
Non-Isolated Neural Tube Defects with Comorbid Malformations Are Responsive to Population-Level Folic Acid Supplementation in Northern China
 , , , , , and
, , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Study Design
2.1. Birth Defects Surveillance
2.2. Case Classification
3. Statistical Analysis
4. Results
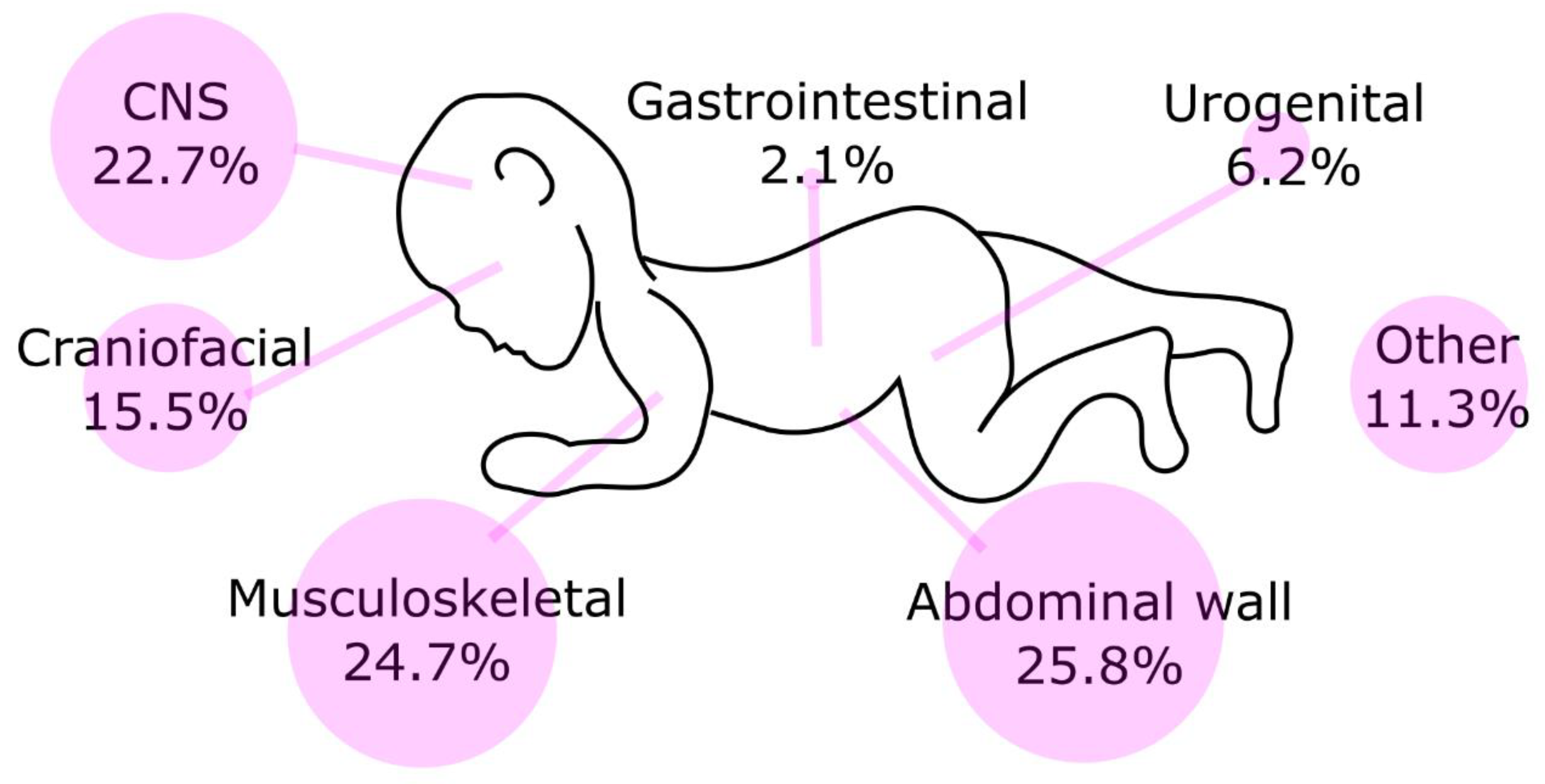
4.1. The Prevalence, Types and Proportion of Defects Co-Occurring with NTDs
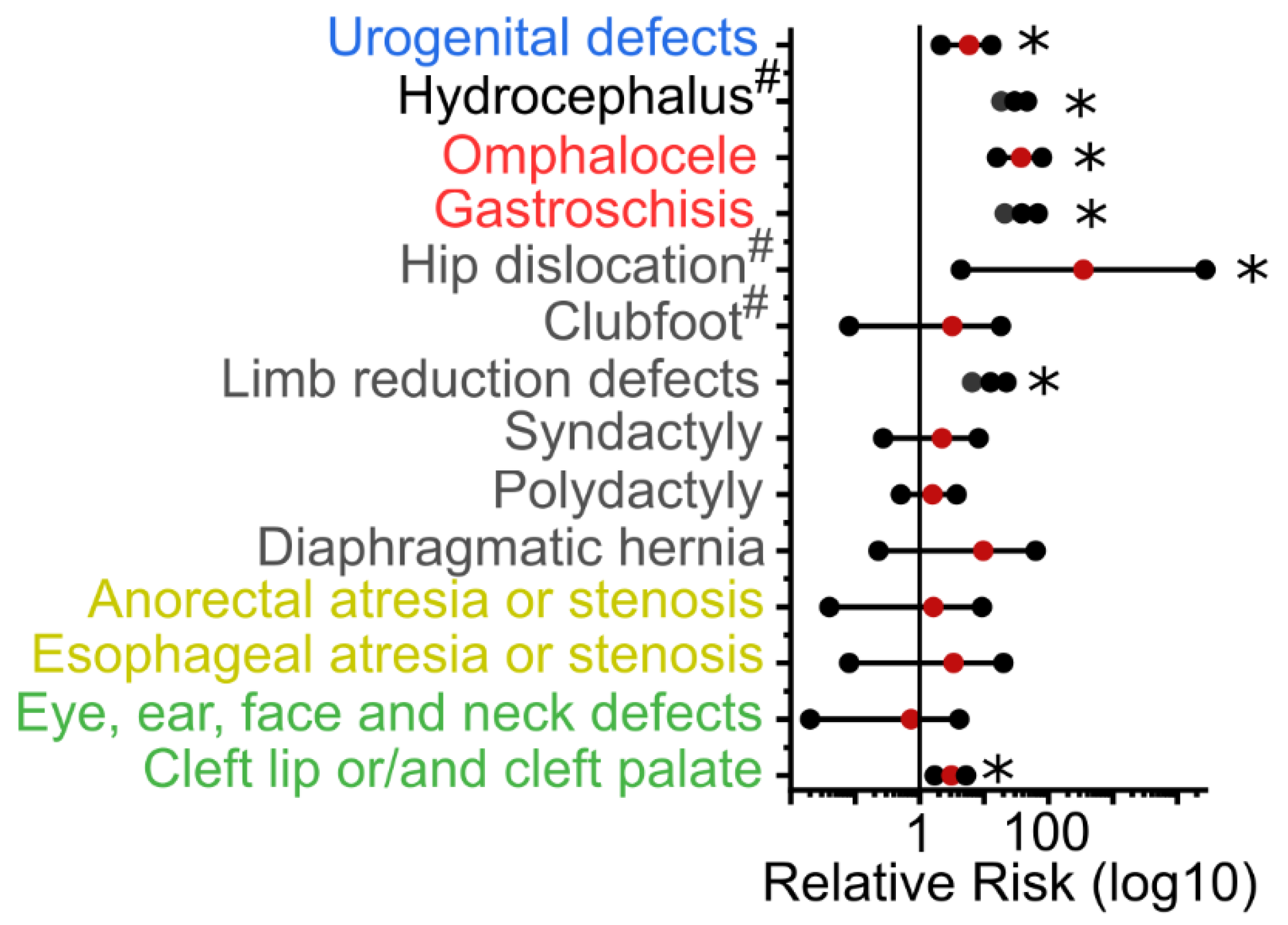
4.2. Comorbid Malformations Over-Represented in Individuals with NTDs
4.3. Epidemiological Characteristics of Isolated and Non-Isolated NTD Cases
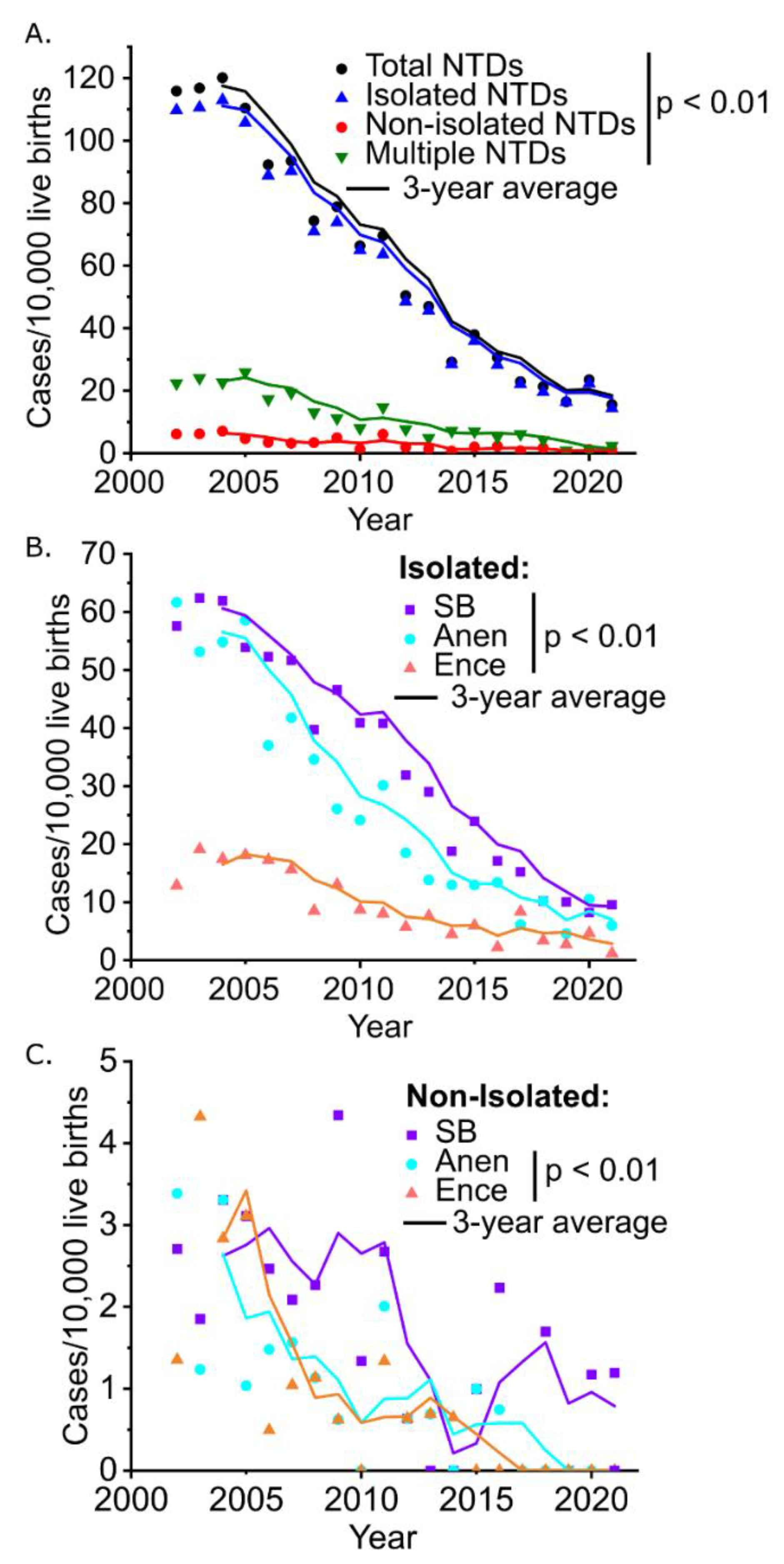
4.4. Temporal Trends in the Prevalence of NTDs
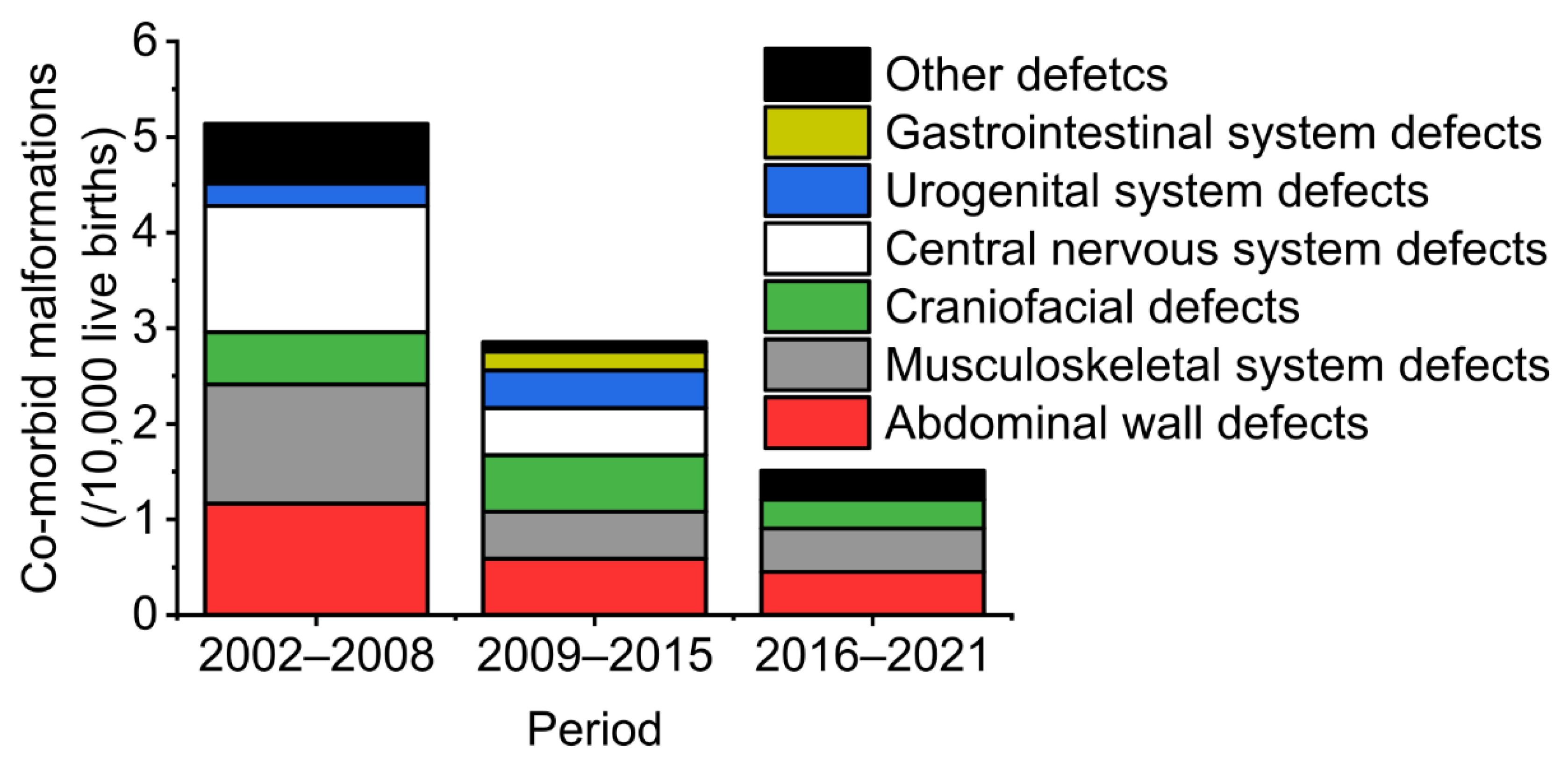
4.5. Prevalence of Isolated and Non-isolated NTDs before and after National Folic Acid Supplementation
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zaganjor, I.; Sekkarie, A.; Tsang, B.L.; Williams, J.; Razzaghi, H.; Mulinare, J.; Sniezek, J.E.; Cannon, M.J.; Rosenthal, J. Describing the prevalence of neural tube defects worldwide: A systematic literature review. PLoS ONE 2016, 11, e0151586. [Google Scholar] [CrossRef]
- Rolo, A.; Galea, G.L.; Savery, D.; Greene, N.D.; Copp, A.J. Novel mouse model of encephalocele: Post-neurulation origin and relationship to open neural tube defects. Dis. Models Mech. 2019, 12, dmm040683. [Google Scholar] [CrossRef]
- Juranek, J.; Salman, M.S. Anomalous development of brain structure and function in spina bifida myelomeningocele. Dev. Disabil. Res. Rev. 2010, 16, 23–30. [Google Scholar] [CrossRef]
