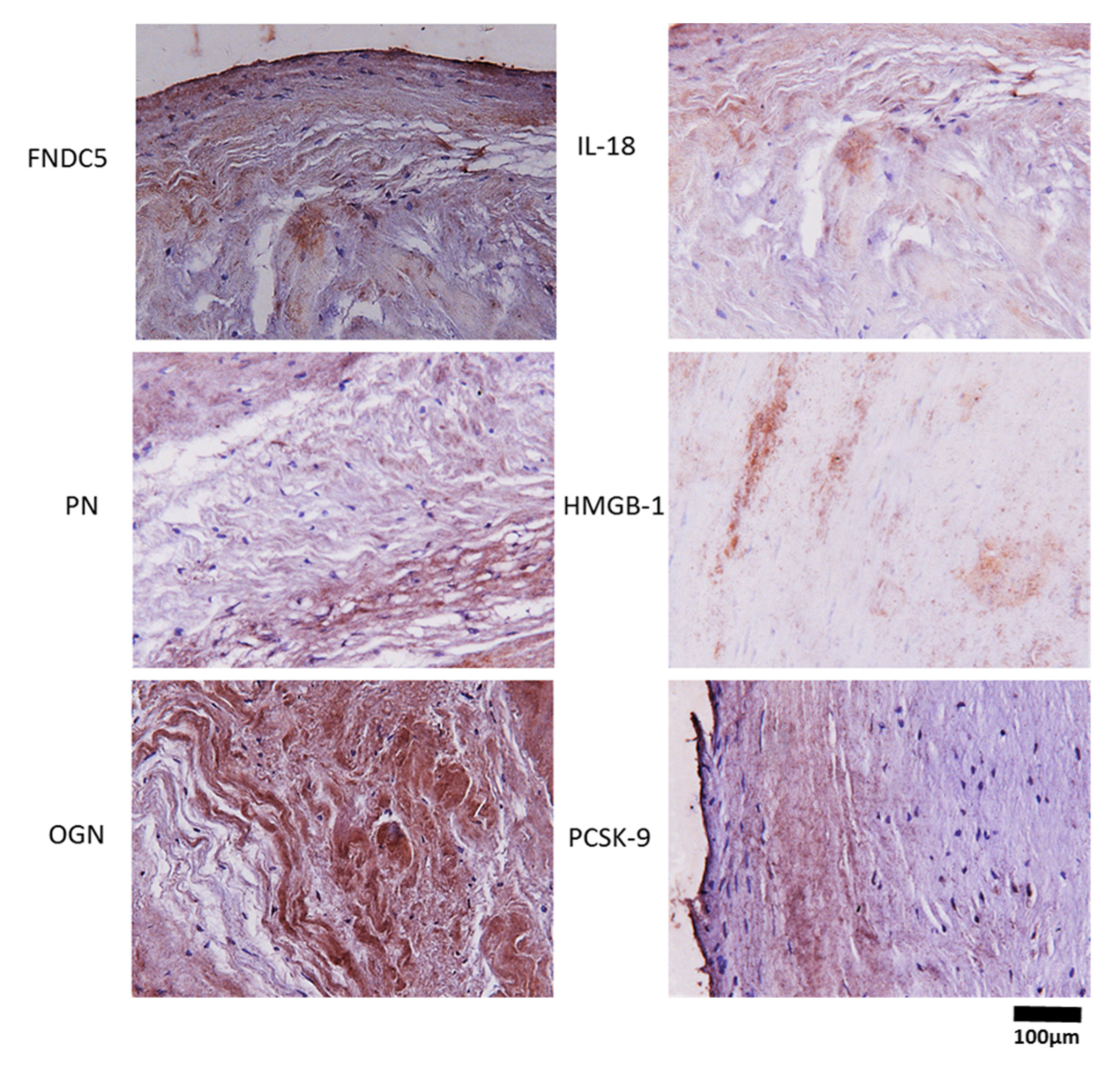
3.3. Immunohistochemistry Biomarkers in Aortic Valve Cusps
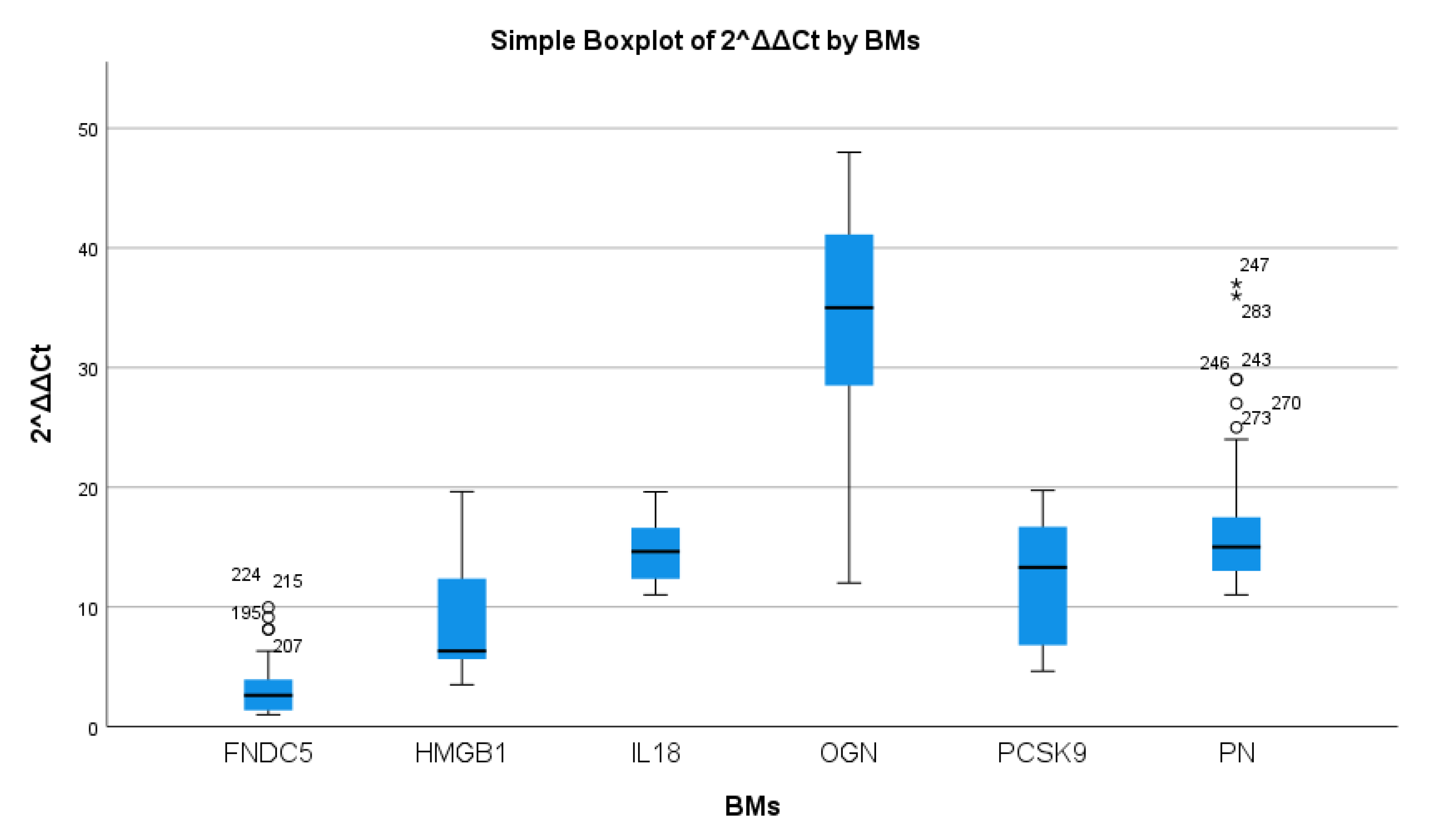
3.4. mRNA Expression of Inflammation and Calcification Biomarkers in AS Patients
3.5. Tissue Biomarkers Correlations
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Otto, C.M.; Prendergast, B. Aortic-Valve Stenosis—From Patients at Risk to Severe Valve Obstruction. N. Engl. J. Med. 2014, 371, 744–756. [Google Scholar] [CrossRef] [PubMed]
- Benamer, H.; Auffret, V.; Cayla, G.; Chevalier, B.; Commeau, P.; Dupouy, P.; Eltchaninoff, H.; Gilard, M.; Guerin, P.; Lung, B.; et al. Position papier français (GACI) pour l’implantation de valve aortique percutanée (TAVI). Arch. Mal. Coeur Vaiss. Prat. 2018, 2018, 32–40. [Google Scholar] [CrossRef]
- Nkomo, V.T.; Gardin, J.M.; Skelton, T.N.; Gottdiener, J.S.; Scott, C.G.; Enriquez-Sarano, M. Burden of valvular heart diseases: A population-based study. Lancet 2006, 368, 1005–1011. [Google Scholar] [CrossRef]
- Ortlepp, J.R.; Schmitz, F.; Bozoglu, T.; Hanrath, P.; Hoffmann, R. Cardiovascular risk factors in patients with aortic stenosis predict prevalence of coronary artery disease but not of aortic stenosis: An angiographic pair matched case-control study. Heart 2003, 89, 1019–1022. [Google Scholar] [CrossRef]
- Kapelouzou, A.; Tsourelis, L.; Kaklamanis, L.; Degiannis, D.; Kogerakis, N.; Cokkinos, D.V. Serum and tissue biomarkers in aortic stenosis. Glob. Cardiol. Sci. Pract. 2015, 2015, 49. [Google Scholar] [CrossRef]
- Helske, S.; Kupari, M.; Lindstedt, K.A.; Kovanen, P.T. Aortic valve stenosis: An active atheroinflammatory process. Curr. Opin. Infect. Dis. 2007, 18, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Kapelouzou, A.; Kontogiannis, C.; Tsilimigras, D.I.; Georgiopoulos, G.; Kaklamanis, L.; Tsourelis, L.; Cokkinos, D.V. Differential expression patterns of Toll Like Receptors and Interleukin-37 between calcific aortic and mitral valve cusps in humans. Cytokine 2019, 116, 150–160. [Google Scholar] [CrossRef]
- Passos, L.S.; Lupieri, A.; Becker-Greene, D.; Aikawa, E. Innate and adaptive immunity in cardiovascular calcification. Atherosclerosis 2020, 306, 59–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aydin, S.; Kuloglu, T.; Aydin, S.; Eren, M.N.; Celik, A.; Yilmaz, M.; Kalayci, M.; Sahin, I.; Gungor, O.; Gurel, A.; et al. Cardiac, skeletal muscle and serum irisin responses to with or without water exercise in young and old male rats: Cardiac muscle produces more irisin than skeletal muscle. Peptides 2014, 52, 68–73. [Google Scholar] [CrossRef]
