
Mesothelin Gene Variants Affect Soluble Mesothelin-Related Protein Levels in the Plasma of Asbestos-Exposed Males and Mesothelioma Patients from Germany
 , , , , , ,
on behalf of the MoMar Study Group
, , , , , ,
on behalf of the MoMar Study Group
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Genotyping of Four MSLN Single-Nucleotide Polymorphisms (SNPs) and Mesothelin Measurements in Plasma
2.3. Statistical Analyses
3. Results
3.1. Characterization of the Study Population
3.2. Distribution of False-Positive and False-Negative Mesothelin Values by Single-Nucleotide Polymorphisms (SNPs) and Haplotype
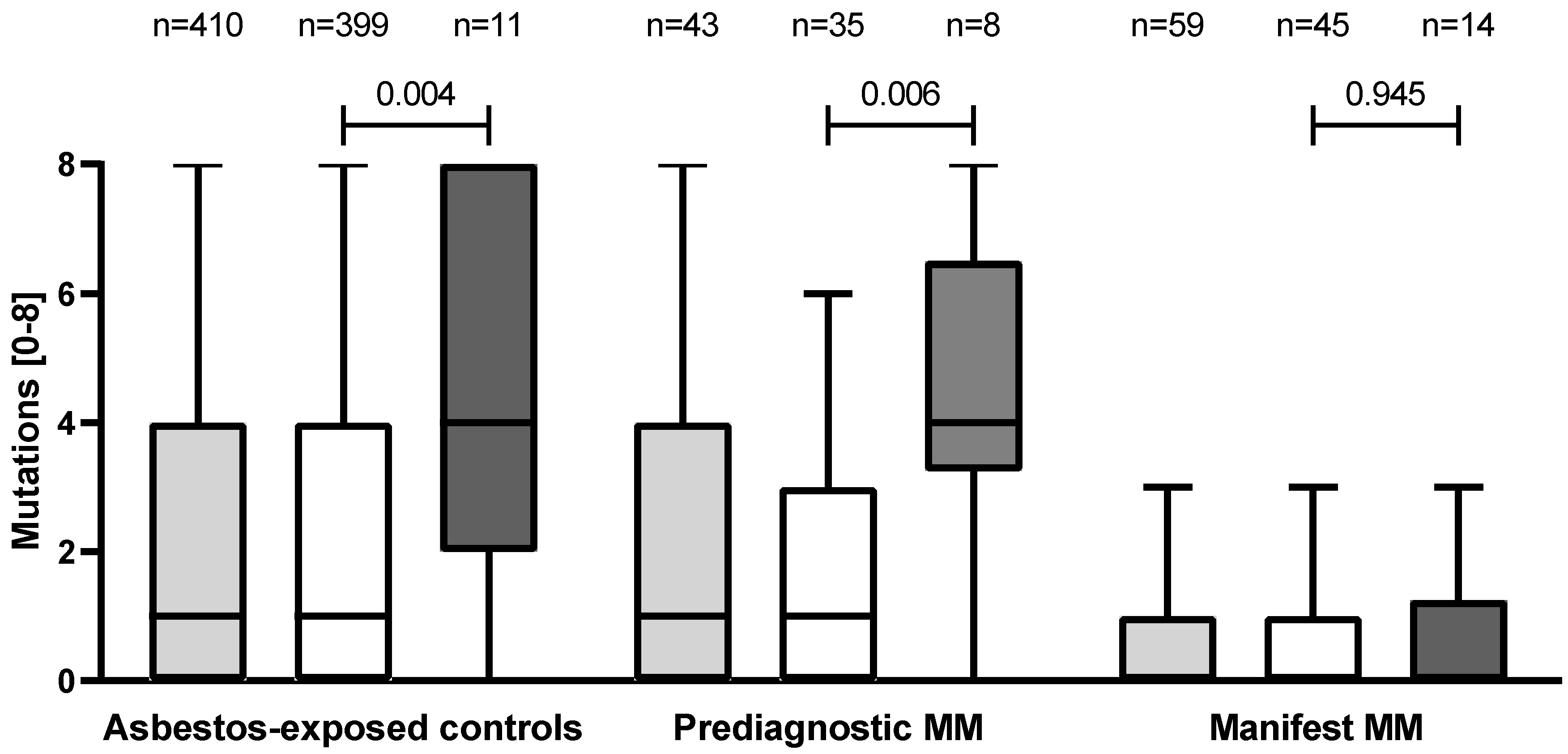
3.3. Distribution of the Four Single-Nucleotide Polymorphism Mutations by Study Group
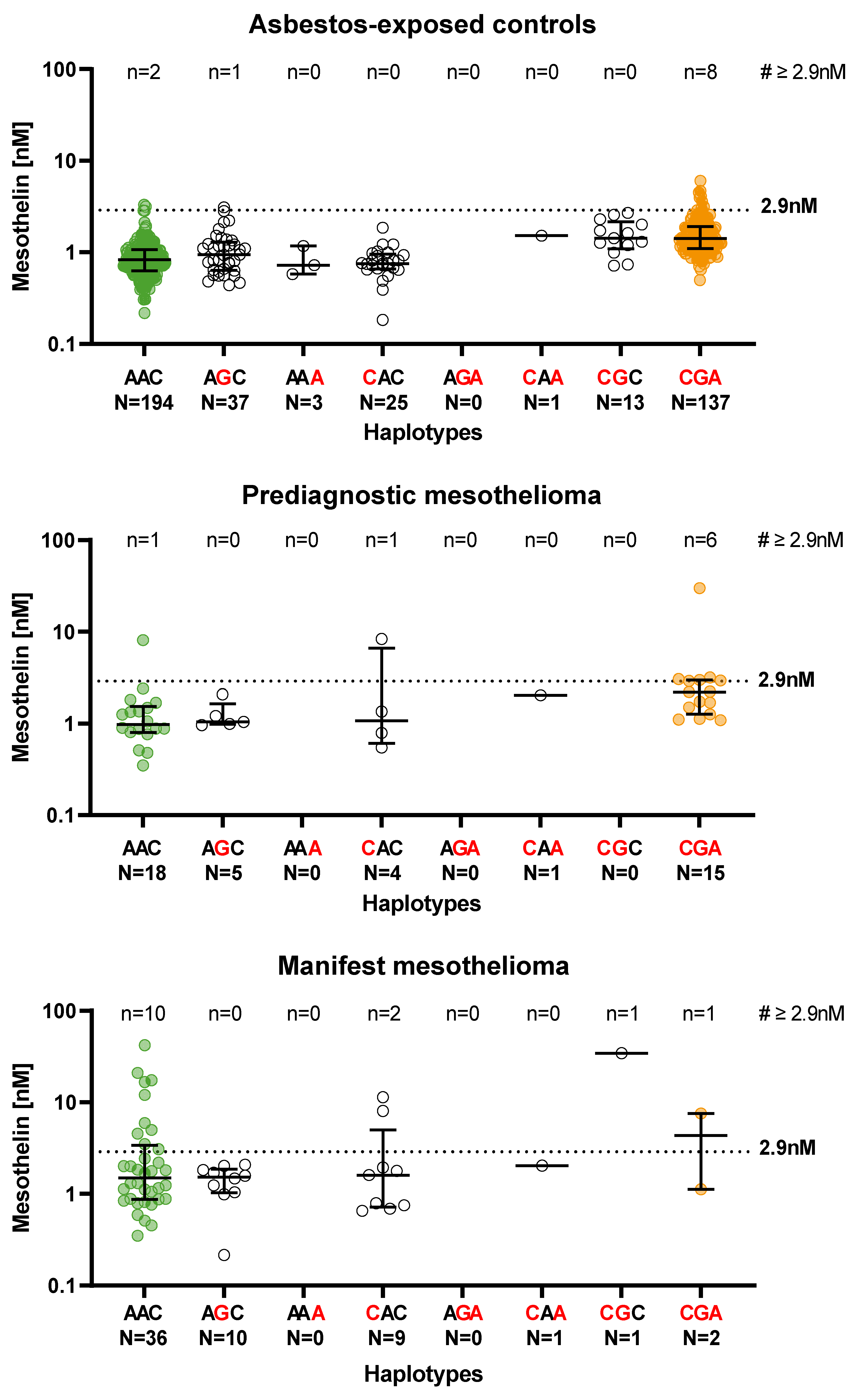
3.4. Distribution of the Mesothelin Concentration between 5′-UTR Haplotypes and Stratified by Study Groups
3.5. Logistic Regression Models in Asbestos-Exposed Controls and MM Groups Adjusted by Age
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Robinson, B.W.; Musk, A.W.; Lake, R.A. Malignant Mesothelioma. Lancet 2005, 366, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Robinson, B.W.; Lake, R.A. Advances in malignant mesothelioma. N. Engl. J. Med. 2005, 353, 1591–1603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pass, H.I.; Alimi, M.; Carbone, M.; Yang, H.; Goparaju, C.M. Mesothelioma Biomarkers: A review highlighting contributions from the early detection research network. Cancer Epidemiol. Biomark. Prev. 2020, 29, 2524–2540. [Google Scholar] [CrossRef] [PubMed]
- Hassan, R.; Remaley, A.T.; Sampson, M.L.; Zhang, J.; Cox, D.D.; Pingpank, J.; Alexander, R.; Willingham, M.; Pastan, I.; Onda, M. Detection and quantification of serum mesothelin, a tumour marker for patients with mesothelioma and ovarian cancer. Clin. Cancer Res. 2006, 12, 447–453. [Google Scholar] [CrossRef] [Green Version]
- Park, E.K.; Sandrini, A.; Yates, D.H.; Creany, J.; Robinson, B.W.; Thomas, P.S.; Johnson, A.R. Soluble mesothelin-related protein in an asbestos-exposed population: The dust diseases board cohort study. Am. J. Respir. Crit. Care Med. 2008, 178, 832–837. [Google Scholar] [CrossRef]