- Oliver, E.; Heuer, G.; Thom, E.A.; Burrows, P.K.; Didier, R.; DeBari, S.; Martin-Saavedra, J.; Moldenhauer, J.; Jatres, J.; Howell, L. Myelomeningocele sac associated with worse lower-extremity neurological sequelae: Evidence for prenatal neural stretch injury? Ultrasound Obstet. Gynecol. 2020, 55, 740–746. [Google Scholar] [CrossRef]
- Viehweger, E.; Kläusler, M.; Loucheur, N. Paralytic dislocation of the hip in children. Orthop. Traumatol. Surg. Res. 2021, 108, 103166. [Google Scholar] [CrossRef]
- Murdoch, J.N.; Damrau, C.; Paudyal, A.; Bogani, D.; Wells, S.; Greene, N.D.; Stanier, P.; Copp, A.J. Genetic interactions between planar cell polarity genes cause diverse neural tube defects in mice. Dis. Models Mech. 2014, 7, 1153–1163. [Google Scholar]
- Wang, B.; Sinha, T.; Jiao, K.; Serra, R.; Wang, J. Disruption of PCP signaling causes limb morphogenesis and skeletal defects and may underlie Robinow syndrome and brachydactyly type B. Hum. Mol. Genet. 2011, 20, 271–285. [Google Scholar] [CrossRef]
- Molè, M.A.; Galea, G.L.; Rolo, A.; Weberling, A.; Nychyk, O.; De Castro, S.C.; Savery, D.; Fässler, R.; Ybot-González, P.; Greene, N.D.; et al. Integrin-mediated focal anchorage drives epithelial zippering during mouse neural tube closure. Dev. Cell 2020, 52, 321–334.e6. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, L.; Li, Z.; Jin, L.; Zhang, Y.; Ye, R.; Liu, J.; Ren, A. Prevalence and trend of neural tube defects in five counties in Shanxi province of Northern China, 2000 to 2014. Birth Defects Res. Part A Clin. Mol. Teratol. 2016, 106, 267–274. [Google Scholar] [CrossRef]
