
Autologous Platelet Concentrates (APCs) for Hard Tissue Regeneration in Oral Implantology, Sinus Floor Elevation, Peri-Implantitis, Socket Preservation, and Medication-Related Osteonecrosis of the Jaw (MRONJ): A Literature Review

 ,
,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
1.1. Dental Implants and Sinus Floor Elevation
1.2. Peri-Implantitis
1.3. Socket Preservation
1.4. MRONJ
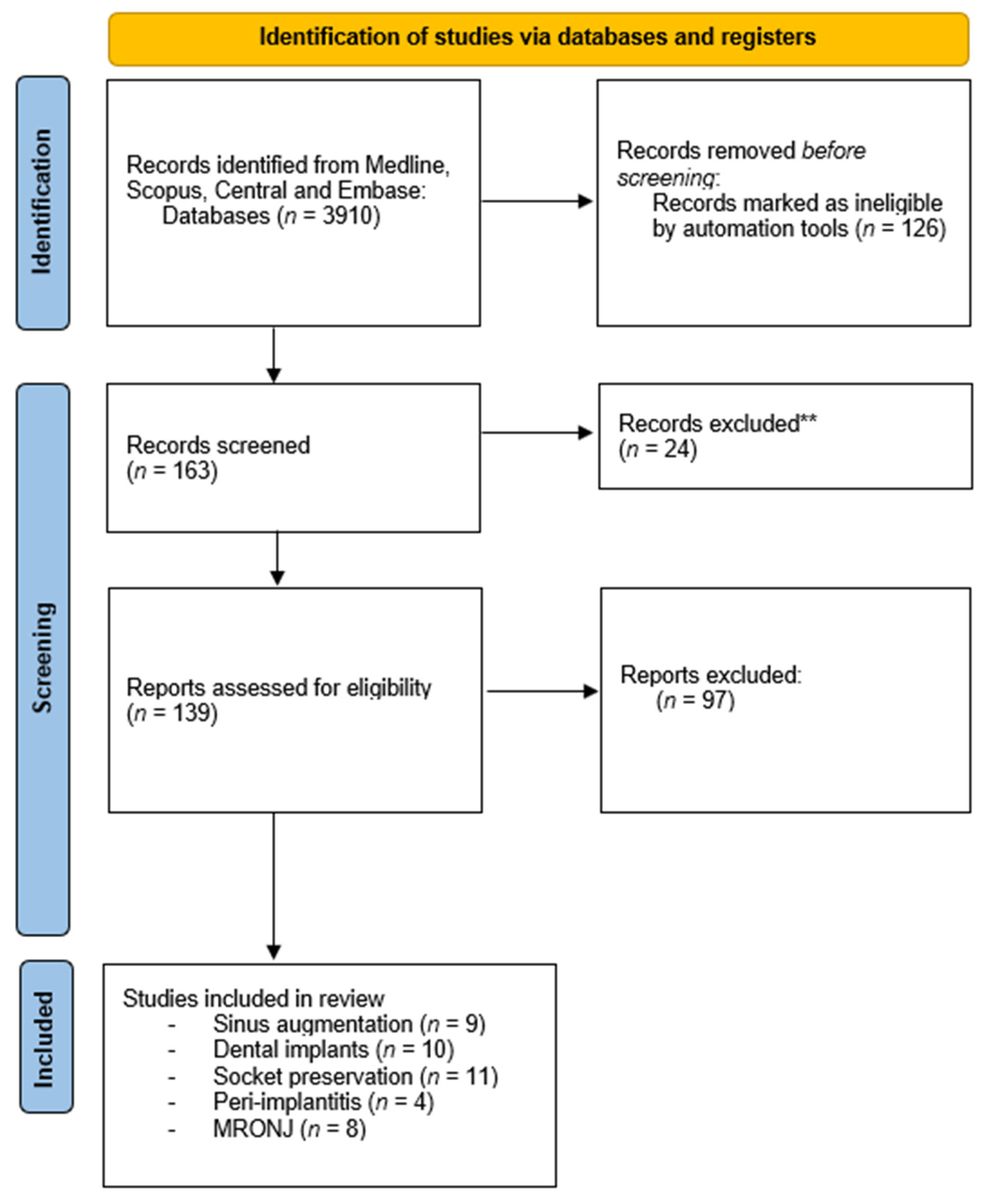
2. Materials and Methods
2.1. APCs in Dental Implants and Sinus Elevation
2.1.1. Inclusion Criteria
- Study design: Randomised controlled trials (RCTs), cohort studies, and cross-sectional studies;
- Population: Human studies, with a minimum of 10 patients and no restriction in terms of patient ages;
- Intervention: Dental implant surgery on patients; only articles with a control group and with data about the follow-up period were included.
2.1.2. General Exclusion Criteria
- Lack of baseline data prior to surgery;
- Patients with systemic diseases or craniofacial anomalies;
- Follow-up of less than 6 months.
2.2. APCs in Peri-Implantitis, Socket Preservation, and MRONJ
2.2.1. Inclusion Criteria
- Study design: Randomised controlled trials (RCTs), cohort studies, cross-sectional studies, case reports, and case series in the English language;
- Population: Only studies on humans were included;
- Intervention: Peri-implantitis, socket preservation, and MRONJ treatments for patients; only articles with a control group and with data about the follow-up period were included;
- Types of outcome: Clinical or histological evaluation.
2.2.2. Exclusion Criteria
- Review articles.
