
SERPINE1 rs6092 Variant Is Related to Plasma Coagulation Proteins in Patients with Severe COVID-19 from a Tertiary Care Hospital

 , , ,
, , ,  , , , ,
, , , ,  , , ,
, , ,  add
Show full author list
add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Genetic Analysis
2.2. Coagulation Proteins Determination
2.3. Statistical Analysis
3. Results
3.1. Genetic Association Study with COVID-19 Severity
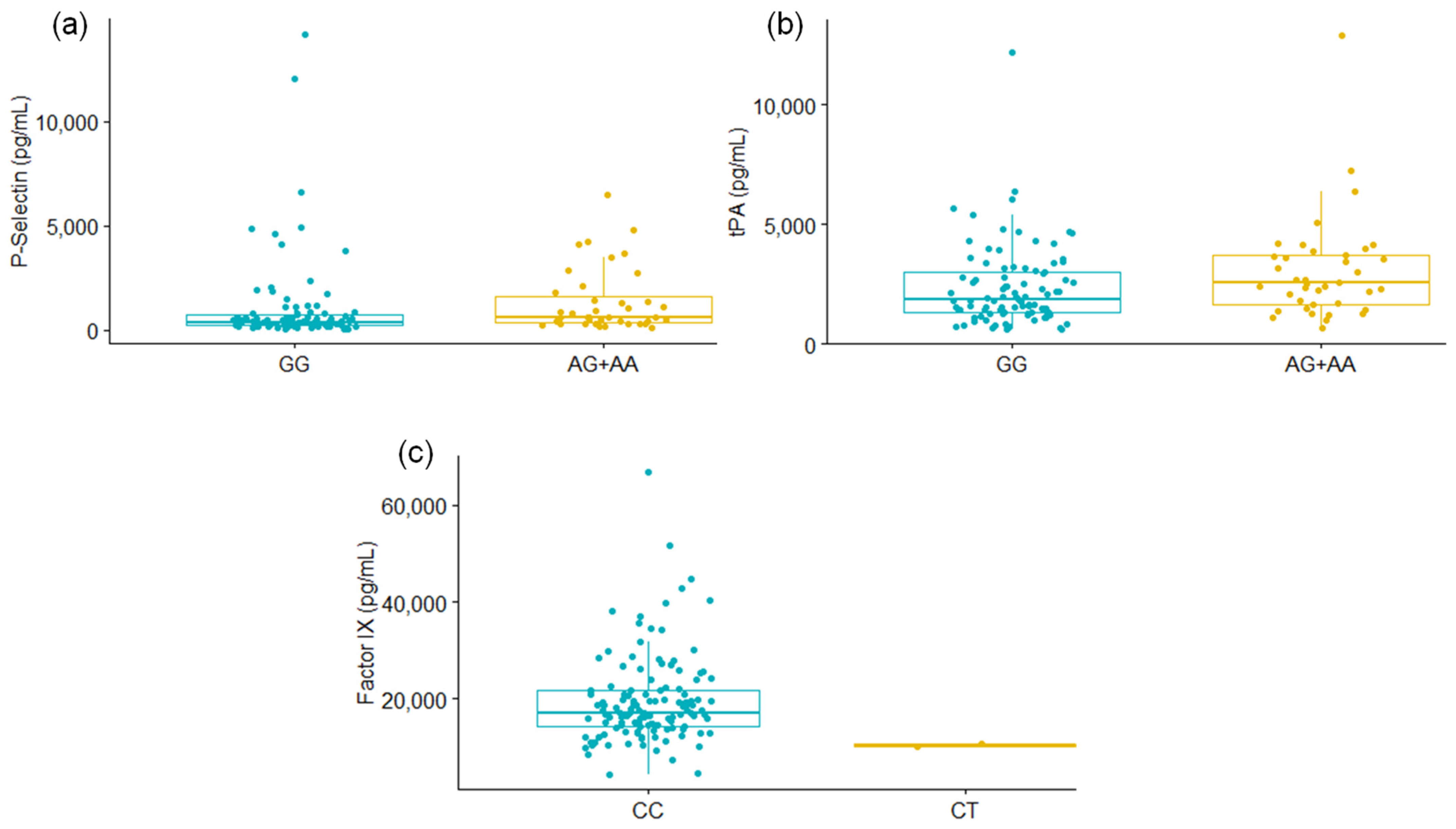
3.2. Levels of PSGL-1 and tPA Were Different According to SERPINE1 rs6092 Genotypes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 9 November 2021).