- Johnen, G.; Burek, K.; Raiko, I.; Wichert, K.; Pesch, B.; Weber, D.G.; Lehnert, M.; Casjens, S.; Hagemeyer, O.; MoMar Study Group. Prediagnostic detection of mesothelioma by circulating calretinin and mesothelin—A case-control comparison nested into a prospective cohort of asbestos-exposed workers. Sci. Rep. 2018, 8, 14321. [Google Scholar] [CrossRef] [Green Version]
- Creaney, J.; Olsen, N.J.; Brims, F.; Dick, I.M.; Musk, A.W.; de Klerk, N.H.; Skates, S.J.; Robinson, B.W. Serum mesothelin for early detection of asbestos-induced cancer malignant mesothelioma. Cancer Epidemiol. Biomark. Prev. 2010, 19, 2238–2246. [Google Scholar] [CrossRef] [Green Version]
- Shiomi, K.; Miyamoto, H.; Segawa, T.; Hagiwara, Y.; Ota, A.; Maeda, M.; Takahashi, K.; Masuda, K.; Sakao, Y.; Hino, O. Novel ELISA system for detection of N-ERC/mesothelin in the sera of mesothelioma patients. Cancer Sci. 2006, 97, 928–932. [Google Scholar] [CrossRef]
- Shiomi, K.; Hagiwara, Y.; Sonoue, K.; Segawa, T.; Miyashita, K.; Maeda, M.; Izumi, H.; Masuda, K.; Hirabayashi, M.; Moroboshi, T.; et al. Sensitive and specific new enzyme-linked immunosorbent assay for N-ERC/mesothelin increases its potential as a useful serum tumour marker for mesothelioma. Clin. Cancer Res. 2008, 14, 1431–1437. [Google Scholar] [CrossRef] [Green Version]
- Hassan, R.; Bera, T.; Pastan, I. Mesothelin: A new target for immunotherapy. Clin. Cancer Res. 2004, 10, 3937–3942. [Google Scholar] [CrossRef]
- Raiko, I.; Rihs, H.P.; Gleichenhagen, J.; Sander, I.; Kollmeier, J.; Lehnert, M.; Brüning, T.; Johnen, G. A recombinant polypeptide of the megakaryocyte potentiating factor is a potential biomarker in plasma for the detection of mesothelioma. Biochem. Biophys. Res. Commun. 2017, 486, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Ramírez, C.; Casjens, S.; Juárez-Pérez, C.A.; Raiko, I.; Del Razo, L.M.; Taeger, D.; Calderón-Aranda, E.S.; Rihs, H.-P.; Acosta-Saavedra, L.C.; Weber, D.G.; et al. Mesothelin, Calretinin, and Megakaryocyte Potentiating Factor as Biomarkers of Malignant Pleural Mesothelioma. Lung 2019, 197, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Scherpereel, A.; Grigoriu, B.; Conti, M.; Gey, T.; Gregoire, M.; Copin, M.C.; Devos, P.; Chahine, B.; Porte, H.; Lassalle, P. Soluble mesothelin related peptides in the diagnosis of malignant pleural mesothelioma. Am. J. Respir. Crit. Care Med. 2006, 173, 1155–1160. [Google Scholar] [CrossRef]