3. Results
3.1. Dental Implants
3.2. Sinus Augmentation
3.3. Socket Preservation
3.3.1. PRP
3.3.2. PRF
3.4. Peri-Implantitis
3.4.1. PRP
3.4.2. PRF
3.4.3. CGF
3.5. MRONJ
3.5.1. PRP

{kind=link}
| Year | First Author | Objectives | Methods | Results (mm) | Authors’ Conclusions |
|---|---|---|---|---|---|
| 2012 | Célio-Mariano et al. [55] | Radiographic evaluation of bone regeneration after application of PRP in tooth sockets. | Thirty bilateral impacted mandibular third molars were divided into a test group (post-extraction socket filled with PRF) and control group. | Increased bone formation in the test group (p < 0.01) in the first month (p < 0.01), second month (p < 0.05), and third month (p < 0.01). | Autologous PRP accelerates alveolar bone regeneration after open tooth extraction. |
| 2020 | Aftab et al. [56] | Efficacy of socket preservation with autologous PRP gel after surgical extraction of the impacted mandibular third molar. | One hundred patients were allocated into two groups. PRP gel was placed in the extraction socket after extraction in the experimental group, while the control group was without PRP gel. | The test group had significantly lower pain scores, reduced facial swelling, and improved interincisal opening. Significant differences (p < 0.005) were observed between the two groups radiographically at the 10th and 16th weeks. | Application of autologous PRP gel may enhance the wound-healing process and promote bone regeneration. |
| 2021 | Ivanova et al. [57] | Randomised controlled clinical trial to evaluate the efficacy of A-PRF alone or in combination with freeze-dried bone allografts in improving vital bone formation and decreasing alveolar bone resorption. | Sixty patients with sixty-three post-extraction sockets were divided into three groups. | Bone resorption was less pronounced in both tested groups than in the control group, where these values were significantly higher. | The study demonstrated a novel in vivo method for measuring bone resorption after ridge augmentation procedures. |
| 2020 | Canellas et al. [58] | A prospective, single-blind, parallel, randomised, controlled clinical trial to evaluate the efficacy of leukocyte- and platelet-rich fibrin (L-PRF) in socket preservation after tooth extraction. | Forty-eight subjects for non-molar tooth extraction randomly assigned to the L-PRF group (n = 24) or the control group (n = 24). Cone-beam computed tomography was performed immediately after tooth extraction and three months after tooth extraction, prior to implant surgery. | A significant difference in bone resorption was registered 1 mm below the crest: 0.93 ± 0.9 mm for the L-PRF group and 2.27 ± 1.2 mm for the control group (p = 0.0001). New bone formation in the L-PRF group was compared with the control group; the values were 55.96 ± 11.97% and 39.69 ± 11.13%, respectively (p = 0.00001). | The administration of L-PRF should always be considered when socket preservation is planned. |
| 2015 | Yelameli et al. [59] | Comparison of the utility and effectiveness of platelet-rich fibrin (PRF) with that of platelet-rich plasma (PRP) in soft tissue healing and bone tissue healing of extracted third molar sockets. | Split mouths of 20 patients underwent bilateral extraction of impacted third molars | Soft tissue healing recorded at one week post-operation for the PRF group was significantly higher than that for the PRP group. | PRF is significantly better than PRP in promoting soft tissue healing and faster regeneration of bone after third-molar extraction. |
| 2013 | Rao et al. [60] | Autologous platelet-rich fibrin gel (PRF gel) for bone regeneration following extraction. | Forty-four bilateral mandibular third molars were divided into a test group (PRF gel) and control group. | Follow-up on the first postoperative day, the first week, and one month, three months, and six months post-operation revealed no statistically significant differences between the groups | Further follow-up of the present patients and a larger sample size are required to obtain conclusive results of the bone regeneration in extraction sockets with PRF gel. |
| 2015 | Baslarli et al. [61] | Clinical and radiological assessment of extraction sockets filled with PRF. | Forty bilateral impacted mandibular third molars were extracted from twenty patients. The test group consisted of post-extraction sockets filled with PRF, while the control group had a blood clot only. | No statistically significant differences between PRF-treated and non-PRF-treated sockets 30 and 90 days post-operation. | More research is needed to support the advantages of PRF in tissue regeneration. |
| 2015 | Kumar et al. [62] | Clinical and radiological assessment of the effects of PRF after third-molar extraction. | Thirty-one patients were included and divided into a test group (PRF placed in the post-extraction socket) and control group. Pain, swelling, maximum mouth opening, periodontal pocket depth, and bone formation were evaluated, with a follow-up period of 3 months. | Significant differences between the control and test groups with regard to the evaluated parameters. | The application of PRF decreases the postoperative pain and swelling, decreases preoperative pocket depth, and induces bone formation. |
| 2016 | Bilginlayar et al. [63] | Postoperative outcomes after removing 80 impacted mandibular third molars from 59 patients. | Eighty impacted mandibular molars were divided into four groups: a control group (with conventional burs), second group (PRF), third group (piezosurgery), and fourth group (piezosurgery and PRF placed in the post-extraction socket). | Significant reduction (p < 0.05) in pain on days 1, 2, and 3, and in the number of analgesics taken on days 2 and 3, in both PRF groups. | There were no significant differences in swelling or trismus between the control group and the other groups. |
| 2015 | Marenzi et al. [64] | Effects of leukocyte- and platelet-rich fibrin (L-PRF) on pain and soft tissue healing after tooth extractions. | Clinical evaluation of 108 tooth extractions performed on 26 patients divided into test and control groups. | After 7 days, modified healing index values in the experimental and control groups were 4.8 ± 0.6 and 5.1 ± 0.9, respectively. | The application of L-PRF in post-extraction sockets is a useful procedure to manage postoperative pain and to promote the soft tissue healing process, reducing the early adverse effects of the inflammation. |
| Year | First Author | Objectives | Methods | Results (mm) | Authors’ Conclusions |
|---|---|---|---|---|---|
| PRP | |||||
| 2019 | Vishnu et al. [65] | Platelet-rich plasma to enhance osseous and associated soft tissue healing around single-piece implants was subjected to immediate loading and compared with a control site not treated with PRP. | Twenty completely edentulous patients were selected, and two one-piece implants were placed for mandibular overdenture. | There was less marginal bone loss, probing depth, percussion, implant mobility, and peri-implantitis around implants treated with PRP. | PRP can be used as a viable treatment adjunct in immediately loaded one-piece implants. |
