
The Impact of Corticosteroid Administration at Different Time Points on Mucosal Wound Healing in Rats: An Experimental Pilot In Vivo Study

 , ,
, ,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals and Preparation of Experimental Model
2.2. Steroid Administration
- -
- Five bottles of 1 mL each with a concentration of 10 mg/mL were used.
- -
- 0.5 mL was aspirated from each bottle and diluted with 4.5 mL saline.
- -
- Of the solution, 1 mg/kg was injected subcutaneously into the abdominal wall.
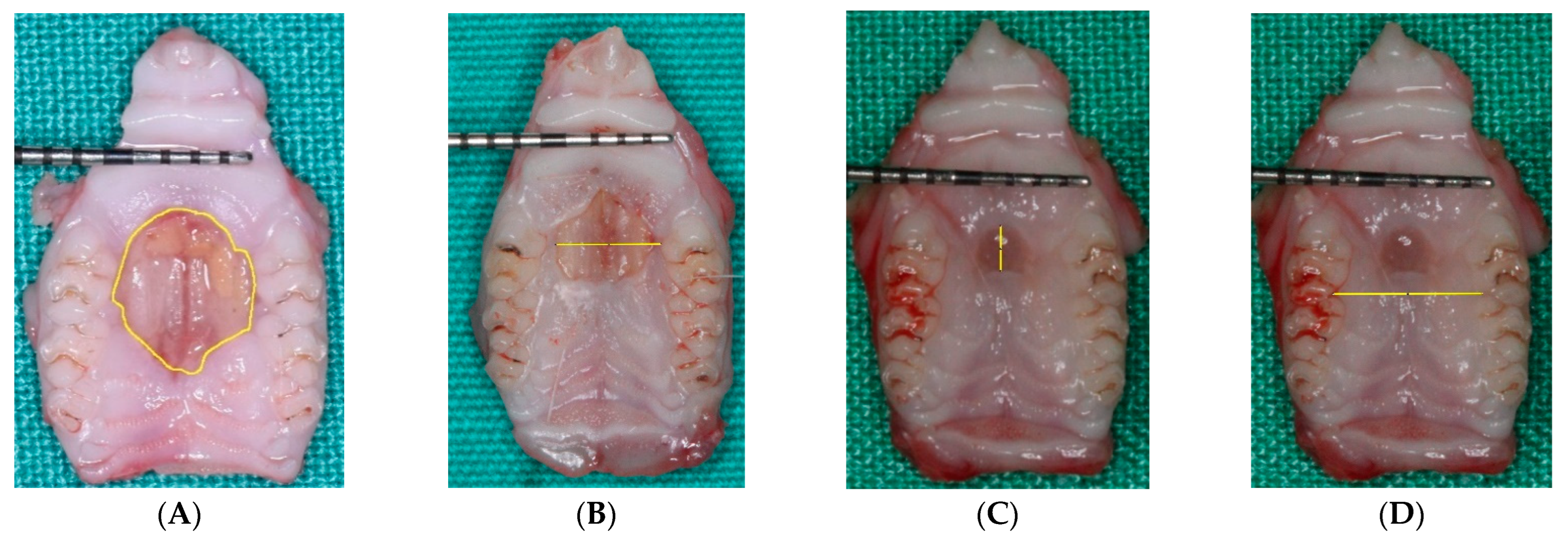
2.3. Macroscopic Evaluation
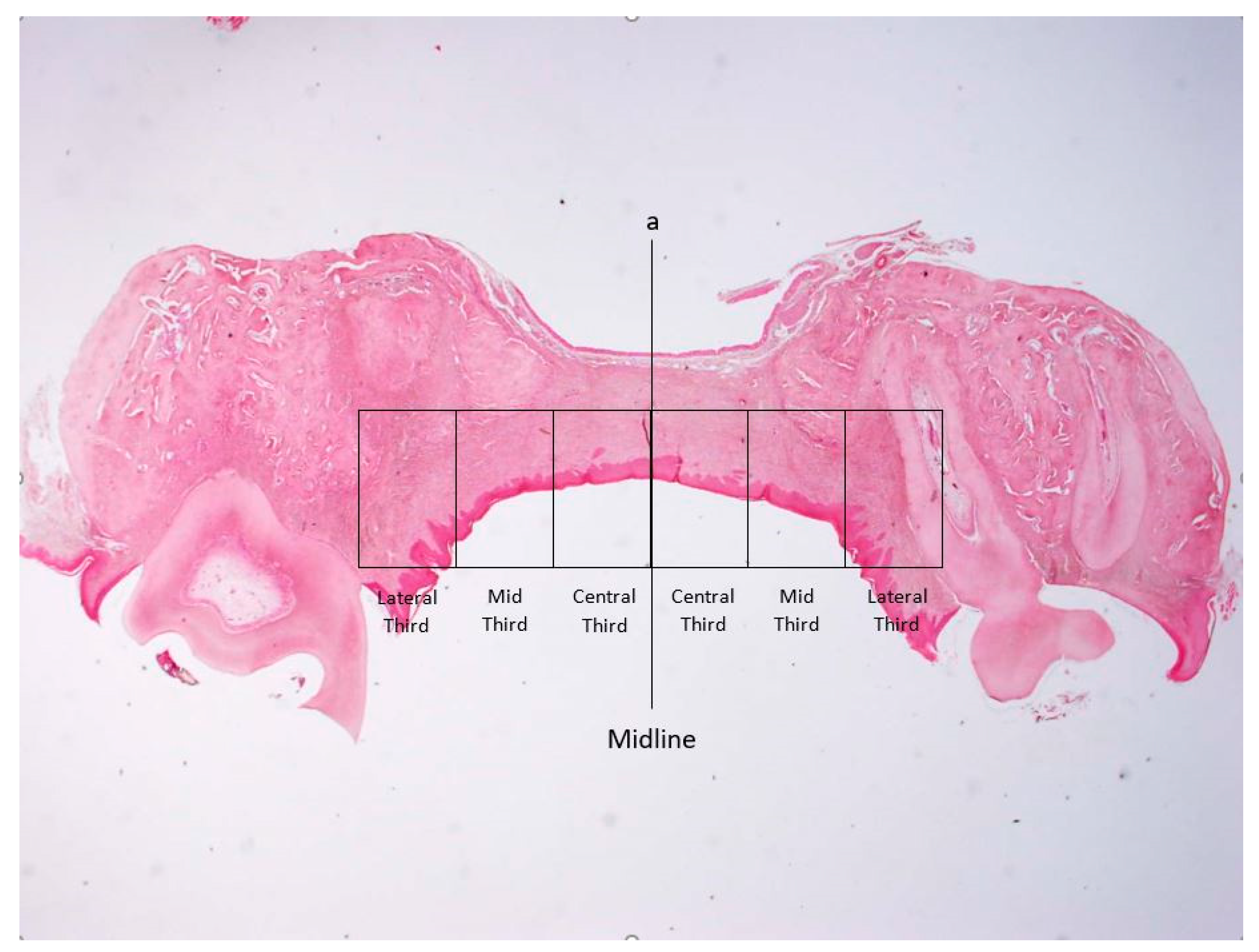
2.4. Microscopic Examination
2.5. Histomorphometry for Assessment of the Intensity of Inflammation
2.6. Statistical Analysis
3. Results
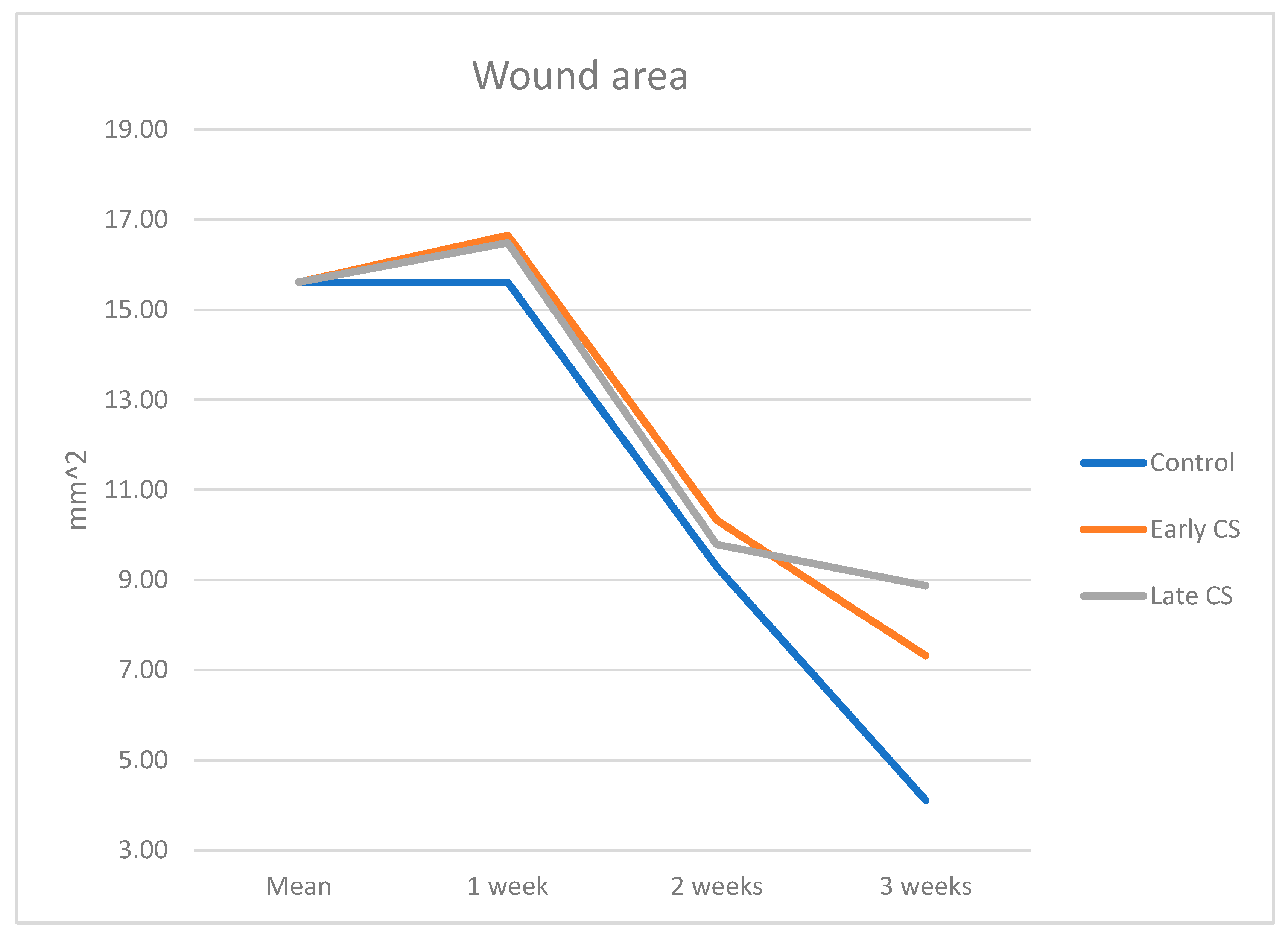
3.1. Macroscopic Evaluation
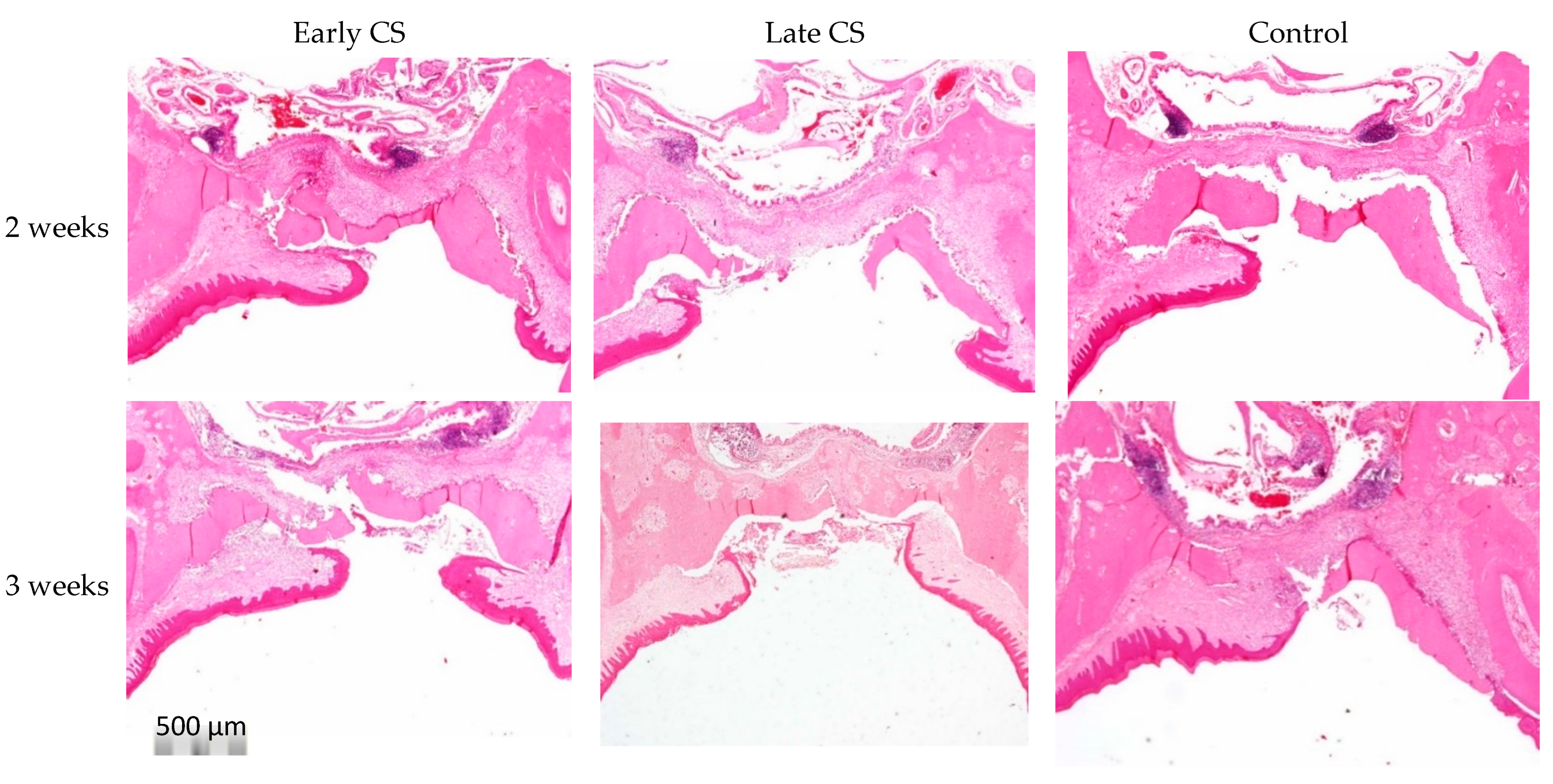
3.2. Microscopic Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Malpartida-Carrillo, V.; Tinedo-Lopez, P.; Guerrero, M.E.; Huamani-Echaccaya, J.L.; Özcan, M.; Rösing, C.K. Outcome measurements following palatal soft tissue graft harvesting: A review. J. Clin. Exp. Dent. 2021, 13, e527–e535. [Google Scholar] [CrossRef]
- Maino, G.N.E.; Valles, C.; Santos, A.; Pascual, A.; Esquinas, C.; Nart, J. Influence of suturing technique on wound healing and patient morbidity after connective tissue harvesting. A randomized clinical trial. J. Clin. Periodontol. 2018, 45, 977–985. [Google Scholar] [CrossRef]
- Carvajal Monroy, P.L.; Grefte, S.; Kuijpers-Jagtman, A.M.; Helmich, M.P.; Wagener, F.A.; Von den Hoff, J.W. Fibrosis impairs the formation of new myofibers in the soft palate after injury. Wound Repair Regen. 2015, 23, 866–873. [Google Scholar] [CrossRef]
- Chaushu, L.; Atzil, S.; Vered, M.; Chaushu, G.; Matalon, S.; Weinberg, E. Age-Related Palatal Wound Healing: An Experimental In Vivo Study. Biology 2021, 10, 240. [Google Scholar] [CrossRef]