- Adzick, N.S.; Thom, E.A.; Spong, C.Y.; Brock, J.W., III; Burrows, P.K.; Johnson, M.P.; Howell, L.J.; Farrell, J.A.; Dabrowiak, M.E.; Sutton, L.N.; et al. A randomized trial of prenatal versus postnatal repair of myelomeningocele. New Engl. J. Med. 2011, 364, 993–1004. [Google Scholar] [CrossRef]
- Ravindra, V.M.; Aldave, G.; Weiner, H.L.; Lee, T.; Belfort, M.A.; Sanz-Cortes, M.; Espinoza, J.; Shamshirsaz, A.A.; Nassr, A.A.; Whitehead, W.E. Prenatal counseling for myelomeningocele in the era of fetal surgery: A shared decision-making approach. J. Neurosurg. Pediatrics. 2020, 25, 640–647. [Google Scholar] [CrossRef]
- Botto, L.D.; Olney, R.S.; Erickson, J.D. Vitamin supplements and the risk for congenital anomalies other than neural tube defects. Am. J. Med. Genet. C Semin. Med. Genet. 2004, 125, 12–21. [Google Scholar] [CrossRef]
- Marean, A.; Graf, A.; Zhang, Y.; Niswander, L. Folic acid supplementation can adversely affect murine neural tube closure and embryonic survival. Hum. Mol. Genet. 2011, 20, 3678–3683. [Google Scholar] [CrossRef]
- Barisic, I.; Boban, L.; Loane, M.; Garne, E.; Wellesley, D.; Calzolari, E.; Dolk, H.; Addor, M.-C.; Bergman, J.E.H.; Braz, P.; et al. Meckel–Gruber Syndrome: A population-based study on prevalence, prenatal diagnosis, clinical features, and survival in Europe. Eur. J. Hum. Genet. 2015, 23, 746–752. [Google Scholar] [CrossRef]
- Group, E.W. Prevalence of neural tube defects in 20 regions of Europe and the impact of prenatal diagnosis, 1980–1986. J. Epidemiol. Community Health 1991, 45, 52–58. [Google Scholar]