| PRF | |||||
| 2015 | Hamzacebi et al. [66] | Clinical effectiveness of the application of platelet-rich fibrin (PRF) and conventional flap surgery to treat peri-implant bone loss. | Nineteen patients with peri-implant bone loss were randomly allocated to the PRF test group or the control group with only an access flap. | The increase in keratinised mucosa from baseline to 6 months post-operation was statistically significant for the PRF group (p < 0.001). | The application of PRF in peri-implant bone loss provided better clinical results than conventional flap surgery. |
| 2021 | Sun et al. [67] | Clinical effects of platelet-rich fibrin (PRF) in guided bone regeneration (GBR) for peri-implantitis bone defects. | Eighty patients were divided into two groups. The control group included patients treated with GBR and flap curettage, and the observation group included patients treated with PRF and bone powder. | Significantly higher bone density in the observation group after 120 days (p < 0.001). Postoperative complaints were milder in the PRF group. | The combination of PRF and GBR has a noticeable effect in repairing bone defects in patients with peri-implantitis, and can reduce patients’ pain during the healing period. |
| CGF | |||||
| 2018 | Isler et al. [68] | Evaluation of the clinical and radiographic results after regenerative surgical treatment (RST) of peri-implantitis with collagen membranes (CMs) or concentrated growth factor (CGF) during 12-month follow-up. | Clinical assessment was conducted on 52 patients with peri-implantitis lesions at baseline, and at 6 and 12 months after the operation. | No statistically significant differences were observed in the clinical parameters between the two groups after six months. | Using a collagen membrane in combination with a bone substitute showed better results at 12 months in RST of peri-implantitis. |
| Year | First Author | Objectives | Methods | Results (mm) | Authors’ Conclusions |
|---|---|---|---|---|---|
| 2014 | Longo et al. [69] | Use of bisphosphonates (BPs) to treat bone metastases and various bone diseases. | Seventy-two patients with BRONJ with nonsurgical therapy, surgical therapy, and surgical therapy with platelet-rich plasma (PRP) gel to evaluate the therapeutic effects. | PRP’s good results in improving wound healing provided definitive evidence of its effectiveness. | Recently, it has been proposed to rename BRONJ to antiresorptive-agent-related osteonecrosis of the jaw (ARONJ). |
| 2020 | Mauceri et al. [70] | Longitudinal hospital-based study evaluation at two years of a standardised medical–surgical protocol for dental extraction, combined with platelet-rich-plasma (PRP) application, compared with a conventional protocol in cancer (ONC) and osteometabolic (OST) patients at risk of bisphosphonate (BP)-related ONJ. | Of 20 patients, 6 received BPs for skeletal-cancer-related events (34.17 ± 19.97 months), and 14 received BPs for metabolic bone disease (74.5 ± 34.73 months). Patients underwent a standardised protocol for dental extraction combined with PRP. | Success in all patients treated with PRP. | Combining a standardised medical–surgical protocol with the application of PRP may limit the occurrence of BP-related ONJ. in both ONC and OST patients. |
| 2014 | Kim et al. [71] | A single-group study using leucocyte-rich and platelet-rich fibrin (L-PRF) for treating bisphosphonate-related osteonecrosis of the jaw (BRONJ). | After treatment with L-PRF, the response of each patient was recorded once per month for four months post-operation. Among the total of 34 patients, 26 (77%) showed complete resolution, 6 (18%) showed delayed resolution, and 2 (6%) showed no resolution. | A significant association between treatment and the stage of BRONJ (p = 0.002). | This study showed that it is feasible to use L-PRF for the treatment of BRONJ, but the effectiveness cannot be judged based on this study’s design. |
| 2016 | Norholt et al. [72] | Treatment of osteonecrosis of the jaw (ONJ) with additional use of autologous membranes of platelet-rich fibrin (PRF). | Fifteen patients with ONJ lesions in the maxilla (n = 3), mandible (n = 11), or both (n = 1). | Follow-up 7–20 months after surgery; complete mucosal healing and absence of symptoms were found in 14 of the 15 patients (93%). | The use of PRF membranes in the surgical treatment of grade 2 ONJ may contribute to successful outcomes. |
| 2016 | Park et al. [73] | Comparison of the healing outcomes of combined use of BMP-2 and L-PRF with those of a single use of L-PRF for treating medication-related osteonecrosis of the jaw (MRONJ). | Of 55 patients with MRONJ, 25 were treated with L-PRF alone, and 30 were treated with L-PRF and recombinant human BMP-2. | Surgical sites were evaluated postoperatively at 4 and 16 weeks, and showed more favourable outcomes with complete resolution of the lesions compared with therapy using L-PRF alone (p = 0.028). | The combined use of BMP-2 and L-PRF leads to the early resolution of MRONJ. |
| 2018 | Giudice et al. [74] | Efficacy of platelet-rich fibrin (PRF) after bone surgery compared to surgery alone for osteonecrosis of the jaw (MRONJ). | Forty-seven patients with a diagnosis of stage II or III MRONJ were allocated to two groups. | Analysis of mucosal integrity, absence of infection, and pain evaluation showed a significant difference in PRF only at T1 (p < 0.05). | Local application of PRF after bone surgery may improve the quality of life during the short-term follow-up and reduce pain and postoperative infections. |
| 2017 | Asaka et al. [75] | Effectiveness of platelet-rich fibrin (PRF) as a wound-healing accelerator in patients undergoing oral bisphosphonate therapy and requiring tooth extractions. | One hundred and two patients were divided into a PRF group and a control group. | There were no intraoperative complications in patients with medication-related osteonecrosis of the jaw (MRONJ). | Early epithelisation was confirmed in all PRF patients. |
3.5.2. PRF
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mijiritsky, E.; Assaf, H.D.; Peleg, O.; Shacham, M.; Cerroni, L.; Mangani, L. Use of PRP, PRF and CGF in periodontal regeneration and facial rejuvenation-a narrative review. Biology 2021, 10, 317. [Google Scholar] [CrossRef]
- Qiao, J.; An, N.; Ouyang, X. Quantification of growth factors in different platelet concentrates. Platelets 2017, 28, 774–778. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, Y. Sinus Grafts: Science and Techniques—Then and Now. J. Maxillofac. Oral Surg. 2017, 16, 135–144. [Google Scholar] [CrossRef]
- Draenert, G.F.; Eisenmenger, W. A new technique for the transcrestal sinus floor elevation and alveolar ridge augmentation with press-fit bone cylinders: A technical note. J. Cranio-Maxillofacial Surg. 2007, 35, 201–206. [Google Scholar] [CrossRef]
