
Comparison of Neural Correlates of Reactive Inhibition in Cocaine, Heroin, and Polydrug Users through a Contextual Go/No-Go Task Using Event-Related Potentials

 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Ethics Statement
2.2. Procedure
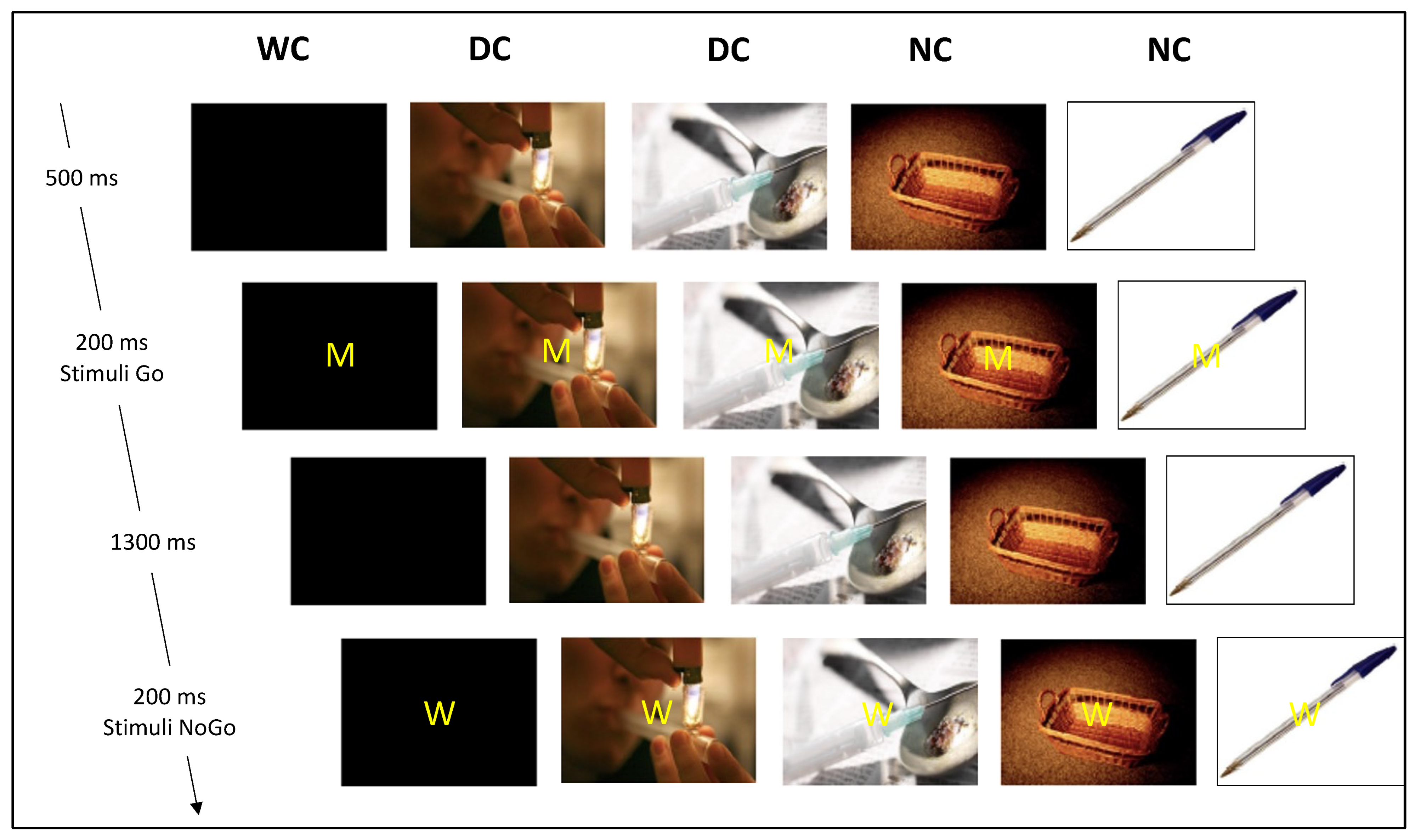
2.3. The Go/No-Go Cognitive Task
2.4. EEG Recording
2.5. Statistics
3. Results
3.1. Behavioral Data
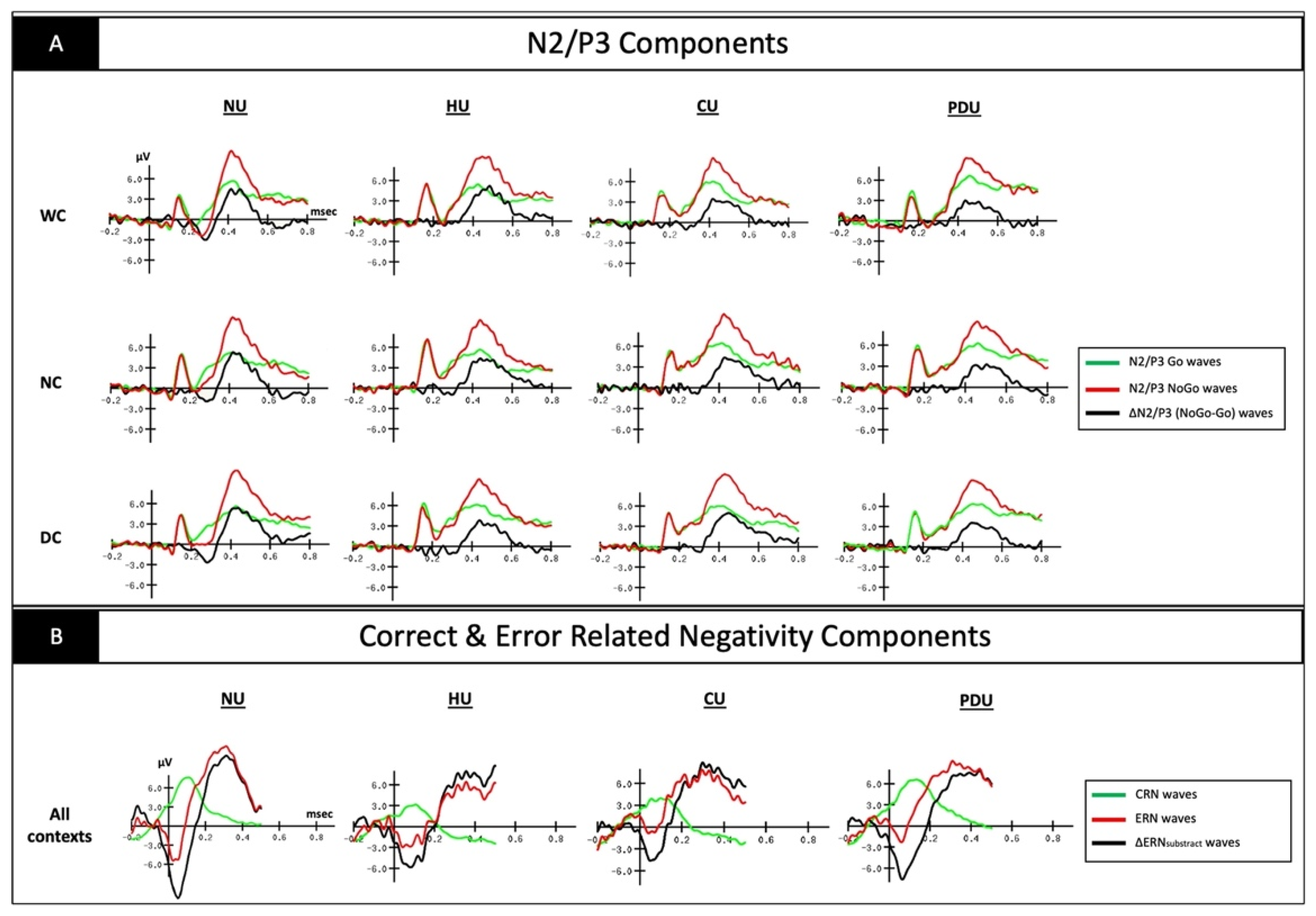
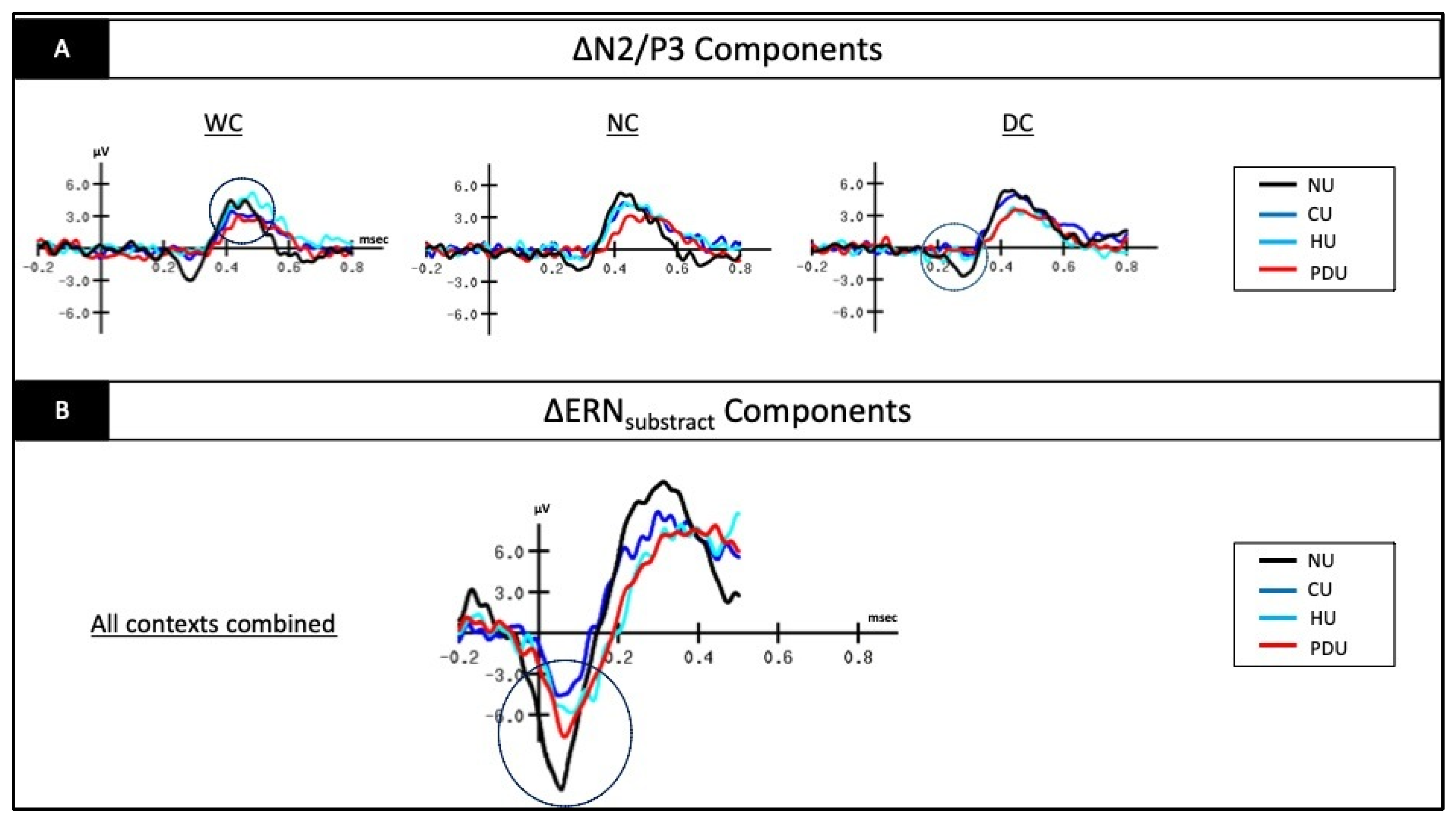
3.2. Electrophysiological Data on the ∆N2 Component
3.3. Electrophysiological Data on the ∆P3 Component
3.4. Electrophysiological Data on the ∆ERNsubtract Component
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aikins, R.D. From recreational to functional drug use: The evolution of drugs in American higher education, 1960–2014. Hist. Educ. 2015, 44, 25–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruisoto, P.; Contador, I. The role of stress in drug addiction. An integrative review. Physiol. Behav. 2019, 202, 62–68. [Google Scholar] [CrossRef]
- Ahmed, S.H.; Badiani, A.; Miczek, K.A.; Müller, C.P. Non-pharmacological factors that determine drug use and addiction. Neurosci. Biobehav. Rev. 2020, 110, 3–27. [Google Scholar] [CrossRef] [PubMed]
- World Drug Report; Technical Report No. E.21.XI.8; United Nations Publication: New York, NY, USA, 2021.
- Twillman, R.K.; Dawson, E.; LaRue, L.; Guevara, M.G.; Whitley, P.; Huskey, A. Evaluation of trends of near-real-time urine drug test results for methamphetamine, cocaine, heroin, and fentanyl. JAMA Netw. Open 2020, 3, e1918514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Serrano, M.J.; Pérez-García, M.; Perales, J.C.; Verdejo-García, A. Prevalence of executive dysfunction in cocaine, heroin and alcohol users enrolled in therapeutic communities. Eur. J. Pharmacol. 