
Use of Diltiazem in Chronic Rate Control for Atrial Fibrillation: A Prospective Case-Control Study
 , , ,
, , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Information
- -
- BB + NDCC: for patients with and without HF
- -
- BB + NDCC + digoxin: for patients with and without HF
- -
- NDCC: for patients with HF
- -
- NDCC + digoxin: for patients with HF
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Clinical Characteristics
3.1.1. Subgroup BB + NDCC (±Digoxin) (Sensitivity Analysis 1)
3.1.2. Subgroup NDCC (±Digoxin) in HF (Sensitivity Analysis 2)
3.1.3. Subgroup HF in PT (Sensitivity Analysis 3)
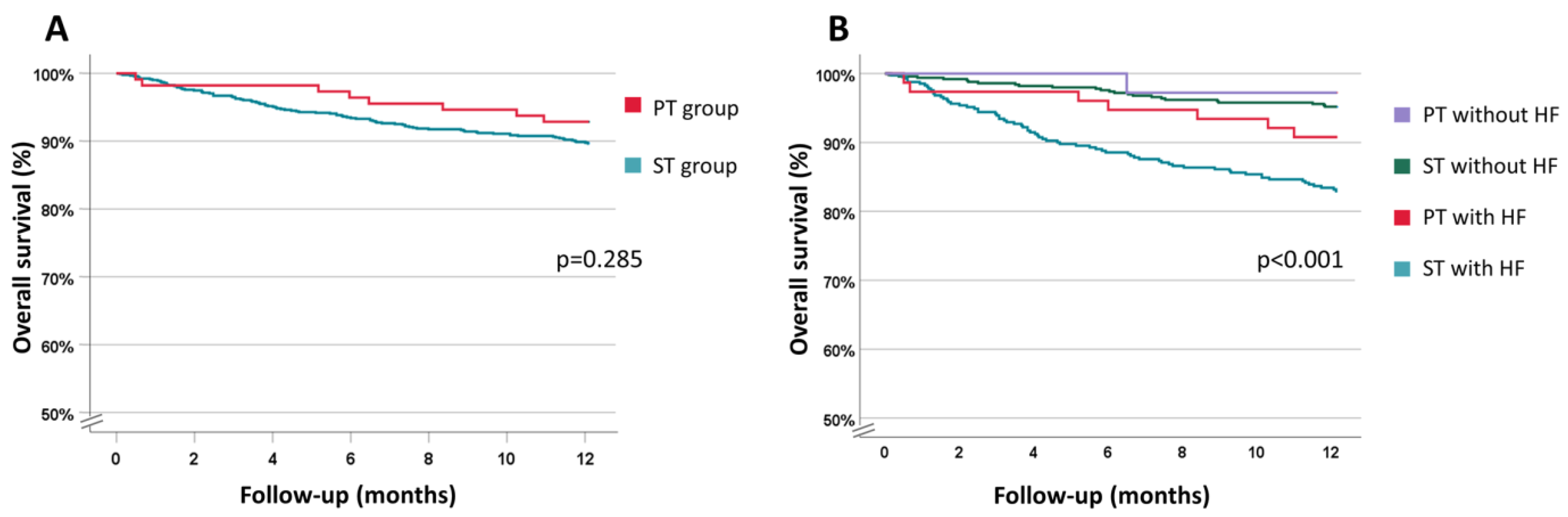
3.2. One-Year All-Cause Survival
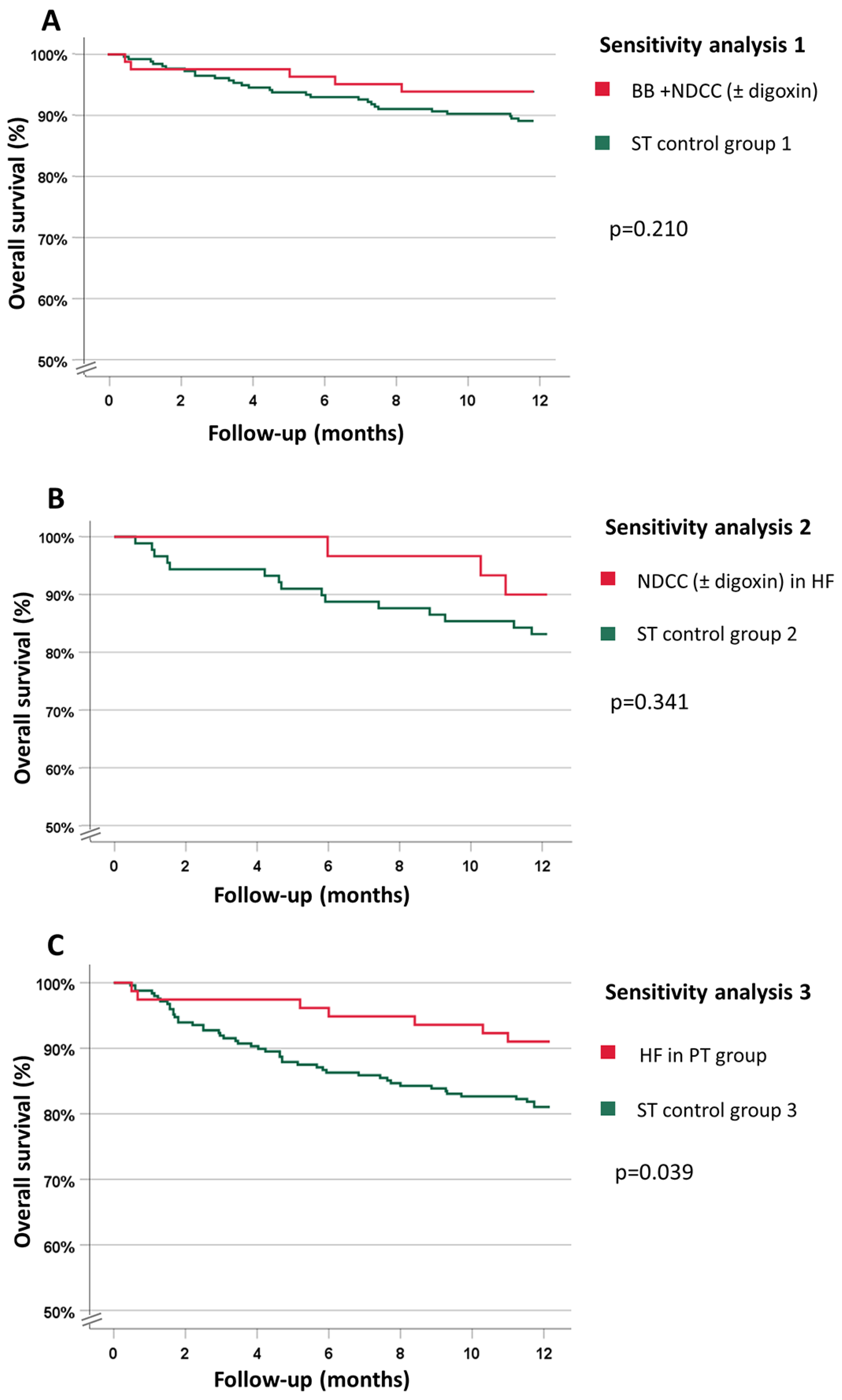
3.2.1. Subgroup BB + NDCC (±Digoxin) (Sensitivity Analysis 1)
3.2.2. Subgroup NDCC (±Digoxin) in HF (Sensitivity Analysis 2)
3.2.3. Subgroup HF in PT (Sensitivity Analysis 3)
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Krijthe, B.P.; Kunst, A.; Benjamin, E.J.; Lip, G.Y.H.; Franco, O.H.; Hofman, A.; Witteman, J.C.M.; Stricker, B.H.; Heeringa, J. Projections on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060. Eur. Heart J. 2013, 34, 2746–2751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Marrouche, N.F.; Brachmann, J.; Andresen, D.; Siebels, J.; Boersma, L.; Jordaens, L.; Merkely, B.; Pokushalov, E.; Sanders, P.; Proff, J.; et al. Catheter Ablation for Atrial Fibrillation with Heart Failure. N. Engl. J. Med. 2018, 378, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Kirchhof, P.; Camm, A.J.; Goette, A.; Brandes, A.; Eckardt, L.; Elvan, A.; Fetsch, T.; van Gelder, I.C.; Haase, D.; Haegeli, L.M.; et al. Early Rhythm-Control Therapy in Patients with Atrial Fibrillation. N. Engl. J. Med. 2020, 383, 1305–1316. [Google Scholar] [CrossRef] [PubMed]
- Wyse, D.G.; Waldo, A.L.; DiMarco, J.P.; Domanski, M.J.; Rosenberg, Y.; Schron, E.B.; Kellen, J.C.; Greene, H.L.; Mickel, M.C.; Dalquist, J.E.; et al. A comparison of rate control and rhythm control in patients with atrial fibrillation. N. Engl. J. Med. 2002, 347, 1825–1833. [Google Scholar] [PubMed]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.-C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camm, A.J.; Lip, G.Y.H.; De Caterina, R.; Savelieva, I.; Atar, D.; Hohnloser, S.H.; Hindricks, G.; Kirchhof, P.; ESC Committee for Practice Guidelines (CPG); Bax, J.J.; et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation. Eur. Heart J. 2012, 33, 2719–2747. [Google Scholar] [PubMed] [Green Version]