- Trombelli, L.; Franceschetti, G.; Rizzi, A.; Minenna, P.; Minenna, L.; Farina, R. Minimally invasive transcrestal sinus floor elevation with graft biomaterials. A randomised clinical trial. Clin. Oral Implant. Res. 2012, 23, 424–432. [Google Scholar] [CrossRef]
- Trombelli, L.; Franceschetti, G.; Stacchi, C.; Minenna, L.; Riccardi, O.; Di Raimondo, R.; Rizzi, A.; Farina, R. Minimally invasive transcrestal sinus floor elevation with deproteinised bovine bone or β-tricalcium phosphate: A multicenter, double-blind, randomised, controlled clinical trial. J. Clin. Periodontol. 2014, 41, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Choukroun, J.; Diss, A.; Simonpieri, A.; Girard, M.O.; Schoeffler, C.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Dohan, D.M. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part V: Histologic evaluations of PRF effects on bone allograft maturation in sinus lift. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Fernández, M.P.R.; Mazón, P.; Gehrke, S.A.; Calvo-Guirado, J.L.; De Aza, P.N. Comparison of two xenograft materials used in sinus lift procedures: Material characterization and in vivo behavior. Materials 2017, 10, 623. [Google Scholar] [CrossRef] [Green Version]
- Correia, F.; Pozza, D.H.; Gouveia, S.; Felino, A.C.; Faria-Almeida, R. Advantages of porcine xenograft over autograft in sinus lift: A randomised clinical trial. Materials 2021, 14, 3439. [Google Scholar] [CrossRef]
- Jimi, E.; Hirata, S.; Osawa, K.; Terashita, M.; Kitamura, C.; Fukushima, H. The current and future therapies of bone regeneration to repair bone defects. Int. J. Dent. 2012, 2012, 148261. [Google Scholar] [CrossRef] [Green Version]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S286–S291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renvert, S.; Samuelsson, E.; Lindahl, C.; Persson, G.R. Mechanical nonsurgical treatment of peri-implantitis: A double-blind randomised longitudinal clinical study. I: Clinical results. J. Clin. Periodontol. 2009, 36, 604–609. [Google Scholar] [CrossRef] [PubMed]
- Merli, M.; Bernardelli, F.; Giulianelli, E.; Carinci, F.; Mariotti, G.; Merli, M.; Pini-Prato, G.; Nieri, M. Short-term comparison of two nonsurgical treatment modalities of peri-implantitis: Clinical and microbiological outcomes in a two-factorial randomised controlled trial. J. Clin. Periodontol. 2020, 47, 1268–1280. [Google Scholar] [CrossRef] [PubMed]
- John, G.; Sahm, N.; Becker, J.; Schwarz, F. Nonsurgical treatment of peri-implantitis using an air-abrasive device or mechanical debridement and local application of chlorhexidine. Twelve-month follow-up of a prospective, randomised, controlled clinical study. Clin. Oral Investig. 2015, 19, 1807–1814. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, F.; Alqhtani, N.; Celur, S.L.; Divakar, D.D.; Al-Kheraif, A.A.; Alkhtani, F. Efficacy of nonsurgical mechanical debridement with and without adjunct low-level laser therapy in the treatment of peri-implantitis: A randomised controlled trial. J. Oral Implantol. 2020, 46, 526–531. [Google Scholar] [CrossRef]
- Mettraux, G.R.; Sculean, A.; Bürgin, W.B.; Salvi, G.E. Two-year clinical outcomes following nonsurgical mechanical therapy of peri-implantitis with adjunctive diode laser application. Clin. Oral Implant. Res. 2016, 27, 845–849. [Google Scholar] [CrossRef]
- Wang, H.; Li, W.; Zhang, D.; Li, W.; Wang, Z. Adjunctive photodynamic therapy improves the outcomes of peri-implantitis: A randomised controlled trial. Aust. Dent. J. 2019, 64, 256–262. [Google Scholar] [CrossRef]
- Hentenaar, D.F.M.; De Waal, Y.C.M.; Stewart, R.E.; Van Winkelhoff, A.J.; Meijer, H.J.A.; Raghoebar, G.M. Erythritol airpolishing in the nonsurgical treatment of peri-implantitis: A randomised controlled trial. Clin. Oral Implants Res. 2021, 32, 840–852. [Google Scholar] [CrossRef]
- Blanco, C.; Pico, A.; Dopico, J.; Gándara, P.; Blanco, J.; Liñares, A. Adjunctive benefits of systemic metronidazole on nonsurgical treatment of peri-implantitis. A randomised placebo-controlled clinical trial. J. Clin. Periodontol. 2022, 49, 15–27. [Google Scholar] [CrossRef]
- Shibli, J.A.; Ferrari, D.S.; Siroma, R.S.; De Figueiredo, L.C.; De Faveri, M.; Feres, M. Microbiological and clinical effects of adjunctive systemic metronidazole and amoxicillin in the nonsurgical treatment of peri-implantitis: 1 year follow-up. Braz. Oral Res. 2019, 33, e080. [Google Scholar] [CrossRef] [Green Version]
- Machtei, E.E.; Romanos, G.; Kang, P.; Travan, S.; Schmidt, S.; Papathanasiou, E.; Tatarakis, N.; Tandlich, M.; Liberman, L.H.; Horwitz, J.; et al. Repeated delivery of chlorhexidine chips for the treatment of peri-implantitis: A multicenter, randomised, comparative clinical trial. J. Periodontol. 2021, 92, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Carcuac, O.; Derks, J.; Charalampakis, G.; Abrahamsson, I.; Wennstrom, J.; Berglundh, T. Adjunctive Systemic and Local Antimicrobial Therapy in the Surgical Treatment of Peri-implantitis: A Randomized Controlled Clinical Trial. J. Dent. Res. 2016, 95, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Carcuac, O.; Derks, J.; Abrahamsson, I.; Wennström, J.L.; Petzold, M.; Berglundh, T. Surgical treatment of peri-implantitis: 3-year results from a randomised controlled clinical trial. J. Clin. Periodontol. 2017, 44, 1294–1303. [Google Scholar] [CrossRef]
- Schwarz, F.; John, G.; Schmucker, A.; Sahm, N.; Becker, J. Combined surgical therapy of advanced peri-implantitis evaluating two methods of surface decontamination: A 7-year follow-up observation. J. Clin. Periodontol. 2017, 44, 337–342. [Google Scholar] [CrossRef]
- de Waal, Y.C.M.; Raghoebar, G.M.; Meijer, H.J.A.; Winkel, E.G.; van Winkelhoff, A.J. Implant decontamination with 2% chlorhexidine during surgical peri-implantitis treatment: A randomised, double-blind, controlled trial. Clin. Oral Implant. Res. 2015, 26, 1015–1023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daugela, P.; Cicciù, M.; Saulacic, N. Surgical Regenerative Treatments for Peri-Implantitis: Meta-analysis of Recent Findings in a Systematic Literature Review. J. Oral Maxillofac. Res. 2016, 7, e15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mordini, L.; Sun, N.; Chang, N.; De Guzman, J.P.; Generali, L.; Consolo, U. Peri-implantitis regenerative therapy: A review. Biology 2021, 10, 773. [Google Scholar] [CrossRef]
- Tan, W.L.; Wong, T.L.T.; Wong, M.C.M.; Lang, N.P. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin. Oral Implants Res. 2012, 23, 1–21. [Google Scholar] [CrossRef]
- Schropp, L. Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. J. Prosthet. Dent. 2004, 91, 92. [Google Scholar] [CrossRef]
- Kassim, B.; Ivanovski, S.; Mattheos, N. Current perspectives on the role of ridge (socket) preservation procedures in dental implant treatment in the aesthetic zone. Aust. Dent. J. 2014, 59, 48–56. [Google Scholar] [CrossRef] [Green Version]