- Alışır, M.; Akpınar, A.; Talmaç, A.C.; Lektemur Alpan, A.; Göze, Ö.F. Humic Acid Enhances Wound Healing in the Rat Palate. Evid. Based Complement. Altern. Med. 2018, 2018, 1783513. [Google Scholar]
- Chaushu, L.; Rahmanov, G.M.; Chaushu, G.; Zar, K.; Vered, M. Curcumin Promotes Primary Oral Wound Healing in a Rat Model. J. Med. Food 2021, 24, 422–430. [Google Scholar] [CrossRef]
- Taskan, M.M.; Balci, Y.H.; Karatas, O.; Gevrek, F.; Isiker Kara, G.; Celt, M.; Sirma Taskan, E. Hyaluronic acid with antioxidants improve wound healing in rats. Biotech. Histochem. 2020, 13, 536–545. [Google Scholar] [CrossRef]
- Chaushu, L.; Rahmanov, G.M.; Chaushu, G.; Zar, K.; Vered, M. Orabase Promotes Oral Epithelization in a Wound Healing Rat Model: An Immunohistochemical Study. Appl. Immunohistochem. Mol. Morphol. 2021, 29, e39–e45. [Google Scholar] [CrossRef]
- Kozlovsky, A.; Artzi, Z.; Hirshberg, A.; Israeli-Tobias, C.; Reich, L. Effect of local antimicrobial agents on excisional palatal wound healing: A clinical and histomorphometric study in rats. J. Clin. Periodontol. 2007, 34, 164–171. [Google Scholar] [CrossRef]
- Kim, Y.J.; Carvalho, F.C.; Souza, J.A.; Gonçalves, P.C.; Nogueira, A.V.; Spolidório, L.C.; Roque-Barreira, M.C.; Cirelli, J.A. Topical application of the lectin Artin M accelerates wound healing in rat oral mucosa by enhancing TGF-beta and VEGF production. Wound Repair Regen. 2013, 21, 456–463. [Google Scholar] [CrossRef]
- Butcher, E.O.; Klingsberg, J. Age, gonadectomy, and wound healing in the palatal mucosa of the rat. Oral Surg. Oral Med. Oral Pathol. 1963, 16, 484–493. [Google Scholar] [CrossRef]
- Engeland, C.G.; Bosch, J.A.; Cacioppo, J.T.; Marucha, P.T. Mucosal wound healing: The roles of age and sex. Arch. Surg. 2006, 141, 1193–1197. [Google Scholar] [CrossRef] [PubMed]