- Baj, J.; Karakuła-Juchnowicz, H.; Teresiński, G.; Buszewicz, G.; Ciesielka, M.; Sitarz, E.; Forma, A.; Karakuła, K.; Flieger, W.; Portincasa, P.; et al. COVID-19: Specific and Non-Specific Clinical Manifestations and Symptoms: The Current State of Knowledge. J. Clin. Med. 2020, 9, 1753. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19 Clinical Management: Living Guidance. 2021. Available online: https://www.who.int/publications/i/item/clinical-management-of-COVID-19 (accessed on 11 October 2021).
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases from the Chinese Center for Disease Control and Prevention. JAMA Am. Med. Assoc. 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Huang, D.Q.; Zou, B.; Yang, H.; Hui, W.Z.; Rui, F.; Yee, N.T.S.; Liu, C.; Nerurkar, S.N.; Kai, J.C.Y.; et al. Epidemiology of COVID-19: A systematic review and meta-analysis of clinical characteristics, risk factors, and outcomes. J. Med. Virol. 2021, 93, 1449–1458. [Google Scholar] [CrossRef] [PubMed]
- Da Rosa Mesquita, R.; Francelino Silva Junior, L.C.; Santos Santana, F.M.; Farias de Oliveira, T.; Campos Alcântara, R.; Monteiro Arnozo, G.; Rodrigues da Silva Filho, E.; Galdino dos Santos, A.G.; Oliveira da Cunha, E.J.; Salgueiro de Aquino, S.H.; et al. Clinical manifestations of COVID-19 in the general population: Systematic review. Wien. Klin. Wochenschr. 2021, 133, 377–382. [Google Scholar] [CrossRef]
- Chen, J.; Qi, T.; Liu, L.; Ling, Y.; Qian, Z.; Li, T.; Li, F.; Xu, Q.; Zhang, Y.; Xu, S.; et al. Clinical progression of patients with COVID-19 in Shanghai, China. J. Infect. 2020, 80, e1–e6. [Google Scholar] [CrossRef]
- Berlin, D.A.; Gulick, R.M.; Martinez, F.J. Severe COVID-19. N. Engl. J. Med. 2020, 383, 2451–2460. [Google Scholar] [CrossRef]
- Oliveira, E.; Parikh, A.; Lopez-Ruiz, A.; Carrilo, M.; Goldberg, J.; Cearras, M.; Fernainy, K.; Andersen, S.; Mercado, L.; Guan, J.; et al. ICU outcomes and survival in patients with severe COVID-19 in the largest health care system in central Florida. PLoS ONE 2021, 16, e0249038. [Google Scholar] [CrossRef]
- Mohamed, M.F.; Al-Shokri, S.D.; Shunnar, K.M.; Mohamed, S.F.; Najim, M.S.; Ibrahim, S.I.; Elewa, H.; Abdalla, L.O.; El-Bardissy, A.; Elshafei, M.N.; et al. Prevalence of Venous Thromboembolism in Critically Ill COVID-19 Patients: Systematic Review and Meta-Analysis. Front. Cardiovasc. Med. 2021, 7, 598846. [Google Scholar] [CrossRef]
- Wu, C.; Liu, Y.; Cai, X.; Zhang, W.; Li, Y.; Fu, C. Prevalence of Venous Thromboembolism in Critically Ill Patients With Coronavirus Disease 2019: A Meta-Analysis. Front. Med. 2021, 8, 603558. [Google Scholar] [CrossRef]