2010, 626, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Verdejo-Garcia, A.; Garcia-Fernandez, G.; Dom, G. Cognition and addiction. Dialogues Clin. Neurosci. 2022, 21, 281–290. [Google Scholar] [CrossRef]
- Zilverstand, A.; Huang, A.S.; Alia-Klein, N.; Goldstein, R.Z. Neuroimaging impaired response inhibition and salience attribution in human drug addiction: A systematic review. Neuron 2018, 98, 886–903. [Google Scholar] [CrossRef] [Green Version]
- Bechara, A.; Berridge, K.C.; Bickel, W.K.; Morón, J.A.; Williams, S.B.; Stein, J.S. A neurobehavioral approach to addiction: Implications for the opioid epidemic and the psychology of addiction. Psychol. Sci. Public Interest 2019, 20, 96–127. [Google Scholar] [CrossRef]
- Wiers, R.W.; Bartholow, B.D.; van den Wildenberg, E.; Thush, C.; Engels, R.C.; Sher, K.J.; Grenard, J.; Ames, S.L.; Stacy, A.W. Automatic and controlled processes and the development of addictive behaviors in adolescents: A review and a model. Pharmacol. Biochem. Behav. 2007, 86, 263–283. [Google Scholar] [CrossRef]
- Robinson, T.E.; Berridge, K.C. The neural basis of drug craving: An incentive-sensitization theory of addiction. Brain Res. Rev. 1993, 18, 247–291. [Google Scholar] [CrossRef]
- Robinson, T.E.; Berridge, K.C. Liking, wanting, and the incentive-sensitization theory of addiction. Am. Psychol. 2016, 71, 670. [Google Scholar]
- Campanella, S. Neurocognitive rehabilitation for addiction medicine: From neurophysiological markers to cognitive rehabilitation and relapse prevention. Prog. Brain Res. 2016, 244, 85–103. [Google Scholar]