- Stevenson, R.E.; Seaver, L.H.; Collins, J.S.; Dean, J.H. Neural tube defects and associated anomalies in South Carolina. Birth Defects Res. Part A Clin. Mol. Teratol. 2004, 70, 554–558. [Google Scholar] [CrossRef]
- Stoll, C.; Dott, B.; Alembik, Y.; Roth, M.P. Associated malformations among infants with neural tube defects. Am. J. Med. Genet. Part A 2011, 155, 565–568. [Google Scholar] [CrossRef]
- McDonnell, R.; Johnson, Z.; Delaney, V.; Dack, P. East Ireland 1980–1994: Epidemiology of neural tube defects. J. Epidemiol. Community Health 1999, 53, 782–788. [Google Scholar] [CrossRef]
- Källén, B.; Robert, E.; Harris, J. Associated malformations in infants and fetuses with upper or lower neural tube defects. Teratology 1998, 57, 56–63. [Google Scholar] [CrossRef]
- Moradi, B.; Shakki Katouli, F.; Gity, M.; Kazemi, M.A.; Shakiba, M.; Fattahi Masrour, F. Neural tube defects: Distribution and associated anomalies diagnosed by prenatal ultrasonography in Iranian fetuses. J. Obstet. Gynecol. Cancer Res. 2017, 2, e64382. [Google Scholar] [CrossRef]
- Yuanyuan, W.; Lei, J.; Jufen, L.; Yali, Z.; Zhiwen, L.; Aiguo, R. Comparative analysis of pathological anatomy results and clinical reports of neural tube defects. Chin. J. Reprod. Health 2015, 26, 207–210. [Google Scholar]
- Liu, J.; Wang, L.; Zhang, Y.; Zhang, L.; Jin, L.; Li, Z.; Ren, A. Selected Structural Birth Defects—Shanxi Province, China, 2000–2019. China CDC Wkly. 2020, 2, 718. [Google Scholar] [CrossRef] [PubMed]
- Czeizel, A.; Opitz, J.M. Schisis-association. Am. J. Med. Genet. 1981, 10, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Opitz, J.M.; Gilbert, E.F. CNS anomalies and the midline as a “developmental field”. Am. J. Med. Genet. 1982, 12, 443–455. [Google Scholar] [CrossRef]