- Liu, Y.; Cai, J.; Wang, C.; Jin, J.; Qu, L. Incidence, prognosis, and laboratory indicators of venous thromboembolism in hospitalized patients with coronavirus disease 2019: A systematic review and meta-analysis. J. Vasc. Surg. Venous Lymphat. Disord. 2021, 9, 1099–1111. [Google Scholar] [CrossRef]
- Franco, R.F.; Reitsma, P.H. Genetic risk factors of venous thrombosis. Hum. Genet. 2001, 109, 369–384. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Gohil, R. Genetic risk factors for venous thrombosis: The end of the beginning? Expert Rev. Cardiovasc. Ther. 2010, 8, 11–13. [Google Scholar] [CrossRef] [PubMed]
- Skille, H.; Paulsen, B.; Hveem, K.; Gabrielsen, M.E.; Brumpton, B.; Hindberg, K.; Gran, O.V.; Rosendaal, F.R.; Brækkan, S.K.; Hansen, J.B. Combined effects of five prothrombotic genotypes and cancer on the risk of a first venous thromboembolic event. J. Thromb. Haemost. 2020, 18, 2861–2869. [Google Scholar] [CrossRef] [PubMed]
- Rinde, L.B.; Morelli, V.M.; Småbrekke, B.; Mathiesen, E.B.; Løchen, M.L.; Njølstad, I.; Wilsgaard, T.; Smith, E.; Rosendaal, F.R.; Frazer, K.A.; et al. Effect of prothrombotic genotypes on the risk of venous thromboembolism in patients with and without ischemic stroke. The Tromsø Study. J. Thromb. Haemost. 2019, 17, 749–758. [Google Scholar] [CrossRef]
- Jeon, Y.J.; Kim, Y.R.; Lee, B.E.; Choi, Y.S.; Kim, J.H.; Shin, J.E.; Rah, H.; Cha, S.H.; Lee, W.S.; Kim, N.K. Genetic association of five plasminogen activator inhibitor-1 (PAI-1) polymorphisms and idiopathic recurrent pregnancy loss in Korean women. Thromb. Haemost. 2013, 110, 742–750. [Google Scholar]
- Lam, W.; Moosavi LPhysiology Factor, V. StatPearls (Internet); StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Cesari, M.; Pahor, M.; Incalzi, R. Plasminogen activator inhibitor (PAI-1): A key factor linkin fibrinolysis and age-related subclinical and clinical conditions. Cardiovasc Ther. 2010, 28, e72–e91. [Google Scholar] [CrossRef] [Green Version]
- Comité-Interinstitucional. Guía Clínica Para el Tratamiento de la COVID-19 en México; Mexican Government: Mexico City, Mexico, 2021.
- Purcell, S.; Neale, B.; Todd-Brown, K.; Thomas, L.; Ferreira, M.A.; Bender, D.; Maller, J.; Sklar, P.; De Bakker, P.I.; Daly, M.J.; et al. PLINK: A toolset for whole-genome association and population-based linkage analysis. Am. J. Hum. Genet. 2007, 81, 559–575. [Google Scholar] [CrossRef] [Green Version]
- RStudio Team. RStudio: Integrated Development for R; Rstudio, PBC: Boston, MA, USA, 2020; Available online: http://www.rstudio.com/ (accessed on 10 September 2021).