- Engeland, C.G.; Sabzehei, B.; Marucha, P.T. Sex hormones and mucosal wound healing. Brain Behav. Immun. 2009, 23, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Dhungel, S.; Bhattarai, K.; Roychoudhury, A. Do the benefits of systemic corticosteroids outweigh adverse effects during maxillofacial trauma surgery? A systematic review and meta-analysis. J. Oral Maxillofac. Surg. 2021, 79, 1530.e1–1530.e21. [Google Scholar] [CrossRef]
- Anstead, G.M. Steroids, retinoids, and wound healing. Adv. Wound Care 1998, 11, 277–285. [Google Scholar]
- Schacke, H.; Docke, W.D.; Asadullah, K. Mechanisms involved in the side effects of glucocorticoids. Pharmacol. Ther. 2002, 96, 23–43. [Google Scholar] [CrossRef]
- Martin, P. Wound healing—Aiming for perfect skin regeneration. Science 1997, 276, 75–81. [Google Scholar] [CrossRef]
- Hübner, G.; Brauchle, M.; Smola, H.; Madlener, M.; Fässler, R.; Werner, S. Differential regulation of proinflammatory cytokines during wound healing in normal and glucocorticoid-treated mice. Cytokine 1996, 8, 548–556. [Google Scholar] [CrossRef]
- Polat, A.; Nayci, A.; Polat, G.; Aksöyek, S. Dexamethasone down-regulates endothelial expression of intercellular adhesion molecule and impairs the healing of bowel anastomoses. Eur. J. Surg. 2002, 168, 500–506. [Google Scholar] [CrossRef]
- Leibovich, S.J.; Ross, R. The role of the macrophage in wound repair. A study with hydrocortisone and antimacrophage serum. Am. J. Pathol. 1975, 78, 71–100. [Google Scholar]
- Brauchle, M.; Fassler, R.; Werner, S. Suppression of keratinocyte growth factor expression by glucocorticoids in vitro and during wound healing. J. Investig. Dermatol. 1995, 105, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Bodner, L.; Dayan, D.; Oberman, M.; Hirshberg, A.; Tal, H. Healing of experimental wounds in sialadenectomized rat. J. Clin. Periodontol. 1992, 19, 345–347. [Google Scholar] [CrossRef] [PubMed]