- Greene, N.D.; Massa, V.; Copp, A.J. Understanding the causes and prevention of neural tube defects: Insights from the splotch mouse model. Birth Defects Res. Part A Clin. Mol. Teratol. 2009, 85, 322–330. [Google Scholar] [CrossRef]
- Zhou, Y.; Crider, K.S.; Yeung, L.F.; Rose, C.E.; Li, Z.; Berry, R.J.; Li, S.; Moore, C.A. Periconceptional folic acid use prevents both rare and common neural tube defects in China. Birth Defects Res. 2022, 114, 184–196. [Google Scholar] [CrossRef]
- Liu, J.; Li, Z.; Ye, R.; Ren, A.; Liu, J. Folic acid supplementation and risk for congenital limb reduction defects in China. Int. J. Epidemiol. 2019, 48, 2010–2017. [Google Scholar] [CrossRef]
- López-Camelo, J.S.; Castilla, E.E.; Orioli, I.M. Folic acid flour fortification: Impact on the frequencies of 52 congenital anomaly types in three South American countries. Am. J. Med. Genet. Part A 2010, 152, 2444–2458. [Google Scholar] [CrossRef]
- Collins, J.S.; Atkinson, K.K.; Dean, J.H.; Best, R.G.; Stevenson, R.E. Long term maintenance of neural tube defects prevention in a high prevalence state. J. Pediatrics 2011, 159, 143–149.e2. [Google Scholar] [CrossRef]
- Khoury, M.J.; Erickson, J.D.; James, L.M. Etiologic heterogeneity of neural tube defects: Clues from epidemiology. Am. J. Epidemiol. 1982, 115, 538–548. [Google Scholar] [CrossRef]
