
Stem Cell Transplantation Therapy and Neurological Disorders: Current Status and Future Perspectives

 , , , , ,
, , , , ,  ,
,  , , ,
, , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Characteristics of Various Stem Cells Utilized for Therapeutic Applications
2.1. Embryonic Stem Cells and Induced Pluripotent Stem Cells
Importance of Pluripotent Stem Cells as Cell Replacements
2.2. Neural Stem Cells
2.3. Mesenchymal Stem Cells
2.3.1. Bone Marrow MSCs
2.3.2. Umbilical Cord Blood
3. New Mechanisms of Grafted Stem Cells in Neuroregeneration
4. Recent Advances in the Treatment of Neurological Disorder
4.1. Parkinson’s Disease
4.2. Temporal Lobe Epilepsy
4.3. Multiple Sclerosis
4.4. Huntington’s Disease
4.5. Amyotrophic Lateral Sclerosis
4.6. Glial and Myelin Disorders
4.7. Disorders of the Hippocampus
4.8. Frontotemporal Dementia
5. Stem Cell Therapy and Treatment
5.1. Patient Selection for HSCT in Multiple Sclerosis
5.2. Stem Cell-Based Therapy for Alzheimer’s Disease
5.3. Stem Cells for Treating ALS: Current Developments
5.4. Encapsulation of hPSC-Derived Pancreatic Progeny for Cell Therapy
5.5. Immune Inflection and Suicide Gene Approach for Improving the Safety of Beta Cell Therapy
5.6. Strategies to Enhance Cell Survival after Transplantation: Genetic Modification and Hypoxic Preconditioning
5.7. Transplanted Neural Stem Cell Therapy for Brain Ischemic Stroke
5.8. Stem Cell Transplantation in Stroke Clinical Trials
5.9. Extracellular Vesicles Derived from Mesenchymal Stem Cells Protect against Neonatal Stroke by Interacting with Microglial Cells
6. Neuro-protective Role of SCs in Neuroinflammation
7. Discussion
7.1. Ethical Issues and Safety Concerns Regarding hESC-Based Therapies
7.2. Surgical Safety Aspects of Cell Transplantation
7.3. Optimizing the Therapeutic Efficacy of Neural Stem Cell Transplantation
8. Future Perspectives
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agrawal, M.; Biswas, A. Molecular Diagnostics of Neurodegenerative Disorders. Front. Mol. Biosci. 2015, 2, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Surugiu, R.; Olaru, A.; Hermann, D.M.; Glavan, D.; Catalin, B.; Popa-Wagner, A. Recent Advances in Mono- and Combined Stem Cell Therapies of Stroke in Animal Models and Humans. Int. J. Mol. Sci. 2019, 20, 6029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang-Lazdunski, L.; Matsushita, K.; Hirt, L.; Waeber, C.; Vonsattel, J.P.; Moskowitz, M.A.; Dietrich, W.D. Spinal Cord Ischemia. Development of a Model in the Mouse. Stroke 2000, 31, 208–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasic, V.; Barth, K.; Schmidt, M.H.H. Neurodegeneration and Neuro-Regeneration-Alzheimer’s Disease and Stem Cell Therapy. Int. J. Mol. Sci. 2019, 20, 4277. [Google Scholar] [CrossRef] [Green Version]
- Marchetto, M.C.; Brennand, K.J.; Boyer, L.F.; Gage, F.H. Induced Pluripotent Stem Cells (IPSCs) and Neurological Disease Modeling: Progress and Promises. Hum. Mol. Genet. 2011, 20, R109–R115. [Google Scholar] [CrossRef] [PubMed]
- Rice, C.M.; Halfpenny, C.A.; Scolding, N.J. Stem Cells for the Treatment of Neurological Disease. Transfus. Med. 2003, 13, 351–361. [Google Scholar] [CrossRef] [PubMed]
- Des Rieux, A. Stem Cells and Their Extracellular Vesicles as Natural and Bioinspired Carriers for the Treatment of Neurological Disorders. Curr. Opin. Colloid Interface Sci. 2021, 54, 101460. [Google Scholar] [CrossRef]
- Fu, M.-H.; Li, C.-L.; Lin, H.-L.; Chen, P.-C.; Calkins, M.J.; Chang, Y.-F.; Cheng, P.-H.; Yang, S.-H. Stem Cell Transplantation Therapy in Parkinson’s Disease. SpringerPlus 2015, 4, 597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freed, C.R.; Greene, P.E.; Breeze, R.E.; Tsai, W.Y.; DuMouchel, W.; Kao, R.; Dillon, S.; Winfield, H.; Culver, S.; Trojanowski, J.Q.; et al. Transplantation of Embryonic Dopamine Neurons for Severe Parkinson’s Disease. N. Engl. J. Med. 2001, 344, 710–719. [Google Scholar] [CrossRef]
- Farhadi, M.; Boroujeni, M.E.; Kamrava, S.K.; Bagher, Z.; Tehrani, A.M.; Aghajanpour, F.; Ezi, S.; Soltani, R.; Khatmi, A.; Alizadeh, R. Implantation of Human Olfactory Ecto-Mesenchymal Stem Cells Restores Locomotion in a Rat Model of Parkinson’s Disease. J. Chem. Neuroanat. 2021, 114, 101961. [Google Scholar] [CrossRef]
- Sharma, P.; Sharma, A.; Fayaz, F.; Wakode, S.; Pottoo, F.H. Biological Signatures of Alzheimer’s Disease. Curr. Top. Med. Chem. 2020, 20, 770–781. [Google Scholar] [CrossRef]
- Yu, D.X.; Marchetto, M.C.; Gage, F.H. Therapeutic Translation of IPSCs for Treating Neurological Disease. Cell Stem Cell 2013, 12, 678–688. [Google Scholar] [CrossRef] [Green Version]
- Zhang, P.; Liu, B. Effect of Autologous Hematopoietic Stem Cell Transplantation on Multiple Sclerosis and Neuromyelitis Optica Spectrum Disorder: A PRISMA-Compliant Meta-Analysis. Bone Marrow Transplant. 2020, 55, 1928–1934. [Google Scholar] [CrossRef]
- Noseworthy, J.H.; Lucchinetti, C.; Rodriguez, M.; Weinshenker, B.G. Multiple Sclerosis. N. Engl. J. Med. 2000, 343, 938–952. [Google Scholar] [CrossRef] [PubMed]
- Burt, R.K.; Loh, Y.; Pearce, W.; Beohar, N.; Barr, W.G.; Craig, R.; Wen, Y.; Rapp, J.A.; Kessler, J. Clinical Applications of Blood-Derived and Marrow-Derived Stem Cells for Nonmalignant Diseases. JAMA 2008, 299, 925–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abrahamsson, S.V.; Angelini, D.F.; Dubinsky, A.N.; Morel, E.; Oh, U.; Jones, J.L.; Carassiti, D.; Reynolds, R.; Salvetti, M.; Calabresi, P.A.; et al. Non-Myeloablative Autologous Haematopoietic Stem Cell Transplantation Expands Regulatory Cells and Depletes IL-17 Producing Mucosal-Associated Invariant T Cells in Multiple Sclerosis. Brain J. Neurol. 2013, 136, 2888–2903. [Google Scholar] [CrossRef] [Green Version]
- Muraro, P.A.; Douek, D.C.; Packer, A.; Chung, K.; Guenaga, F.J.; Cassiani-Ingoni, R.; Campbell, C.; Memon, S.; Nagle, J.W.; Hakim, F.T.; et al. Thymic Output Generates a New and Diverse TCR Repertoire after Autologous Stem Cell Transplantation in Multiple Sclerosis Patients. J. Exp. Med. 2005, 201, 805–816. [Google Scholar] [CrossRef] [PubMed]
- Ishii, T.; Eto, K. Fetal Stem Cell Transplantation: Past, Present, and Future. World J. Stem Cells 2014, 6, 404–420. [Google Scholar] [CrossRef]
- Lindvall, O.; Kokaia, Z. Stem Cells for the Treatment of Neurological Disorders. Nature 2006, 441, 1094–1096. [Google Scholar] [CrossRef] [PubMed]
- Hess, D.C.; Borlongan, C.V. Stem Cells and Neurological Diseases. Cell Prolif. 2008, 41 (Suppl. 1), 94–114. [Google Scholar] [CrossRef]
- Bjorklund, L.M.; Sánchez-Pernaute, R.; Chung, S.; Andersson, T.; Chen, I.Y.C.; McNaught, K.S.P.; Brownell, A.-L.; Jenkins, B.G.; Wahlestedt, C.; Kim, K.-S.; et al. Embryonic Stem Cells Develop into Functional Dopaminergic Neurons after Transplantation in a Parkinson Rat Model. Proc. Natl. Acad. Sci. USA 2002, 99, 2344–2349. [Google Scholar] [CrossRef] [Green Version]
- Takagi, Y.; Takahashi, J.; Saiki, H.; Morizane, A.; Hayashi, T.; Kishi, Y.; Fukuda, H.; Okamoto, Y.; Koyanagi, M.; Ideguchi, M.; et al. Dopaminergic Neurons Generated from Monkey Embryonic Stem Cells Function in a Parkinson Primate Model. J. Clin. Investig. 2005, 115, 102–109. [Google Scholar] [CrossRef] [Green Version]
- Ferrari, D.; Sanchez-Pernaute, R.; Lee, H.; Studer, L.; Isacson, O. Transplanted Dopamine Neurons Derived from Primate ES Cells Preferentially Innervate DARPP-32 Striatal Progenitors within the Graft. Eur. J. Neurosci. 2006, 24, 1885–1896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, S.; Qu, Y.; Stewart, T.J.; Howard, M.J.; Chakrabortty, S.; Holekamp, T.F.; McDonald, J.W. Embryonic Stem Cells Differentiate into Oligodendrocytes and Myelinate in Culture and after Spinal Cord Transplantation. Proc. Natl. Acad. Sci. USA 2000, 97, 6126–6131. [Google Scholar] [CrossRef] [Green Version]
- Bottai, D.; Cigognini, D.; Madaschi, L.; Adami, R.; Nicora, E.; Menarini, M.; Di Giulio, A.M.; Gorio, A. Embryonic Stem Cells Promote Motor Recovery and Affect Inflammatory Cell Infiltration in Spinal Cord Injured Mice. Exp. Neurol. 2010, 223, 452–463. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.; Cui, L.; Snider, B.J.; Rivkin, M.; Yu, S.S.; Lee, C.-S.; Adams, L.D.; Gottlieb, D.I.; Johnson, E.M.; Yu, S.P.; et al. Transplantation of Embryonic Stem Cells Overexpressing Bcl-2 Promotes Functional Recovery after Transient Cerebral Ischemia. Neurobiol. Dis. 2005, 19, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.J.; Lee, N.; Park, I.H.; Choi, C.; Jeon, I.; Kwon, J.; Oh, S.H.; Shin, D.A.; Do, J.T.; Lee, D.R.; et al. Therapeutic Potential of Human Induced Pluripotent Stem Cells in Experimental Stroke. Cell Transplant. 2013, 22, 1427–1440. [Google Scholar] [CrossRef] [PubMed]
- Li, P.-J.; Jin, T.; Luo, D.-H.; Shen, T.; Mai, D.-M.; Hu, W.-H.; Mo, H.-Y. Effect of Prolonged Radiotherapy Treatment Time on Survival Outcomes after Intensity-Modulated Radiation Therapy in Nasopharyngeal Carcinoma. PLoS ONE 2015, 10, e0141332. [Google Scholar] [CrossRef]