- Casjens, S.; Weber, D.G.; Johnen, G.; Raiko, I.; Taeger, D.; Meinig, C.; Moebus, S.; Jöckel, K.-H.; Brüning, T.; Pesch, B. Assessment of potential predictors of calretinin and mesothelin to improve the diagnostic performance to detect malignant mesothelioma: Results from a population-based cohort study. BMJ Open 2017, 7, e017104. [Google Scholar] [CrossRef] [PubMed]
- Casjens, S.; Johnen, G.; Raiko, I.; Pesch, B.; Taeger, D.; Töpfer, C.; Schonefeld, S.; Moebus, S.; Jöckel, K.-H.; Brüning, T.; et al. Re-evaluation of potential predictors of calretinin and mesothelin in a population-based cohort study using assays for the routine application in clinical medicine. BMJ Open 2021, 11, e039079. [Google Scholar] [CrossRef] [PubMed]
- Cristaudo, A.; Foddis, R.; Bonotti, A.; Simonini, S.; Vivaldi, A.; Guglielmi, G.; Bruno, R.; Gemignani, F.; Landi, S. Two novel polymorphisms in 5′ flanking region of the mesothelin gene are associated with soluble mesothelin-related peptide (SMRP) levels. Int. J. Biol. Markers 2011, 26, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Garritano, S.; De Santi, C.; Silvestri, R.; Melaiu, O.; Cipollini, M.; Barone, E.; Lucchi, M.; Barale, R.; Mutti, L.; Gemignani, F.; et al. A common polymorphism within MSLN affects miR-611 binding site and soluble mesothelin levels in healthy people. J. Thorac. Oncol. 2014, 9, 1662–1668. [Google Scholar] [CrossRef] [Green Version]
- De Santi, C.; Pucci, P.; Bonotti, A.; Melaiu, O.; Cipollini, M.; Silvestri, R.; Vymetalkova, V.; Barone, E.; Paolicchi, E.; Corrado, A.; et al. Mesothelin promoter variants are associated with increased soluble mesothelin-related peptide levels in asbestos-exposed individuals. Occup. Environ. Med. 2017, 74, 456–463. [Google Scholar] [CrossRef] [Green Version]
- Silvestri, R.; Pucci, P.; De Santi, C.; Dell’Anno, I.; Miglietta, S.; Corrado, A.; Nicolí, V.; Marolda, D.; Cipollini, M.; Pellegrino, E.; et al. Variation rs2235503C>A within the promoter of MSLN affects transcriptional rate of mesothelin and plasmatic levels of the soluble mesothelin-related peptide. Front. Genet. 2020, 18, 975. [Google Scholar] [CrossRef]