- Krantz, D.A.; Hallahan, T.W.; Carmichael, J.B. Screening for open neural tube defects. Clin. Lab. Med. 2016, 36, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Erol, S.A.; Tanacan, A.; Oguz, E.F.; Anuk, A.T.; Ayhan, S.G.; Neselioglu, S.; Sahin, D. A comparison of the maternal levels of serum proprotein convertase subtilisin/kexin type 9 in pregnant women with the complication of fetal open neural tube defects. Congenit. Anom. 2021, 61, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Song, L.; Qiu, J.; Jing, W.; Wang, L.; Dai, Y.; Qin, G.; Liu, M. Reducing maternal mortality in China in the era of the two-child policy. BMJ Glob. Health 2020, 5, e002157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berihu, B.A.; Welderufael, A.L.; Berhe, Y.; Magana, T.; Mulugeta, A.; Asfaw, S.; Gebreselassie, K. Maternal risk factors associated with neural tube defects in Tigray regional state of Ethiopia. Brain Dev. 2019, 41, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Evans, J.; Macfarlane, A.J.; Ananth, C.V.; Little, J.; Kramer, M.S.; Joseph, K. Association of maternal risk factors with the recent rise of neural tube defects in Canada. Paediatr. Perinat. Epidemiol. 2019, 33, 145–153. [Google Scholar] [CrossRef]
- Li, Z.; Ren, A.; Zhang, L.; Ye, R.; Li, S.; Zheng, J.; Hong, S.; Wang, T.; Li, Z. Extremely high prevalence of neural tube defects in a 4-county area in Shanxi Province, China. Birth Defects Res. Part A Clin. Mol. Teratol. 2006, 76, 237–240. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Birth Defects | Spina Bifida (n = 1175) | Anencephaly (n = 916) | Encephalocele (n = 339) | All NTDs (n = 2031) | Non-NTDs (n = 294,275) |
|---|---|---|---|---|---|
| Craniofacial defects | |||||
| Cleft lip or/and cleft palate | 9 † | 5 | 3 & | 14 ※ | 650 †&※ |
| Eye, ear, face and neck defects | 1 | 0 | 0 | 1 | 199 |