- Bodner, L.; Dayan, D.; Pinto, Y.; Hammel, I. Characteristics of palatal wound healing in desalivated rats. Arch. Oral Biol. 1993, 38, 17–21. [Google Scholar] [CrossRef]
- Bodner, L.; Dayan, D. Epithelium and connective tissue regeneration during palatal wound healing in desalivated rats—A comparative study. Comp. Biochem. Physiol. A Physiol. 1995, 111, 415–419. [Google Scholar] [CrossRef]
- Kido, D.; Mizutani, K.; Takeda, K.; Mikami, R.; Matsuura, T.; Iwasaki, K.; Izumi, Y. Impact of diabetes on gingival wound healing via oxidative stress. PLoS ONE 2017, 12, e0189601. [Google Scholar] [CrossRef]
- Lee, H.G.; Eun, H.C. Differences between fibroblasts cultured from oral mucosa and normal skin: Implication to wound healing. J. Dermatol. Sci. 1999, 21, 176–182. [Google Scholar] [CrossRef]
- Szpaderska, A.M.; Zuckerman, J.D.; DiPietro, L.A. Differential injury responses in oral mucosal and cutaneous wounds. J. Dent. Res. 2003, 82, 621–626. [Google Scholar] [CrossRef]
- Sandberg, N. Time relationship between administration of cortisone and wound healing in rats. Acta Chir. Scand. 1964, 127, 446–455. [Google Scholar]
- Blomgran, P.; Hammerman, M.; Aspenberg, P. Systemic corticosteroids improve tendon healing when given after the early inflammatory phase. Sci. Rep. 2017, 7, 12468. [Google Scholar] [CrossRef]
- Sandberg, O.H.; Aspenberg, P. Glucocorticoids inhibit shaft fracture healing but not metaphyseal bone regeneration under stable mechanical conditions. Bone Jt. Res. 2015, 4, 170–175. [Google Scholar] [CrossRef]
- Kilkenny, C.; Browne, W.J.; Cuthill, I.C.; Emerson, M.; Altman, D.G. Improving bioscience research reporting: The ARRIVE guidelines for reporting animal research. Osteoarthr. Cartil. 2012, 20, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, E.; Vered, M.; Atzil, S.; Chaushu, G.; Chaushu, L. The dynamics of closure following excisional mid-palatal mucoperiosteal wound in a rat model. Clin. Oral Investig. 2020, 24, 4385–4393. [Google Scholar] [CrossRef] [PubMed]