- Silvestrini, A.; Bruno, C.; Vergani, E.; Venuti, A.; Favuzzi, A.M.R.; Guidi, F.; Nicolotti, N.; Meucci, E.; Mordente, A.; Mancini, A. Circulating irisin levels in heart failure with preserved or reduced ejection fraction: A pilot study. PLoS ONE 2019, 14, e0210320. [Google Scholar] [CrossRef] [PubMed]
- Shen, S.; Gao, R.; Bei, Y.; Li, J.; Zhang, H.; Zhou, Y.; Yao, W.; Xu, D.; Zhou, F.; Jin, M.; et al. Serum Irisin Predicts Mortality Risk in Acute Heart Failure Patients. Cell. Physiol. Biochem. 2017, 42, 615–622. [Google Scholar] [CrossRef]
- Emanuele, E.; Minoretti, P.; Pareja-Galeano, H.; Sanchis-Gomar, F.; Garatachea, N.; Lucia, A. Serum Irisin Levels, Precocious Myocardial Infarction, and Healthy Exceptional Longevity. Am. J. Med. 2014, 127, 888–890. [Google Scholar] [CrossRef]
- Kuloglu, T.; Aydin, S.; Eren, M.N.; Yilmaz, M.; Sahin, I.; Kalayci, M.; Sarman, E.; Kaya, N.; Yilmaz, O.F.; Turk, A.; et al. Irisin: A potentially candidate marker for myocardial infarction. Peptides 2014, 55, 85–91. [Google Scholar] [CrossRef]
- Efe, T.H.; Açar, B.; Ertem, A.G.; Yayla, K.G.; Algül, E.; Yayla, K.G.; Ünal, S.; Bilgin, M.; Çimen, T.; Kirbaş, Ö.; et al. Serum Irisin Level Can Predict the Severity of Coronary Artery Disease in Patients with Stable Angina. Korean Circ. J. 2017, 47, 44–49. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.T.; Wang, H.; Zhang, S.; Du, J.; Zhuang, S.; Zhao, T.C. Irisin Ameliorates Hypoxia/Reoxygenation-Induced Injury through Modulation of Histone Deacetylase 4. PLoS ONE 2016, 11, e0166182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiao, X.; Nie, Y.; Ma, Y.; Chen, Y.; Cheng, R.; Yin, W.; Hu, Y.; Xu, W.; Xu, L. Irisin promotes osteoblast proliferation and differentiation via activating the MAP kinase signaling pathways. Sci. Rep. 2016, 6, 18732. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Wrann, C.D.; Jedrychowski, M.; Vidoni, S.; Kitase, Y.; Nagano, K.; Zhou, C.; Chou, J.; Parkman, V.J.A.; Novick, S.J.; et al. Irisin mediates effects on bone and fat via αV Integrin receptors. Cell 2018, 175, 1756–1768. [Google Scholar] [CrossRef] [Green Version]
- Colaianni, G.; Cinti, S.; Colucci, S.; Grano, M. Irisin and musculoskeletal health. Ann. N. Y. Acad. Sci. 2017, 1402, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Hakuno, D.; Kimura, N.; Yoshioka, M.; Mukai, M.; Kimura, T.; Okada, Y.; Yozu, R.; Shukunami, C.; Hiraki, Y.; Kudo, A.; et al. Periostin advances atherosclerotic and rheumatic cardiac valve degeneration by inducing angiogenesis and MMP production in humans and rodents. J. Clin. Investig. 2010, 120, 2292–2306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, S.; Wu, H.; Xia, W.; Chen, X.; Zhu, S.; Zhang, S.; Shao, Y.; Ma, W.; Yang, D.; Zhang, J. Periostin expression is upregulated and associated with myocardial fibrosis in human failing hearts. J. Cardiol. 2014, 63, 373–378. [Google Scholar] [CrossRef] [Green Version]