- Boriani, G.; Cimaglia, P.; Fantecchi, E.; Mantovani, V.; Ziacchi, M.; Valzania, C.; Martignani, C.; Biffi, M.; Diemberger, I. Non-valvular atrial fibrillation: Potential clinical implications of the heterogeneous definitions used in trials on new oral anticoagulants. J. Cardiovasc. Med. 2015, 16, 491–496. [Google Scholar] [CrossRef]
- Sara, J.D.; Toya, T.; Taher, R.; Lerman, A.; Gersh, B.; Anavekar, N.S. Asymptomatic Left Ventricle Systolic Dysfunction. Eur. Cardiol. Rev. 2020, 15, e13. [Google Scholar] [CrossRef]
- Iwagami, M.; Shinozaki, T. Introduction to Matching in Case-Control and Cohort Studies. Ann. Clin. Epidemiol. 2022, 4, 33–40. [Google Scholar] [CrossRef]
- Kwon, S.; Kim, T.J.; Choi, E.K.; Ahn, H.J.; Lee, E.; Lee, S.R.; Ko, S.B.; Oh, S.; Lip, G.Y.H. Predictors of ischemic stroke for low-risk patients with atrial fibrillation: A matched case-control study. Heart Rhythm. 2021, 18, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Dahlqvist, S.; Rosengren, A.; Gudbjornsdottir, S.; Pivodic, A.; Wedel, H.; Kosiborod, M.; Svensson, A.M.; Lind, M. Risk of atrial fibrillation in people with type 1 diabetes compared with matched controls from the general population: A prospective case-control study. Lancet Diabetes Endocrinol. 2017, 5, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Zaman, N.; Naccarelli, G.; Foy, A. A Comparison of Rate Control Agents for the Treatment of Atrial Fibrillation: Follow-Up Investigation of the AFFIRM Study. J. Cardiovasc. Pharmacol. Ther. 2021, 26, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Boriani, G.; Biffi, M.; Diemberger, I.; Martignani, C.; Branzi, A. Rate control in atrial fibrillation: Choice of treatment and assessment of efficacy. Drugs 2003, 63, 1489–1509. [Google Scholar] [CrossRef] [PubMed]