- Goricar, K.; Kovac, V.; Dodic-Fikfak, M.; Dolzan, V.; Franko, A. Evaluation of soluble mesothelin-related peptides and MSLN genetic variability in asbestos-related diseases. Radiol. Oncol. 2020, 54, 86–95. [Google Scholar] [CrossRef]
- Shen, K.; Liu, K.; Wang, Y.; Ni, P.; Xiao, J.; Hao, F.; Zhou, X.; Xu, Z.; Yang, L. Polymorphisms of an oncogenic gene, mesothelin, predict the risk and prognosis of gastric cancer in a Chinese Han population. Arch. Toxicol. 2022, 96, 2097–2111. [Google Scholar] [CrossRef] [PubMed]
- Taeger, D.; Wichert, K.; Lehnert, M.; Casjens, S.; Pesch, B.; Weber, D.G.; Brüning, T.; Johnen, G.; Behrens, T. Lung cancer and mesothelioma risks in a prospective cohort of workers with asbestos-related lung or pleural diseases. Am. J. Ind. Med. 2022, 65, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Weber, D.G.; Brik, A.; Casjens, S.; Burek, K.; Lehnert, M.; Pesch, B.; Taeger, D.; Brüning, T.; Johnen, G.; the MoMar study group; et al. Are circulating microRNAs suitable for the early detection of malignant mesothelioma? Results from a nested cohort study. BMC Res. Notes 2019, 12, 77. [Google Scholar] [CrossRef]
- Hollevoet, K.; Bernard, D.; De Geeter, F.; Walgraeve, N.; Van den Eeckhaut, A.; Vanholder, R.; Van de Wiele, C.; Stove, V.; van Meerbeeck, J.P.; Delanghe, J.R. Glomerular filtration rate is a confounder for the measurement of soluble mesothelin in serum. Clin. Chem. 2009, 55, 1431–1433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oudkerk, M.; Liu, S.; Heuvelmans, M.A.; Walter, J.E.; Field, J.K. Lung cancer LDCT screening and mortality reduction—Evidence, pitfalls and future perspectives. Nat. Rev. Clin. Oncol. 2021, 18, 135–151. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Asbestos-Exposed Controls | Prediagnostic MM | Manifest MM | |||
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | p Value c | ||
| N | 410 | 43 | 59 | ||
| Mesothelin (nM) | Median (IQR b) | 1.02 (0.74–1.41) | 1.34 (0.90–2.21) | 1.61 (0.88–2.43) | <0.001 |
| Age (years) | Median (IQR b) | 73 (69–77) | 74 (71–77) | 72 (66–75) | 0.206 |
| Smoking status | Never | 129 (31.5) | 12 (27.9) | 22 (37.3) | 0.791 |