- Clavero, J.; Lundgren, S. Ramus or Chin Grafts for Maxillary Sinus Inlay and Local Onlay Augmentation: Comparison of Donor Site Morbidity and Complications. Clin. Implant. Dent. Relat. Res. 2003, 5, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Ohta, K.; Yoshimura, H. Medication-Related Osteonecrosis of the Jaw. Am. J. Med. Sci. 2020, 360, 316–317. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, M.; Gallesio, G.; Mozzati, M. Autologous platelet concentrates for bisphosphonate-related osteonecrosis of the jaw treatment and prevention. A systematic review of the literature. Eur. J. Cancer 2015, 51, 62–74. [Google Scholar] [CrossRef] [PubMed]
- Al-Hamed, F.S.; Mahri, M.; Al-Waeli, H.; Torres, J.; Badran, Z.; Tamimi, F. Regenerative Effect of Platelet Concentrates in Oral and Craniofacial Regeneration. Front. Cardiovasc. Med. 2019, 6, 126. [Google Scholar] [CrossRef] [Green Version]
- Gönen, Z.B.; Yılmaz Asan, C. Treatment of bisphosphonate-related osteonecrosis of the jaw using platelet-rich fibrin. Cranio—J. Craniomandib. Pract. 2017, 35, 332–336. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Dodson, T.B.; Aghaloo, T.; Carlson, E.R.; Ward, B.B.; Kademani, D. American Association of Oral and Maxillofacial Surgeons’ Position Paper on Medication-Related Osteonecrosis of the Jaws—2022 Update. J. Oral Maxillofac. Surg. 2022, 80, 920–943. [Google Scholar] [CrossRef]
- Hartlev, J.; Schou, S.; Isidor, F.; Nørholt, S.E. A clinical and radiographic study of implants placed in autogenous bone grafts covered by either a platelet-rich fibrin membrane or deproteinised bovine bone mineral and a collagen membrane: A pilot randomised controlled clinical trial with a 2-year follo. Int. J. Implant Dent. 2021, 7, 8. [Google Scholar] [CrossRef]
- Pichotano, E.C.; de Molon, R.S.; de Souza, R.V.; Austin, R.S.; Marcantonio, E.; Zandim-Barcelos, D.L. Evaluation of L-PRF combined with deproteinised bovine bone mineral for early implant placement after maxillary sinus augmentation: A randomised clinical trial. Clin. Implant Dent. Relat. Res. 2019, 21, 253–262. [Google Scholar] [CrossRef] [Green Version]
- Tabrizi, R.; Arabion, H.; Does, T.K.K. Does platelet-rich fibrin increase the stability of implants in the posterior of the maxilla? A split-mouth randomised clinical trial. Int. J. Oral Maxillofac. Surg. 2018, 47, 672–675. [Google Scholar] [CrossRef]
- Boora, P.; Rathee, M.; Bhoria, M. Effect of Platelet Rich Fibrin (PRF) on peri-implant soft tissue and crestal bone in one-stage implant placement: A randomised controlled trial. J. Clin. Diagnostic Res. 2015, 9, ZC18–ZC21. [Google Scholar] [CrossRef]
- Attia, S.; Narberhaus, C.; Schaaf, H.; Streckbein, P.; Pons-Kühnemann, J.; Schmitt, C.; Neukam, F.W.; Howaldt, H.-P.; Böttger, S. Long-Term Influence of Platelet-Rich Plasma (PRP) on Dental Implants after Maxillary Augmentation: Implant Survival and Success Rates. J. Clin. Med. 2020, 9, 391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kundu, R.; Rathee, M. Effect of Platelet-Rich-Plasma (PRP) and implant surface topography on implant stability and bone. J. Clin. Diagnostic Res. 2014, 8, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.; Han, X.H.; Hu, L.H.; Wu, H.W.; Huang, S.Y.; Lü, Y.P. Efficacy of concentrated growth factors combined with mineralised collagen on quality of life and bone reconstruction of guided bone regeneration. Regen. Biomater. 2020, 7, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Cai, Z.; Zheng, D.; Lin, P.; Cai, Y.; Hong, S.; Lai, Y.; Wu, D. Inlay osteotome sinus floor elevation with concentrated growth factor application and simultaneous short implant placement in severely atrophic maxilla. Sci. Rep. 2016, 6, 27348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Özveri Koyuncu, B.; İçpınar Çelik, K.; Özden Yüce, M.; Günbay, T.; Çömlekoğlu, M.E. The role of concentrated growth factor on implant stability: A preliminary study. J. Stomatol. Oral Maxillofac. Surg. 2020, 121, 363–367. [Google Scholar] [CrossRef]
- Pirpir, C.; Yilmaz, O.; Candirli, C.; Balaban, E. Evaluation of effectiveness of concentrated growth factor on osseointegration. Int. J. Implant Dent. 2017, 3, 7. [Google Scholar] [CrossRef] [Green Version]
- Stumbras, A.; Januzis, G.; Gervickas, A.; Kubilius, R.; Juodzbalys, G. Randomized and controlled clinical trial of bone healing after alveolar ridge preservation using xenografts and allografts versus plasma rich in growth factors. J. Oral Implantol. 2020, 46, 515–525. [Google Scholar] [CrossRef]
- Zhang, Y.; Tangl, S.; Huber, C.D.; Lin, Y.; Qiu, L.; Rausch-Fan, X. Effects of Choukroun’s platelet-rich fibrin on bone regeneration in combination with deproteinised bovine bone mineral in maxillary sinus augmentation: A histological and histomorphometric study. J. Cranio-Maxillofac. Surg. 2012, 40, 321–328. [Google Scholar] [CrossRef]
- Simonpieri, A.; Choukroun, J.; Del Corso, M.; Sammartino, G.; Ehrenfest, D.M.D. Simultaneous sinus-lift and implantation using microthreaded implants and leukocyte- and platelet-rich fibrin as sole grafting material: A six-year experience. Implant. Dent. 2011, 20, 2–12. [Google Scholar] [CrossRef] [Green Version]
- Aoki, N.; Maeda, M.; Kurata, M.; Hirose, M.; Ojima, Y.; Wada, K.; Shibuya, Y. Sinus floor elevation with platelet-rich fibrin alone: A Clinical retrospective study of 1-7 years. J. Clin. Exp. Dent. 2018, 10, e984–e991. [Google Scholar] [CrossRef]
- Olgun, E.; Ozkan, S.Y.; Atmaca, H.T.; Yalim, M.; Hendek, M.K. Comparison of the clinical, radiographic, and histological effects of titanium-prepared platelet rich fibrin to allograft materials in sinus-lifting procedures. J. Investig. Clin. Dent. 2018, 9, e12347. [Google Scholar] [CrossRef] [PubMed]
- Tatullo, M.; Marrelli, M.; Cassetta, M.; Pacifici, A.; Stefanelli, L.V.; Scacco, S.; Dipalma, G.; Pacifici, L.; Inchingolo, F. Platelet rich fibrin (PRF) in reconstructive surgery of atrophied maxillary bones: Clinical and histological evaluations. Int. J. Med. Sci. 2012, 9, 872–880. [Google Scholar] [CrossRef] [PubMed]
- Khairy, N.M.; Shendy, E.E.; Askar, N.A.; El-Rouby, D.H. Effect of platelet rich plasma on bone regeneration in maxillary sinus augmentation (randomised clinical trial). Int. J. Oral Maxillofac. Surg. 2013, 42, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Nizam, N.; Eren, G.; Akcalı, A.; Donos, N. Maxillary sinus augmentation with leukocyte and platelet-rich fibrin and deproteinised bovine bone mineral: A split-mouth histological and histomorphometric study. Clin. Oral Implants Res. 2018, 29, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Célio-Mariano, R.; De Melo, W.M.; Carneiro-Avelino, C. Comparative radiographic evaluation of alveolar bone healing associated with autologous platelet-rich plasma after impacted mandibular third molar surgery. J. Oral Maxillofac. Surg. 2012, 70, 19–24. [Google Scholar] [CrossRef]