- Dayan, D.; Salo, T.; Salo, S.; Nyberg, P.; Nurmenniemi, S.; Costea, D.E.; Vered, M. Molecular crosstalk between cancer cells and tumor microenvironment components suggests potential targets for new therapeutic approaches in mobile tongue cancer. Cancer Med. 2012, 1, 128–140. [Google Scholar] [CrossRef]
- Ashcroft, G.S.; Dodsworth, J.; van Boxtel, E.; Tarnuzzer, R.W.; Horan, M.A.; Schultz, G.S.; Ferguson, M.W. Estrogen accelerates cutaneous wound healing associated with an increase in TGF-beta1 levels. Nat. Med. 1997, 3, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Ashcroft, G.S.; Mills, S.J. Androgen receptor-mediated inhibition of cutaneous wound healing. J. Clin. Investig. 2002, 110, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, L.N.; Sorensen, L.T.; Kallehave, F.; Vange, J.; Gottrup, F. Premenopausal women deposit more collagen than men during healing of an experimental wound. Surgery 2002, 131, 338–343. [Google Scholar] [CrossRef]
- Gilliver, S.C.; Ashworth, J.J.; Ashcroft, G.S. The hormonal regulation of cutaneous wound healing. Clin. Dermatol. 2007, 25, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Conrad, S.M.; Blakey, G.H.; Shugars, D.A.; Marciani, R.D.; Phillips, C.; White, R.P., Jr. Patients’ perception of recovery after third molar surgery. J. Oral Maxillofac. Surg. 1999, 57, 1288–1294. [Google Scholar] [CrossRef]
- Phillips, C.; White, R.P., Jr.; Shugars, D.A.; Zhou, X. Risk factors associated with prolonged recovery and delayed healing after third molar surgery. J. Oral Maxillofac. Surg. 2003, 61, 1436–1448. [Google Scholar] [CrossRef]
- Benediktsdottir, I.S.; Wenzel, A.; Petersen, J.K.; Hintze, H. Mandibular third molar removal: Risk indicators for extended operation time, postoperative pain, and complications. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2004, 97, 438–446. [Google Scholar] [CrossRef]