| Gastrointestinal system defects | |||||
| Esophageal atresia or stenosis | 1 | 0 | 0 | 1 | 43 |
| Anorectal atresia or stenosis | 1 | 0 | 0 | 1 | 89 |
| Musculoskeletal system defects | |||||
| Diaphragmatic hernia | 1 | 1 # | 0 | 1 | 15 # |
| Polydactyly | 3 | 0 | 4 ∮ | 5 | 459 ∮ |
| Syndactyly | 2 | 0 | 0 | 2 | 131 |
| Limb reduction defects | 12 † | 4 ‡ | 0 | 13 ※ | 150 †‡※ |
| Clubfoot * | / | 0 | 1 | 1 | 107 |
| Hip dislocation * | / | 0 | 1 ∮ | 1 ※ | 1 ∮※ |
| Abdominal wall defects | |||||
| Gastroschisis | 13 † | 9 ‡ | 0 | 16 ※ | 60 †‡※ |
| Omphalocele | 7 † | 4 ‡ | 0 | 9 ※ | 35 †‡※ |
| Central nervous system defects | |||||
| Hydrocephalus * | / | 3 # | 19 ∮ | 22 ※ | 253 #∮※ |
| Urogenital system defects | 5 † | 1 | 0 | 6 ※ | 149 †※ |
| Characteristics | Isolated NTDs (n = 1934) | Non-Isolated NTDs (n = 97) | χ2 | P | |
|---|---|---|---|---|---|
| Residence | Rural | 1694 (87.6) | 83 (85.6) | 0.346 | 0.556 |
| Urban | 240 (12.4) | 14 (14.4) | |||
| Infant Sex | Male | 865 (44.7) | 40(41.2) | 0.021 | 0.885 |
| Female | 1027 (53.1) | 46 (47.4) | |||
| Unknown | 42 (2.2) | 11 (11.3) | |||
| Gestational weeks | <28w | 1260 (65.1) | 61 (62.9) | 0.208 | 0.648 |
| ≥28w | 674 (34.9) | 36 (37.1) | |||
| NTDs by type | Anencephaly | 585 (30.2) | 13 (13.4) | 34.068 | <0.01 |
| Spina bifida | 787 (40.7) | 35 (36.1) | |||
| Encephalocele | 206 (10.7) | 27 (27.8) | |||
| Multiple NTDs | 356 (18.4) | 22 (22.7) | |||
| Delivery time | Before 2009 | 1262 (65.3) | 62 (63.9) | 0.073 | 0.787 |
| After 2009 | 672 (34.7) | 35 (36.1) | |||
| Type of NTD | Folic Acid Supplementation | χ2 | p | ||