| Former | 233 (56.8) | 27 (62.8) | 32 (54.2) | ||
| Current | 44 (10.7) | 4 (9.3) | 4 (6.8) | ||
| Missing | 4 (1.0) | 0 (0) | 1 (1.7) | ||
| Hypertension a | Yes | 262 (63.9) | 26 (60.5) | 27 (45.8) | 0.082 |
| Diabetes mellitus a | Yes | 61 (14.9) | 7 (16.3) | 9 (15.3) | 0.244 |
| Rheumatoid arthritis a | Yes | 17 (4.2) | 2 (4.7) | 1 (1.7) | 0.167 |
| Liver disease a | Yes | 8 (2.0) | 2 (4.7) | 2 (3.4) | 0.076 |
| Intestinal disease a | Yes | 10 (2.4) | 3 (7.0) | 1 (1.7) | 0.055 |
| Renal insufficiency a | Yes | 6 (1.5) | 1 (2.3) | 2 (3.4) | 0.092 |
| Asbestos-Exposed Controls (N = 410) | Prediagnostic Mesothelioma (N = 43) | Manifest Mesothelioma (N = 59) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mesothelin < 2.9 nM (True-Negative) | Mesothelin ≥ 2.9 nM (False-Positive) | Mesothelin < 2.9 nM (False-Negative) | Mesothelin ≥ 2.9 nM (True-Positive) | Mesothelin < 2.9 nM (False-Negative) | Mesothelin ≥ 2.9 nM (True-Positive) | |||||||||||||
| N = 399 (97.3%) | N = 11 (2.7%) | N = 35 (81.4%) | N = 8 (18.6%) | N = 45 (76.3%) | N = 14 (23.7%) | |||||||||||||
| N | % | 95% CI | N | % | 95% CI | N | % | 95% CI | N | % | 95% CI | N | % | 95% CI | N | % | 95% CI | |
| SNPs from 5′-UTR | ||||||||||||||||||
| MSLN rs3764247 A > C | ||||||||||||||||||
| AA | 231 | 57.9 | 53.1–62.7 | 3 | 27.3 | 1.0–53.6 | 22 | 62.9 | 46.8–78.9 | 1 | 12.5 | 0–35.4 | 36 | 80.0 | 68.3–91.7 | 10 | 71.4 | 47.8–95.1 |
| AC | 141 | 35.3 | 30.6–40.0 | 4 | 36.4 | 7.9–64.8 | 10 | 28.6 | 13.6–43.5 | 4 | 50.0 | 15.4–84.6 | 8 | 17.8 | 6.6–28.9 | 3 | 21.4 | 0–42.9 |
| CC | 27 | 6.8 | 4.3–9.2 | 4 | 36.4 | 7.9–64.8 | 3 | 8.6 | 0–17.8 | 3 | 37.5 | 4.0–71.0 | 1 | 2.2 | 0–6.5 | 1 | 7.1 | 0–20.6 |
| MSLN rs3764246 A > G | ||||||||||||||||||
| AA | 221 | 55.4 | 50.5–60.3 | 2 | 18.2 | 0–41.0 | 21 | 60.0 | 43.8–76.2 | 2 | 25.0 | 0–55.0 | 34 | 75.6 | 63–88.1 | 12 | 85.7 | 67.4–100 |
| AG | 141 | 35.3 | 30.6–40.0 | 4 | 36.4 | 7.9–64.8 | 13 | 37.1 | 21.1–53.2 | 4 | 50.0 | 15.4–84.6 | 11 | 24.4 | 11.9–37.0 | 2 | 14.3 | 0–32.6 |
| GG | 37 | 9.3 | 6.4–12.1 | 5 | 45.5 | 16.0–74.9 | 1 | 2.9 | 0–8.4 | 2 | 25.0 | 0–55.0 | 0 | 0 | ||||
| MSLN rs2235503 C > A | ||||||||||||||||||
