



Low and Moderate Doses of Caffeinated Coffee Improve Repeated Sprint Performance in Female Team Sport Athletes

 , , ,
, , ,  , , ,
, , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Protocol
2.3. Repeated Sprint Test
2.4. Supplementation Protocol Coffee Preparation
2.5. Blood Sampling
2.6. Statistical Analyses
3. Results
3.1. Repeated Sprint Performance
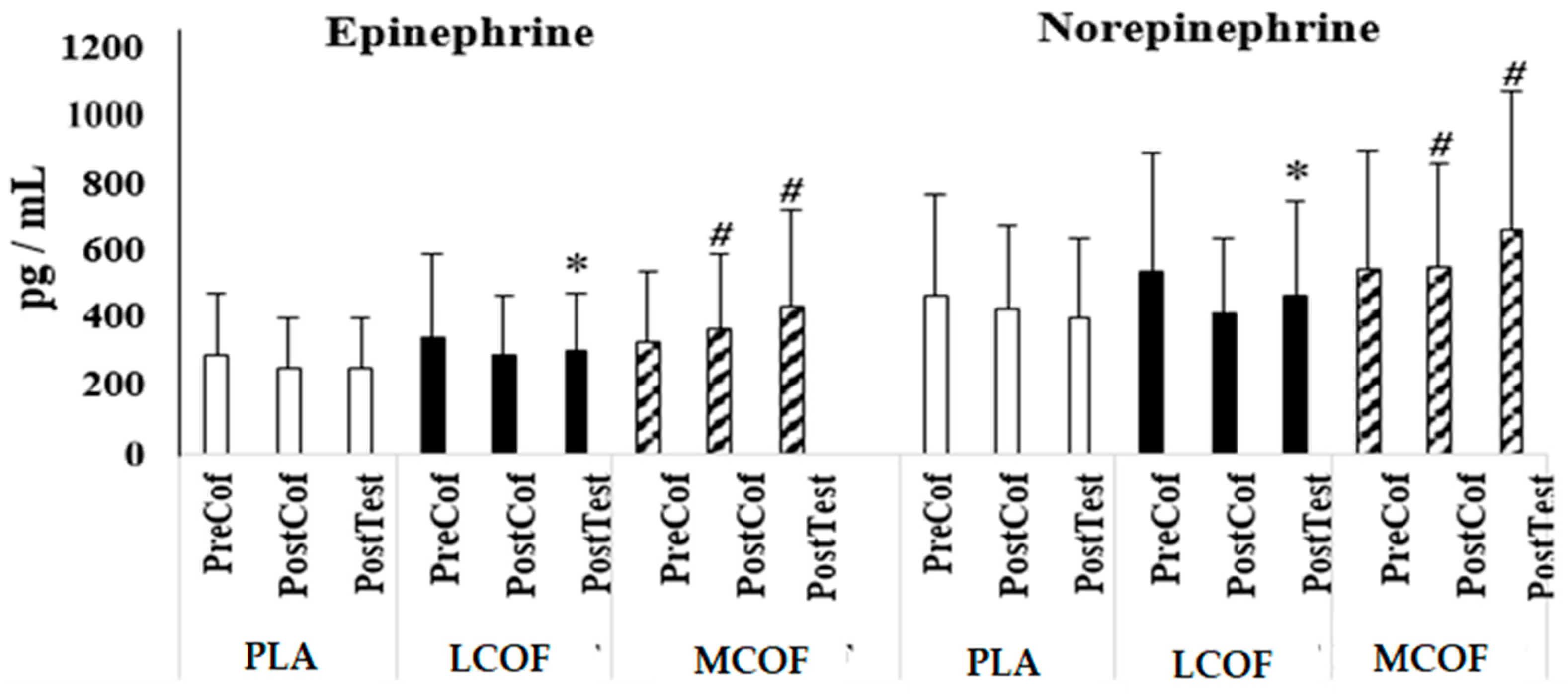
3.2. Catecholamines
3.3. Heart Rate, RPE, Glucose, and Lactate
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grgic, J.; Grgic, I.; Pickering, C.; Schoenfeld, B.J.; Bishop, D.J.; Pedisic, Z. Wake up and smell the coffee: Caffeine supplementation and exercise performance—An umbrella review of 21 published meta-analyses. Br. J. Sports Med. 2019, 54, 681–688. [Google Scholar] [CrossRef]
- Tarnapolsky, M.A. Effect of caffeine on the neuromuscular system–potential as an ergogenic aid. Appl. Physiol. Nutr. Metab. 2008, 33, 1284–1289. [Google Scholar] [CrossRef]
- Tarnopolsky, M.; Cupido, C. Caffeine potentiates low frequency skeletal muscle force in habitual and nonhabitual caffeine consumers. J. Appl. Physiol. 2000, 89, 1719–1724. [Google Scholar] [CrossRef]
- Stuart, G.R.; Hopkins, W.G.; Cook, C.; Cairns, S.P. Multiple effects of caffeine on simulated high-intensity team-sport performance. Med. Sci. Sports Exerc. 2005, 37, 1998–2005. [Google Scholar] [CrossRef]
- Greer, F.; McLean, C.; Graham, T.E. Caffeine, performance, and metabolism during repeated wingate exercise tests. J. Appl. Physiol. 1998, 85, 1502–1508. [Google Scholar] [CrossRef]
- Graham, T.E.; Spriet, L.L. Metabolic, catecholamine, and exercise performance responses to various doses of caffeine. J. Appl. Physiol. 1995, 78, 867–874. [Google Scholar] [CrossRef]
- Graham, T.E.; Hibbert, E.; Sathasivam, P. Metabolic and exercise endurance effects of coffee and caffeine ingestion. J. Appl. Physiol. 1998, 85, 883–889. [Google Scholar] [CrossRef]
- Mohr, M.; Nielsen, J.J.; Bangsbo, J. Caffeine intake improves intense intermittent exercise performance and reduces muscle interstitial potassium accumulation. J. Appl. Physiol. 2011, 111, 1372–1379. [Google Scholar] [CrossRef]
- Glaister, M.; Patterson, S.D.; Foley, P.; Pedlar, C.R.; Pattison, J.R.; McInnes, G. Caffeine and sprinting performance: Dose responses and efficacy. J. Strength Cond. Res. 2012, 26, 1001–1005. [Google Scholar] [CrossRef] [Green Version]
- Anderson, D.E.; LeGrand, S.E.; Mccart, R.D. Effect of caffeine on sprint cycling in experienced cyclists. J. Strength Cond. Res. 2018, 32, 2221–2226. [Google Scholar] [CrossRef]
- Schneiker, K.T.; Bishop, D.; Dawson, B.; Hackett, L.P. Effects of caffeine on prolonged intermittent–sprint ability in team-sport athletes. Med. Sci. Sports Exerc. 2006, 38, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-L.; Cheng, C.-F.; Lin, J.-C.; Huang, H.-W. Caffeine’s effect on intermittent sprint cycling performance with different rest intervals. Eur. J. Appl. Physiol. 2012, 112, 2107–2116. [Google Scholar] [CrossRef]