- Ovsiew, F. What Is Wrong in Conversion Disorder? J. Neurol. Neurosurg. Psychiatry 2003, 74, 557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, K.; Tanabe, K.; Ohnuki, M.; Narita, M.; Ichisaka, T.; Tomoda, K.; Yamanaka, S. Induction of Pluripotent Stem Cells from Adult Human Fibroblasts by Defined Factors. Cell 2007, 131, 861–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abad, M.; Mosteiro, L.; Pantoja, C.; Cañamero, M.; Rayon, T.; Ors, I.; Graña, O.; Megías, D.; Domínguez, O.; Martínez, D.; et al. Reprogramming in Vivo Produces Teratomas and IPS Cells with Totipotency Features. Nature 2013, 502, 340–345. [Google Scholar] [CrossRef] [Green Version]
- Cai, J.; Yang, M.; Poremsky, E.; Kidd, S.; Schneider, J.S.; Iacovitti, L. Dopaminergic Neurons Derived from Human Induced Pluripotent Stem Cells Survive and Integrate into 6-OHDA-Lesioned Rats. Stem Cells Dev. 2010, 19, 1017–1023. [Google Scholar] [CrossRef] [Green Version]
- Wernig, M.; Zhao, J.-P.; Pruszak, J.; Hedlund, E.; Fu, D.; Soldner, F.; Broccoli, V.; Constantine-Paton, M.; Isacson, O.; Jaenisch, R. Neurons Derived from Reprogrammed Fibroblasts Functionally Integrate into the Fetal Brain and Improve Symptoms of Rats with Parkinson’s Disease. Proc. Natl. Acad. Sci. USA 2008, 105, 5856–5861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ray, S.; Maunsell, J.H.R. Different Origins of Gamma Rhythm and High-Gamma Activity in Macaque Visual Cortex. PLOS Biol. 2011, 9, e1000610. [Google Scholar] [CrossRef] [Green Version]
- Swistowski, A.; Peng, J.; Liu, Q.; Mali, P.; Rao, M.S.; Cheng, L.; Zeng, X. Efficient Generation of Functional Dopaminergic Neurons from Human Induced Pluripotent Stem Cells under Defined Conditions. Stem Cells 2010, 28, 1893–1904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soldner, F.; Hockemeyer, D.; Beard, C.; Gao, Q.; Bell, G.W.; Cook, E.G.; Hargus, G.; Blak, A.; Cooper, O.; Mitalipova, M.; et al. Parkinson’s Disease Patient-Derived Induced Pluripotent Stem Cells Free of Viral Reprogramming Factors. Cell 2009, 136, 964–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimos, J.T.; Rodolfa, K.T.; Niakan, K.K.; Weisenthal, L.M.; Mitsumoto, H.; Chung, W.; Croft, G.F.; Saphier, G.; Leibel, R.; Goland, R.; et al. Induced Pluripotent Stem Cells Generated from Patients with ALS Can Be Differentiated into Motor Neurons. Science 2008, 321, 1218–1221. [Google Scholar] [CrossRef] [Green Version]
- Park, I.-H.; Arora, N.; Huo, H.; Maherali, N.; Ahfeldt, T.; Shimamura, A.; Lensch, M.W.; Cowan, C.; Hochedlinger, K.; Daley, G.Q. Disease-Specific Induced Pluripotent Stem Cells. Cell 2008, 134, 877–886. [Google Scholar] [CrossRef] [Green Version]
- Esteban, M.A.; Xu, J.; Yang, J.; Peng, M.; Qin, D.; Li, W.; Jiang, Z.; Chen, J.; Deng, K.; Zhong, M.; et al. Generation of Induced Pluripotent Stem Cell Lines from Tibetan Miniature Pig. J. Biol. Chem. 2009, 284, 17634–17640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, M.-Y.; Kim, D.; Kim, C.-H.; Kang, H.-C.; Yang, E.; Moon, J.-I.; Ko, S.; Park, J.; Park, K.-S.; Lee, K.-A.; et al. Direct Reprogramming of Rat Neural Precursor Cells and Fibroblasts into Pluripotent Stem Cells. PLoS ONE 2010, 5, e9838. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Zhu, F.; Yong, J.; Zhang, P.; Hou, P.; Li, H.; Jiang, W.; Cai, J.; Liu, M.; Cui, K.; et al. Generation of Induced Pluripotent Stem Cells from Adult Rhesus Monkey Fibroblasts. Cell Stem Cell 2008, 3, 587–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Zhang, Y.; Mishra, A.; Tardif, S.D.; Hornsby, P.J. Generation of Induced Pluripotent Stem Cells from Newborn Marmoset Skin Fibroblasts. Stem Cell Res. 2010, 4, 180–188. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.B.; Greber, B.; Araúzo-Bravo, M.J.; Meyer, J.; Park, K.I.; Zaehres, H.; Schöler, H.R. Direct Reprogramming of Human Neural Stem Cells by OCT4. Nature 2009, 461, 649–653. [Google Scholar] [CrossRef] [PubMed]
- Kaji, K.; Norrby, K.; Paca, A.; Mileikovsky, M.; Mohseni, P.; Woltjen, K. Virus-Free Induction of Pluripotency and Subsequent Excision of Reprogramming Factors. Nature 2009, 458, 771–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woltjen, K.; Michael, I.P.; Mohseni, P.; Desai, R.; Mileikovsky, M.; Hämäläinen, R.; Cowling, R.; Wang, W.; Liu, P.; Gertsenstein, M.; et al. PiggyBac Transposition Reprograms Fibroblasts to Induced Pluripotent Stem Cells. Nature 2009, 458, 766–770. [Google Scholar] [CrossRef]
- Okita, K.; Nakagawa, M.; Hyenjong, H.; Ichisaka, T.; Yamanaka, S. Generation of Mouse Induced Pluripotent Stem Cells without Viral Vectors. Science 2008, 322, 949–953. [Google Scholar] [CrossRef]
- Yu, J.; Hu, K.; Smuga-Otto, K.; Tian, S.; Stewart, R.; Slukvin, I.I.; Thomson, J.A. Human Induced Pluripotent Stem Cells Free of Vector and Transgene Sequences. Science 2009, 324, 797–801. [Google Scholar] [CrossRef] [Green Version]
- Warren, L.; Manos, P.D.; Ahfeldt, T.; Loh, Y.-H.; Li, H.; Lau, F.; Ebina, W.; Mandal, P.K.; Smith, Z.D.; Meissner, A.; et al. Highly Efficient Reprogramming to Pluripotency and Directed Differentiation of Human Cells with Synthetic Modified MRNA. Cell Stem Cell 2010, 7, 618–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, H.; Wu, S.; Joo, J.Y.; Zhu, S.; Han, D.W.; Lin, T.; Trauger, S.; Bien, G.; Yao, S.; Zhu, Y.; et al. Generation of Induced Pluripotent Stem Cells Using Recombinant Proteins. Cell Stem Cell 2009, 4, 381–384. [Google Scholar] [CrossRef] [Green Version]
- Lyssiotis, C.A.; Foreman, R.K.; Staerk, J.; Garcia, M.; Mathur, D.; Markoulaki, S.; Hanna, J.; Lairson, L.L.; Charette, B.D.; Bouchez, L.C.; et al. Reprogramming of Murine Fibroblasts to Induced Pluripotent Stem Cells with Chemical Complementation of Klf4. Proc. Natl. Acad. Sci. USA 2009, 106, 8912–8917. [Google Scholar] [CrossRef] [Green Version]
- Jang, J.; Yoo, J.-E.; Lee, J.-A.; Lee, D.R.; Kim, J.Y.; Huh, Y.J.; Kim, D.-S.; Park, C.-Y.; Hwang, D.-Y.; Kim, H.-S.; et al. Disease-Specific Induced Pluripotent Stem Cells: A Platform for Human Disease Modeling and Drug Discovery. Exp. Mol. Med. 2012, 44, 202–213. [Google Scholar] [CrossRef] [Green Version]
- Chou, Y.-F.; Chen, H.-H.; Eijpe, M.; Yabuuchi, A.; Chenoweth, J.G.; Tesar, P.; Lu, J.; McKay, R.D.G.; Geijsen, N. The Growth Factor Environment Defines Distinct Pluripotent Ground States in Novel Blastocyst-Derived Stem Cells. Cell 2008, 135, 449–461. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Cheung, H.-H. Stem Cell-Based Therapies for Parkinson Disease. Int. J. Mol. Sci. 2020, 21, 8060. [Google Scholar] [CrossRef]
- Saeedi, P.; Halabian, R.; Imani Fooladi, A.A. A Revealing Review of Mesenchymal Stem Cells Therapy, Clinical Perspectives and Modification Strategies. Stem Cell Investig. 2019, 6, 34. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.J.; Peacock, S.; Chaudhry, A.N.; Bradley, J.A.; Bolton, E.M. Generating an IPSC Bank for HLA-Matched Tissue Transplantation Based on Known Donor and Recipient HLA Types. Cell Stem Cell 2012, 11, 147–152. [Google Scholar] [CrossRef] [Green Version]
- Nakatsuji, N.; Nakajima, F.; Tokunaga, K. HLA-Haplotype Banking and IPS Cells. Nat. Biotechnol. 2008, 26, 739–740. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Huh, J.Y.; Turner, D.M.; Lee, S.; Robinson, J.; Stein, J.E.; Shim, S.H.; Hong, C.P.; Kang, M.S.; Nakagawa, M.; et al. Repurposing the Cord Blood Bank for Haplobanking of HLA-Homozygous IPSCs and Their Usefulness to Multiple Populations. Stem Cells 2018, 36, 1552–1566. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, Y.; Choi, J.; Park, N.; Kang, J.; Kim, M.; Kim, Y.; Ju, J.H. Development of Immunocompatible Pluripotent Stem Cells via CRISPR-Based Human Leukocyte Antigen Engineering. Exp. Mol. Med. 2019, 51, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vescovi, A.L.; Gritti, A.; Galli, R.; Parati, E.A. Isolation and Intracerebral Grafting of Nontransformed Multipotential Embryonic Human CNS Stem Cells. J. Neurotrauma 1999, 16, 689–693. [Google Scholar] [CrossRef] [PubMed]
- Gritti, A.; Frölichsthal-Schoeller, P.; Galli, R.; Parati, E.A.; Cova, L.; Pagano, S.F.; Bjornson, C.R.; Vescovi, A.L. Epidermal and Fibroblast Growth Factors Behave as Mitogenic Regulators for a Single Multipotent Stem Cell-like Population from the Subventricular Region of the Adult Mouse Forebrain. J. Neurosci. Off. J. Soc. Neurosci. 1999, 19, 3287–3297. [Google Scholar] [CrossRef] [Green Version]
- Bottai, D.; Fiocco, R.; Gelain, F.; Defilippis, L.; Galli, R.; Gritti, A.; Vescovi, L.A. Neural Stem Cells in the Adult Nervous System. J. Hematother. Stem Cell Res. 2003, 12, 655–670. [Google Scholar] [CrossRef] [PubMed]