- Triska, J.; Tamargo, J.; Bozkurt, B.; Elkayam, U.; Taylor, A.; Birnbaum, Y. An Updated Review on the Role of Non-dihydropyridine Calcium Channel Blockers and Beta-blockers in Atrial Fibrillation and Acute Decompensated Heart Failure: Evidence and Gaps. Cardiovasc. Drugs Ther. 2022. [Google Scholar] [CrossRef]
- Horodinschi, R.N.; Diaconu, C.C. Comorbidities Associated with One-Year Mortality in Patients with Atrial Fibrillation and Heart Failure. Healthcare 2021, 9, 830. [Google Scholar] [CrossRef]
- McManus, D.D.; Rienstra, M.; Benjamin, E.J. An Update on the Prognosis of Patients With Atrial Fibrillation. Circulation 2012, 126, e143–e146. [Google Scholar] [CrossRef] [Green Version]
- Olshansky, B.; Rosenfeld, L.E.; Warner, A.L.; Solomon, A.J.; O'Neill, G.; Sharma, A.; Platia, E.; Feld, G.K.; Akiyama, T.; Brodsky, M.A.; et al. The Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) study. J. Am. Coll. Cardiol. 2004, 43, 1201–1208. [Google Scholar] [CrossRef] [Green Version]
- Van Gelder, I.C.; Groenveld, H.F.; Crijns, H.J.G.M.; Tuininga, Y.S.; Tijssen, J.G.P.; Alings, A.M.; Hillege, H.L.; Bergsma-Kadijk, J.A.; Cornel, J.H.; Kamp, O.; et al. Lenient versus Strict Rate Control in Patients with Atrial Fibrillation. N. Engl. J. Med. 2010, 362, 1363–1373. [Google Scholar] [CrossRef] [Green Version]
- Edoute, Y.; Nagachandran, P.; Svirski, B.; Ben-Ami, H. Cardiovascular adverse drug reaction associated with combined beta-adrenergic and calcium entry-blocking agents. J. Cardiovasc. Pharmacol. 2000, 35, 556–559. [Google Scholar] [CrossRef]
- Knight, C.J.; Fox, K.M. Amlodipine versus diltiazem as additional antianginal treatment to atenolol. Am. J. Cardiol. 1998, 81, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Alowais, S.A.; Hayes, B.D.; Wilcox, S.R.; Le, J.; Koehl, J.L.; Fuh, L. Heart rate outcomes with concomitant parenteral calcium channel blockers and beta blockers in rapid atrial fibrillation or flutter. Am. J. Emerg. Med. 2021, 44, 407–410. [Google Scholar] [CrossRef] [PubMed]
- Schwinger, R.H.; Böhm, M.; Erdmann, E. Different negative inotropic activity of Ca2+-antagonists in human myocardial tissue. Klin. Wochenschr. 1990, 68, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Heywood, J.T.; Graham, B.; Marais, G.E.; Jutzy, K.R. Effects of intravenous diltiazem on rapid atrial fibrillation accompanied by congestive heart failure. Am. J. Cardiol. 1991, 67, 1150–1152. [Google Scholar] [CrossRef] [PubMed]