- Evans, M.; Tierney, P.; Gray, N.; Hawe, G.; Macken, M.; Egan, B. Acute ingestion of caffeinated chewing gum improves repeated sprint performance of team sport athletes with low habitual caffeine consumption. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Lara, B.; Hellin, H.G.; Ruiz-Moreno, C.; Romero-Moraleda, B.; Del Coso, J. Acute caffeine intake increases performance in the 15-s wingate test during the menstrual cycle. Br. J. Clin. Pharmacol. 2020, 86, 745–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Coso, J.; Portillo, J.; Munoz, G.; Abian-Vicen, J.; Gonzalez-Millan, C.; Munoz-Guerra, J. Caffeine-containing energy drink improves sprint performance during an international rugby sevens competition. Amino Acids 2013, 44, 1511–1519. [Google Scholar] [CrossRef] [PubMed]
- Lara, B.; Salinero, J.J.; Giraldez-Costas, V.; Del Coso, J. Similar ergogenic effect of caffeine on anaerobic performance in men and women athletes. Eur. J. Nutr. 2021, 60, 4107–4114. [Google Scholar] [CrossRef]
- Skinner, T.L.; Desbrow, B.; Arapova, J.; Schaumberg, M.A.; Osborne, J.; Grant, G.D.; Anoopkumar-Dukie, S.; Leveritt, M.D. Women experience the same ergogenic response to caffeine as men. Med. Sci. Sports Exerc. 2019, 51, 1195–1202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spriet, L.L. Exercise and sport performance with low doses of caffeine. Sports Med. 2014, 44, 175–184. [Google Scholar] [CrossRef] [Green Version]
- Wickham, K.A.; Spriet, L.L. Administration of caffeine in alternate forms. Sports Med. 2018, 48, 79–91. [Google Scholar] [CrossRef] [Green Version]
- Hodgson, A.B.; Randell, R.K.; Jeukendrup, A.E. The metabolic and performance effects of caffeine compared to coffee during endurance exercise. PLoS ONE 2013, 8, e59561. [Google Scholar] [CrossRef]
- Richardson, D.L.; Clarke, N.D. Effect of coffee and caffeine ingestion on resistance exercise performance. J. Strength Cond. Res. 2016, 30, 2892–2900. [Google Scholar] [CrossRef] [PubMed]
- Clarke, N.; Baxter, H.; Fajemilua, E.; Jones, V.; Oxford, S.; Richardson, D.; Wyatt, C.; Mundy, P. Coffee and caffeine ingestion have little effect on repeated sprint cycling in relatively untrained males. Sports 2016, 4, 45. [Google Scholar] [CrossRef] [Green Version]
- Guest, N.S.; VanDusseldorp, T.A.; Nelson, M.T.; Grgic, J.; Schoenfeld, B.J.; Jenkins, N.D.M.; Arent, S.M.; Antonio, J.; Stout, J.R.; Trexler, E.T.; et al. International society of sports nutrition position stand: Caffeine and exercise performance. J. Int. Soc. Sport Nutr. 2021, 18, 1. [Google Scholar] [CrossRef] [PubMed]
- Astorino, T.A.; Roberson, D.W. Efficacy of acute caffeine ingestion for short-term high-intensity exercise performance: A systematic review. J. Strength Cond. Res. 2010, 24, 257–265. [Google Scholar] [CrossRef]
- Bühler, E.; Lachenmeier, D.W.; Schlegel, K.; Winkler, G. Development of a tool to assess the caffeine intake among teenagers and young adults. Ernahr. Umsch. 2013, 61, 58–63. [Google Scholar]