- Pluchino, S.; Quattrini, A.; Brambilla, E.; Gritti, A.; Salani, G.; Dina, G.; Galli, R.; Del Carro, U.; Amadio, S.; Bergami, A.; et al. Injection of Adult Neurospheres Induces Recovery in a Chronic Model of Multiple Sclerosis. Nature 2003, 422, 688–694. [Google Scholar] [CrossRef] [PubMed]
- Bottai, D.; Madaschi, L.; Di Giulio, A.M.; Gorio, A. Viability-Dependent Promoting Action of Adult Neural Precursors in Spinal Cord Injury. Mol. Med. 2008, 14, 634–644. [Google Scholar] [CrossRef]
- Fiorio, M.; Tinazzi, M.; Aglioti, S.M. Selective Impairment of Hand Mental Rotation in Patients with Focal Hand Dystonia. Brain J. Neurol. 2006, 129, 47–54. [Google Scholar] [CrossRef] [Green Version]
- Xu, L.; Shen, P.; Hazel, T.; Johe, K.; Koliatsos, V.E. Dual Transplantation of Human Neural Stem Cells into Cervical and Lumbar Cord Ameliorates Motor Neuron Disease in SOD1 Transgenic Rats. Neurosci. Lett. 2011, 494, 222–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Coppi, P.; Bartsch, G.; Siddiqui, M.M.; Xu, T.; Santos, C.C.; Perin, L.; Mostoslavsky, G.; Serre, A.C.; Snyder, E.Y.; Yoo, J.J.; et al. Isolation of Amniotic Stem Cell Lines with Potential for Therapy. Nat. Biotechnol. 2007, 25, 100–106. [Google Scholar] [CrossRef]
- Bottai, D.; Cigognini, D.; Nicora, E.; Moro, M.; Grimoldi, M.G.; Adami, R.; Abrignani, S.; Marconi, A.M.; Di Giulio, A.M.; Gorio, A. Third Trimester Amniotic Fluid Cells with the Capacity to Develop Neural Phenotypes and with Heterogeneity among Sub-Populations. Restor. Neurol. Neurosci. 2012, 30, 55–68. [Google Scholar] [CrossRef]
- Moroni, L.; Fornasari, P.M. Human Mesenchymal Stem Cells: A Bank Perspective on the Isolation, Characterization and Potential of Alternative Sources for the Regeneration of Musculoskeletal Tissues. J. Cell. Physiol. 2013, 228, 680–687. [Google Scholar] [CrossRef]
- Rao, M.S.; Mattson, M.P. Stem Cells and Aging: Expanding the Possibilities. Mech. Ageing Dev. 2001, 122, 713–734. [Google Scholar] [CrossRef]
- Rubio, D.; Garcia-Castro, J.; Martín, M.C.; de la Fuente, R.; Cigudosa, J.C.; Lloyd, A.C.; Bernad, A. Spontaneous Human Adult Stem Cell Transformation. Cancer Res. 2005, 65, 3035–3039. [Google Scholar] [CrossRef] [Green Version]
- De la Fuente, R.; Bernad, A.; Garcia-Castro, J.; Martin, M.C.; Cigudosa, J.C. Retraction: Spontaneous Human Adult Stem Cell Transformation. Cancer Res. 2010, 70, 6682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobolak, J.; Dinnyes, A.; Memic, A.; Khademhosseini, A.; Mobasheri, A. Mesenchymal Stem Cells: Identification, Phenotypic Characterization, Biological Properties and Potential for Regenerative Medicine through Biomaterial Micro-Engineering of Their Niche. Methods 2016, 99, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Bianco, P. “Mesenchymal” Stem Cells. Annu. Rev. Cell Dev. Biol. 2014, 30, 677–704. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Zhang, W.; Ran, Q.; Xiang, Y.; Zhong, J.F.; Li, S.C.; Li, Z. The Differentiation Balance of Bone Marrow Mesenchymal Stem Cells Is Crucial to Hematopoiesis. Stem Cells Int. 2018, 2018, 1540148. [Google Scholar] [CrossRef]
- Miao, C.; Lei, M.; Hu, W.; Han, S.; Wang, Q. A Brief Review: The Therapeutic Potential of Bone Marrow Mesenchymal Stem Cells in Myocardial Infarction. Stem Cell Res. Ther. 2017, 8, 242. [Google Scholar] [CrossRef] [Green Version]
- Klontzas, M.E.; Kenanidis, E.I.; Heliotis, M.; Tsiridis, E.; Mantalaris, A. Bone and Cartilage Regeneration with the Use of Umbilical Cord Mesenchymal Stem Cells. Expert Opin. Biol. Ther. 2015, 15, 1541–1552. [Google Scholar] [CrossRef] [PubMed]
- Kargozar, S.; Lotfibakhshaiesh, N.; Ai, J.; Mozafari, M.; Brouki Milan, P.; Hamzehlou, S.; Barati, M.; Baino, F.; Hill, R.G.; Joghataei, M.T. Strontium- and Cobalt-Substituted Bioactive Glasses Seeded with Human Umbilical Cord Perivascular Cells to Promote Bone Regeneration via Enhanced Osteogenic and Angiogenic Activities. Acta Biomater. 2017, 58, 502–514. [Google Scholar] [CrossRef]
- Tsang, W.P.; Shu, Y.; Kwok, P.L.; Zhang, F.; Lee, K.K.H.; Tang, M.K.; Li, G.; Chan, K.M.; Chan, W.-Y.; Wan, C. CD146+ Human Umbilical Cord Perivascular Cells Maintain Stemness under Hypoxia and as a Cell Source for Skeletal Regeneration. PLoS ONE 2013, 8, e76153. [Google Scholar] [CrossRef] [PubMed]
- Bosch, J.; Houben, A.P.; Radke, T.F.; Stapelkamp, D.; Bünemann, E.; Balan, P.; Buchheiser, A.; Liedtke, S.; Kögler, G. Distinct Differentiation Potential of “MSC” Derived from Cord Blood and Umbilical Cord: Are Cord-Derived Cells True Mesenchymal Stromal Cells? Stem Cells Dev. 2012, 21, 1977–1988. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.J.; Bae, Y.K.; Kim, M.; Kwon, S.-J.; Jeon, H.B.; Choi, S.J.; Kim, S.W.; Yang, Y.S.; Oh, W.; Chang, J.W. Comparative Analysis of Human Mesenchymal Stem Cells from Bone Marrow, Adipose Tissue, and Umbilical Cord Blood as Sources of Cell Therapy. Int. J. Mol. Sci. 2013, 14, 17986–18001. [Google Scholar] [CrossRef] [PubMed]
- Bosch, J.; Houben, A.P.; Hennicke, T.; Deenen, R.; Köhrer, K.; Liedtke, S.; Kögler, G. Comparing the Gene Expression Profile of Stromal Cells from Human Cord Blood and Bone Marrow: Lack of the Typical “Bone” Signature in Cord Blood Cells. Stem Cells Int. 2013, 2013, e631984. [Google Scholar] [CrossRef] [PubMed]
- Maher, S.; Kolieb, E.; Sabik, N.A.; Abd-Elhalim, D.; El-Serafi, A.T.; El-Wazir, Y. Comparison of the Osteogenic Differentiation Potential of Mesenchymal Cells Isolated from Human Bone Marrow, Umbilical Cord Blood and Placenta Derived Stem Cells. Beni-Suef Univ. J. Basic Appl. Sci. 2015, 4, 80–85. [Google Scholar] [CrossRef] [Green Version]
- McDonald, C.A.; Fahey, M.C.; Jenkin, G.; Miller, S.L. Umbilical Cord Blood Cells for Treatment of Cerebral Palsy; Timing and Treatment Options. Pediatr. Res. 2018, 83, 333–344. [Google Scholar] [CrossRef]
- Jin, Y.-Z.; Lee, J.H. Mesenchymal Stem Cell Therapy for Bone Regeneration. Clin. Orthop. Surg. 2018, 10, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Steinbeck, J.A.; Studer, L. Moving Stem Cells to the Clinic: Potential and Limitations for Brain Repair. Neuron 2015, 86, 187–206. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, T.; Adler, A.F.; Mattsson, B.; Hoban, D.B.; Nolbrant, S.; Wahlestedt, J.N.; Kirkeby, A.; Grealish, S.; Björklund, A.; Parmar, M. Target-Specific Forebrain Projections and Appropriate Synaptic Inputs of HESC-Derived Dopamine Neurons Grafted to the Midbrain of Parkinsonian Rats. J. Comp. Neurol. 2018, 526, 2133–2146. [Google Scholar] [CrossRef]
- Carpenter, M.K. Regulatory Considerations for Pluripotent Stem Cell Therapies. Prog. Brain Res. 2017, 230, 151–163. [Google Scholar] [CrossRef]
- Dunnett, S.B.; Rosser, A.E. Challenges for Taking Primary and Stem Cells into Clinical Neurotransplantation Trials for Neurodegenerative Disease. Neurobiol. Dis. 2014, 61, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Forraz, N.; Wright, K.E.; Jurga, M.; McGuckin, C.P. Experimental Therapies for Repair of the Central Nervous System: Stem Cells and Tissue Engineering. J. Tissue Eng. Regen. Med. 2013, 7, 523–536. [Google Scholar] [CrossRef]
- Cossetti, C.; Alfaro-Cervello, C.; Donegà, M.; Tyzack, G.; Pluchino, S. New Perspectives of Tissue Remodelling with Neural Stem and Progenitor Cell-Based Therapies. Cell Tissue Res. 2012, 349, 321–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dzamba, D.; Harantova, L.; Butenko, O.; Anderova, M. Glial Cells—The Key Elements of Alzheimer’s Disease. Curr. Alzheimer Res. 2016, 13, 894–911. [Google Scholar] [CrossRef] [PubMed]
- Mendonça, L.S.; Nóbrega, C.; Hirai, H.; Kaspar, B.K.; Pereira de Almeida, L. Transplantation of Cerebellar Neural Stem Cells Improves Motor Coordination and Neuropathology in Machado-Joseph Disease Mice. Brain J. Neurol. 2015, 138, 320–335. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Yao, W.; Deng, Q.; Zhang, X.; Zhang, J. Protective Effects of BDNF Overexpression Bone Marrow Stromal Cell Transplantation in Rat Models of Traumatic Brain Injury. J. Mol. Neurosci. MN 2013, 49, 409–416. [Google Scholar] [CrossRef]
- Ma, H.; Yu, B.; Kong, L.; Zhang, Y.; Shi, Y. Neural Stem Cells Over-Expressing Brain-Derived Neurotrophic Factor (BDNF) Stimulate Synaptic Protein Expression and Promote Functional Recovery Following Transplantation in Rat Model of Traumatic Brain Injury. Neurochem. Res. 2012, 37, 69–83. [Google Scholar] [CrossRef]
- Bacigaluppi, M.; Pluchino, S.; Peruzzotti-Jametti, L.; Jametti, L.P.; Kilic, E.; Kilic, U.; Salani, G.; Brambilla, E.; West, M.J.; Comi, G.; et al. Delayed Post-Ischaemic Neuroprotection Following Systemic Neural Stem Cell Transplantation Involves Multiple Mechanisms. Brain J. Neurol. 2009, 132, 2239–2251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boltze, J.; Zille, M.; Schilling, S.; Gelderblom, M.; Bix, G.J.; Walczak, P.; Harms, C.; Rosado-de-Castro, P.H.; Pinteaux, E. Cutting-Edge Approaches for CNS Protection and Repair: Focus on Vascular and Degenerative Disorders; Frontiers Media SA: Lausanne, Switzerland, 2021; ISBN 978-2-88971-177-2. [Google Scholar]