- Kotecha, D.; Piccini, J.P. Atrial fibrillation in heart failure: What should we do? Eur. Heart J. 2015, 36, ehv513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldenberg, I.F.; Lewis, W.R.; Dias, V.C.; Heywood, J.T.; Pedersen, W.R. Intravenous diltiazem for the treatment of patients with atrial fibrillation or flutter and moderate to severe congestive heart failure. Am. J. Cardiol. 1994, 74, 884–889. [Google Scholar] [CrossRef]
- Hirschy, R.; Ackerbauer, K.A.; Peksa, G.D.; O'Donnell, E.P.; DeMott, J.M. Metoprolol vs. diltiazem in the acute management of atrial fibrillation in patients with heart failure with reduced ejection fraction. Am. J. Emerg. Med. 2019, 37, 80–84. [Google Scholar] [CrossRef] [Green Version]
- Multicenter Diltiazem Postinfarction Trial Research Group. The effect of diltiazem on mortality and reinfarction after myocardial infarction. N. Engl. J. Med. 1988, 319, 385–392. [Google Scholar] [CrossRef]
- Goldstein, R.E.; Boccuzzi, S.J.; Cruess, D.; Nattel, S. Diltiazem increases late-onset congestive heart failure in postinfarction patients with early reduction in ejection fraction. The Adverse Experience Committee; and the Multicenter Diltiazem Postinfarction Research Group. Circulation 1991, 83, 52–60. [Google Scholar] [CrossRef] [Green Version]
- Kostis, J.B.; Lacy, C.R.; Cosgrove, N.M.; Wilson, A.C. Association of calcium channel blocker use with increased rate of acute myocardial infarction in patients with left ventricular dysfunction. Am. Heart J. 1997, 133, 550–557. [Google Scholar] [CrossRef]
- Hager, W.D.; Davis, B.R.; Riba, A.; Moye, L.A.; Wun, C.C.; Rouleau, J.L.; Lamas, G.A.; Pfeffer, M.A. Absence of a deleterious effect of calcium channel blockers in patients with left ventricular dysfunction after myocardial infarction: The SAVE Study Experience. Am. Heart J. 1998, 135, 406–413. [Google Scholar] [CrossRef]