- Goldstein, R.Z.; Volkow, N.D. Drug addiction and its underlying neurobiological basis: Neuroimaging evidence for the involvement of the frontal cortex. Am. J. Psychiatry 2002, 159, 1642–1652. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, R.Z.; Volkow, N.D. Dysfunction of the prefrontal cortex in addiction: Neuroimaging findings and clinical implications. Nat. Rev. Neurosci. 2011, 12, 652–669. [Google Scholar] [CrossRef]
- Leung, D.; Staiger, P.K.; Hayden, M.; Lum, J.A.; Hall, K.; Manning, V.; Verdejo-Garcia, A. Meta-analysis of the relationship between impulsivity and substance-related cognitive biases. Drug Alcohol Depend. 2017, 172, 21–33. [Google Scholar] [CrossRef]
- Luijten, M.; Machielsen, M.W.; Veltman, D.J.; Hester, R.; de Haan, L.; Franken, I.H. Systematic review of ERP and fMRI studies investigating inhibitory control and error processing in people with substance dependence and behavioural addictions. J. Psychiatry Neurosci. 2014, 39, 149–169. [Google Scholar] [CrossRef] [Green Version]
- Koob, G.F.; Volkow, N.D. Neurobiology of addiction: A neurocircuitry analysis. Lancet Psychiatry 2016, 3, 760–773. [Google Scholar] [CrossRef]
- Zilverstand, A.; Parvaz, M.A.; Moeller, S.J.; Goldstein, R.Z. Cognitive interventions for addiction medicine: Understanding the underlying neurobiological mechanisms. Prog. Brain Res. 2016, 224, 285–304. [Google Scholar]
- Verdejo-Garcia, A.; Lorenzetti, V.; Manning, V.; Piercy, H.; Bruno, R.; Hester, R.; Pennington, D.; Tolomeo, S.; Arunogiri, S.; Bates, M.E.; et al. A roadmap for integrating neuroscience into addiction treatment: A consensus of the neuroscience interest Group of the international society of addiction medicine. Front. Psychiatry 2019, 10, 877. [Google Scholar] [CrossRef]