| CC | 266 | 66.7 | 62.0–71.3 | 3 | 27.3 | 1.0–53.6 | 25 | 71.4 | 56.5–86.4 | 2 | 25.0 | 0–55.0 | 43 | 95.6 | 89.5–100 | 13 | 92.9 | 79.4–100 |
| CA | 117 | 29.3 | 24.9–33.8 | 4 | 36.4 | 7.9–64.8 | 10 | 28.6 | 13.6–43.5 | 4 | 50.0 | 15.4–84.6 | 2 | 4.4 | 0–10.5 | 1 | 7.1 | 0–20.6 |
| AA | 16 | 4.0 | 2.1–5.9 | 4 | 36.4 | 7.9–64.8 | 0 | 2 | 25.0 | 0–55.0 | 0 | 0 | ||||||
| Haplotype of the three SNPs from 5′-UTR | ||||||||||||||||||
| No mutation (AAC) | 192 | 48.1 | 43.2–53.0 | 2 | 18.2 | 0–41.0 | 17 | 48.6 | 32–65.1 | 1 | 12.5 | 0–35.4 | 26 | 57.8 | 43.3–72.2 | 10 | 71.4 | 47.8–95.1 |
| 1–2 mutations * | 78 | 19.5 | 15.7–23.4 | 1 | 9.1 | 0–26.1 | 9 | 25.7 | 11.2–40.2 | 1 | 12.5 | 0–35.4 | 18 | 40.0 | 25.7–54.3 | 3 | 21.4 | 0–42.9 |
| 3 mutations (CGA) | 129 | 32.3 | 27.7–36.9 | 8 | 72.7 | 46.4–99.0 | 9 | 25.7 | 11.2–40.2 | 6 | 75.0 | 45–100 | 1 | 2.2 | 0–6.5 | 1 | 7.1 | 0–20.6 |
| MSLN rs1057147 G > A from 3′-UTR | ||||||||||||||||||
| GG | 243 | 60.9 | 56.1–65.7 | 3 | 27.3 | 1.0–53.6 | 22 | 62.9 | 46.8–78.9 | 1 | 12.5 | 0–35.4 | 38 | 84.4 | 73.9–95.0 | 12 | 85.7 | 67.4–100 |
| GA | 132 | 33.1 | 28.5–37.7 | 5 | 45.5 | 16.0–74.9 | 10 | 28.6 | 13.6–43.5 | 5 | 62.5 | 29–96 | 5 | 11.1 | 1.9–20.3 | 2 | 14.3 | 0–32.6 |
| AA | 24 | 6.0 | 3.7–8.3 | 3 | 27.3 | 1.0–53.6 | 3 | 8.6 | 0–17.8 | 2 | 25.0 | 0–55.0 | 2 | 4.4 | 0–10.5 | 0 | ||
| Model | Effect | Asbestos-Exposed Controls (N = 410) | Prediagnostic MM (N = 43) | Manifest MM (N = 59) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | OR | 95% CI | p Value | |||||
| Age (years) | 1.10 | 1.00 | 1.23 | 0.060 | 1.06 | 0.90 | 1.24 | 0.515 | 1.03 | 0.97 | 1.10 | 0.312 | |
| Haplotype (3 SNPs of the 5′-UTR) | 3 mutations | 6.00 | 1.25 | 28.90 | 0.025 | 11.03 | 1.13 | 107.5 | 0.039 | 1.69 | 0.09 | 32.20 | 0.728 |
| Ref b: no mutation | 1–2 mutations | 1.29 | 0.11 | 14.54 | 0.835 | 1.91 | 0.11 | 34.43 | 0.660 | 0.35 | 0.08 | 1.53 | 0.164 |
| MSLN rs3764247 A > C (ref b: AA) | AC | 2.06 | 0.45 | 9.40 | 0.350 | 8.32 | 0.81 | 85.23 | 0.074 | 1.22 | 0.26 | 5.58 | 0.802 |
| CC | 10.83 | 2.26 | 51.99 | 0.003 | 22.74 | 1.72 | 300.1 | 0.018 | 2.94 | 0.16 | 52.69 | 0.464 | |
| MSLN rs3764247 A > C (ref b: common genotype) | Non-common genotype | 3.45 | 0.90 | 13.30 | 0.072 | 11.56 | 1.27 | 105.2 | 0.030 | 1.42 | 0.35 | 5.73 | 0.625 |