- Figulla, H.R.; Gietzen, F.; Zeymer, U.; Raiber, M.; Hegselmann, J.; Soballa, R.; Hilgers, R. Diltiazem improves cardiac function and exercise capacity in patients with idiopathic dilated cardiomyopathy. Results of the Diltiazem in Dilated Cardiomyopathy Trial. Circulation 1996, 94, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Kotecha, D.; Holmes, J.; Krum, H.; Altman, D.G.; Manzano, L.; Cleland, J.G.F.; Lip, G.Y.H.; Coats, A.J.S.; Andersson, B.; Kirchhof, P.; et al. Efficacy of β blockers in patients with heart failure plus atrial fibrillation: An individual-patient data meta-analysis. Lancet 2014, 384, 2235–2243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trongtorsak, A.; Kewcharoen, J.; Saowapa, S.; Polpichai, N.; Thangjui, S.; Navaravong, L. Comparison of mortality rates among rate-control agents in patients with atrial fibrillation: A systematic review and meta-analysis. J. Cardiovasc. Med. 2022, 23, e39–e41. [Google Scholar] [CrossRef] [PubMed]
- Paolillo, S.; Dell'Aversana, S.; Esposito, I.; Poccia, A.; Perrone Filardi, P. The use of beta-blockers in patients with heart failure and comorbidities: Doubts, certainties and unsolved issues. Eur. J. Intern. Med. 2021, 88, 9–14. [Google Scholar] [CrossRef]
- Bisson, A.; Ding, W.Y.; Bodin, A.; Lip, G.Y.H.; Fauchier, L. Clinical outcomes with digoxin vs. beta-blocker for heart rate control in permanent atrial fibrillation with heart failure. Eur. J. Heart Fail. 2021, 23, 1563–1565. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Standard Therapy (987 Patients) | Patient-Specific Therapy (125 Patients) | p-Value | |
|---|---|---|---|
| Age (years) | 73.5 ± 12.0 | 72.5 ± 12.7 | 0.366 |
| Male | 62.8% | 62.4% | 0.928 |
| BMI (kg/m2) | 26.5 ± 4.7 | 26.6 ± 4.9 | 0.794 |
| Systolic blood pressure (mmHg) | 125.4 ± 18.0 | 121.1 ± 16.3 | 0.012 |
| Hypertension | 73.2% | 72.0% | 0.771 |
| Diabetes | 21.7% | 28.0% | 0.110 |
| COPD | 17.6 | 21.6 | 0.28 |
| TIA | 5.8% | 4.0% | 0.411 |
| Ischemic stroke | 4.9% | 11.2% | 0.004 |
| Thromboembolic events | 4.1% | 8.8% | 0.017 |
| Major bleedings | 5.6% | 5.6% | 1.00 |
| Haemorrhagic stroke | 1.6% | 2.4% | 0.464 |
| Creatinine (mg/dL) | 1.2 ± 0.7 | 1.2 ± 0.5 | 0.532 |
| Ejection fraction (%) | 53.3 ± 15.0 | 53.0 ± 15.2 | 0.795 |
| NYHA class ≥ 2 | 41.3% | 64.8% | <0.001 |
| CAD | 38.5% | 35.2% | 0.477 |
| CHA2DS2-VASc score | 3.9 ± 1.8 | 4.1 ± 2.0 | 0.161 |
| CHA2DS2-VASc score ≥ 4 | 60.4% | 58.1% | 0.613 |
| HAS-BLED score | 2.0 ± 0.9 | 2.0 ± 1.0 | 0.351 |