- Oka, T.; Xu, J.; Kaiser, R.A.; Melendez, J.; Hambleton, M.; Sargent, M.A.; Lorts, A.; Brunskill, E.W.; Dorn, G.W.; Conway, S.J.; et al. Genetic manipulation of periostin expression reveals a role in cardiac hypertrophy and ventricular remodeling. Circ. Res. 2007, 101, 313–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stansfield, W.E.; Andersen, N.M.; Tang, R.-H.; Selzman, C.H. Periostin Is a Novel Factor in Cardiac Remodeling After Experimental and Clinical Unloading of the Failing Heart. Ann. Thorac. Surg. 2009, 88, 1916–1921. [Google Scholar] [CrossRef] [Green Version]
- Qiu, X.; Ma, F.; Zhang, H. Circulating Levels of IL-13, TGF-β1, and Periostin as Potential Biomarker for Coronary Artery Disease with Acute Heart Failure. Evid. Based Complement. Altern. Med. 2021, 2021, 1690421. [Google Scholar] [CrossRef] [PubMed]
- Deckx, S.; Heggermont, W.; Carai, P.; Rienks, M.; Dresselaers, T.; Himmelreich, U.; van Leeuwen, R.; Lommen, W.; van der Velden, J.; Gonzalez, A.; et al. Osteoglycin prevents the development of age-related diastolic dysfunction during pressure overload by reducing cardiac fibrosis and inflammation. Matrix Biol. 2018, 66, 110–124. [Google Scholar] [CrossRef] [PubMed]
- Van Aelst, L.N.; Voss, S.; Carai, P.; Van Leeuwen, R.; Vanhoutte, D.; Sanders-van Wijk, S.; Eurlings, L.; Swinnen, M.; Verheyen, F.K.; Verbeken, E.; et al. Osteoglycin prevents cardiac dilatation and dysfunction after myocardial infarction through infarct collagen strengthening. Circ. Res. 2015, 116, 425–436. [Google Scholar] [CrossRef] [Green Version]
- Zuo, C.; Li, X.; Huang, J.; Chen, D.; Ji, K.; Yang, Y.; Xu, T.; Zhu, D.; Yan, C.; Gao, P. Osteoglycin attenuates cardiac fibrosis by suppressing cardiac myofibroblast proliferation and migration through antagonizing lysophosphatidic acid 3/matrix metalloproteinase 2/epidermal growth factor receptor signalling. Cardiovasc. Res. 2018, 114, 703–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, J.M.; Akkerhuis, K.M.; Meilhac, O.; Oemrawsingh, R.M.; Garcia-Garcia, H.M.; van Geuns, R.-J.; Piquer, D.; Merle, D.; du Paty, E.; Galéa, P.; et al. Circulating Osteoglycin and NGAL/MMP9 Complex Concentrations Predict 1-Year Major Adverse Cardiovascular Events after Coronary Angiography. Arter. Thromb. Vasc. Biol. 2014, 34, 1078–1084. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, K.-I.; Matsumoto, E.; Higashimaki, Y.; Katagiri, T.; Sugimoto, T.; Seino, S.; Kaji, H. Role of Osteoglycin in the Linkage between Muscle and Bone. J. Biol. Chem. 2012, 287, 11616–11628. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Markel, T.A.; Meldrum, D.R. Interleukin 18 in the heart. Shock 2008, 30, 3–10. [Google Scholar] [CrossRef]