- Noël, X.; Brevers, D.; Bechara, A. A triadic neurocognitive approach to addiction for clinical interventions. Front. Psychiatry 2013, 4, 179. [Google Scholar] [CrossRef] [Green Version]
- Bastiaansen, M.; Mazaheri, A.; Jensen, O. Beyond ERPs: Oscillatory Neuronal. Oxf. Handb. Event Relat. Potential Compon. 2011, 31–50. [Google Scholar]
- Campanella, S. Why it is time to develop the use of cognitive event-related potentials in the treatment of psychiatric diseases. Neuropsychiatr. Dis. Treat. 2013, 9, 1835–1845. [Google Scholar] [CrossRef] [PubMed]
- Moreno-López, L.; Stamatakis, E.A.; Fernández-Serrano, M.J.; Gómez-Río, M.; Rodríguez-Fernández, A.; Pérez-García, M.; Verdejo-García, A. Neural correlates of the severity of cocaine, heroin, alcohol, MDMA and cannabis use in polysubstance abusers: A resting-PET brain metabolism study. PLoS ONE 2012, 7, e39830. [Google Scholar] [CrossRef] [PubMed]
- Campanella, S.; Pogarell, O.; Boutros, N. Event-related potentials in substance use disorders: A narrative review based on articles from 1984 to 2012. Clin. EEG Neurosci. 2014, 45, 67–76. [Google Scholar] [CrossRef]
- Smith, J.L.; Mattick, R.P.; Jamadar, S.D.; Iredale, J.M. Deficits in behavioural inhibition in substance abuse and addiction: A meta-analysis. Drug Alcohol Depend. 2014, 145, 1–33. [Google Scholar] [CrossRef]
- European Monitoring Centre for Drugs and Drug Addiction. European Drug Report 2021: Statistical Bulletin; Publications Office of the European Union: Luxembourg, 2021.