| EHRA score | 1.8 ± 1.5 | 2.0 ± 1.4 | 0.348 |
| Coumadin | 70.3% | 82.4% | 0.005 |
| DOAC | 13% | 11.3% | 0.575 |
| Aspirin | 29.3% | 25.6% | 0.390 |
| ACE inhibitors or Sartans | 56.5% | 48.8% | 0.104 |
| BB | 70.8% | 74.4% | 0.399 |
| Digoxin | 9.9% | 17.6% | 0.009 |
| Diuretics | 72.2% | 88.0% | <0.001 |
| Aldosterone antagonists | 38.0% | 46.3% | 0.073 |
| NDCC | 5.3% | 100.0% | <0.001 |

| Sensitivity Analysis 1 | Sensitivity Analysis 2 | Sensitivity Analysis 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| BB + NDCC ±(Digoxin) (n° 93) | ST Control Group 1 (n° 79) | p-Value | NDCC (±Digoxin) in HF (n° 32) | ST Control Group 2 (n° 96) | p-Value | HF in PT Group(n° 85) | ST Control Group 3 (n° 255) | p-Value | |
| Age (years) | 72.8 ± 11.5 | 72.8 ± 11.7 | 1.000 | 71.8 ± 16.2 | 72.2 ± 12.9 | 0.877 | 72.0 ± 13.6 | 71.9 ± 12.0 | 0.978 |
| Male | 64.5% | 64.5% | 1.00 | 56.3% | 56.3% | 1.00 | 58.8% | 62.4% | 0.563 |
| BMI (kg/m2) | 27.1 ± 4.8 | 26.3 ± 4.4 | 0.109 | 25 ± 4.9 | 26.3 ± 5.0 | 0.224 | 26.8 ± 5.4 | 26.4 ± 4.7 | 0.444 |
| Systolic blood pressure (mmHg) | 122.0 ± 16.3 | 125.3 ± 18.2 | 0.119 | 118.6 ± 16.5 | 122.3 ± 19.3 | 0.334 | 118 ± 16.0 | 122 ± 19.5 | 0.128 |
| Hypertension | 72.0% | 70.6% | 0.792 | 71.9% | 69.8% | 0.823 | 69.4% | 70.2% | 0.891 |
| Diabetes | 29.0% | 23.3% | 0.267 | 25% | 25% | 1.00 | 31.8% | 29.4% | 0.682 |
| COPD | 19.4 | 18.3 | 0.82 | 28.1% | 24.0% | 0.637 | 25.9% | 23.5% | 0.661 |
| TIA | 4.3% | 4.3% | 1.00 | 3.1% | 8.3% | 0.318 | 3.5% | 5.1% | 0.554 |
| Ischemic stroke | 11.8% | 3.9% | 0.005 | 9.4 | 3.1 | 0.147 | 11.8% | 3.1% | <0.001 |
| Thromboembolic events | 9.7% | 4.3% | 0.052 | 6.3 | 5.2% | 0.822 | 9.4% | 5.9% | 0.262 |
| Major bleedings | 5.1% | 4.8% | 1.00 | 6.9% | 7.5% | 0.915 | 6.7% | 5.8% | 0.779 |
| Haemorrhagic stroke | 0% | 1.8% | 0.337 | 9.4 | 3.1 | 0.147 | 3.5% | 2.4% | 0.558 |
| Creatinine (mg/dL) | 1.2 ± 0.7 | 1.1 ± 0.5 | 0.074 | 1.27 ± 0.5 | 1.22 ± 0.5 | 0.627 | 1.2 ± 0.5 | 1.3 ± 0.8 | 0.171 |
| Ejection fraction (%) | 52.3 ± 15.5 | 52.4 ± 15.2 | 0.917 | 55.1 ± 14.4 | 53.1 ± 14.9 | 0.506 | 49.1 ± 16.0 | 47.3 ± 16.6 | 0.381 |
| NYHA ≥ 2 | 54.8% | 39.8% | 0.011 | 93.8% | 93.8% | 1.00 | 95.3% | 88.6% | 0.072 |
| CAD | 43.0% | 41.9% | 0.856 | 12.5% | 36.5% | 0.001 | 31.8% | 40.8% | 0.139 |