- Fricke-Galindo, I.; Falfán-Valencia, R. Genetics Insight for COVID-19 Susceptibility and Severity: A Review. Front. Immunol. 2021, 12, 622176. [Google Scholar] [CrossRef]
- Abu-Farha, M.; Al-Sabah, S.; Hammad, M.M.; Hebbar, P.; Channanath, A.M.; John, S.E.; Taher, I.; Almaeen, A.; Ghazy, A.; Mohammad, A.; et al. Prognostic Genetic Markers for Thrombosis in COVID-19 Patients: A Focused Analysis on D-Dimer, Homocysteine and Thromboembolism. Front. Pharmacol. 2020, 11, 587451. [Google Scholar] [CrossRef]
- Dolan, M.E.; Hill, D.P.; Mukherjee, G.; Mcandrews, M.S.; Chesler, E.J.; Blake, J.A. Investigation of COVID-19 comorbidities reveals genes and pathways coincident with the SARS-CoV-2 viral disease. Sci. Rep. 2020, 10, 20848. [Google Scholar] [CrossRef]
- Vlieg, A.V.H.; Callas, P.W.; Cushman, Z.M.; Bertinay, R.M.; Rosendaal, F.R. Inter-relation of coagulation factors and D-dimer levels in healthy individuals. J. Thromb. Haemost. 2003, 1, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Van Hylckama Vlieg, A.; Van Der Linden, I.K.; Bertina, R.M.; Rosendaal, F.R. High levels of factor IX increase the risk of venous thrombosis. Blood J. Am. Soc. Hematol. 2000, 95, 3678–3682. [Google Scholar]
- Lowe, G.D.O. Factor IX and thrombosis. Br. J. Haematol. 2001, 115, 507–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, N.; Srinivasan, J.K.; Priya, M.H.; Sibiya, V. Role of Serpine gene polymorphism in recurrent implantation failure and preeclampsia. J. Hum. Reprod. Sci. 2017, 10, 135–137. [Google Scholar] [CrossRef] [PubMed]
- Fan, Q.; Li, H.; Qin, Y.; Li, L.; Chen, L.; Zhang, L.; Lv, Y.; Liang, D.; Liang, Y.; Long, T.; et al. Association of SERPINE1 rs6092 with type 2 diabetes and related metabolic traits in a Chinese population. Gene 2018, 661, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Garte, S.; Gaspari, L.; Alexandrie, A.K.; Ambrosone, C.; Autrup, H.; Autrup, J.L.; Baranova, H.; Bathum, L.; Benhamou, S.; Boffetta, P.; et al. Metabolic gene polymorphism frequencies in control populations. Cancer Epidemiol. Biomark. Prev. 2001, 10, 1239–1248. [Google Scholar]
- Tjärnlund-Wolf, A.; Brogren, H.; Lo, E.H.; Wang, X. Plasminogen activator inhibitor-1 and thrombotic cerebrovascular diseases. Stroke 2012, 43, 2833–2839. [Google Scholar] [CrossRef]
- Aref, S.; Sakrana, M.; Hafez, A.A.; Hamdy, M. Soluble P-selectin levels in Diabetes mellitus patients with coronary artery disease. Hematology 2005, 10, 183–187. [Google Scholar] [CrossRef]
- Goshua, G.; Pine, A.B.; Meizlish, M.L.; Chang, C.H.; Zhang, H.; Bahel, P.; Baluha, A.; Bar, N.; Bona, R.D.; Burns, A.J.; et al. Endotheliopathy in COVID-19-associated coagulopathy: Evidence from a single-centre, cross-sectional study. Lancet Haematol. 2020, 7, e575–e582. [Google Scholar] [CrossRef]
- Karsli, E.; Sabirli, R.; Altintas, E.; Canacik, O.; Sabirli, G.T.; Kaymaz, B.; Kurt, Ö.; Koseler, A. Soluble P-selectin as a potential diagnostic and prognostic biomarker for COVID-19 disease: A case-control study. Life Sci. 2021, 277, 119634. [Google Scholar] [CrossRef]