- Adeyemo, W.L.; Ladeinde, A.L.; Ogunlewe, M.O. Clinical evaluation of postextraction site wound healing. J. Contemp. Dent. Pract. 2006, 7, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Chen, S.W.; Jiang, S.Y. Relationship between gingival inflammation and pregnancy. Mediat. Inflamm. 2015, 2015, 623427. [Google Scholar] [CrossRef] [PubMed]
- Mascarenhas, P.; Gapski, R.; Al Shammari, K.; Wang, H.L. Influence of sex hormones on the periodontium. J. Clin. Periodontol. 2003, 30, 671–681. [Google Scholar] [CrossRef]
- Singer, A.J.; Clark, R.A. Cutaneous wound healing. N. Engl. J. Med. 1999, 341, 738–746. [Google Scholar] [CrossRef]
- Hämmerle, C.H.F.; Giannobile, W.V. Biology of soft tissue wound healing and regeneration—Consensus report of group one of the 10th European workshop on periodontology. J. Clin. Periodontol. 2014, 41, S1–S5. [Google Scholar] [CrossRef] [PubMed]
- McGowan, S.L.; Edelhauser, H.F.; Pfister, R.R.; Whikehart, D.R. Stem cell markers in the human posterior limbus and corneal endothelium of unwounded and wounded corneas. Mol. Vis. 2007, 13, 1984–2000. [Google Scholar] [PubMed]
- Verstappen, J.; Van Rheden, R.E.M.; Katsaros, C.; Torensma, R.; Von den Hoff, J.W. Preferential recruitment of bone marrow-derived cells to rat palatal wounds but not to skin wounds. Arch. Oral Biol. 2012, 57, 102–108. [Google Scholar] [CrossRef]
- Yamaguchi, R.; Takami, Y.; Yamaguchi, Y.; Shimazaki, S. Bone marrow-derived myofibroblasts recruited to the upper dermis appear beneath regenerating epidermis after deep dermal burn injury. Wound Repair Regen. 2007, 15, 87–93. [Google Scholar] [CrossRef]
- Direkze, N.C.; Forbes, S.J.; Brittan, M.; Hunt, T.; Jeffery, R.; Preston, S.L.; Poulsom, R.; Hodivala-Dilke, K.; Alison, M.R.; Wright, N.A. Multiple organ engraftment by bone-marrow derived myofibroblasts and fibroblasts in bone-marrow transplanted mice. Stem Cells 2003, 21, 514–520. [Google Scholar] [CrossRef]