- Camponeschi, F.; Valensin, D.; Tessari, I.; Bubacco, L.; Dell’Acqua, S.; Casella, L.; Monzani, E.; Gaggelli, E.; Valensin, G. Copper(I)-α-Synuclein Interaction: Structural Description of Two Independent and Competing Metal Binding Sites. Inorg. Chem. 2013, 52, 1358–1367. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.S.S.J.; Santosh, W. Metallomic Profiling and Linkage Map Analysis of Early Parkinson’s Disease: A New Insight to Aluminum Marker for the Possible Diagnosis. PLoS ONE 2010, 5, e11252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younes-Mhenni, S.; Aissi, M.; Mokni, N.; Boughammoura-Bouatay, A.; Chebel, S.; Frih-Ayed, M.; Kerkeni, A.; Bost, M.; Chazot, G.; Sfar, M.T.; et al. Serum Copper, Zinc and Selenium Levels in Tunisian Patients with Parkinson’s Disease. Tunis. Med. 2013, 91, 402–405. [Google Scholar] [PubMed]
- Tolleson, C.M.; Fang, J.Y. Advances in the Mechanisms of Parkinson’s Disease. Discov. Med. 2013, 15, 61–66. [Google Scholar] [PubMed]
- Pringsheim, T.; Jette, N.; Frolkis, A.; Steeves, T.D.L. The Prevalence of Parkinson’s Disease: A Systematic Review and Meta-Analysis. Mov. Disord. Off. J. Mov. Disord. Soc. 2014, 29, 1583–1590. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Sun, T.; An, J.; Wen, L.; Liu, F.; Bu, Z.; Cui, Y.; Feng, J. Potential Roles of Exosomes in Parkinson’s Disease: From Pathogenesis, Diagnosis, and Treatment to Prognosis. Front. Cell Dev. Biol. 2020, 8, 86. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.-H.; Wu, K.-C.; Harn, H.-J.; Lin, S.-Z.; Ding, D.-C. Exosomes and Stem Cells in Degenerative Disease Diagnosis and Therapy. Cell Transplant. 2018, 27, 349–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teixeira, F.G.; Carvalho, M.M.; Panchalingam, K.M.; Rodrigues, A.J.; Mendes-Pinheiro, B.; Anjo, S.; Manadas, B.; Behie, L.A.; Sousa, N.; Salgado, A.J. Impact of the Secretome of Human Mesenchymal Stem Cells on Brain Structure and Animal Behavior in a Rat Model of Parkinson’s Disease. Stem Cells Transl. Med. 2017, 6, 634–646. [Google Scholar] [CrossRef] [PubMed]
- Clark, C.M.; Xie, S.; Chittams, J.; Ewbank, D.; Peskind, E.; Galasko, D.; Morris, J.C.; McKeel, D.W.; Farlow, M.; Weitlauf, S.L.; et al. Cerebrospinal Fluid Tau and Beta-Amyloid: How Well Do These Biomarkers Reflect Autopsy-Confirmed Dementia Diagnoses? Arch. Neurol. 2003, 60, 1696–1702. [Google Scholar] [CrossRef] [Green Version]
- Xin, H.; Katakowski, M.; Wang, F.; Qian, J.-Y.; Liu, X.S.; Ali, M.M.; Buller, B.; Zhang, Z.G.; Chopp, M. MicroRNA-17–92 Cluster in Exosomes Enhance Neuroplasticity and Functional Recovery After Stroke in Rats. Stroke 2017, 48, 747–753. [Google Scholar] [CrossRef]
- Mohanraj, R.; Norrie, J.; Stephen, L.J.; Kelly, K.; Hitiris, N.; Brodie, M.J. Mortality in Adults with Newly Diagnosed and Chronic Epilepsy: A Retrospective Comparative Study. Lancet Neurol. 2006, 5, 481–487. [Google Scholar] [CrossRef]
- Lawn, N.D.; Bamlet, W.R.; Radhakrishnan, K.; O’Brien, P.C.; So, E.L. Injuries Due to Seizures in Persons with Epilepsy: A Population-Based Study. Neurology 2004, 63, 1565–1570. [Google Scholar] [CrossRef]
- McCagh, J.; Fisk, J.E.; Baker, G.A. Epilepsy, Psychosocial and Cognitive Functioning. Epilepsy Res. 2009, 86, 1–14. [Google Scholar] [CrossRef]
- Jobst, B.C.; Cascino, G.D. Resective Epilepsy Surgery for Drug-Resistant Focal Epilepsy: A Review. JAMA 2015, 313, 285–293. [Google Scholar] [CrossRef]
- Krumholz, A.; Wiebe, S.; Gronseth, G.; Shinnar, S.; Levisohn, P.; Ting, T.; Hopp, J.; Shafer, P.; Morris, H.; Seiden, L.; et al. Practice Parameter: Evaluating an Apparent Unprovoked First Seizure in Adults (an Evidence-Based Review): Report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Neurology 2007, 69, 1996–2007. [Google Scholar] [CrossRef] [Green Version]
- Kang, J.Y.; Wu, C.; Tracy, J.; Lorenzo, M.; Evans, J.; Nei, M.; Skidmore, C.; Mintzer, S.; Sharan, A.D.; Sperling, M.R. Laser Interstitial Thermal Therapy for Medically Intractable Mesial Temporal Lobe Epilepsy. Epilepsia 2016, 57, 325–334. [Google Scholar] [CrossRef]
- Arcos, A.; Romero, L.; Gelabert, M.; Prieto, A.; Pardo, J.; Osorio, X.R.; Arráez, M.A. Can We Predict the Response in the Treatment of Epilepsy with Vagus Nerve Stimulation? Neurosurg. Rev. 2014, 37, 661–668. [Google Scholar] [CrossRef]
- Kuba, R.; Brázdil, M.; Novák, Z.; Chrastina, J.; Rektor, I. Effect of Vagal Nerve Stimulation on Patients with Bitemporal Epilepsy. Eur. J. Neurol. 2003, 10, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Guerreiro, C.A.M. Epilepsy: Is There Hope? Indian J. Med. Res. 2016, 144, 657–660. [Google Scholar] [CrossRef]
- Wang, A.J.; Bick, S.K.; Williams, Z.M. Vagus Nerve Stimulation versus Responsive Neurostimulator System in Patients with Temporal Lobe Epilepsy. Stereotact. Funct. Neurosurg. 2020, 98, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Kobelt, G.; Thompson, A.; Berg, J.; Gannedahl, M.; Eriksson, J. New Insights into the Burden and Costs of Multiple Sclerosis in Europe. Mult. Scler. J. 2017, 23, 1123–1136. [Google Scholar] [CrossRef]
- Browne, P.; Chandraratna, D.; Angood, C.; Tremlett, H.; Baker, C.; Taylor, B.V.; Thompson, A.J. Atlas of Multiple Sclerosis 2013: A Growing Global Problem with Widespread Inequity. Neurology 2014, 83, 1022–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristiano, E.; Patrucco, L.; Miguez, J.; Giunta, D.; Peroni, J.; Rojas, J.I. Increasing Incidence of Multiple Sclerosis among Women in Buenos Aires: A 22 Year Health Maintenance Organization Based Study. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2016, 37, 1621–1626. [Google Scholar] [CrossRef] [PubMed]
- Greenfield, A.L.; Hauser, S.L. B-Cell Therapy for Multiple Sclerosis: Entering an Era. Ann. Neurol. 2018, 83, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Leray, E.; Yaouanq, J.; Le Page, E.; Coustans, M.; Laplaud, D.; Oger, J.; Edan, G. Evidence for a Two-Stage Disability Progression in Multiple Sclerosis. Brain 2010, 133, 1900–1913. [Google Scholar] [CrossRef] [Green Version]
- Coles, A.J.; Cox, A.; Le Page, E.; Jones, J.; Trip, S.A.; Deans, J.; Seaman, S.; Miller, D.H.; Hale, G.; Waldmann, H.; et al. The Window of Therapeutic Opportunity in Multiple Sclerosis: Evidence from Monoclonal Antibody Therapy. J. Neurol. 2006, 253, 98–108. [Google Scholar] [CrossRef]
- Ramagopalan, S.V.; Dobson, R.; Meier, U.C.; Giovannoni, G. Multiple Sclerosis: Risk Factors, Prodromes, and Potential Causal Pathways. Lancet Neurol. 2010, 9, 727–739. [Google Scholar] [CrossRef]
- Dobson, R.; Giovannoni, G. Multiple Sclerosis—A Review. Eur. J. Neurol. 2019, 26, 27–40. [Google Scholar] [CrossRef] [Green Version]
- Rizvi, S.A.; Stone, J.A.; Chaudhry, S.T.; Haddad, N.; Wong, B.; Grimes, J.O. Clinical decision-making in the management of multiple sclerosis. In Clinical Neuroimmunology: Multiple Sclerosis and Related Disorders; Rizvi, S.A., Cahill, J.F., Coyle, P.K., Eds.; Current Clinical Neurology; Springer International Publishing: Cham, Switzerland, 2020; pp. 159–177. ISBN 978-3-030-24436-1. [Google Scholar]
- Gross, R.H.; Corboy, J.R. Monitoring, Switching, and Stopping Multiple Sclerosis Disease-Modifying Therapies. Continuum 2019, 25, 715–735. [Google Scholar] [CrossRef]
- Li, Z.; Liu, F.; He, X.; Yang, X.; Shan, F.; Feng, J. Exosomes Derived from Mesenchymal Stem Cells Attenuate Inflammation and Demyelination of the Central Nervous System in EAE Rats by Regulating the Polarization of Microglia. Int. Immunopharmacol. 2019, 67, 268–280. [Google Scholar] [CrossRef]
- Farinazzo, A.; Angiari, S.; Turano, E.; Bistaffa, E.; Dusi, S.; Ruggieri, S.; Bonafede, R.; Mariotti, R.; Constantin, G.; Bonetti, B. Nanovesicles from Adipose-Derived Mesenchymal Stem Cells Inhibit T Lymphocyte Trafficking and Ameliorate Chronic Experimental Autoimmune Encephalomyelitis. Sci. Rep. 2018, 8, 7473. [Google Scholar] [CrossRef]
- Hands, S.L.; Mason, R.; Sajjad, M.U.; Giorgini, F.; Wyttenbach, A. Metallothioneins and Copper Metabolism Are Candidate Therapeutic Targets in Huntington’s Disease. Biochem. Soc. Trans. 2010, 38, 552–558. [Google Scholar] [CrossRef] [Green Version]
- Dusek, P.; Jankovic, J.; Le, W. Iron Dysregulation in Movement Disorders. Neurobiol. Dis. 2012, 46, 1–18. [Google Scholar] [CrossRef]
- Malecki, E.A.; Devenyi, A.G.; Beard, J.L.; Connor, J.R. Existing and Emerging Mechanisms for Transport of Iron and Manganese to the Brain. J. Neurosci. Res. 1999, 56, 113–122. [Google Scholar] [CrossRef]
- Caron, N.S.; Wright, G.E.; Hayden, M.R. Huntington Disease. In GeneReviews®; Adam, M.P., Ardinger, H.H., Pagon, R.A., Wallace, S.E., Bean, L.J., Mirzaa, G., Amemiya, A., Eds.; University of Washington, Seattle: Seattle, WA, USA, 1993. [Google Scholar]