- Khajehpour, H.; Mohagheghian, F.; Bakht, S.; Samadzadehaghdam, N.; Eqlimi, E.; Makkiabadi, B. Event-related potential correlates of biased cognitive processing and control in substance abusers: A review. Front. Biomed. Technol. 2019, 6, 41–63. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, WA, USA, 2013. [Google Scholar]
- Heimberg, R.G.; Horner, K.J.; Juster, H.R.; Safren, S.A.; Brown, E.J.; Schneier, F.R.; Liebowitz, M.R. Psychometric properties of the Liebowitz social anxiety scale. Psychol. Med. 1999, 29, 199–212. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Beck Depression Inventory (BDI-II); Pearson: London, UK, 1996. [Google Scholar]
- Spielberger, C.D. State-Trait Anxiety Inventory for Adults; Mind Garden: Menlo Park, CA, USA, 1983. [Google Scholar]
- Whiteside, S.P.; Lynam, D.R. Understanding the role of impulsivity and externalizing psychopathology in alcohol abuse: Application of the UPPS impulsive behavior scale. Exp. Clin. Psychopharmacol. 2003, 11, 210. [Google Scholar] [CrossRef]
- Caci, H.; Deschaux, O.; Baylé, F.J. Psychometric properties of the French versions of the BIS/BAS scales and the SPSRQ. Personal. Individ. Differ. 2007, 42, 987–998. [Google Scholar] [CrossRef]
- Hogue, A.; Dauber, S.; Morgenstern, J. Validation of a contemplation ladder in an adult substance use disorder sample. Psychol. Addict. Behav. 2010, 24, 137. [Google Scholar] [CrossRef] [Green Version]
- Daeppen, J.B.; Burnand, B.; Schnyder, C. Validation of the Addiction Severity Index in French-speaking alcoholic patients. J. Stud. Alcohol 1996, 57, 585–590. [Google Scholar] [CrossRef]
- Lecrubier, Y.; Sheehan, D.; Hergueta, T.; Weiller, E. The mini-international neuropsychiatric interview. Eur. Psychiatry 1998, 13, 198s. [Google Scholar] [CrossRef]
- Petit, G.; Kornreich, C.; Noël, X.; Verbanck, P.; Campanella, S. Alcohol-related context modulates performance of social drinkers in a visual Go/No-Go task: A preliminary assessment of event-related potentials. PLoS ONE 2012, 7, e37466. [Google Scholar] [CrossRef] [PubMed]
- Falkenstein, M.; Hoormann, J.; Hohnsbein, J. ERP components in go/nogo tasks and their relation to inhibition. Acta Psychol. 1999, 101, 267–291. [Google Scholar] [CrossRef]
- Klawohn, J.; Meyer, A.; Weinberg, A.; Hajcak, G. Methodological choices in event-related potential (ERP) research and their impact on internal consistency reliability and individual differences: An examination of the error-related negativity (ERN) and anxiety. J. Abnorm. Psychol. 2020, 129, 29. [Google Scholar] [CrossRef] [PubMed]
- Verdejo-García, A.J.; Perales, J.C.; Pérez-García, M. Cognitive impulsivity in cocaine and heroin polysubstance abusers. Addict. Behav. 2007, 32, 950–966. [Google Scholar] [CrossRef]
- Su, B.; Li, S.; Yang, L.; Zheng, M. Reduced response inhibition after exposure to drug-related cues in male heroin abstainers. Psychopharmacology 2020, 237, 1055–1062. [Google Scholar] [CrossRef]
- Yang, B.; Yang, S.; Zhao, L.; Yin, L.; Liu, X.; An, S. Event-related potentials in a Go/Nogo task of abnormal response inhibition in heroin addicts. Sci. China Ser. C Life Sci. 2009, 52, 780–788. [Google Scholar] [CrossRef]
- Morie, K.P.; Garavan, H.; Bell, R.P.; De Sanctis, P.; Krakowski, M.I.; Foxe, J.J. Intact inhibitory control processes in abstinent drug abusers (II): A high-density electrical mapping study in former cocaine and heroin addicts. Neuropharmacology 2014, 82, 151–160. [Google Scholar] [CrossRef]
- Su, B.; Wang, S.; Sumich, A.; Li, S.; Yang, L.; Cai, Y.; Wang, G.Y. Reduction in N2 amplitude in response to deviant drug-related stimuli during a two-choice oddball task in long-term heroin abstainers. Psychopharmacology 2017, 234, 3195–3205. [Google Scholar] [CrossRef] [Green Version]