- Van Beurden, H.E.; Von den Hoff, J.W.; Torensma, R.; Maltha, J.C.; Kuijpers-Jagtman, A.M. Myofibroblasts in palatal wound healing: Prospects for the reduction of wound contraction after cleft palate repair. J. Dent. Res. 2005, 84, 871–880. [Google Scholar] [CrossRef]
- Nguyen, H.; Lim, J.; Dresner, M.L.; Nixon, B. Effect of local corticosteroids on early inflammatory function in surgical wound of rats. J. Foot Ankle Surg. 1998, 37, 313–318. [Google Scholar] [CrossRef]
- Sulijaya, B.; Takahashi, N.; Yamazaki, K. Host modulation therapy using anti-inflammatory and antioxidant agents in periodontitis: A review to a clinical translation. Arch. Oral Biol. 2019, 105, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Preshaw, P.M. Host modulation therapy with anti-inflammatory agents. Periodontology 2000 2018, 76, 131–149. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.S.; April, W.; Armstrong, P.M. Corticosteroids and wound healing: Clinical considerations in the perioperative period. Am. J. Surg. 2013, 206, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Klinefelter, H.F.; Winkenwerder, W.L.; Bledsoe, T. Single daily dose prednisone therapy. JAMA 1979, 241, 2721–2723. [Google Scholar] [CrossRef]
- Meadows, E.C.; Prudden, J.F. A study of the influence of adrenal steroids on the strength of healing wounds; preliminary report. Surgery 1953, 33, 841–848. [Google Scholar]
- Keskiner, I.; Aydogdu, A.; Balli, U.; Kaleli, A.E. Quantitative changes in palatal donor site thickness after free gingival graft harvesting: A pilot study. J. Clin. Periodontol. 2016, 43, 976–984. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A-P (mm) | L-L (mm) | Area (mm2) | |
|---|---|---|---|
| Group A—Early CS | |||
| Week 1 | 4.98 ± 0.71 | 4.63 ± 0.22 | 16.66 ± 3.43 |
| Week 2 | 3.71 ± 1.08 | 3.76 ± 1.05 | 10.33 ± 4.80 |