- Croese, T.; Furlan, R. Extracellular Vesicles in Neurodegenerative Diseases. Mol. Asp. Med. 2018, 60, 52–61. [Google Scholar] [CrossRef]
- Lee, M.; Liu, T.; Im, W.; Kim, M. Exosomes from Adipose-Derived Stem Cells Ameliorate Phenotype of Huntington’s Disease in Vitro Model. Eur. J. Neurosci. 2016, 44, 2114–2119. [Google Scholar] [CrossRef]
- Lee, S.-T.; Im, W.; Ban, J.-J.; Lee, M.; Jung, K.-H.; Lee, S.K.; Chu, K.; Kim, M. Exosome-Based Delivery of MiR-124 in a Huntington’s Disease Model. J. Mov. Disord. 2017, 10, 45–52. [Google Scholar] [CrossRef]
- Trumbull, K.A.; Beckman, J.S. A Role for Copper in the Toxicity of Zinc-Deficient Superoxide Dismutase to Motor Neurons in Amyotrophic Lateral Sclerosis. Antioxid. Redox Signal. 2009, 11, 1627–1639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinceti, M.; Bottecchi, I.; Fan, A.; Finkelstein, Y.; Mandrioli, J. Are Environmental Exposures to Selenium, Heavy Metals, and Pesticides Risk Factors for Amyotrophic Lateral Sclerosis? Rev. Environ. Health 2012, 27, 19–41. [Google Scholar] [CrossRef]
- Kanias, G.D.; Kapaki, E. Trace Elements, Age, and Sex in Amyotrophic Lateral Sclerosis Disease. Biol. Trace Elem. Res. 1997, 56, 187–201. [Google Scholar] [CrossRef] [PubMed]
- Ignjatović, A.; Stević, Z.; Lavrnić, D.; Nikolić-Kokić, A.; Blagojević, D.; Spasić, M.; Spasojević, I. Inappropriately Chelated Iron in the Cerebrospinal Fluid of Amyotrophic Lateral Sclerosis Patients. Amyotroph. Lateral Scler. Off. Publ. World Fed. Neurol. Res. Group Mot. Neuron Dis. 2012, 13, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Roos, P.M.; Lierhagen, S.; Flaten, T.P.; Syversen, T.; Vesterberg, O.; Nordberg, M. Manganese in Cerebrospinal Fluid and Blood Plasma of Patients with Amyotrophic Lateral Sclerosis. Exp. Biol. Med. 2012, 237, 803–810. [Google Scholar] [CrossRef]
- Mitchell, R.M.; Simmons, Z.; Beard, J.L.; Stephens, H.E.; Connor, J.R. Plasma Biomarkers Associated with ALS and Their Relationship to Iron Homeostasis. Muscle Nerve 2010, 42, 95–103. [Google Scholar] [CrossRef]
- Nadjar, Y.; Gordon, P.; Corcia, P.; Bensimon, G.; Pieroni, L.; Meininger, V.; Salachas, F. Elevated Serum Ferritin Is Associated with Reduced Survival in Amyotrophic Lateral Sclerosis. PLoS ONE 2012, 7, e45034. [Google Scholar] [CrossRef]
- Pfaender, S.; Grabrucker, A.M. Characterization of Biometal Profiles in Neurological Disorders. Met. Integr. Biometal Sci. 2014, 6, 960–977. [Google Scholar] [CrossRef]
- Azevedo, F.A.C.; Carvalho, L.R.B.; Grinberg, L.T.; Farfel, J.M.; Ferretti, R.E.L.; Leite, R.E.P.; Jacob Filho, W.; Lent, R.; Herculano-Houzel, S. Equal Numbers of Neuronal and Nonneuronal Cells Make the Human Brain an Isometrically Scaled-up Primate Brain. J. Comp. Neurol. 2009, 513, 532–541. [Google Scholar] [CrossRef]
- Pelvig, D.P.; Pakkenberg, H.; Stark, A.K.; Pakkenberg, B. Neocortical Glial Cell Numbers in Human Brains. Neurobiol. Aging 2008, 29, 1754–1762. [Google Scholar] [CrossRef]
- Dwork, A.J.; Mancevski, B.; Rosoklija, G. White Matter and Cognitive Function in Schizophrenia. Int. J. Neuropsychopharmacol. 2007, 10, 513–536. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, H.-G.; Steiner, J.; Guest, P.C.; Dobrowolny, H.; Bogerts, B. Glial Cells as Key Players in Schizophrenia Pathology: Recent Insights and Concepts of Therapy. Schizophr. Res. 2015, 161, 4–18. [Google Scholar] [CrossRef]
- Yamamuro, K.; Kimoto, S.; Rosen, K.M.; Kishimoto, T.; Makinodan, M. Potential Primary Roles of Glial Cells in the Mechanisms of Psychiatric Disorders. Front. Cell. Neurosci. 2015, 9, 154. [Google Scholar] [CrossRef] [Green Version]
- Walterfang, M.; Wood, S.J.; Velakoulis, D.; Copolov, D.; Pantelis, C. Diseases of White Matter and Schizophrenia-like Psychosis. Aust. N. Z. J. Psychiatry 2005, 39, 746–756. [Google Scholar] [CrossRef] [PubMed]
- Mighdoll, M.I.; Tao, R.; Kleinman, J.E.; Hyde, T.M. Myelin, Myelin-Related Disorders, and Psychosis. Schizophr. Res. 2015, 161, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Rempel-Clower, N.L.; Zola, S.M.; Squire, L.R.; Amaral, D.G. Three Cases of Enduring Memory Impairment after Bilateral Damage Limited to the Hippocampal Formation. J. Neurosci. Off. J. Soc. Neurosci. 1996, 16, 5233–5255. [Google Scholar] [CrossRef]
- Squire, L.R. Memory and the Hippocampus: A Synthesis from Findings with Rats, Monkeys, and Humans. Psychol. Rev. 1992, 99, 195–231. [Google Scholar] [CrossRef] [PubMed]
- Squire, L.R.; Zola-Morgan, S. The Medial Temporal Lobe Memory System. Science 1991, 253, 1380–1386. [Google Scholar] [CrossRef] [Green Version]
- Grasby, P.M.; Frith, C.D.; Friston, K.J.; Simpson, J.; Fletcher, P.C.; Frackowiak, R.S.; Dolan, R.J. A Graded Task Approach to the Functional Mapping of Brain Areas Implicated in Auditory-Verbal Memory. Brain J. Neurol. 1994, 117 Pt 6, 1271–1282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapur, S.; Craik, F.I.; Tulving, E.; Wilson, A.A.; Houle, S.; Brown, G.M. Neuroanatomical Correlates of Encoding in Episodic Memory: Levels of Processing Effect. Proc. Natl. Acad. Sci. USA 1994, 91, 2008–2011. [Google Scholar] [CrossRef] [Green Version]
- Shallice, T.; Fletcher, P.; Frith, C.D.; Grasby, P.; Frackowiak, R.S.; Dolan, R.J. Brain Regions Associated with Acquisition and Retrieval of Verbal Episodic Memory. Nature 1994, 368, 633–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tulving, E.; Kapur, S.; Markowitsch, H.J.; Craik, F.I.; Habib, R.; Houle, S. Neuroanatomical Correlates of Retrieval in Episodic Memory: Auditory Sentence Recognition. Proc. Natl. Acad. Sci. USA 1994, 91, 2012–2015. [Google Scholar] [CrossRef] [Green Version]
- Andreasen, N.C.; O’Leary, D.S.; Arndt, S.; Cizadlo, T.; Hurtig, R.; Rezai, K.; Watkins, G.L.; Ponto, L.L.; Hichwa, R.D. Short-Term and Long-Term Verbal Memory: A Positron Emission Tomography Study. Proc. Natl. Acad. Sci. USA 1995, 92, 5111–5115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fletcher, P.C.; Frith, C.D.; Grasby, P.M.; Shallice, T.; Frackowiak, R.S.; Dolan, R.J. Brain Systems for Encoding and Retrieval of Auditory-Verbal Memory. An in Vivo Study in Humans. Brain J. Neurol. 1995, 118 Pt 2, 401–416. [Google Scholar] [CrossRef] [Green Version]
- Henke, K.; Buck, A.; Weber, B.; Wieser, H.G. Human Hippocampus Establishes Associations in Memory. Hippocampus 1997, 7, 249–256. [Google Scholar] [CrossRef]
- Vieira, R.T.; Caixeta, L.; Machado, S.; Silva, A.C.; Nardi, A.E.; Arias-Carrión, O.; Carta, M.G. Epidemiology of Early-Onset Dementia: A Review of the Literature. Clin. Pract. Epidemiol. Ment. Health CP EMH 2013, 9, 88–95. [Google Scholar] [CrossRef]
- Pick, A. Uber Die Beziehungen Der Senilen Hirnatrophie Zur Aphasie. Prag. Med. Wochenschr. 1892, 17, 165–167. [Google Scholar]
- Alzheimer, A. Über eigenartige Krankheitsfälle des späteren Alters. Z. Gesamte Neurol. Psychiatr. 1911, 4, 356. [Google Scholar] [CrossRef]
- Bang, J.; Spina, S.; Miller, B.L. Non-Alzheimer’s Dementia 1. Lancet 2015, 386, 1672–1682. [Google Scholar] [CrossRef] [Green Version]
- Gorno-Tempini, M.L.; Hillis, A.E.; Weintraub, S.; Kertesz, A.; Mendez, M.; Cappa, S.F.; Ogar, J.M.; Rohrer, J.D.; Black, S.; Boeve, B.F.; et al. Classification of Primary Progressive Aphasia and Its Variants. Neurology 2011, 76, 1006–1014. [Google Scholar] [CrossRef] [Green Version]
- Warren, J.D.; Rohrer, J.D.; Rossor, M.N. Frontotemporal Dementia. BMJ 2013, 347, f4827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hao, L.; Zou, Z.; Tian, H.; Zhang, Y.; Zhou, H.; Liu, L. Stem Cell-Based Therapies for Ischemic Stroke. BioMed Res. Int. 2014, 2014, e468748. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.-C.; Jin, C.-Y.; Kim, H.-S.; Kim, J.-H.; Kim, M.-K.; Kim, H.-I.; Lee, Y.-J.; Son, Y.-J.; Kim, Y.-O.; Woo, Y.-J. Stem Cell Dynamics in an Experimental Model of Stroke. Chonnam Med. J. 2011, 47, 90–98. [Google Scholar] [CrossRef] [Green Version]
- Muraro, P.A.; Pasquini, M.; Atkins, H.L.; Bowen, J.D.; Farge, D.; Fassas, A.; Freedman, M.S.; Georges, G.E.; Gualandi, F.; Hamerschlak, N.; et al. Long-Term Outcomes After Autologous Hematopoietic Stem Cell Transplantation for Multiple Sclerosis. JAMA Neurol. 2017, 74, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Muraro, P.A.; Martin, R.; Mancardi, G.L.; Nicholas, R.; Sormani, M.P.; Saccardi, R. Autologous Haematopoietic Stem Cell Transplantation for Treatment of Multiple Sclerosis. Nat. Rev. Neurol. 2017, 13, 391–405. [Google Scholar] [CrossRef] [PubMed]
- Alexander, T.; Farge, D.; Badoglio, M.; Lindsay, J.O.; Muraro, P.A.; Snowden, J.A. Autoimmune Diseases Working Party (ADWP) of the European Society for Blood and Marrow Transplantation (EBMT) Hematopoietic Stem Cell Therapy for Autoimmune Diseases—Clinical Experience and Mechanisms. J. Autoimmun. 2018, 92, 35–46. [Google Scholar] [CrossRef]