- Naito, Y.; Tsujino, T.; Wakabayashi, K.; Matsumoto, M.; Ohyanagi, M.; Mitsuno, M.; Miyamoto, Y.; Hao, H.; Hirota, S.; Okamura, H.; et al. Increased interleukin-18 expression in nonrheumatic aortic valve stenosis. Int. J. Cardiol. 2010, 144, 260–263. [Google Scholar] [CrossRef]
- Zhou, J.; Zhu, J.; Jiang, L.; Zhang, B.; Zhu, D.; Wu, Y. Interleukin 18 promotes myofibroblast activation of valvular interstitial cells. Int. J. Cardiol. 2016, 221, 998–1003. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.; Vazquez, R.; Khojeini, E.V.; Patel, C.; Venkataramani, R.; Larson, D.F. IL-18 induction of osteopontin mediates cardiac fibrosis and diastolic dysfunction in mice. Am. J. Physiol. Heart Circ. Physiol. 2009, 297, H76–H85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jefferis, B.J.; Papacosta, O.; Owen, C.G.; Wannamethee, S.G.; Humphries, S.E.; Woodward, M.; Lennon, L.T.; Thomson, A.; Welsh, P.; Rumley, A.; et al. Interleukin 18 and coronary heart disease: Prospective study and systematic review. Atherosclerosis 2011, 217, 227–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, W.; Zhou, J.; Wang, C.; Xu, G.; Wu, Y.; Hu, Z. High mobility group box 1 induces calcification of aortic valve interstitial cells via toll-like receptor 4. Mol. Med. Rep. 2017, 15, 2530–2536. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.; Li, F.; Zhang, C.; Wei, G.; Liao, P.; Dong, N. High-mobility group box-1 protein induces osteogenic phenotype changes in aortic valve interstitial cells. J. Thorac. Cardiovasc. Surg. 2016, 151, 255–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, X.; Jiang, H.; Bai, Q.; Zhou, X.; Xu, C.; Lu, Z.; Cui, B.; Wen, H. Increased serum HMGB1 is related to the severity of coronary artery stenosis. Clin. Chim. Acta 2009, 406, 139–142. [Google Scholar] [CrossRef]
- Cheng, J.M.; Oemrawsingh, R.M.; Garcia-Garcia, H.M.; Boersma, E.; van Geuns, R.-J.; Serruys, P.W.; Kardys, I.; Akkerhuis, K.M. PCSK9 in relation to coronary plaque inflammation: Results of the ATHEROREMO-IVUS study. Atherosclerosis 2016, 248, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.; Xing, C.Y.; Zhao, K.; Deng, J.; Olmedo, D.A.; Ma, Z.; Zhang, M.; Wang, Y. Associations of pro-protein convertase subtilisin-like kexin type 9, soluble low-density lipoprotein receptor and coronary artery disease: A case-control study. Int. J. Cardiol. 2022, 350, 9–15. [Google Scholar] [CrossRef]
- Donato, L.J.; Saenger, A.K.; Train, L.J.; Kotzer, K.E.; Lagerstedt, S.A.; Hornseth, J.M.; Basu, A.; Winters, J.L.; Baudhuin, L.M. Genetic and biochemical analyses in dyslipidemic patients undergoing LDL apheresis. J. Clin. Apher. 2014, 29, 256–265. [Google Scholar] [CrossRef]