- Donkers, F.C.; Van Boxtel, G.J. The N2 in go/no-go tasks reflects conflict monitoring not response inhibition. Brain Cogn. 2004, 56, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.N.; Ross, T.J.; Stein, E.A.; Garavan, H. Cingulate hypoactivity in cocaine users during a GO-NOGO task as revealed by event-related functional magnetic resonance imaging. J. Neurosci. 2003, 23, 7839–7843. [Google Scholar] [CrossRef] [Green Version]
- Franklin, T.R.; Acton, P.D.; Maldjian, J.A.; Gray, J.D.; Croft, J.R.; Dackis, C.A.; O’Brien, C.P.; Childress, A.R. Decreased gray matter concentration in the insular, orbitofrontal, cingulate, and temporal cortices of cocaine patients. Biol. Psychiatry 2002, 51, 134–142. [Google Scholar] [CrossRef]
- Goldstein, R.Z.; Bechara, A.; Garavan, H.; Childress, A.R.; Paulus, M.P.; Volkow, N.D. The neurocircuitry of impaired insight in drug addiction. Trends Cogn. Sci. 2009, 13, 372–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hester, R.; Luijten, M. Neural correlates of attentional bias in addiction. CNS Spectr. 2014, 19, 231–238. [Google Scholar] [CrossRef] [Green Version]
- Marhe, R.; Luijten, M.; Franken, I.H. The clinical relevance of neurocognitive measures in addiction. Front. Psychiatry 2014, 4, 185. [Google Scholar] [CrossRef] [Green Version]
- Forman, S.D.; Dougherty, G.G.; Casey, B.J.; Siegle, G.J.; Braver, T.S.; Barch, D.M.; Stenger, V.A.; Wick-Hull, C.; Pisarov, L.A.; Lorensen, E. Opiate addicts lack error-dependent activation of rostral anterior cingulate. Biol. Psychiatry 2004, 55, 531–537. [Google Scholar] [CrossRef]
- Franken, I.H.; van Strien, J.W.; Franzek, E.J.; van de Wetering, B.J. Error-processing deficits in patients with cocaine dependence. Biol. Psychol. 2007, 75, 45–51. [Google Scholar] [CrossRef]
- Lutz, M.C.; Kok, R.; Verveer, I.; Malbec, M.; Koot, S.; van Lier, P.A.; Franken, I.H. Diminished error-related negativity and error positivity in children and adults with externalizing problems and disorders: A meta-analysis on error processing. J. Psychiatry Neurosci. 2021, 46, 615–627. [Google Scholar] [CrossRef]
- Holroyd, C.B.; Coles, M.G. The neural basis of human error processing: Reinforcement learning, dopamine, and the error-related negativity. Psychol. Rev. 2002, 109, 679. [Google Scholar] [CrossRef]
- Garavan, H.; Stout, J.C. Neurocognitive insights into substance abuse. Trends Cogn. Sci. 2005, 9, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Volkow, N.D.; Wang, G.J.; Telang, F.; Fowler, J.S.; Logan, J.; Jayne, M.; Ma, Y.; Pradhan, K.; Wong, C. Profound decreases in dopamine release in striatum in detoxified alcoholics: Possible orbitofrontal involvement. J. Neurosci. 2007, 27, 12700–12706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volkow, N.D.; Fowler, J.S.; Wang, G.J. Imaging studies on the role of dopamine in cocaine reinforcement and addiction in humans. J. Psychopharmacol. 1999, 13, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Volkow, N.D.; Fowler, J.S.; Wang, G.J. The addicted human brain viewed in the light of imaging studies: Brain circuits and treatment strategies. Neuropharmacology 2004, 47, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Ceceli, A.O.; Bradberry, C.W.; Goldstein, R.Z. The neurobiology of drug addiction: Cross-species insights into the dysfunction and recovery of the prefrontal cortex. Neuropsychopharmacology 2022, 47, 276–291. [Google Scholar] [CrossRef]
- Suchting, R.; Beard, C.L.; Schmitz, J.M.; Soder, H.E.; Yoon, J.H.; Hasan, K.M.; Narayana, P.A.; Lane, S.D. A meta-analysis of tract-based spatial statistics studies examining white matter integrity in cocaine use disorder. Addict. Biol. 2021, 26, e12902. [Google Scholar] [CrossRef]
- Kloppenborg, R.P.; Nederkoorn, P.J.; Geerlings, M.I.; van den Berg, E. Presence and progression of white matter hyperintensities and cognition: A meta-analysis. Neurology 2014, 82, 2127–2138. [Google Scholar] [CrossRef] [Green Version]