| MSLN rs3764246 A > G (ref b: AA) | AG | 3.47 | 0.62 | 19.32 | 0.156 | 2.60 | 0.39 | 17.37 | 0.323 | 0.41 | 0.08 | 2.22 | 0.302 |
| GG | 15.59 | 2.87 | 84.66 | 0.001 | 33.29 | 1.57 | 703.8 | 0.024 | -a | ||||
| MSLN rs3764246 A > G (ref b: common genotype) | Non-common genotype | 6.11 | 1.29 | 28.85 | 0.022 | 4.31 | 0.75 | 24.83 | 0.102 | 0.41 | 0.08 | 2.22 | 0.302 |
| MSLN rs2235503 C > A (ref b: CC) | CA | 3.07 | 0.67 | 13.98 | 0.148 | -a | 1.54 | 0.12 | 19.08 | 0.735 | |||
| AA | 20.68 | 4.14 | 103.4 | <0.001 | -a | -a | |||||||
| MSLN rs2235503 C > A (ref b: common genotype) | Non-common genotype | 5.31 | 1.38 | 20.48 | 0.015 | 7.25 | 1.22 | 42.99 | 0.029 | 1.54 | 0.12 | 19.08 | 0.735 |
| MSLN rs1057147 G > A (ref b: GG) | GA | 3.10 | 0.73 | 13.23 | 0.127 | 10.69 | 1.09 | 104.6 | 0.042 | -a | |||
| AA | 8.87 | 1.66 | 47.50 | 0.011 | 15.40 | 1.03 | 229.6 | 0.047 | -a | ||||
| MSLN rs1057147 G > A (ref b: common genotype) | Non-common genotype | 4.08 | 1.06 | 15.70 | 0.041 | 11.74 | 1.29 | 106.9 | 0.029 | 1.02 | 0.18 | 5.76 | 0.983 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rihs, H.-P.; Casjens, S.; Raiko, I.; Kollmeier, J.; Lehnert, M.; Nöfer, K.; May-Taube, K.; Kaiser, N.; Taeger, D.; Behrens, T.; et al. Mesothelin Gene Variants Affect Soluble Mesothelin-Related Protein Levels in the Plasma of Asbestos-Exposed Males and Mesothelioma Patients from Germany. Biology 2022, 11, 1826. https://doi.org/10.3390/biology11121826
Rihs H-P, Casjens S, Raiko I, Kollmeier J, Lehnert M, Nöfer K, May-Taube K, Kaiser N, Taeger D, Behrens T, et al. Mesothelin Gene Variants Affect Soluble Mesothelin-Related Protein Levels in the Plasma of Asbestos-Exposed Males and Mesothelioma Patients from Germany. Biology. 2022; 11(12):1826. https://doi.org/10.3390/biology11121826
Chicago/Turabian StyleRihs, Hans-Peter, Swaantje Casjens, Irina Raiko, Jens Kollmeier, Martin Lehnert, Kerstin Nöfer, Kerstin May-Taube, Nina Kaiser, Dirk Taeger, Thomas Behrens, and et al. 2022. "Mesothelin Gene Variants Affect Soluble Mesothelin-Related Protein Levels in the Plasma of Asbestos-Exposed Males and Mesothelioma Patients from Germany" Biology 11, no. 12: 1826. https://doi.org/10.3390/biology11121826