- Filip, A.; Wilk, M.; Krzystofik, M.; Del Coso, J. Inconsistency in the ergogenic effect of caffeine in athletes who regularly consume caffeine: Is it due to the disparity in the criteria that defines habitual caffeine intake? Nutrients 2020, 12, 1087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Storer, T.W.; Davis, J.A.; Caiozzo, V.J. Accurate prediction of VO2max in cycle ergometry. Med. Sci. Sports Exerc. 1990, 22, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Glaister, M.; Howatson, G.; Pattison, J.R.; McInnes, G. The reliability and validity of fatigue measures during multiple-sprint work: An issue revisited. J. Strength Cond. Res. 2008, 22, 1597–1601. [Google Scholar] [CrossRef] [Green Version]
- Clarke, N.D.; Kirwan, N.A.; Richardson, D.L. Coffee ingestion improves 5 km cycling performance in men and women by a similar magnitude. Nutrients 2019, 11, 2575. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J.A. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Paton, C.D.; Lowe, T.; Irvine, A. Cafffeinated chewing gum increases repeated sprint performance and augments increases in testosterone in competitive cyclists. Eur. J. Appl. Physiol. 2010, 110, 1243–1250. [Google Scholar] [CrossRef]
- Lara, B.; Gonzalez-Millan, C.; Salinero, J.J.; Abian-Vicen, J.; Areces, F.; Barbero-Alvarez, J.C.; Munoz, V.; Portillo, L.J.; Gonzalez-Rave, J.M.; Del Coso, J. Caffeine-containing energy drink improves physical performance in female soccer players. Amino Acids 2014, 46, 1385–1392. [Google Scholar] [CrossRef]
- Crowe, M.J.; Leicht, A.S.; Spinks, W.L. Physiological and cognitive responses to caffeine during repeated, high-intensity exercise. Int. J. Sport Nutr. Exerc. Metab. 2006, 16, 528–544. [Google Scholar] [CrossRef]
- Holloszy, J.O. Muscle metabolism during exercise. Arch. Phys. Med. Rehabil. 1982, 63, 231–234. [Google Scholar]
- Spriet, L.L.; Lindinger, M.I.; McKelvie, R.S.; Heigenhauser, G.J.; Jones, N.L. Muscle glycogenolysis and H? Concentration during maximal intermittent cycling. J. Appl. Physiol. 1989, 66, 8–13. [Google Scholar] [CrossRef]
- Wang, C.; Zhu, Y.; Dong, C.; Zhou, Z.; Zheng, X. Effects of various doses of caffeine ingestion on intermittent exercise performance and cognition. Brain Sci. 2020, 10, 595. [Google Scholar] [CrossRef]
- Anderson, D.E.; German, R.E.; Harrison, M.E.; Bourassa, K.N.; Taylor, C.E. Real and perceived effects of caffeine on sprint cycling in experienced cyclists. J. Strength Cond. Res. 2020, 34, 929–933. [Google Scholar] [CrossRef]
- Pickering, C.; Kiely, J. What should we do about habitual caffeine use in athletes? Sports Med. 2019, 49, 833–842. [Google Scholar] [CrossRef] [Green Version]
- Durkalec-Michalski, K.; Nowaczyk, P.M.; Glowka, N.; Grygiel, A. Dose-dependent effect of caffeine supplementation on judo-specific performance and training activity: A randomized placebo-controlled crossover trial. J. Int. Soc. Sports Nutr. 2019, 16, 38. [Google Scholar] [CrossRef] [Green Version]