| CHA2DS2-VASc score | 4.1 ± 2.0 | 3.7 ± 1.8 | 0.114 | 4.3 ± 2.0 | 4.4 ± 1.7 | 0.665 | 4.6 ± 2.0 | 4.3 ± 1.8 | 0.354 |
| CHA2DS2-VASc score ≥4 | 57.0% | 55.4% | 0.794 | 65.6% | 75.0% | 0.303 | 65.5% | 69.8% | 0.458 |
| HAS-BLED score | 2.0 ± 0.9 | 2.0 ± 0.9 | 0.819 | 2.2 ± 1.0 | 2.0 ± 0.8 | 0.545 | 2.1 ± 1.0 | 2.1 ± 0.9 | 0.914 |
| EHRA score | 1.9 ± 1.6 | 2.1 ± 1.5 | 0.824 | 1.6 ± 1.2 | 1.8 ± 1.5 | 0.576 | 1.9 ± 1.5 | 1.8 ± 1.5 | 0.633 |
| Coumadin | 82.8% | 71.0% | 0.024 | 81.3% | 87.5% | 0.378 | 78.8% | 85.1% | 0.177 |
| DOAC | 12.9% | 12.3% | 0.835 | 9.3% | 5.2% | 0.500 | 15.3% | 9.8% | 0.250 |
| Aspirin | 29.0% | 31.2% | 0.697 | 15.6% | 25% | 0.273 | 18.8% | 25.5% | 0.211 |
| ACE inhibitors or Sartans | 49.5% | 60.9% | 0.052 | 46.9% | 49.05 | 0.838 | 49.4% | 53.3% | 0.531 |
| BB | 100% | 74.2% | <0.001 | 0% | 71.9% | <0.001 | 62.4% | 76.9% | 0.009 |
| Digoxin | 10.8% | 10.8% | 1.00 | 37.5% | 37.5% | 1.00 | 23.5% | 23.1% | 0.941 |
| Diuretics | 84.9% | 74.2% | 0.033 | 96.9% | 90.6% | 0.254 | 95.3% | 92.9% | 0.445 |
| Aldosterone antagonists | 47.3% | 39.1% | 0.168 | 43.8% | 50% | 0.543 | 48.8% | 55.3% | 0.301 |
| NDCC | 100% | 5.4% | <0.001 | 100% | 0% | <0.001 | 100.0% | 0% | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diemberger, I.; Spadotto, A.; Massaro, G.; Amadori, M.; Damaschin, L.; Martignani, C.; Ziacchi, M.; Biffi, M.; Galiè, N.; Boriani, G. Use of Diltiazem in Chronic Rate Control for Atrial Fibrillation: A Prospective Case-Control Study. Biology 2023, 12, 22. https://doi.org/10.3390/biology12010022
Diemberger I, Spadotto A, Massaro G, Amadori M, Damaschin L, Martignani C, Ziacchi M, Biffi M, Galiè N, Boriani G. Use of Diltiazem in Chronic Rate Control for Atrial Fibrillation: A Prospective Case-Control Study. Biology. 2023; 12(1):22. https://doi.org/10.3390/biology12010022
Chicago/Turabian StyleDiemberger, Igor, Alberto Spadotto, Giulia Massaro, Martina Amadori, Liviu Damaschin, Cristian Martignani, Matteo Ziacchi, Mauro Biffi, Nazzareno Galiè, and Giuseppe Boriani. 2023. "Use of Diltiazem in Chronic Rate Control for Atrial Fibrillation: A Prospective Case-Control Study" Biology 12, no. 1: 22. https://doi.org/10.3390/biology12010022