- Snowden, J.A.; Sharrack, B.; Akil, M.; Kiely, D.G.; Lobo, A.; Kazmi, M.; Muraro, P.A.; Lindsay, J.O. Autologous Haematopoietic Stem Cell Transplantation (AHSCT) for Severe Resistant Autoimmune and Inflammatory Diseases—A Guide for the Generalist. Clin. Med. 2018, 18, 329–334. [Google Scholar] [CrossRef] [Green Version]
- Das, J.; Sharrack, B.; Snowden, J.A. Autologous Haematopoietic Stem Cell Transplantation in Multiple Sclerosis: A Review of Current Literature and Future Directions for Transplant Haematologists and Oncologists. Curr. Hematol. Malig. Rep. 2019, 14, 127–135. [Google Scholar] [CrossRef] [Green Version]
- Duarte, R.F.; Labopin, M.; Bader, P.; Basak, G.W.; Bonini, C.; Chabannon, C.; Corbacioglu, S.; Dreger, P.; Dufour, C.; Gennery, A.R.; et al. Indications for Haematopoietic Stem Cell Transplantation for Haematological Diseases, Solid Tumours and Immune Disorders: Current Practice in Europe, 2019. Bone Marrow Transplant. 2019, 54, 1525–1552. [Google Scholar] [CrossRef] [PubMed]
- Sormani, M.P.; Muraro, P.A.; Saccardi, R.; Mancardi, G. NEDA Status in Highly Active MS Can Be More Easily Obtained with Autologous Hematopoietic Stem Cell Transplantation than Other Drugs. Mult. Scler. 2017, 23, 201–204. [Google Scholar] [CrossRef]
- Sormani, M.P.; Muraro, P.A.; Schiavetti, I.; Signori, A.; Laroni, A.; Saccardi, R.; Mancardi, G.L. Autologous Hematopoietic Stem Cell Transplantation in Multiple Sclerosis: A Meta-Analysis. Neurology 2017, 88, 2115–2122. [Google Scholar] [CrossRef] [PubMed]
- Burt, R.K.; Balabanov, R.; Voltarelli, J.; Barreira, A.; Burman, J. Autologous Hematopoietic Stem Cell Transplantation for Multiple Sclerosis--If Confused or Hesitant, Remember: “Treat with Standard Immune Suppressive Drugs and If No Inflammation, No Response”. Mult. Scler. 2012, 18, 772–775. [Google Scholar] [CrossRef] [Green Version]
- Mancardi, G.; Sormani, M.P.; Muraro, P.A.; Boffa, G.; Saccardi, R. Intense Immunosuppression Followed by Autologous Haematopoietic Stem Cell Transplantation as a Therapeutic Strategy in Aggressive Forms of Multiple Sclerosis. Mult. Scler. 2018, 24, 245–255. [Google Scholar] [CrossRef]
- Cohen, J.A.; Baldassari, L.E.; Atkins, H.L.; Bowen, J.D.; Bredeson, C.; Carpenter, P.A.; Corboy, J.R.; Freedman, M.S.; Griffith, L.M.; Lowsky, R.; et al. Autologous Hematopoietic Cell Transplantation for Treatment-Refractory Relapsing Multiple Sclerosis: Position Statement from the American Society for Blood and Marrow Transplantation. Biol. Blood Marrow Transplant. J. Am. Soc. Blood Marrow Transplant. 2019, 25, 845–854. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Weick, J.P.; Liu, H.; Krencik, R.; Zhang, X.; Ma, L.; Zhou, G.; Ayala, M.; Zhang, S.-C. Medial Ganglionic Eminence-like Cells Derived from Human Embryonic Stem Cells Correct Learning and Memory Deficits. Nat. Biotechnol. 2013, 31, 440–447. [Google Scholar] [CrossRef] [Green Version]
- Park, D.; Yang, Y.-H.; Bae, D.K.; Lee, S.H.; Yang, G.; Kyung, J.; Kim, D.; Choi, E.-K.; Lee, S.W.; Kim, G.H.; et al. Improvement of Cognitive Function and Physical Activity of Aging Mice by Human Neural Stem Cells Over-Expressing Choline Acetyltransferase. Neurobiol. Aging 2013, 34, 2639–2646. [Google Scholar] [CrossRef]
- Tang, J.; Xu, H.; Fan, X.; Li, D.; Rancourt, D.; Zhou, G.; Li, Z.; Yang, L. Embryonic Stem Cell-Derived Neural Precursor Cells Improve Memory Dysfunction in Abeta(1-40) Injured Rats. Neurosci. Res. 2008, 62, 86–96. [Google Scholar] [CrossRef] [PubMed]
- Yagi, T.; Ito, D.; Okada, Y.; Akamatsu, W.; Nihei, Y.; Yoshizaki, T.; Yamanaka, S.; Okano, H.; Suzuki, N. Modeling Familial Alzheimer’s Disease with Induced Pluripotent Stem Cells. Hum. Mol. Genet. 2011, 20, 4530–4539. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Mucke, L. Alzheimer Mechanisms and Therapeutic Strategies. Cell 2012, 148, 1204–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reiss, A.B.; Arain, H.A.; Stecker, M.M.; Siegart, N.M.; Kasselman, L.J. Amyloid Toxicity in Alzheimer’s Disease. Rev. Neurosci. 2018, 29, 613–627. [Google Scholar] [CrossRef] [PubMed]
- Saman, S.; Kim, W.; Raya, M.; Visnick, Y.; Miro, S.; Saman, S.; Jackson, B.; McKee, A.C.; Alvarez, V.E.; Lee, N.C.Y.; et al. Exosome-Associated Tau Is Secreted in Tauopathy Models and Is Selectively Phosphorylated in Cerebrospinal Fluid in Early Alzheimer Disease. J. Biol. Chem. 2012, 287, 3842–3849. [Google Scholar] [CrossRef] [Green Version]
- Lewczuk, P.; Kornhuber, J.; Vanmechelen, E.; Peters, O.; Heuser, I.; Maier, W.; Jessen, F.; Bürger, K.; Hampel, H.; Frölich, L.; et al. Amyloid Beta Peptides in Plasma in Early Diagnosis of Alzheimer’s Disease: A Multicenter Study with Multiplexing. Exp. Neurol. 2010, 223, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Fiandaca, M.S.; Kapogiannis, D.; Mapstone, M.; Boxer, A.; Eitan, E.; Schwartz, J.B.; Abner, E.L.; Petersen, R.C.; Federoff, H.J.; Miller, B.L.; et al. Identification of Preclinical Alzheimer’s Disease by a Profile of Pathogenic Proteins in Neurally Derived Blood Exosomes: A Case-Control Study. Alzheimers Dement. J. Alzheimers Assoc. 2015, 11, 600–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, L.; Doecke, J.D.; Sharples, R.A.; Villemagne, V.L.; Fowler, C.J.; Rembach, A.; Martins, R.N.; Rowe, C.C.; Macaulay, S.L.; Masters, C.L.; et al. Prognostic Serum MiRNA Biomarkers Associated with Alzheimer’s Disease Shows Concordance with Neuropsychological and Neuroimaging Assessment. Mol. Psychiatry 2015, 20, 1188–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gui, Y.; Liu, H.; Zhang, L.; Lv, W.; Hu, X. Altered MicroRNA Profiles in Cerebrospinal Fluid Exosome in Parkinson Disease and Alzheimer Disease. Oncotarget 2015, 6, 37043–37053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elia, C.A.; Tamborini, M.; Rasile, M.; Desiato, G.; Marchetti, S.; Swuec, P.; Mazzitelli, S.; Clemente, F.; Anselmo, A.; Matteoli, M.; et al. Intracerebral Injection of Extracellular Vesicles from Mesenchymal Stem Cells Exerts Reduced Aβ Plaque Burden in Early Stages of a Preclinical Model of Alzheimer’s Disease. Cells 2019, 8, 1059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reza-Zaldivar, E.E.; Hernández-Sapiéns, M.A.; Gutiérrez-Mercado, Y.K.; Sandoval-Ávila, S.; Gomez-Pinedo, U.; Márquez-Aguirre, A.L.; Vázquez-Méndez, E.; Padilla-Camberos, E.; Canales-Aguirre, A.A. Mesenchymal Stem Cell-Derived Exosomes Promote Neurogenesis and Cognitive Function Recovery in a Mouse Model of Alzheimer’s Disease. Neural Regen. Res. 2019, 14, 1626–1634. [Google Scholar] [CrossRef]
- Li, B.; Liu, J.; Gu, G.; Han, X.; Zhang, Q.; Zhang, W. Impact of Neural Stem Cell-Derived Extracellular Vesicles on Mitochondrial Dysfunction, Sirtuin 1 Level, and Synaptic Deficits in Alzheimer’s Disease. J. Neurochem. 2020, 154, e15001. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Mal, G.; Verma, V.; Tiwari, R.; Khan, M.I.; Mohapatra, R.K.; Mitra, S.; Alyami, S.A.; Emran, T.B.; Dhama, K.; et al. Stem cell therapies and benefaction of somatic cell nuclear transfer cloning in COVID-19 era. Stem Cell Res. Ther. 2021, 12, 1–16. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. The Safety and The Efficacy Evaluation of NEUROSTEM®-AD in Patients with Alzheimer’s Disease. Available online: https://clinicaltrials.gov/ct2/show/results/NCT01297218?view=results (accessed on 27 September 2020).
- ClinicalTrials.gov. Efficacy and Safety of Filgrastim in Alzheimer’s Disease. Available online: https://clinicaltrials.gov/ct2/show/NCT01617577 (accessed on 4 October 2020).
- Na, D.L. The Long-Term Safety and Efficacy Follow-up Study of Subjects Who Completed the Phase I Clinical Trial of Neurostem®-AD; Clinicaltrials.gov. 2012. Available online: https://clinicaltrials.gov/ct2/show/NCT01696591 (accessed on 15 November 2020).
- ClinicalTrials.gov. Safety and Exploratory Efficacy Study of NEUROSTEM® Versus Placebo in Patients with Alzheimer’s Disease. Available online: https://clinicaltrials.gov/ct2/show/NCT02054208 (accessed on 4 October 2020).
- ClinicalTrials.gov. Allogeneic Human Mesenchymal Stem Cell Infusion Versus Placebo in Patients with Alzheimer’s Disease. Available online: https://clinicaltrials.gov/ct2/show/NCT02600130 (accessed on 27 September 2020).
- ClinicalTrials.gov. Safety and Exploratory Efficacy Study of UCMSCs in Patients with Alzheimer’s Disease. Available online: https://clinicaltrials.gov/ct2/show/NCT02672306 (accessed on 4 October 2020).
- ClinicalTrials.gov. Follow-up Study of Safety and Efficacy in Subjects Who Completed NEUROSTEM® Phase-I/IIa Clinical Trial. Available online: https://clinicaltrials.gov/ct2/show/NCT03172117 (accessed on 4 October 2020).
- ClinicalTrials.gov. Alzheimer’s Autism and Cognitive Impairment Stem Cell Treatment Study. Available online: https://clinicaltrials.gov/ct2/show/NCT03724136 (accessed on 27 September 2020).