- Lyoo, I.K.; Streeter, C.C.; Ahn, K.H.; Lee, H.K.; Pollack, M.H.; Silveri, M.M.; Nassar, L.; Levin, J.M.; Sarid-Segal, O.; Ciraulo, D.A.; et al. White matter hyperintensities in subjects with cocaine and opiate dependence and healthy comparison subjects. Psychiatry Res. Neuroimaging 2004, 131, 135–145. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Non-Users Healthy Controls n = 19 | Heroin-Users n = 21 | Cocaine-Users n = 23 | Polydrug-Users n = 19 | Statistical Data | Post-Hoc Analyses | ||
|---|---|---|---|---|---|---|---|
| Demographical and clinical data | Gender (male:female) | 13:6 | 16:5 | 21:2 | 17:2 | χ2(12) = 16.342; p = 0.176 | NA |
| Education (number of years) | 11.32 ± 2.98 | 9.29 ± 2.83 | 10.91 ± 2.98 | 9.47 ± 3.20 | F(3,78) = 2.325; p = 0.081 | NA | |
| Age | 37.89 ± 11.49 | 41.14 ± 9.01 | 36.83 ± 6.62 | 39.11 ± 8.85 | F(3,78 ) = 0.903; p = 0.444 | NA | |
| Drug consumption among family members (none:extended family:close family) | 15:3:1 | 13:3:5 | 15:1:7 | 9:2:8 | χ2(6) = 8.374; p = 0.212 | NA | |
| Alcohol consumption among family members (none:extended family:close family) | 16:3:0 | 6:7:8 | 14:2:7 | 9:2:8 | χ²(6) = 18.136; p = 0.006 ** | NU < HU = CU = PDU | |
| Number of past treatment programs | NA | 2.00 ± 2.65 | 1.13 ± 2.36 | 1.37 ± 2.03 | F(2,60) = 0.776; p = 0.465 | NA | |
| Psychological questionnaires | BDI-II | 5.37 ± 8.31 | 16.29 ± 8.41 | 19.14 ± 12.35 | 20.63 ± 8.60 | F(3,78) = 9.831; p < 0.001 *** | NU < HU = CU = PDU |
| STAI-state A | 44.21 ± 11.21 | 51.52 ± 10.97 | 58.00 ± 9.55 | 52.79 ± 9.05 | F(3,78) = 6.242; p < 0.001*** | NU < CU | |
| STAI-trait B | 41.84 ± 9.45 | 53.24 ± 10.23 | 56.68 ± 9.55 | 54.89 ± 9.56 | F(3,78) = 9.303; p < 0.001 *** | NU < HU = CU = PDU | |
| FNE | 10.63 ± 6.08 | 14.90 ± 5.87 | 17.95 ± 6.13 | 14.68 ± 5.13 | F(3,78) = 5.373; p = 0.002 ** | NU < CU | |
| BIS | 17.26 ± 5.22 | 19.57 ± 2.31 | 20.68 ± 3.40 | 20.11 ± 2.47 | F(3,78) = 3.588; p = 0.017 * | NU < CU | |
| BAS drive | 8.84 ± 2.50 | 9.00 ± 2.49 | 11.41 ± 2.84 | 10.32 ± 2.58 | F(3,78) = 4.470; p = 0.006 ** | NU < CU | |
| BAS fun seeking | 11.79 ± 1.47 | 11.81 ± 1.86 | 12.64 ± 2.17 | 12.47 ± 2.06 | F(3,78) = 1.084; p = 0.361 | NA | |
| BAS reward responsiveness | 15.95 ± 2.55 | 17.38 ± 2.27 | 17.18 ± 2.01 | 17.47 ± 1.71 | F(3,78) = 2.085; p = 0.109 | NA | |
| UPPS Total | 103.32 ± 13.90 | 103.29 ± 8.38 | 107.82 ± 20.97 | 102.16 ± 13.81 | F(3,78) = 0.584; p = 0.627 | NA | |
| Urgency | 30.89 ± 8.23 | 30.38 ± 4.21 | 30.55 ± 8.66 | 28.79 ± 6.10 | F(3,78) = 0.338; p = 0.798 | NA | |
| Lack of premeditation | 22.41 ± 6.09 | 21.29 ± 4.55 | 25.50 ± 6.06 | 21.32 ± 4.77 | F(3,78) = 2.861; p = 0.042 * | NU = HU = CU = PDU | |
| Lack of perseverance | 21.74 ± 4.77 | 21.67 ± 3.89 | 21.86 ± 3.94 | 21.53 ± 3.47 | F(3,78) = 0.025; p = 0.995 | NA | |
| Sensation seeking | 27.85 ± 9.02 | 30.19 ± 6.67 | 28.36 ± 10.57 | 30.53 ± 9.44 | F(3,78) = 0.424; p = 0.736 | NA | |
| Ladder | NA | 8.10 ± 8.95 | 8.45 ± 1.22 | 7.95 ± 1.35 | F(2,60) = 0.693; p = 0.504 | NA | |
| ∆Craving(pre-post) | NA | −0.45 ± 2.77 | 0.12 ± 2.04 | 0.00 ± 0.82 | F(2,60) = 0.456; p = 0.636 | NA | |
| A.S.I | Medical status | 0.74 ± 1.63 | 1.90 ± 1.95 | 1.96 ± 1.85 | 2.26 ± 2.18 | F(3,78) = 2.376; p = 0.076 | NA |
| Employment and support | 0.95 ± 2.07 | 4.10 ± 2.84 | 2.87 ± 2.24 | 4.47 ± 2.34 | F(3,78) = 8.466; p < 0.001 *** | NU < HU = CU | |
| Drug use | 0.00 ± 0.00 | 7.48 ± 1.25 | 7.61 ± 1.23 | 7.89 ± 1.05 | F(3,78) = 263.45; p < 0.001 *** | NU < HU = CU = PDU | |
| Legal status | 0.00 ± 0.00 | 2.67 ± 2.56 | 2.48 ± 2.69 | 4.00 ± 2.54 | F(3,78) = 10.17; p < 0.001 *** | NU < HU = CU = PDU | |
| Family/social status | 0.53 ± 0.84 | 3.62 ± 2.76 | 3.52 ± 2.21 | 4.53 ± 2.50 | F(3,78) = 11.73; p < 0.001 *** | NU < HU = CU = PDU | |