- Liberale, L.; Montecucco, F.; Camici, G.G.; Dallegri, F.; Vecchie, A.; Carbone, F.; Bonaventura, A. Treatment with Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitors to Reduce Cardiovascular Inflammation and Outcomes. Curr. Med. Chem. 2017, 24, 1403–1416. [Google Scholar] [CrossRef]
- Vavlukis, M.; Kedev, S. Effects of High Intensity Statin Therapy in the Treatment of Diabetic Dyslipidemia in Patients with Coronary Artery Disease. Curr. Pharm. Des. 2018, 24, 427–441. [Google Scholar] [CrossRef]
- Wang, W.-G.; He, Y.-F.; Chen, Y.-L.; Zhao, F.-M.; Song, Y.-Q.; Zhang, H.; Ma, Y.-H.; Guan, X.; Zhang, W.-Y.; Chen, X.-L.; et al. Proprotein convertase subtilisin/kexin type 9 levels and aortic valve calcification: A prospective, cross sectional study. J. Int. Med. Res. 2016, 44, 865–874. [Google Scholar] [CrossRef] [Green Version]
- Poggio, P.; Songia, P.; Cavallotti, L.; Barbieri, S.S.; Zanotti, I.; Arsenault, B.J.; Valerio, V.; Ferri, N.; Capoulade, R.; Camera, M. PCSK9 Involvement in Aortic Valve Calcification. J. Am. Coll. Cardiol. 2018, 72, 3225–3227. [Google Scholar] [CrossRef] [PubMed]
- Salaun, E.; Mahjoub, H.; Dahou, A.; Mathieu, P.; Larose, É.; Després, J.-P.; Rodés-Cabau, J.; Arsenault, B.J.; Puri, R.; Clavel, M.-A.; et al. Hemodynamic Deterioration of Surgically Implanted Bioprosthetic Aortic Valves. J. Am. Coll. Cardiol. 2018, 72, 241–251. [Google Scholar] [CrossRef]
- Kysenius, K.; Muggalla, P.; Mätlik, K.; Arumäe, U.; Huttunen, H.J. PCSK9 regulates neuronal apoptosis by adjusting ApoER2 levels and signaling. Cell. Mol. Life Sci. 2012, 69, 1903–1916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chomczynski, P.; Sacchi, N. Single-step method of RNA isolation by acid guanidinium thiocyanate-phenol-chloroform extraction. Anal. Biochem. 1987, 162, 156–159. [Google Scholar] [CrossRef]
- Weber, M.; Arnold, R.; Rau, M.; Brandt, R.; Berkovitsch, A.; Mitrovic, V.; Hamm, C. Relation of N-Terminal Pro–B-Type Natriuretic Peptide to Severity of Valvular Aortic Stenosis. Am. J. Cardiol. 2004, 94, 740–745. [Google Scholar] [CrossRef] [PubMed]
- Everett, R.J.; Clavel, M.-A.; Pibarot, P.; Dweck, M.R. Timing of intervention in aortic stenosis: A review of current and future strategies. Heart 2018, 104, 2067–2076. [Google Scholar] [CrossRef] [Green Version]
- Dweck, M.R.; Jones, C.; Joshi, N.V.; Fletcher, A.M.; Richardson, H.; White, A.; Marsden, M.; Pessotto, R.; Clark, J.C.; Wallace, W.A.; et al. Assessment of Valvular Calcification and Inflammation by Positron Emission Tomography in Patients with Aortic Stenosis. Circulation 2012, 125, 76–86. [Google Scholar] [CrossRef] [Green Version]