- Zinman, L.; Cudkowicz, M. Emerging Targets and Treatments in Amyotrophic Lateral Sclerosis. Lancet Neurol. 2011, 10, 481–490. [Google Scholar] [CrossRef]
- Chiò, A.; Mora, G.; Calvo, A.; Mazzini, L.; Bottacchi, E.; Mutani, R. PARALS Epidemiology of ALS in Italy: A 10-Year Prospective Population-Based Study. Neurology 2009, 72, 725–731. [Google Scholar] [CrossRef]
- Robberecht, W.; Philips, T. The Changing Scene of Amyotrophic Lateral Sclerosis. Nat. Rev. Neurosci. 2013, 14, 248–264. [Google Scholar] [CrossRef] [PubMed]
- Gordon, P.; Corcia, P.; Meininger, V. New Therapy Options for Amyotrophic Lateral Sclerosis. Expert Opin. Pharmacother. 2013, 14, 1907–1917. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, A.K.; Bulte, J.W.M. Seeing Stem Cells at Work in Vivo. Stem Cell Rev. Rep. 2014, 10, 127–144. [Google Scholar] [CrossRef] [Green Version]
- Karumbayaram, S.; Novitch, B.G.; Patterson, M.; Umbach, J.A.; Richter, L.; Lindgren, A.; Conway, A.E.; Clark, A.T.; Goldman, S.A.; Plath, K.; et al. Directed Differentiation of Human-Induced Pluripotent Stem Cells Generates Active Motor Neurons. Stem Cells 2009, 27, 806–811. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Kim, H.Y.; Choi, M.R.; Hwang, S.; Nam, K.-H.; Kim, H.-C.; Han, J.S.; Kim, K.S.; Yoon, H.S.; Kim, S.H. Dose-Dependent Efficacy of ALS-Human Mesenchymal Stem Cells Transplantation into Cisterna Magna in SOD1-G93A ALS Mice. Neurosci. Lett. 2010, 468, 190–194. [Google Scholar] [CrossRef]
- Boucherie, C.; Schäfer, S.; Lavand’homme, P.; Maloteaux, J.-M.; Hermans, E. Chimerization of Astroglial Population in the Lumbar Spinal Cord after Mesenchymal Stem Cell Transplantation Prolongs Survival in a Rat Model of Amyotrophic Lateral Sclerosis. J. Neurosci. Res. 2009, 87, 2034–2046. [Google Scholar] [CrossRef]
- Ohnishi, S.; Ito, H.; Suzuki, Y.; Adachi, Y.; Wate, R.; Zhang, J.; Nakano, S.; Kusaka, H.; Ikehara, S. Intra-Bone Marrow-Bone Marrow Transplantation Slows Disease Progression and Prolongs Survival in G93A Mutant SOD1 Transgenic Mice, an Animal Model Mouse for Amyotrophic Lateral Sclerosis. Brain Res. 2009, 1296, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Corti, S.; Nizzardo, M.; Nardini, M.; Donadoni, C.; Salani, S.; Simone, C.; Falcone, M.; Riboldi, G.; Govoni, A.; Bresolin, N.; et al. Systemic Transplantation of C-Kit+ Cells Exerts a Therapeutic Effect in a Model of Amyotrophic Lateral Sclerosis. Hum. Mol. Genet. 2010, 19, 3782–3796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corti, S.; Locatelli, F.; Papadimitriou, D.; Del Bo, R.; Nizzardo, M.; Nardini, M.; Donadoni, C.; Salani, S.; Fortunato, F.; Strazzer, S.; et al. Neural Stem Cells LewisX+ CXCR4+ Modify Disease Progression in an Amyotrophic Lateral Sclerosis Model. Brain J. Neurol. 2007, 130, 1289–1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, L.; Yan, J.; Chen, D.; Welsh, A.M.; Hazel, T.; Johe, K.; Hatfield, G.; Koliatsos, V.E. Human Neural Stem Cell Grafts Ameliorate Motor Neuron Disease in SOD-1 Transgenic Rats. Transplantation 2006, 82, 865–875. [Google Scholar] [CrossRef] [PubMed]
- Abdelalim, E.M.; Bonnefond, A.; Bennaceur-Griscelli, A.; Froguel, P. Pluripotent Stem Cells as a Potential Tool for Disease Modelling and Cell Therapy in Diabetes. Stem Cell Rev. Rep. 2014, 10, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Cnop, M.; Welsh, N.; Jonas, J.-C.; Jörns, A.; Lenzen, S.; Eizirik, D.L. Mechanisms of Pancreatic Beta-Cell Death in Type 1 and Type 2 Diabetes: Many Differences, Few Similarities. Diabetes 2005, 54 Suppl. 2, S97–S107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Khawaga, S.; Memon, B.; Butler, A.E.; Taheri, S.; Abou-Samra, A.B.; Abdelalim, E.M. Pathways Governing Development of Stem Cell-Derived Pancreatic β Cells: Lessons from Embryogenesis. Biol. Rev. Camb. Philos. Soc. 2018, 93, 364–389. [Google Scholar] [CrossRef] [PubMed]
- van der Torren, C.R.; Zaldumbide, A.; Duinkerken, G.; Brand-Schaaf, S.H.; Peakman, M.; Stangé, G.; Martinson, L.; Kroon, E.; Brandon, E.P.; Pipeleers, D.; et al. Immunogenicity of Human Embryonic Stem Cell-Derived Beta Cells. Diabetologia 2017, 60, 126–133. [Google Scholar] [CrossRef] [Green Version]
- Roscioni, S.S.; Migliorini, A.; Gegg, M.; Lickert, H. Impact of Islet Architecture on β-Cell Heterogeneity, Plasticity and Function. Nat. Rev. Endocrinol. 2016, 12, 695–709. [Google Scholar] [CrossRef]
- Chandrakasan, S.; Malik, P. Gene Therapy for Hemoglobinopathies: The State of the Field and the Future. Hematol. Oncol. Clin. North Am. 2014, 28, 199–216. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; Methot, D.; Poppa, V.; Fujio, Y.; Walsh, K.; Murry, C.E. Cardiomyocyte Grafting for Cardiac Repair: Graft Cell Death and Anti-Death Strategies. J. Mol. Cell. Cardiol. 2001, 33, 907–921. [Google Scholar] [CrossRef]
- Shirai, T.; Rao, V.; Weisel, R.D.; Ikonomidis, J.S.; Li, R.K.; Tumiati, L.C.; Merante, F.; Mickle, D.A. Preconditioning Human Cardiomyocytes and Endothelial Cells. J. Thorac. Cardiovasc. Surg. 1998, 115, 210–219. [Google Scholar] [CrossRef] [Green Version]
- Jiang, S.; Haider, H.K.; Idris, N.M.; Salim, A.; Ashraf, M. Supportive Interaction between Cell Survival Signaling and Angiocompetent Factors Enhances Donor Cell Survival and Promotes Angiomyogenesis for Cardiac Repair. Circ. Res. 2006, 99, 776–784. [Google Scholar] [CrossRef] [Green Version]
- Yau, T.M.; Kim, C.; Ng, D.; Li, G.; Zhang, Y.; Weisel, R.D.; Li, R.-K. Increasing Transplanted Cell Survival with Cell-Based Angiogenic Gene Therapy. Ann. Thorac. Surg. 2005, 80, 1779–1786. [Google Scholar] [CrossRef] [PubMed]
- Shintani, S.; Kusano, K.; Ii, M.; Iwakura, A.; Heyd, L.; Curry, C.; Wecker, A.; Gavin, M.; Ma, H.; Kearney, M.; et al. Synergistic Effect of Combined Intramyocardial CD34+ Cells and VEGF2 Gene Therapy after MI. Nat. Clin. Pract. Cardiovasc. Med. 2006, 3 (Suppl. 1), S123–S128. [Google Scholar] [CrossRef] [PubMed]
- Christman, K.L.; Vardanian, A.J.; Fang, Q.; Sievers, R.E.; Fok, H.H.; Lee, R.J. Injectable Fibrin Scaffold Improves Cell Transplant Survival, Reduces Infarct Expansion, and Induces Neovasculature Formation in Ischemic Myocardium. J. Am. Coll. Cardiol. 2004, 44, 654–660. [Google Scholar] [CrossRef] [Green Version]
- Kutschka, I.; Chen, I.Y.; Kofidis, T.; Arai, T.; von Degenfeld, G.; Sheikh, A.Y.; Hendry, S.L.; Pearl, J.; Hoyt, G.; Sista, R.; et al. Collagen Matrices Enhance Survival of Transplanted Cardiomyoblasts and Contribute to Functional Improvement of Ischemic Rat Hearts. Circulation 2006, 114, I167–I173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feigin, V.L.; Forouzanfar, M.H.; Krishnamurthi, R.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.; Truelsen, T.; et al. Global and Regional Burden of Stroke during 1990-2010: Findings from the Global Burden of Disease Study 2010. Lancet Lond. Engl. 2014, 383, 245–254. [Google Scholar] [CrossRef]
- Langhorne, P.; Bernhardt, J.; Kwakkel, G. Stroke Rehabilitation. Lancet Lond. Engl. 2011, 377, 1693–1702. [Google Scholar] [CrossRef]
- Hankey, G.J. Stroke. Lancet Lond. Engl. 2017, 389, 641–654. [Google Scholar] [CrossRef]
- Kalladka, D.; Sinden, J.; Pollock, K.; Haig, C.; McLean, J.; Smith, W.; McConnachie, A.; Santosh, C.; Bath, P.M.; Dunn, L.; et al. Human Neural Stem Cells in Patients with Chronic Ischaemic Stroke (PISCES): A Phase 1, First-in-Man Study. Lancet 2016, 388, 787–796. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Zhang, G.; Gu, Y.; Guo, X. Meta-Analysis and Systematic Review of Neural Stem Cells Therapy for Experimental Ischemia Stroke in Preclinical Studies. Sci. Rep. 2016, 6, 32291. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Zhang, G.; Khan, A.A.; Guo, X.; Gu, Y. Clinical Efficacy and Meta-Analysis of Stem Cell Therapies for Patients with Brain Ischemia. Stem Cells Int. 2016, 2016, 6129579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakagomi, N.; Nakagomi, T.; Kubo, S.; Nakano-Doi, A.; Saino, O.; Takata, M.; Yoshikawa, H.; Stern, D.M.; Matsuyama, T.; Taguchi, A. Endothelial Cells Support Survival, Proliferation, and Neuronal Differentiation of Transplanted Adult Ischemia-Induced Neural Stem/Progenitor Cells after Cerebral Infarction. Stem Cells 2009, 27, 2185–2195. [Google Scholar] [CrossRef]
- Müller, F.-J.; Snyder, E.Y.; Loring, J.F. Gene Therapy: Can Neural Stem Cells Deliver? Nat. Rev. Neurosci. 2006, 7, 75–84. [Google Scholar] [CrossRef]
- Christian, K.M.; Song, H.; Ming, G. Functions and Dysfunctions of Adult Hippocampal Neurogenesis. Annu. Rev. Neurosci. 2014, 37, 243–262. [Google Scholar] [CrossRef] [Green Version]
- Chollet, F.; Cramer, S.C.; Stinear, C.; Kappelle, L.J.; Baron, J.C.; Weiller, C.; Azouvi, P.; Hommel, M.; Sabatini, U.; Moulin, T.; et al. Pharmacological Therapies in Post Stroke Recovery: Recommendations for Future Clinical Trials. J. Neurol. 2014, 261, 1461–1468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, S.; Bliss, T.M.; Shah, A.K.; Sun, G.H.; Ma, M.; Foo, W.C.; Masel, J.; Yenari, M.A.; Weissman, I.L.; Uchida, N.; et al. Transplanted Human Fetal Neural Stem Cells Survive, Migrate, and Differentiate in Ischemic Rat Cerebral Cortex. Proc. Natl. Acad. Sci. USA 2004, 101, 11839–11844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martino, G.; Pluchino, S. The Therapeutic Potential of Neural Stem Cells. Nat. Rev. Neurosci. 2006, 7, 395–406. [Google Scholar] [CrossRef]
- Li, J.; Tang, Y.; Wang, Y.; Tang, R.; Jiang, W.; Yang, G.-Y.; Gao, W.-Q. Neurovascular Recovery via Cotransplanted Neural and Vascular Progenitors Leads to Improved Functional Restoration after Ischemic Stroke in Rats. Stem Cell Rep. 2014, 3, 101–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ullah, M.; Ng, N.N.; Concepcion, W.; Thakor, A.S. Emerging Role of Stem Cell-Derived Extracellular MicroRNAs in Age-Associated Human Diseases and in Different Therapies of Longevity. Ageing Res. Rev. 2020, 57, 100979. [Google Scholar] [CrossRef] [PubMed]
- Barzegar, M.; Wang, Y.; Yun, J.W.; Chernyshev, O.; Kelley, R.; Alexander, J.S. Abstract TP102: Human Placental Mesenchymal Stem Cells Derived Exosome-Angiotensin Converting Enzyme-2 Dependent Protection in Ischemic Stroke Injury. Stroke 2020, 51, ATP102. [Google Scholar] [CrossRef]
- Wang, C.; Börger, V.; Sardari, M.; Murke, F.; Skuljec, J.; Pul, R.; Hagemann, N.; Dzyubenko, E.; Dittrich, R.; Gregorius, J.; et al. Mesenchymal Stromal Cell–Derived Small Extracellular Vesicles Induce Ischemic Neuroprotection by Modulating Leukocytes and Specifically Neutrophils. Stroke 2020, 51, 1825–1834. [Google Scholar] [CrossRef] [PubMed]