| Week 3 | 2.23 ± 0.55 | 3.21 ± 0.44 | 7.32 ± 2.11 |
| Group B—Late CS | |||
| Week 1 | 5.04 ± 0.70 | 4.41 ± 0.60 | 16.49 ± 2.16 |
| Week 2 | 3.32 ± 0.66 | 3.99 ± 0.54 | 9.79 ± 2.45 |
| Week 3 | 3.64 ± 0.97 | 3.60 ± 1.37 | 8.87 ± 3.01 |
| Group C—Control | |||
| Week 1 | 4.97 ±0.56 | 4.43 ± 0.53 | 15.61 ± 2.54 |
| Week 2 | 3.59 ± 0.22 | 3.71 ± 0.74 | 9.29 ± 1.54 |
| Week 3 | 2.13 ± 0.38 | 2.41 ± 0.30 | 4.11 ± 0.88 |
| Early CS | Late CS | Control | p-Value | ||||
|---|---|---|---|---|---|---|---|
| weeks | 2 weeks | 3 weeks | 2 weeks | 3 weeks | 2 weeks | 3 weeks | NS |
| Central | 2.13 ± 0.47 | 1.00 ± 0.40 | 1.88 ± 0.47 | 1.25 ± 0.28 | 2.13 ± 0.47 | 0.63 ± 0.47 | |
| Mid | 2.00 ± 0.00 | 1.13 ± 0.25 | 1.88 ± 0.25 | 1.00 ± 0.40 | 2.00 ± 0.40 | 0.88 ± 0.25 | |
| Lateral | 1.75 ± 0.28 | 1.25 ± 0.28 | 2.00 ± 0.00 | 1.00 ± 0.57 | 2.00 ± 0.40 | 0.50 ± 0.40 | |
| p-value | p-0.000 | p-0.000 | p-0.000 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weinberg, E.; Tagger-Green, N.; Lusthaus, M.; Vered, M.; Mijiritsky, E.; Chaushu, L.; Kolerman, R. The Impact of Corticosteroid Administration at Different Time Points on Mucosal Wound Healing in Rats: An Experimental Pilot In Vivo Study. Biology 2022, 11, 1309. https://doi.org/10.3390/biology11091309
Weinberg E, Tagger-Green N, Lusthaus M, Vered M, Mijiritsky E, Chaushu L, Kolerman R. The Impact of Corticosteroid Administration at Different Time Points on Mucosal Wound Healing in Rats: An Experimental Pilot In Vivo Study. Biology. 2022; 11(9):1309. https://doi.org/10.3390/biology11091309
Chicago/Turabian StyleWeinberg, Evgeny, Nirit Tagger-Green, Michal Lusthaus, Marilena Vered, Eitan Mijiritsky, Liat Chaushu, and Roni Kolerman. 2022. "The Impact of Corticosteroid Administration at Different Time Points on Mucosal Wound Healing in Rats: An Experimental Pilot In Vivo Study" Biology 11, no. 9: 1309. https://doi.org/10.3390/biology11091309