- Awan, M.S.; Irfan, B.; Zahid, I.; Mirza, Y.; Ali, S.A. Comparison of Polymerase Chain Reaction and Immunohistochemistry Assays for Analysing Human Papillomavirus Infection in Oral Squamous Cell Carcinoma. J. Clin. Diagn. Res. 2017, 11, XC10–XC13. [Google Scholar] [CrossRef]
- Bergmark, B.A.; O’Donoghue, M.L.; Murphy, S.A.; Kuder, J.F.; Ezhov, M.V.; Ceška, R.; Gouni-Berthold, I.; Jensen, H.K.; Tokgozoglu, S.L.; Mach, F.; et al. An Exploratory Analysis of Proprotein Convertase Subtilisin/Kexin Type 9 Inhibition and Aortic Stenosis in the FOURIER Trial. JAMA Cardiol. 2020, 5, 709–713. [Google Scholar] [CrossRef]
- Cowell, S.J.; Newby, D.E.; Prescott, R.J.; Bloomfield, P.; Reid, J.; Northridge, D.B.; Boon, N.A. A Randomized Trial of Intensive Lipid-Lowering Therapy in Calcific Aortic Stenosis. N. Engl. J. Med. 2005, 352, 2389–2397. [Google Scholar] [CrossRef]
- Rossebø, A.B.; Pedersen, T.R.; Boman, K.; Brudi, P.; Chambers, J.B.; Egstrup, K.; Gerdts, E.; Gohlke-Bärwolf, C.; Holme, I.; Kesäniemi, Y.A.; et al. Intensive Lipid Lowering with Simvastatin and Ezetimibe in Aortic Stenosis. N. Engl. J. Med. 2008, 359, 1343–1356. [Google Scholar] [CrossRef] [Green Version]
- Moura, L.M.; Ramos, S.F.; Zamorano, J.L.; Barros, I.M.; Azevedo, L.F.; Rocha-Gonçalves, F.; Rajamannan, N.M. Rosuvastatin affecting aortic valve endothelium to slow the progression of aortic stenosis. J. Am. Coll. Cardiol. 2007, 49, 554–561. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.L.; Teo, K.; Dumesnil, J.G.; Ni, A.; Tam, J.; ASTRONOMER Investigators. Effect of Lipid lowering with rosuvastatin on progression of aortic stenosis: Results of the aortic stenosis progression observation: Measuring effects of rosuvastatin (ASTRONOMER) trial. Circulation 2010, 121, 306–314. [Google Scholar] [CrossRef] [Green Version]
- Cokkinos, D.V.; Cokkinos, P.; Kolovou, G. Proprotein convertase subtilisin/kexin type 9 inhibitors: New insights into cardiovascular atherosclerotic pathophysiology with therapeutic implications. Arch. Cardiovasc. Dis. 2019, 112, 455–458. [Google Scholar] [CrossRef]
- Ferencik, M.; Chatzizisis, Y.S. Statins and the coronary plaque calcium “paradox”: Insights from non-invasive and invasive imaging. Atherosclerosis 2015, 241, 783–785. [Google Scholar] [CrossRef]
- Perrot, N.; Valerio, V.; Moschetta, D.; Boekholdt, S.M.; Dina, C.; Chen, H.Y.; Abner, E.; Martinsson, A.; Manikpurage, H.D.; Rigade, S.; et al. Genetic and In Vitro Inhibition of PCSK9 and Calcific Aortic Valve Stenosis. JACC Basic Transl. Sci. 2020, 5, 649–661. [Google Scholar] [CrossRef]
- Sundararaman, S.S.; Döring, Y.; van Der Vorst, E.P. PCSK9: A multi-faceted protein that is involved in cardiovascular biology. Biomedicines 2021, 9, 793. [Google Scholar] [CrossRef]