- de Sá, M.C.; de Medeiros, F.A.; Iriyoda, T.M.V.; Costa, N.T.; Alfieri, D.F.; Flauzino, T.; Sekiguchi, B.A.; Lozovoy, M.A.B.; Reiche, E.M.V.; Maes, M.; et al. Cell adhesion molecules and plasminogen activator inhibitor type-1 (PAI-1) in patients with rheumatoid arthritis: Influence of metabolic syndrome. Clin. Exp. Med. 2018, 18, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Samprathi, M.; Jayashree, M. Biomarkers in COVID-19: An Up-To-Date Review. Front. Pediatr. 2021, 8, 607647. [Google Scholar] [CrossRef] [PubMed]
- Dabbagh, D.; He, S.; Hetrick, B.; Chilin, L.; Andalibi, A.; Wu, Y. Identification of the shrek family of proteins as broad-spectrum host antiviral factors. Viruses 2021, 13, 832. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Waheed, A.A.; Hetrick, B.; Dabbagh, D.; Akhrymuk, I.V.; Kehn-Hall, K.; Freed, E.O.; Wu, Y. Psgl-1 inhibits the incorporation of SARS-CoV and SARS-CoV-2 spike glycoproteins into pseudovirions and impairs pseudovirus attachment and infectivity. Viruses 2021, 13, 46. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.L.; Deng, H.F.; Tan, C.Y.; Xiao, Z.H.; Liu, M.D.; Liu, K.; Zhang, H.L.; Xiao, X.Z. The role of PSGL-1 in pathogenesis of systemic inflammatory response and coagulopathy in.n endotoxemic mice. Thromb. Res. 2019, 182, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Jamaly, S.; Basavaraj, M.G.; Starikova, I.; Olsen, R.; Brækkan, S.K.; Hansen, J.B. Elevated plasma levels of P-selectin glycoprotein ligand-1-positive microvesicles in patients with unprovoked venous thromboembolism. J. Thromb. Haemost. 2018, 16, 1546–1554. [Google Scholar] [CrossRef] [PubMed]
- Whyte, C.S.; Morrow, G.B.; Mitchell, J.L.; Chowdary, P.; Mutch, N.J. Fibrinolytic abnormalities in acute respiratory distress syndrome (ARDS) and versatility of thrombolytic drugs to treat COVID-19. J. Thromb. Haemost. 2020, 18, 1548–1555. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Y.; Warnock, M.; Harbaugh, A.; Yalavarthi, S.; Gockman, K.; Zuo, M.; Madison, J.A.; Knight, J.S.; Kanthi, Y.; Lawrence, D.A. Plasma tissue plasminogen activator and plasminogen activator inhibitor-1 in hospitalized COVID-19 patients. Sci. Rep. 2021, 11, 1580. [Google Scholar] [CrossRef]
- Cugno, M.; Meroni, P.L.; Gualtierotti, R.; Griffini, S.; Grovetti, E.; Torri, A.; Lonati, P.; Grossi, C.; Borghi, M.O.; Novembrino, C.; et al. Complement activation and endothelial perturbation parallel COVID-19 severity and activity. J. Autoimmun. 2021, 116, 102560. [Google Scholar] [CrossRef]
- Wang, J.; Hajizadeh, N.; Moore, E.E.; McIntyre, R.C.; Moore, P.K.; Veress, L.A.; Yaffe, M.B.; Moore, H.B.; Barrett, C.D. Tissue plasminogen activator (tPA) treatment for COVID-19 associated acute respiratory distress syndrome (ARDS): A case series. J. Thromb. Haemost. 2020, 18, 1752–1755. [Google Scholar] [CrossRef]