- Aftab, A.; Joshi, U.K.M.; Patil, S.K.G.; Hussain, E.; Bhatnagar, S. Efficacy of autologous platelet rich plasma gel in soft and hard tissue healing after surgical extraction of impacted mandibular third molar—A prospective study. J. Oral Maxillofac. Surg. Med. Pathol. 2020, 32, 241–246. [Google Scholar] [CrossRef]
- Ivanova, V.; Chenchev, I.; Zlatev, S.; Mijiritsky, E. Comparison Study of the Histomorphometric Results after Socket Preservation with PRF and Allograft Used for Socket Preservation-Randomized Controlled Trials. Int. J. Env. Res. Public Health 2021, 18, 7451. [Google Scholar] [CrossRef]
- dos Santos Canellas, J.V.; da Costa, R.C.; Breves, R.C.; de Oliveira, G.P.; da Silva Figueredo, C.M.; Fischer, R.G.; Thole, A.A.; Medeiros, P.J.D.A.; Ritto, F.G. Tomographic and histomorphometric evaluation of socket healing after tooth extraction using leukocyte- and platelet-rich fibrin: A randomised, single-blind, controlled clinical trial. J. Cranio-Maxillofac. Surg. 2020, 48, 24–32. [Google Scholar] [CrossRef]
- Yelamali, T.; Saikrishna, D. Role of Platelet Rich Fibrin and Platelet Rich Plasma in Wound Healing of Extracted Third Molar Sockets: A Comparative Study. J. Maxillofac. Oral Surg. 2015, 14, 410–416. [Google Scholar] [CrossRef] [Green Version]
- Girish Rao, S.; Bhat, P.; Nagesh, K.S.; Rao, G.H.R.; Mirle, B.; Kharbhari, L.; Gangaprasad, B. Bone Regeneration in Extraction Sockets with Autologous Platelet Rich Fibrin Gel. J. Maxillofac. Oral Surg. 2013, 12, 11–16. [Google Scholar] [CrossRef]
- Baslarli, O.; Tumer, C.; Ugur, O.; Vatankulu, B. Evaluation of osteoblastic activity in extraction sockets treated with platelet-rich fibrin. Med. Oral Patol. Oral Cir. Bucal 2015, 20, e111–e116. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Prasad, K.; Ramanujam, L.; Ranganath, R.; Dexith, J.; Chauhan, A. Evaluation of treatment outcome after impacted mandibular third molar surgery with the use of autologous platelet-rich fibrin: A randomised controlled clinical study. J. Oral Maxillofac. Surg. 2015, 73, 1042–1049. [Google Scholar] [CrossRef] [PubMed]
- Bilginaylar, K.; Uyanik, L.O. Evaluation of the effects of platelet-rich fibrin and piezosurgery on outcomes after removal of ımpacted mandibular third molars. Br. J. Oral Maxillofac. Surg. 2016, 54, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Marenzi, G.; Riccitiello, F.; Tia, M.; Di Lauro, A.; Sammartino, G. Influence of leukocyte- and platelet-rich fibrin (L-PRF) in the healing of simple postextraction sockets: A split-mouth study. Biomed. Res. Int. 2015, 2015, 369273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vishnu, V.A.; Sanyal, P.K.; Tewary, S.; Nilesh, K.; Suresh Prasad, R.M.; Pawashe, K. A split-mouth clinico-radiographic comparative study for evaluation of crestal bone and peri-implant soft tissues in immediately loaded implants with and without platelet-rich plasma bioactivation. J. Dent. Res. Dent. Clin. Dent. Prospect. 2019, 13, 117–122. [Google Scholar] [CrossRef]
- Hamzacebi, B.; Oduncuoglu, B.; Alaaddinoglu, E. Treatment of Peri-implant Bone Defects with Platelet-Rich Fibrin. Int. J. Periodontics Restorative Dent. 2015, 35, 415–422. [Google Scholar] [CrossRef] [Green Version]
- Sun, G.; Cao, L.; Li, H. Effects of platelet-rich fibrin combined with guided bone regeneration in the reconstruction of peri-implantitis bone defect. Am. J. Transl. Res. 2021, 13, 8397–8402. [Google Scholar]
- Isler, S.C.; Soysal, F.; Ceyhanlı, T.; Bakırarar, B.; Unsal, B. Regenerative surgical treatment of peri-implantitis using either a collagen membrane or concentrated growth factor: A 12-month randomised clinical trial. Clin. Implant. Dent. Relat. Res. 2018, 20, 703–712. [Google Scholar] [CrossRef]
- Longo, F.; Guida, A.; Aversa, C.; Pavone, E.; Di Costanzo, G.; Ramaglia, L.; Ionna, F. Platelet rich plasma in the treatment of bisphosphonate-related osteonecrosis of the jaw: Personal experience and review of the literature. Int. J. Dent. 2014, 2014, 298945. [Google Scholar] [CrossRef] [Green Version]
- Mauceri, R.; Panzarella, V.; Pizzo, G.; Oteri, G.; Cervino, G.; Mazzola, G.; Di Fede, O.; Campisi, G. Platelet-Rich Plasma (PRP) in dental extraction of patients at risk of bisphosphonate-related osteonecrosis of the jaws: A two-year longitudinal study. Appl. Sci. 2020, 10, 4487. [Google Scholar] [CrossRef]
- Kim, J.W.; Kim, S.J.; Kim, M.R. Leucocyte-rich and platelet-rich fibrin for the treatment of bisphosphonate-related osteonecrosis of the jaw: A prospective feasibility study. Br. J. Oral Maxillofac. Surg. 2014, 52, 854–859. [Google Scholar] [CrossRef] [PubMed]
- Nørholt, S.E.; Hartlev, J. Surgical treatment of osteonecrosis of the jaw with the use of platelet-rich fibrin: A prospective study of 15 patients. Int. J. Oral Maxillofac. Surg. 2016, 45, 1256–1260. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Kim, J.W.; Kim, S.J. Does the Addition of Bone Morphogenetic Protein 2 to Platelet-Rich Fibrin Improve Healing After Treatment for Medication-Related Osteonecrosis of the Jaw? J. Oral Maxillofac. Surg. 2017, 75, 1176–1184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giudice, A.; Barone, S.; Giudice, C.; Bennardo, F.; Fortunato, L. Can platelet-rich fibrin improve healing after surgical treatment of medication-related osteonecrosis of the jaw? A pilot study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, 390–403. [Google Scholar] [CrossRef]
- Asaka, T.; Ohga, N.; Yamazaki, Y.; Sato, J.; Satoh, C.; Kitagawa, Y. Platelet-rich fibrin may reduce the risk of delayed recovery in tooth-extracted patients undergoing oral bisphosphonate therapy: A trial study. Clin. Oral Investig. 2017, 21, 2165–2172. [Google Scholar] [CrossRef]
- Adell, R.; Eriksson, B.; Lekholm, U.; Brånemark, P.I.; Jemt, T. Long-term follow-up study of osseointegrated implants in the treatment of totally edentulous jaws. Int. J. Oral Maxillofac. Implant. 1990, 5, 347–359. [Google Scholar]
- Raghavendra, S.; Wood, M.C.; Taylor, T.D. Early wound healing around endosseous implants: A review of the literature. Int. J. Oral Maxillofac. Implant. 2005, 20, 425–431. [Google Scholar]
- Öncü, E.; Bayram, B.; Kantarcı, A.; Gülsever, S.; Alaaddinoğlu, E.E. Posıtıve effect of platelet rich fibrin on osseointegration. Med. Oral Patol. Oral Cir. Bucal. 2016, 21, e601–e607. [Google Scholar] [CrossRef]
- Dohan, D.M.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part I: Technological concepts and evolution. Oral Surg. Oral Med. Oral Pathol Oral Radiol. Endod. 2006, 101, e37–e44. [Google Scholar] [CrossRef]
- Masuki, H.; Okudera, T.; Watanebe, T.; Suzuki, M.; Nishiyama, K.; Okudera, H.; Nakata, K.; Uematsu, K.; Su, C.Y.; Kawase, T. Growth factor and pro-inflammatory cytokine contents in platelet-rich plasma (PRP), plasma rich in growth factors (PRGF), advanced platelet-rich fibrin (A-PRF), and concentrated growth factors (CGF). Int. J. Implant. Dent. 2016, 2, 19. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, E.; Flückiger, L.; Fujioka-Kobayashi, M.; Sawada, K.; Sculean, A.; Schaller, B.; Miron, R.J. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin. Oral Investig. 2016, 20, 2353–2360. [Google Scholar] [CrossRef] [PubMed]