- Beaumont, R.; Cordery, P.; Funnell, M.; Mears, S.; James, L.; Watson, P. Chronic ingestion of a low dose of caffeine induces tolerance to the performance benefits of caffeine. J. Sports Sci. 2017, 35, 1920–1927. [Google Scholar] [CrossRef]
- Lara, B.; Ruiz-Moreno, C.; Salinero, J.J.; Del Coso, J. Time course of tolerance to the performance benefits of caffeine. PLoS ONE 2019, 14, e0210275. [Google Scholar] [CrossRef]
- Ruiz-Moreno, C.; Lara, B.; Salinero, J.J.; Souza, D.B.; Ordovas, J.M.; Del Coso, J. Time course of tolerance to adverse effects of associated with the ingestion of a moderate dose of caffeine. Eur. J. Nutr. 2020, 59, 3293–3302. [Google Scholar] [CrossRef]
- Meeusen, R.; Roelands, B.; Spriet, L.L. Caffeine, exercise and the brain. Nestle Nutr. Inst. Workshop Ser. 2013, 76, 1–12. [Google Scholar]
- Graham, T.E.; Helge, J.W.; MacLean, D.A.; Kiens, B.; Richter, E.A. Caffeine ingestion does not alter carbohydrate or fat metabolism in human skeletal muscle during exercise. J. Physiol. 2000, 529, 837–847. [Google Scholar] [CrossRef]
- Graham, T.E.; Battram, D.S.; Dela, F.; El-Sohemy, A.; Thong, F.S. Does caffeine alter muscle carbohydrate and fat metabolism during exercise? Appl. Physiol. Nutr. Metab. 2008, 33, 1311–1318. [Google Scholar] [CrossRef]
- Spencer, M.; Bishop, D.; Dawson, B.; Goodman, C. Physiological and metabolic responses of repeated-sprint activities: Specific to field-based team sports. Sports Med. 2005, 35, 1025–1044. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Time Point | PLA | LCOF | MCOF | |
|---|---|---|---|---|
| Lactate (mmol·L−1) | PreCof | 1.8 ± 0.5 | 1.7 ± 0.5 | 1.8 ± 0.4 |
| PostRST | 11.9 ± 1.3 | 13.8 ± 1.4 * | 13.7 ± 1.6 * | |
| Glucose (mmol·L−1) | PreCof | 93.3 ± 8.0 | 101.9 ± 19.0 | 98.4 ± 10.4 |
| PostRST | 119.1 ± 13.5 | 121.9 ± 15.1 | 117.0 ± 15.9 | |
| Heart rate (beat/min) | PreCof | 67.0 ± 7.9 | 63.9 ± 5.5 | 64.4 ± 5.6 |
| MidRST | 179.4 ± 5.5 | 180.3 ± 4.4 | 179.3 ± 5.3 | |
| PostRST | 180.4 ± 6.3 | 179.8 ± 4.6 | 180.4 ± 6.3 | |
| RPE (AU) | MidRST | 15.1 ± 1.5 | 15.0 ± 1.5 | 15.2 ± 1.5 |
| PostRST | 17.6 ± 1.6 | 17.6 ± 1.4 | 17.8 ± 1.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karayigit, R.; Forbes, S.C.; Osmanov, Z.; Yilmaz, C.; Yasli, B.C.; Naderi, A.; Buyukcelebi, H.; Benesova, D.; Gabrys, T.; Esen, O. Low and Moderate Doses of Caffeinated Coffee Improve Repeated Sprint Performance in Female Team Sport Athletes. Biology 2022, 11, 1498. https://doi.org/10.3390/biology11101498
Karayigit R, Forbes SC, Osmanov Z, Yilmaz C, Yasli BC, Naderi A, Buyukcelebi H, Benesova D, Gabrys T, Esen O. Low and Moderate Doses of Caffeinated Coffee Improve Repeated Sprint Performance in Female Team Sport Athletes. Biology. 2022; 11(10):1498. https://doi.org/10.3390/biology11101498
Chicago/Turabian StyleKarayigit, Raci, Scott C. Forbes, Zakir Osmanov, Canan Yilmaz, Burak Caglar Yasli, Alireza Naderi, Hakan Buyukcelebi, Daniela Benesova, Tomasz Gabrys, and Ozcan Esen. 2022. "Low and Moderate Doses of Caffeinated Coffee Improve Repeated Sprint Performance in Female Team Sport Athletes" Biology 11, no. 10: 1498. https://doi.org/10.3390/biology11101498