- Ruberto, F.; Chistolini, A.; Curreli, M.; Frati, G.; Marullo, A.G.; Biondi-Zoccai, G.; Mancone, M.; Sciarretta, S.; Miraldi, F.; Alessandri, F.; et al. Von Willebrand factor with increased binding capacity is associated with reduced platelet aggregation but enhanced agglutination in COVID-19 patients: Another COVID-19 paradox? J. Thromb. Thrombolysis. 2021, 52, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, W. Thromboinflammation in COVID-19 acute lung injury. Paediatr. Respir. Rev. 2020, 35, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Wool, G.D.; Miller, J.L. The Impact of COVID-19 Disease on Platelets and Coagulation. Pathobiology 2021, 88, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Cardinal-Fernández, P.; Cuesta, E.G.; Barberán, J.; Varona, J.F.; Estirado, A.; Moreno, A.; Villanueva, J.; Villareal, M.; Baez-Pravia, O.; Menéndez, J.; et al. Clinical characteristics and outcomes of 1331 patients with COVID-19: HM Spanish Cohort. Rev. Española Quimioter. 2021, 34, 342–352. [Google Scholar] [CrossRef]
- Zhan, X.Y.; Li, L.; Hu, Y.; Li, Q.; Kong, H.; Ng, M.H.; Chen, C.; He, Y.; Huang, B.; Yang, M. Elderly Male With Cardiovascular-Related Comorbidities Has a Higher Rate of Fatal Outcomes: A Retrospective Study in 602 Patients With Coronavirus Disease 2019. Front. Cardiovasc. Med. 2021, 8, 680604. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All (n = 455) | IMV (n = 331) | Non-IMV (n = 124) | p-Value * | |
|---|---|---|---|---|
| Age, yr | 58 [49–67] | 58 [49–68] | 56 [48–65.3] | 0.188 |
| Gender, F/M n (%) | 144 (31.6)/311 (68.4) | 98 (29.6)/233 (70.4) | 46 (37.1)/78 (62.9) | 0.141 |
| BMI, kg/m2 | 29.7 [26.1–33.1] | 29.9 [26.5–33.1] | 28.9 [25.8–33.1] | 0.466 |
| Smoking, n (%) | 117 (25.7) | 83 (25.1) | 34 (27.4) | 0.697 |
| Hospitalization Days | 18 [12–30] | 21 [16–35] | 11 [8.3–15] | <0.001 |
| Symptoms Onset, days | 9 [7–12] | 9 [7–13] | 9 [6–11] | 0.236 |
| Diabetes, n (%) | 138 (30.3) | 106 (32.0) | 32 (25.8) | 0.200 |
| Hypertension, n (%) | 152 (33.4) | 110 (33.2) | 42 (33.9) | 1.000 |
| Leukocyte, [109/L] | 9.6 [7.2–12.9] | 10.6 [7.7–13.7] | 7.9 [5.9–9.9] | <0.001 |
| Lymphocyte, [109/L] | 0.7 [0.5–1.2] | 0.7 [0.5–1.2] | 0.8 [0.6–1.2] | 0.095 |
| Platelets, [109/L] | 280 [214–356] | 273 [210.8–343.2] | 307 [226.8–393] | 0.018 |
| IMV Days | 10 [0–21] | 18 [11–28.5] | NA | NA |
| PaO2/FiO2 | 166 [114–214] | 149 [103–193.2] | 213.5 [165.8–248.0] | <0.001 |
| Protein (pg/mL) | IMV (n = 94) | Non-IMV (n = 37) | p-Value * |
|---|---|---|---|
| P-Selectin | 415 [221–1004] | 533 [291–837] | 0.3225 |
| D-dimer | 586 [313–1140] | 355 [261–534] | 0.0156 |
| PSGL-1 | 6016 [5083–7175] | 5058 [4612–6414] | 0.0210 |
| tPA | 2309 [1502–3620] | 1517 [1274–2395] | 0.0044 |
| PAI-1 | 81,326 [73,927–88,980] | 76,344 [72,747–80,737] | 0.0122 |
| Factor IX | 17,956 [14,651–22,189] | 15,821 [12,710–18,935] | 0.0365 |
| Variants | All (n = 455) | IMV (n = 331) | Non-IMV (n = 124) | p-Value * |
|---|---|---|---|---|
| F5 rs6025 | ||||
| CC | 453 (0.996) | 329 (0.994) | 124 (1.000) | 1.000 |
| CT | 2 (0.004) | 2 (0.006) | 0 | |
| C | 908 (0.998) | 660 (0.997) | 248 (1.000) | 1.000 |
| T | 2 (0.002) | 2 (0.003) | 0 | |