- Anitua, E.; Prado, R.; Sánchez, M.; Orive, G. Platelet-rich plasma: Preparation and formulation. Oper. Tech. Orthop. 2012, 22, 25–32. [Google Scholar] [CrossRef]

| Year | First Author | Objectives | Methods | Results (mm) | Authors’ Conclusions |
|---|---|---|---|---|---|
| PRP | |||||
| 2018 | Tabrizi et al. [39] | Evaluation of the impact of PRF on implant stability in the distal areas of the upper jaw. | Twenty patients requiring bilateral implants in the distal areas of the maxilla were included and divided into PRF and control groups. Implant stability was assessed by resonance frequency analysis (RFA) at 2, 4, and 6 weeks after placement. | Significant differences in the mean ISQ values were found between the groups at two weeks (p = 0.04), four weeks (p = 0.014), and six weeks (p = 0.027) after placement. | PRF may enhance implant stability during the healing period of implants placed in the posterior maxilla. |
| 2015 | Boora et al. [40] | Clinical and radiological evaluation of the effect of PRF on bone and soft tissue structures following one-stage implant placement in the maxillary aesthetic area. | The patients were divided into a PRF group and a control group. The parameters of interest were probing depth and marginal bone level around implants. | In 3 months, there was a decrease in probing depth in both groups. There were no significant changes in probing depth or bleeding in either group after 1 and 3 months. The marginal bone level changes had a statistically significantly lower mean value in the PRF group | PRF may have a beneficial effect on the peri-implant tissues. |
| 2020 | Attia et al. [41] | The long-term impact of PRP regarding clinical and radiological outcomes on the inserted implants after maxillary augmentation in the RCT. | Consideration of plaque index, probing depth, bleeding index, mobility grade, Periotest® values, and radiological bone loss. | In 36% of the results, the PRP group was superior to the control group. | The results showed no positive effect of PRP on the clinical and radiological outcomes. |
| 2014 | Kundu et al. [42] | Evaluation of the impact of PRP and different implant surface topographies on the stability of implants that were immediately loaded. | The patients were divided into two groups—with or without PRP. | PRP had no statistically significant effect on bone height changes. | The results revealed no significant effect of PRP on bone height. There was an improvement in implant stability in the PRP and square thread-form implant group. |
| 2020 | Dai et al. [43] | Clinical evaluation of the effectiveness of concentrated growth factor (CGF) in combination with mineralised collagen (MC) in guided bone regeneration (GBR). | GBR technique with simultaneous implant placement was performed on 29 patients with CGF and MC, or with MC as the sole grafting material. CBCT was examined immediately after the operation, as well as at three and six months. | Benefits to the CGF + MC group in terms of rapid relief from discomfort after the operation and reduced swelling. | Milder clinical symptoms, reduced postoperative discomfort, and increased bone regeneration were observed in the CGF + MC group. |
| PRF | |||||
| 2021 | Hartlev et al. [37] | Survival and clinical performance of implants placed in sites previously augmented with autogenous bone grafts covered by PRF membrane (PRF group) or autogenous bone graft with deproteinised bovine bone mineral and a resorbable collagen membrane (control group). | The test group included 14 placed implants, while the control group included 13. Patients were recalled for evaluation 24 months after prosthetic rehabilitation. | The radiographic peri-implant marginal bone change at follow-up was 0.26 in the PRF group and 0.68 in the control group. | Both approaches can be used for bone augmentation. There was an increased marginal bone level in the PRF group compared to the control group. |
| 2018 | Pichotano et al. [38] | Evaluation of the impact of leukocyte- and platelet-rich fibrin (L-PRF) added to deproteinised bovine bone mineral (DBBM) for early implant placement after maxillary sinus augmentation. | In a split-mouth design, 12 patients were divided into a test group (DBBM + L-PRF) and a control group (DBBM as the sole grafting material). Implants were placed four months after the augmentation in the test group, and after eight months in the control group. | Primary stability was significantly higher in the control group (75.13 ± 5.69). Newly formed bone was higher in the test group (44.58% ± 13.9%). | Adding PRF to DBBM allowed early implant placement (4 months, versus 8 months of healing in the control group) with increased new bone formation. |
| 2015 | Boora et al. [40] | Effect of PRF on peri-implant tissue three months following one-stage implant placement in the maxillary aesthetic area. | Twenty patients were randomly divided into a test group (PRF) group and a control group. | There were no significant changes in probing depth or bleeding in either group after 1 and 3 months. | PRF could be considered a therapeutic s supplement in cases of one -tage, single-tooth implant placement in the aesthetic area of the maxilla. |
| CGF | |||||
| 2016 | Chen et al. [44] | Clinical and radiological results of modified osteotome sinus floor elevation (OSFE) with CGF and simultaneous short implant placement in cases with residual bone height (RBH) of 2–4 mm in the severely atrophic maxilla. | Sixteen patients were included in the study. Twenty-five short implants were placed using the modified OSFE with CGF. Vertical bone gain (VBG) was measured using cone-beam computed tomography. | The mean residual bone height 12 months after surgery was 9.40 ± 0.47 mm. | Modified OSFE with CGF application and simultaneous short implant placement resulted in predictable clinical results for severely atrophic maxilla with RBH of 2–4 mm. |
| 2020 | Koyuncu et al. [45] | Effect of concentrated growth factor (CGF) on dental implant stability in type 2 bone using the resonance frequency analysis (RFA) device Smartpeg®. | The study included 12 patients who required dental implants in the anterior mandible. One socket was prepared conventionally (control group), while the other was covered with a CGF membrane. Implant stability was measured upon implant placement and at the first, second, and fourth weeks. | No statistically significant differences were observed between the ISQ values in either of the groups. | CGF did not benefit dental implant stability in the early healing period in type 2 bone. |