| Psychiatric status | 0.53 ± 1.61 | 3.81 ± 2.84 | 5.30 ± 2.36 | 4.53 ± 1.90 | F(3,78) = 17.31; p < 0.001 *** | NU < HU = CU = PDU | |
| M.I.N.I | Major depressive episode (MDE) (none:past:current) | 16:3:0 | 9:9:3 | 7:10:6 | 5:11:3 | χ²(6) = 18.297; p = 0.006 * | NU < HU = CU = PDU |
| MDE with melancholic features (none:current) | 19:0 | 19:2 | 20:3 | 16:3 | χ2(3) = 3.123; p = 0.373 | NA | |
| Dysthymia (none:current) | 19:0 | 17:4 | 20:3 | 18:1 | χ2(3) = 4.831; p = 0.185 | NA | |
| Suicidality (none:medium risk:high risk) | 18:1:0 | 14:5:2 | 16:4:2 | 6:8:5 | χ2(6) = 18.093; p = 0.006 * | NU < HU = CU = PDU | |
| Manic episode (none:current) | 19:0 | 19:2 | 19:4 | 16:3 | χ2(3) = 6.974; p = 0.323 | NA | |
| Panic disorder (none:current) | 19:0 | 19:2 | 20:3 | 18:1 | χ2(3) = 2.881; p = 0.410 | NA | |
| Agoraphobia (none:current) | 18:1 | 20:1 | 20:3 | 15:4 | χ2(3) = 3.540; p = 0.316 | NA | |
| Social phobia (none:current) | 18:1 | 18:3 | 20:3 | 17:2 | χ2(3) = 0.975; p = 0.807 | NA | |
| Post Traumatic Stress Disorder (none: current) | 19:0 | 20:1 | 19:4 | 16:3 | χ2(3) = 4.957; p = 0.175 | NA | |
| Alcohol abuse (none:current) | 19:0 | 17:4 | 8:15 | 12:7 | χ2(3) = 22.534; p < 0.001 *** | NU < CU | |
| Generalized anxiety disorder (none: current) | 18:1 | 12:9 | 16:7 | 12:7 | χ2(3) = 7.703; p = 0.053 | NA | |
| Non-Users Healthy Controls n = 19 | Heroin-Users n = 21 | Cocaine-Users n = 23 | Polydrug-Users n = 19 | Statistical Data Group * Context Interaction Group Effect Context Effect | Post-Hoc Analyses | ||
|---|---|---|---|---|---|---|---|
| Commission error rates (%) | WC | 10.16 ± 7.52 | 24.94 ± 20.28 | 17.95 ± 12.10 | 24.14 ± 12.25 | F(5.6,146.6) = 0.970; p = 0.445 F(3,78) = 4.390; p = 0.007 ** F(1.9,146.6) = 2.800; p = 0.067 | NA NU = CU < HU = PDU NA |
| NC | 10.99 ± 7.28 | 22.86 ± 17.37 | 19.67 ± 15.52 | 25.80 ± 12.34 | |||
| DC | 10.66 ± 6.91 | 20.95 ± 17.90 | 16.58 ± 14.25 | 23.42 ± 11.81 | |||
| Total | 10.60 ± 6.78 | 22.92 ± 17.95 | 18.07 ± 13.24 | 24.46 ± 11.01 | |||
| Ommission error rates (%) | WC | 98.44 ± 2.60 | 96.34 ± 4.69 | 95.27 ± 10.43 | 96.26 ± 5.37 | F(4.1,108.0) = 0.843; p = 0.505 F(3,78) = 1.864; p = 0.143 F(1.4,108.0) = 2.463; p = 0.108 | NA NA NA |
| NC | 99.01 ± 2.22 | 96.54 ± 4.12 | 98.20 ± 2.09 | 96.97 ± 4.21 | |||
| DC | 99.43 ± 0.73 | 96.03 ± 6.04 | 97.82 ± 2.80 | 97.68 ± 3.12 | |||
| Total | 98.96 ± 1.72 | 96.30 ± 4.25 | 97.10 ± 4.18 | 96.97 ± 3.83 | |||
| Reaction times (ms) | WC | 370.11 ± 63.52 | 413.33 ± 68.55 | 381.50 ± 54.50 | 388.00 ± 70.18 | F(4.6,120.2) = 0.845; p = 0.513 F(3,78) = 1.526; p = 0.214 F(1.5,120.2) = 2.607; p = 0.092 | NA NA NA |
| NC | 376.51 ± 91.23 | 400.64 ± 70.38 | 373.15 ± 52.76 | 379.24 ± 55.16 | |||
| DC | 355.47 ± 53.12 | 400.00 ± 53.27 | 374.39 ± 56.67 | 382.10 ± 56.80 | |||
| Total | 367.37 ± 58.51 | 404.66 ± 61.82 | 376.35 ± 53.52 | 383.11 ± 59.28 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dousset, C.; Chenut, C.; Kajosch, H.; Kornreich, C.; Campanella, S. Comparison of Neural Correlates of Reactive Inhibition in Cocaine, Heroin, and Polydrug Users through a Contextual Go/No-Go Task Using Event-Related Potentials. Biology 2022, 11, 1029. https://doi.org/10.3390/biology11071029
Dousset C, Chenut C, Kajosch H, Kornreich C, Campanella S. Comparison of Neural Correlates of Reactive Inhibition in Cocaine, Heroin, and Polydrug Users through a Contextual Go/No-Go Task Using Event-Related Potentials. Biology. 2022; 11(7):1029. https://doi.org/10.3390/biology11071029
Chicago/Turabian StyleDousset, Clémence, Christie Chenut, Hendrik Kajosch, Charles Kornreich, and Salvatore Campanella. 2022. "Comparison of Neural Correlates of Reactive Inhibition in Cocaine, Heroin, and Polydrug Users through a Contextual Go/No-Go Task Using Event-Related Potentials" Biology 11, no. 7: 1029. https://doi.org/10.3390/biology11071029