| SERPINE1 rs6092 | ||||
| GG | 400 (0.879) | 290 (0.876) | 110 (0.887) | 0.632 |
| AG | 54 (0.119) | 40 (0.121) | 14 (0.113) | |
| AA | 1 (0.002) | 1 (0.003) | 0 | |
| G | 854 (0.938) | 620 (0.937) | 234 (0.943) | 0.876 |
| A | 56 (0.061) | 42 (0.063) | 14 (0.057) | |
| Protein (pg/mL) | SERPINE1 rs6092 | p-Value * | |
| GG (n = 92) | AG+AA (n = 39) | ||
| P-Selectin | 385 [215–720] | 632.3 [358–1617] | 0.0037 |
| D-dimer | 508 [275–1020] | 468 [296–1022] | 0.8582 |
| PSGL-1 | 5822 [4899–7034] | 6008 [4995–7171] | 0.3128 |
| tPA | 1858 [1310–3017] | 2546 [1674.3–3689] | 0.0284 |
| PAI-1 | 78,027 [72,987–87,230] | 80,737 [75,598–86,422] | 0.1647 |
| Factor IX | 16,890 [14,287–21,699] | 18,363 [13,732–20,751] | 0.7152 |
| F5 rs6025 | |||
| CC (n = 129) | CT (n = 2) | ||
| P-Selectin | 447 [243–951] | 1392 [904–1880] | 0.4250 |
| D-dimer | 485 [277–1001] | 1498 [1168–1828] | 0.1406 |
| PSGL-1 | 5944 [4931–7045] | 6334 [5812–6856] | 0.6796 |
| tPA | 2112 [1406–3227] | 2447 [1840–3055] | 0.9701 |
| PAI-1 | 78,763 [73,462–87,210] | 81,797 [79,485–84,109] | 0.7073 |
| Factor IX | 17,136 [14,323–21,662] | 10,247 [10,108–10,386] | 0.0355 |
| Protein (pg/mL) | Time 1 (0–9 Days) | Time 2 (10–24 Days) | p-Value * | Δ (Time 1–Time 2) |
| P-Selectin | 416 [226–781] | 482 [164–880] | 0.3547 | −72 [−603–223] |
| D-Dimer | 660 [341–1654] | 922 [486–1915] | 0.1032 | −183 [−1012–171] |
| PSGL-1 | 5944 [4940–6884] | 6830 [5307–8810] | 0.0059 | −1371 [−3237–270] |
| tPA | 2093 [1457–3487] | 2295 [1471–3581] | 0.1819 | −399 [−2014–881] |
| PAI-1 | 80,462 [74,035–87,832] | 78,763 [70,988–93,465] | 0.7370 | −2718 [−1800–8437] |
| Factor IX | 17,621 [14,833–23,071] | 19,413 [11,519–24,126] | 0.8506 | −397 [−4729–5452] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fricke-Galindo, I.; Buendia-Roldan, I.; Chavez-Galan, L.; Pérez-Rubio, G.; Hernández-Zenteno, R.d.J.; Ramos-Martinez, E.; Zazueta-Márquez, A.; Reyes-Melendres, F.; Alarcón-Dionet, A.; Guzmán-Vargas, J.; et al. SERPINE1 rs6092 Variant Is Related to Plasma Coagulation Proteins in Patients with Severe COVID-19 from a Tertiary Care Hospital. Biology 2022, 11, 595. https://doi.org/10.3390/biology11040595
Fricke-Galindo I, Buendia-Roldan I, Chavez-Galan L, Pérez-Rubio G, Hernández-Zenteno RdJ, Ramos-Martinez E, Zazueta-Márquez A, Reyes-Melendres F, Alarcón-Dionet A, Guzmán-Vargas J, et al. SERPINE1 rs6092 Variant Is Related to Plasma Coagulation Proteins in Patients with Severe COVID-19 from a Tertiary Care Hospital. Biology. 2022; 11(4):595. https://doi.org/10.3390/biology11040595
Chicago/Turabian StyleFricke-Galindo, Ingrid, Ivette Buendia-Roldan, Leslie Chavez-Galan, Gloria Pérez-Rubio, Rafael de Jesús Hernández-Zenteno, Espiridión Ramos-Martinez, Armando Zazueta-Márquez, Felipe Reyes-Melendres, Aimé Alarcón-Dionet, Javier Guzmán-Vargas, and et al. 2022. "SERPINE1 rs6092 Variant Is Related to Plasma Coagulation Proteins in Patients with Severe COVID-19 from a Tertiary Care Hospital" Biology 11, no. 4: 595. https://doi.org/10.3390/biology11040595