- Lee, Y.S.; Chou, Y.Y. Pathogenetic mechanism of senile calcific aortic stenosis: The role of apoptosis. Chin. Med. J. 1998, 111, 934–939. [Google Scholar]
- Punch, E.; Klein, J.; Diaba-Nuhoho, P.; Morawietz, H.; Garelnabi, M. Effects of PCSK9 Targeting: Alleviating Oxidation, Inflammation, and Atherosclerosis. J. Am. Heart Assoc. 2022, 11, e023328. [Google Scholar] [CrossRef] [PubMed]
- Jigheh, Z.A.; Haghjo, A.G.; Argani, H.; Roshangar, L.; Rashtchizadeh, N.; Sanajou, D.; Ahmad, S.N.S.; Rashedi, J.; Dastmalchi, S.; Abbasi, M.M. Empagliflozin alleviates renal inflammation and oxidative stress in streptozotocin-induced diabetic rats partly by repressing HMGB1-TLR4 receptor axis. Iran. J. Basic Med. Sci. 2019, 22, 384–390. [Google Scholar] [CrossRef]
- Sukhanov, S.; Higashi, Y.; Yoshida, T.; Mummidi, S.; Aroor, A.R.; Russell, J.J.; Bender, S.B.; DeMarco, V.G.; Chandrasekar, B. The SGLT2 inhibitor Empagliflozin attenuates interleukin-17A-induced human aortic smooth muscle cell proliferation and migration by targeting TRAF3IP2/ROS/NLRP3/Caspase-1-dependent IL-1β and IL-18 secretion. Cell. Signal. 2021, 77, 109825. [Google Scholar] [CrossRef]
- Uthman, L.; Homayr, A.; Hollmann, M.W.; Zuurbier, C.J.; Weber, N.C. Administration of SGLT2 inhibitor empagliflozin against TNF-α induced endothelial dysfunction in human venous and arterial endothelial cells. FASEB J. 2018, 32, 569.4. [Google Scholar] [CrossRef]
- Pirklbauer, M.; Sallaberger, S.; Staudinger, P.; Corazza, U.; Leierer, J.; Mayer, G.; Schramek, H. Empagliflozin Inhibits IL-1β-Mediated Inflammatory Response in Human Proximal Tubular Cells. Int. J. Mol. Sci. 2021, 22, 5089. [Google Scholar] [CrossRef]
- Tsai, K.-F.; Chen, Y.-L.; Chiou, T.; Chu, T.-H.; Li, L.-C.; Ng, H.-Y.; Lee, W.-C.; Lee, C.-T. Emergence of SGLT2 Inhibitors as Powerful Antioxidants in Human Diseases. Antioxidants 2021, 10, 1166. [Google Scholar] [CrossRef]
- Kvidal, P.; Bergström, P.R.; Hörte, L.G.; Ståhle, E. Observed and relative survival after aortic valve replacement. J. Am. Coll. Cardiol. 2000, 35, 747–756. [Google Scholar] [CrossRef] [Green Version]
- Adler, Y.; Vaturi, M.; Herz, I.; Iakobishvili, Z.; Toaf, J.; Fink, N.; Battler, A.; Sagie, A. Nonobstructive aortic valve calcification: A window to significant coronary artery disease. Atherosclerosis 2002, 161, 193–197. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primers | Forward | Reverse | bp | NM |
|---|---|---|---|---|
| b actin | CACCATTGGCAATGAGCGGTTC | AGGTCTTTGCGGATGTCCACGT | 101 | 1101 |
| FNDC5 | AGCGAGCCTGTGCTCTTCAAGA | GAACAGGACCACGACGATGATC | 120 | 1171940 |
| PN | CAGCAAACCACCTTCACGGATC | TTAAGGAGGCGCTGAACCATGC | 118 | 1135934 |
| OGN | CCATAATGCCCTGGAATCCGTG | CAGGCGTATCTCTTCAATGCGG | 125 | 14057 |