| 2017 | Pirpir et al. [46] | The effects of CGF on implant stability and osseointegration. | Twelve patients were divided into a test group (where implant bed was covered with a CGF membrane) and a control group. Implant stability was measured immediately after implant placement and at the first and fourth weeks. | The mean ISQ values were significantly higher in the test group during the period of evaluation. | Concentrated growth factors had positive effects on implant stabilisation. The ISQ measurements in week one and week four were notably higher in the study group. |
| Year | First Author | Objectives | Methods | Results (mm) | Authors’ Conclusions |
|---|---|---|---|---|---|
| PRP | |||||
| 2014 | Kundu et al. [42] | Evaluation of the effects of platelet-rich plasma (PRP) and different implant surface topography on implant stability and bone levels around immediately loaded dental implants. | A total of 30 implants divided into Group 1 (without PRP) and Group 2 (where implants were placed after dipping in activated PRP). Implant stability was measured with Periotest. | A statistically significant difference was noted in implant stability with PRP at baseline. | PRP-treated implant surfaces resulted in improved implant stability and bone levels. |
| PRF | |||||
| 2012 | Zhang et al. [48] | Influence of PRF on bone regeneration in sinus augmentation combined with DBBM. | Eleven sinuses were divided into a test group (DBBM + PRF) and control group (DBBM as the sole grafting material). | After six months, similar composition and distribution were found in both of the groups. | No significant difference between the groups was found. |
| 2011 | Somonpieri [49] | Clinical and radiological evaluation of the application of L-PRF as a sole grafting material in lateral sinus elevation procedures with simultaneous implant placement. | Twenty-three lateral sinus elevations were performed on 20 patients with simultaneous implant placement. | Six months after surgery, all implants were clinically stable during abutment tightening. Maximum follow-up at six years. Vertical bone gain between 8.5 and 12 mm. | L-PRF as the sole filling material during simultaneous sinus lift and implantation seems to be a reliable surgical option, promoting natural bone regeneration. |
| 2018 | Aoki et al. [50] | Evaluation of the application of PRF as a sole grafting material in sinus lift procedures. | A total of 71 implants in 34 patients after 1–7 years’ follow-up time. Statistical models for implant survival and potential factors associated with implant loss. | Seven implants were lost, and the cumulative survival rate at seven years by implant-based and patient-based analyses was 85.5% and 85.7%, respectively. Mean residual bone height (RBH) 4.26 mm. Greater implant survival rate for RBH < 4 mm than RBH ≥ 4 mm. | Sinus floor elevation with PRF alone could be applied in cases of lower RBH. However, it should be performed carefully in cases of RBH < 4 mm. |
| 2018 | Olgun et al. [51] | Clinical, histological, and radiographic comparison between autologous titanium-prepared PRF (T-PRF) and allografts in sinus lifting procedures. | Ten sinuses were randomly assigned to T-PRF as the test group, and 8 were assigned to allografts as the control group. | The control group showed better radiological results (62% in volume, 53% in density, and 69% in height) than the T-PRF group. Newly formed bone ratios were 17.28 ± 2.53 and 16.58 ± 1.05 in the allograft and T-PRF groups, respectively. There was no difference between the test and control groups (p = 0.611) in terms of implant stability values. | T-PRF alone in sinus lifting procedures revealed successful clinical and histomorphometric results. |
| 2012 | Tatullo et al. [52] | Clinical and histological evaluation of PRF in combination with deproteinised bovine bone (Bio-Oss) compared to DBBM alone in sinus elevation procedures. | Seventy-two sinus lifts with subsequent implant insertions. | Histological results after 106 days revealed that adding of PRF resulted in the formation of lamellar bone tissue with an interposed, richly vascularised stroma. | PRF and piezosurgery reduced the healing time compared to the 150 days described in the literature, facilitating optimal bone regeneration. At 106 days, it was possible to achieve good primary stability of endosseous implants, although lacking functional loading. |
| 2013 | Khairy et al. [53] | Evaluation of bone quality in sinuses augmented with autogenous bone, with or without platelet-rich plasma (PRP) mix. | In group “I”, five maxillary sinus lifts with autogenous bone augmentation and implant insertion were performed six months after grafting. Ten maxillary sinus lifts with autogenous bone augmentation were mixed with PRP, with implant insertion at 4 or 6 months post-grafting in Group II. | Six months after implant placement, Group II showed significantly higher mean bone density (p = 0.041). Histomorphometric analysis revealed that Group I had the highest mean value, and was statistically significant (39.5 ± 7.4; p = 0.003). | PRP did not reveal any significant impact on bone quality at 3 months after placement. Bone density was improved after 6 months. |
| 2018 | Nizam et al. [54] | Evaluation of the effects of leukocyte- and platelet-rich fibrin (L-PRF) combined with deproteinised bovine bone mineral (DBBM) on bone regeneration in maxillary sinus augmentation. | Twenty-six maxillary sinus augmentation procedures were randomly divided into a test group (DBBM + L-PRF) and control group (DBBM alone in a split-mouth design). | No significant differences in the evaluated parameters were observed. | Both techniques were effective for maxillary sinus augmentation. After six months of healing, adding L-PRF to DBBM did not improve the amount of regenerated bone or the amount of the graft integrated under histological and histomorphometric evaluation. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mijiritsky, E.; Assaf, H.D.; Kolerman, R.; Mangani, L.; Ivanova, V.; Zlatev, S. Autologous Platelet Concentrates (APCs) for Hard Tissue Regeneration in Oral Implantology, Sinus Floor Elevation, Peri-Implantitis, Socket Preservation, and Medication-Related Osteonecrosis of the Jaw (MRONJ): A Literature Review. Biology 2022, 11, 1254. https://doi.org/10.3390/biology11091254
Mijiritsky E, Assaf HD, Kolerman R, Mangani L, Ivanova V, Zlatev S. Autologous Platelet Concentrates (APCs) for Hard Tissue Regeneration in Oral Implantology, Sinus Floor Elevation, Peri-Implantitis, Socket Preservation, and Medication-Related Osteonecrosis of the Jaw (MRONJ): A Literature Review. Biology. 2022; 11(9):1254. https://doi.org/10.3390/biology11091254
Chicago/Turabian StyleMijiritsky, Eitan, Haya Drora Assaf, Roni Kolerman, Luca Mangani, Vasilena Ivanova, and Stefan Zlatev. 2022. "Autologous Platelet Concentrates (APCs) for Hard Tissue Regeneration in Oral Implantology, Sinus Floor Elevation, Peri-Implantitis, Socket Preservation, and Medication-Related Osteonecrosis of the Jaw (MRONJ): A Literature Review" Biology 11, no. 9: 1254. https://doi.org/10.3390/biology11091254