|---|---|---|---|---|---|
| Before (n = 128,477) | After (n = 167,829) | ||||
| Total NTD | Isolated | 1262 (98.2) | 672 (40.0) | 379.954 | <0.01 |
| Non-isolated | 62 (4.8) | 35 (2.1) | 16.698 | <0.01 | |
| Spina bifida | Isolated | 696 (54.2) | 423 (25.2) | 162.319 | <0.01 |
| Non-isolated | 33 (2.6) | 23 (1.4) | 5.528 | 0.019 | |
| Anencephaly | Isolated | 633 (49.3) | 262 (15.6) | 273.760 | <0.01 |
| Non-isolated | 24 (1.9) | 8 (0.5) | 13.046 | <0.01 | |
| Encephalocele | Isolated | 202 (15.7) | 105 (6.3) | 63.003 | <0.01 |
| Non-isolated | 26 (2.0) | 6 (0.4) | 18.709 | <0.01 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Che, X.; Liu, J.; Galea, G.L.; Zhang, Y.; Greene, N.D.E.; Zhang, L.; Jin, L.; Wang, L.; Ren, A.; Li, Z. Non-Isolated Neural Tube Defects with Comorbid Malformations Are Responsive to Population-Level Folic Acid Supplementation in Northern China. Biology 2022, 11, 1371. https://doi.org/10.3390/biology11091371
Che X, Liu J, Galea GL, Zhang Y, Greene NDE, Zhang L, Jin L, Wang L, Ren A, Li Z. Non-Isolated Neural Tube Defects with Comorbid Malformations Are Responsive to Population-Level Folic Acid Supplementation in Northern China. Biology. 2022; 11(9):1371. https://doi.org/10.3390/biology11091371
Chicago/Turabian StyleChe, Xiaoyu, Jufen Liu, Gabriel L Galea, Yali Zhang, Nicholas D. E. Greene, Le Zhang, Lei Jin, Linlin Wang, Aiguo Ren, and Zhiwen Li. 2022. "Non-Isolated Neural Tube Defects with Comorbid Malformations Are Responsive to Population-Level Folic Acid Supplementation in Northern China" Biology 11, no. 9: 1371. https://doi.org/10.3390/biology11091371