| IL-18 | GATAGCCAGCCTAGAGGTATGG | CCTTGATGTTATCAGGAGGATTCA | 120 | 1243211 |
| HMGB-1 | GCGAAGAAACTGGGAGAGATGTG | GCATCAGGCTTTCCTTTAGCTCG | 114 | 1313892 |
| PCKS-9 | GACACCAGCATACAGAGTGACC | GTGCCATGACTGTCACACTTGC | 118 | 174936 |
| Serum Markers | Median Control [95% CI] | Median AS [95% CI] | Mann–Whitney U | p-Value |
|---|---|---|---|---|
| IL-18 | 2.46 [1.26, 3.02] | 3.36 [2.95, 3.56] | 259.5 | 0.004 |
| HMGB1 | 0.59 [0.44, 0.76] | 2.98 [2.4, 13.86] | 0.00 | <0.001 |
| PCSK9 | 2.05 [1.2, 82.86] | 262.00 [1.57, 224.286] | 0.00 | <0.001 |
| OGN | 4.7 [3.5, 29.78] | 29.5 [27.64, 30.9] | 0.00 | <0.001 |
| PN | 25.00 [23.28, 45.75] | 240.00 [227.54, 265.36] | 0.00 | <0.001 |
| FNDC5 | 1.63 [1.1, 43.74] | 2.955 [2.2, 3.73] | 31.00 | <0.001 |
| Biomarkers Compared | Spearman Rho | p-Value | 95% Confidence Intervals | |
|---|---|---|---|---|
| Serum vs. serum | OGN with PN | −0.359 | 0.005 | [−0.567, 0.108] |
| IL-18 with OGN | −0.441 | <0.001 | [−0.630, 0.203] | |
| HMGB1 with PCSK9 | 0.445 | 0.001 | [0.173, 0.610] | |
| PN vs PSCK9 | 0.286 | 0.027 | [ 0.027, 0.509] | |
| Tissue vs. tissue | IL-18 with HMGB1 | −0.425 | <0.001 | [−0.618, −0.185] |
| IL-18 with PCSK9 | −0.528 | <0.001 | [−0.694, −0.310] | |
| HMGB1 with PCSK9 | 0.420 | 0.001 | [0.178, 0.613] | |
| Tissue vs. serum | IL-18 with FNDC5 | −0.291 | 0.024 | [−0.513, −0.033] |
| IL-18 with OGN | −0.419 | 0.001 | [−0.613, −0.177] | |
| HMGB1 with IL-18 | −0.326 | 0.011 | [−0.541, −0.071] | |
| HMGB1 with OGN | 0.282 | 0.029 | [0.022, 0.506] | |
| PCSK9 with IL-18 | −0.405 | 0.001 | [−0.602, −0.161] | |
| PCSK9 with HMGB1 | −0.326 | 0.011 | [−0.541, −0.070] | |
| PCSK9 with OGN | 0.604 | <0.001 | [0.407, 0.747] | |
| PN with PN | 0.289 | 0.025 | [0.030, 0.511] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kapelouzou, A.; Geronikolou, S.; Lidoriki, I.; Kontogiannis, C.; Kaklamanis, L.; Tsourelis, L.; Cokkinos, D.V. Tissue and Serum Biomarkers in Degenerative Aortic Stenosis-Insights into Pathogenesis, Prevention and Therapy. Biology 2023, 12, 347. https://doi.org/10.3390/biology12030347
Kapelouzou A, Geronikolou S, Lidoriki I, Kontogiannis C, Kaklamanis L, Tsourelis L, Cokkinos DV. Tissue and Serum Biomarkers in Degenerative Aortic Stenosis-Insights into Pathogenesis, Prevention and Therapy. Biology. 2023; 12(3):347. https://doi.org/10.3390/biology12030347
Chicago/Turabian StyleKapelouzou, Alkistis, Styliani Geronikolou, Irene Lidoriki, Christos Kontogiannis, Loukas Kaklamanis, Loukas Tsourelis, and Dennis V. Cokkinos. 2023. "Tissue and Serum Biomarkers in Degenerative Aortic Stenosis-Insights into Pathogenesis, Prevention and Therapy" Biology 12, no. 3: 347. https://doi.org/10.3390/biology12030347