- Moon, G.J.; Sung, J.H.; Kim, D.H.; Kim, E.H.; Cho, Y.H.; Son, J.P.; Cha, J.M.; Bang, O.Y. Application of Mesenchymal Stem Cell-Derived Extracellular Vesicles for Stroke: Biodistribution and MicroRNA Study. Transl. Stroke Res. 2019, 10, 509–521. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Jung, J.-H.; Arvola, O.; Santoso, M.R.; Giffard, R.G.; Yang, P.C.; Stary, C.M. Stem Cell-Derived Exosomes Protect Astrocyte Cultures From in vitro Ischemia and Decrease Injury as Post-Stroke Intravenous Therapy. Front. Cell. Neurosci. 2019, 13, 394. [Google Scholar] [CrossRef]
- Wei, L.; Wei, Z.Z.; Jiang, M.Q.; Mohamad, O.; Yu, S.P. Stem Cell Transplantation Therapy for Multifaceted Therapeutic Benefits after Stroke. Prog. Neurobiol. 2017, 157, 49–78. [Google Scholar] [CrossRef]
- Borlongan, C.V.; Koutouzis, T.K.; Jorden, J.R.; Martinez, R.; Rodriguez, A.I.; Poulos, S.G.; Freeman, T.B.; McKeown, P.; Cahill, D.W.; Nishino, H.; et al. Neural Transplantation as an Experimental Treatment Modality for Cerebral Ischemia. Neurosci. Biobehav. Rev. 1997, 21, 79–90. [Google Scholar] [CrossRef]
- Liska, M.G.; Crowley, M.G.; Nguyen, H.; Borlongan, C.V. Biobridge Concept in Stem Cell Therapy for Ischemic Stroke. J. Neurosurg. Sci. 2017, 61, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.-R.; Duan, W.-M.; Reyes, M.; Keene, C.D.; Verfaillie, C.M.; Low, W.C. Human Bone Marrow Stem Cells Exhibit Neural Phenotypes and Ameliorate Neurological Deficits after Grafting into the Ischemic Brain of Rats. Exp. Neurol. 2002, 174, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Kurozumi, K.; Nakamura, K.; Tamiya, T.; Kawano, Y.; Kobune, M.; Hirai, S.; Uchida, H.; Sasaki, K.; Ito, Y.; Kato, K.; et al. BDNF Gene-Modified Mesenchymal Stem Cells Promote Functional Recovery and Reduce Infarct Size in the Rat Middle Cerebral Artery Occlusion Model. Mol. Ther. J. Am. Soc. Gene Ther. 2004, 9, 189–197. [Google Scholar] [CrossRef]
- Veizovic, T.; Beech, J.S.; Stroemer, R.P.; Watson, W.P.; Hodges, H. Resolution of Stroke Deficits Following Contralateral Grafts of Conditionally Immortal Neuroepithelial Stem Cells. Stroke 2001, 32, 1012–1019. [Google Scholar] [CrossRef] [Green Version]
- Modo, M.; Rezaie, P.; Heuschling, P.; Patel, S.; Male, D.K.; Hodges, H. Transplantation of Neural Stem Cells in a Rat Model of Stroke: Assessment of Short-Term Graft Survival and Acute Host Immunological Response. Brain Res. 2002, 958, 70–82. [Google Scholar] [CrossRef]
- Nagai, A.; Kim, W.K.; Lee, H.J.; Jeong, H.S.; Kim, K.S.; Hong, S.H.; Park, I.H.; Kim, S.U. Multilineage Potential of Stable Human Mesenchymal Stem Cell Line Derived from Fetal Marrow. PLoS ONE 2007, 2, e1272. [Google Scholar] [CrossRef]
- Lee, H.J.; Kim, K.S.; Kim, E.J.; Choi, H.B.; Lee, K.H.; Park, I.H.; Ko, Y.; Jeong, S.W.; Kim, S.U. Brain Transplantation of Immortalized Human Neural Stem Cells Promotes Functional Recovery in Mouse Intracerebral Hemorrhage Stroke Model. Stem Cells 2007, 25, 1204–1212. [Google Scholar] [CrossRef]
- Abeysinghe, H.C.S.; Bokhari, L.; Quigley, A.; Choolani, M.; Chan, J.; Dusting, G.J.; Crook, J.M.; Kobayashi, N.R.; Roulston, C.L. Pre-Differentiation of Human Neural Stem Cells into GABAergic Neurons Prior to Transplant Results in Greater Repopulation of the Damaged Brain and Accelerates Functional Recovery after Transient Ischemic Stroke. Stem Cell Res. Ther. 2015, 6, 186. [Google Scholar] [CrossRef] [Green Version]
- Drury-Stewart, D.; Song, M.; Mohamad, O.; Guo, Y.; Gu, X.; Chen, D.; Wei, L. Highly Efficient Differentiation of Neural Precursors from Human Embryonic Stem Cells and Benefits of Transplantation after Ischemic Stroke in Mice. Stem Cell Res. Ther. 2013, 4, 93. [Google Scholar] [CrossRef] [Green Version]
- Bühnemann, C.; Scholz, A.; Bernreuther, C.; Malik, C.Y.; Braun, H.; Schachner, M.; Reymann, K.G.; Dihné, M. Neuronal Differentiation of Transplanted Embryonic Stem Cell-Derived Precursors in Stroke Lesions of Adult Rats. Brain J. Neurol. 2006, 129, 3238–3248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chau, M.J.; Deveau, T.C.; Song, M.; Gu, X.; Chen, D.; Wei, L. IPSC Transplantation Increases Regeneration and Functional Recovery after Ischemic Stroke in Neonatal Rats. Stem Cells 2014, 32, 3075–3087. [Google Scholar] [CrossRef]
- Nakazaki, M.; Sasaki, M.; Kataoka-Sasaki, Y.; Oka, S.; Namioka, T.; Namioka, A.; Onodera, R.; Suzuki, J.; Sasaki, Y.; Nagahama, H.; et al. Intravenous Infusion of Mesenchymal Stem Cells Inhibits Intracranial Hemorrhage after Recombinant Tissue Plasminogen Activator Therapy for Transient Middle Cerebral Artery Occlusion in Rats. J. Neurosurg. 2017, 127, 917–926. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Sanberg, P.R.; Li, Y.; Wang, L.; Lu, M.; Willing, A.E.; Sanchez-Ramos, J.; Chopp, M. Intravenous Administration of Human Umbilical Cord Blood Reduces Behavioral Deficits after Stroke in Rats. Stroke 2001, 32, 2682–2688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Zhang, Z.G.; Li, Y.; Wang, L.; Xu, Y.X.; Gautam, S.C.; Lu, M.; Zhu, Z.; Chopp, M. Intravenous Administration of Human Bone Marrow Stromal Cells Induces Angiogenesis in the Ischemic Boundary Zone After Stroke in Rats. Circ. Res. 2003, 92, 692–699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeong, S.-W.; Chu, K.; Jung, K.-H.; Kim, S.U.; Kim, M.; Roh, J.-K. Human Neural Stem Cell Transplantation Promotes Functional Recovery in Rats with Experimental Intracerebral Hemorrhage. Stroke 2003, 34, 2258–2263. [Google Scholar] [CrossRef] [Green Version]
- Toyoshima, A.; Yasuhara, T.; Kameda, M.; Morimoto, J.; Takeuchi, H.; Wang, F.; Sasaki, T.; Sasada, S.; Shinko, A.; Wakamori, T.; et al. Intra-Arterial Transplantation of Allogeneic Mesenchymal Stem Cells Mounts Neuroprotective Effects in a Transient Ischemic Stroke Model in Rats: Analyses of Therapeutic Time Window and Its Mechanisms. PLoS ONE 2015, 10, e0127302. [Google Scholar] [CrossRef]
- Fukuda, Y.; Horie, N.; Satoh, K.; Yamaguchi, S.; Morofuji, Y.; Hiu, T.; Izumo, T.; Hayashi, K.; Nishida, N.; Nagata, I. Intra-Arterial Transplantation of Low-Dose Stem Cells Provides Functional Recovery without Adverse Effects after Stroke. Cell. Mol. Neurobiol. 2015, 35, 399–406. [Google Scholar] [CrossRef]
- Wei, Z.Z.; Gu, X.; Ferdinand, A.; Lee, J.H.; Ji, X.; Ji, X.M.; Yu, S.P.; Wei, L. Intranasal Delivery of Bone Marrow Mesenchymal Stem Cells Improved Neurovascular Regeneration and Rescued Neuropsychiatric Deficits after Neonatal Stroke in Rats. Cell Transplant. 2015, 24, 391–402. [Google Scholar] [CrossRef] [Green Version]
- Nelson, P.T.; Kondziolka, D.; Wechsler, L.; Goldstein, S.; Gebel, J.; DeCesare, S.; Elder, E.M.; Zhang, P.J.; Jacobs, A.; McGrogan, M.; et al. Clonal Human (HNT) Neuron Grafts for Stroke Therapy: Neuropathology in a Patient 27 Months after Implantation. Am. J. Pathol. 2002, 160, 1201–1206. [Google Scholar] [CrossRef]
- Hallett, P.J.; Cooper, O.; Sadi, D.; Robertson, H.; Mendez, I.; Isacson, O. Long-Term Health of Dopaminergic Neuron Transplants in Parkinson’s Disease Patients. Cell Rep. 2014, 7, 1755–1761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stem Cell Therapies as an Emerging Paradigm in Stroke Participants. Stem Cell Therapies as an Emerging Paradigm in Stroke (STEPS): Bridging Basic and Clinical Science for Cellular and Neurogenic Factor Therapy in Treating Stroke. Stroke 2009, 40, 510–515. [Google Scholar] [CrossRef] [Green Version]
- Savitz, S.I.; Chopp, M.; Deans, R.; Carmichael, T.; Phinney, D.; Wechsler, L. STEPS Participants Stem Cell Therapy as an Emerging Paradigm for Stroke (STEPS) II. Stroke 2011, 42, 825–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Ye, R.; Yan, T.; Yu, S.P.; Wei, L.; Xu, G.; Fan, X.; Jiang, Y.; Stetler, R.A.; Liu, G.; et al. Cell Based Therapies for Ischemic Stroke: From Basic Science to Bedside. Prog. Neurobiol. 2014, 115, 92–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kondziolka, D.; Wechsler, L.; Goldstein, S.; Meltzer, C.; Thulborn, K.R.; Gebel, J.; Jannetta, P.; DeCesare, S.; Elder, E.M.; McGrogan, M.; et al. Transplantation of Cultured Human Neuronal Cells for Patients with Stroke. Neurology 2000, 55, 565–569. [Google Scholar] [CrossRef] [PubMed]
- Kondziolka, D.; Steinberg, G.K.; Wechsler, L.; Meltzer, C.C.; Elder, E.; Gebel, J.; Decesare, S.; Jovin, T.; Zafonte, R.; Lebowitz, J.; et al. Neurotransplantation for Patients with Subcortical Motor Stroke: A Phase 2 Randomized Trial. J. Neurosurg. 2005, 103, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Bang, O.Y.; Lee, J.S.; Lee, P.H.; Lee, G. Autologous Mesenchymal Stem Cell Transplantation in Stroke Patients. Ann. Neurol. 2005, 57, 874–882. [Google Scholar] [CrossRef] [PubMed]
- Savitz, S.I.; Dinsmore, J.; Wu, J.; Henderson, G.V.; Stieg, P.; Caplan, L.R. Neurotransplantation of Fetal Porcine Cells in Patients with Basal Ganglia Infarcts: A Preliminary Safety and Feasibility Study. Cerebrovasc. Dis. 2005, 20, 101–107. [Google Scholar] [CrossRef]
- Sharma, A.; Sane, H.; Gokulchandran, N.; Khopkar, D.; Paranjape, A.; Sundaram, J.; Gandhi, S.; Badhe, P. Autologous Bone Marrow Mononuclear Cells Intrathecal Transplantation in Chronic Stroke. Stroke Res. Treat. 2014, 2014, 234095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suárez-Monteagudo, C.; Hernández-Ramírez, P.; Alvarez-González, L.; García-Maeso, I.; de la Cuétara-Bernal, K.; Castillo-Díaz, L.; Bringas-Vega, M.L.; Martínez-Aching, G.; Morales-Chacón, L.M.; Báez-Martín, M.M.; et al. Autologous Bone Marrow Stem Cell Neurotransplantation in Stroke Patients. An Open Study. Restor. Neurol. Neurosci. 2009, 27, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Battistella, V.; de Freitas, G.R.; da Fonseca, L.M.B.; Mercante, D.; Gutfilen, B.; Goldenberg, R.C.S.; Dias, J.V.; Kasai-Brunswick, T.H.; Wajnberg, E.; Rosado-de-Castro, P.H.; et al. Safety of Autologous Bone Marrow Mononuclear Cell Transplantation in Patients with Nonacute Ischemic Stroke. Regen. Med. 2011, 6, 45–52. [Google Scholar] [CrossRef]
- Honmou, O.; Houkin, K.; Matsunaga, T.; Niitsu, Y.; Ishiai, S.; Onodera, R.; Waxman, S.G.; Kocsis, J.D. Intravenous Administration of Auto Serum-Expanded Autologous Mesenchymal Stem Cells in Stroke. Brain J. Neurol. 2011, 134, 1790–1807. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.-M.; Zhang, Z.-T.; Guo, C.-J.; Geng, F.-Y.; Qiang, F.; Wang, L.-X. Autologous Bone Marrow Mononuclear Cell Implantation for Intracerebral Hemorrhage-a Prospective Clinical Observation. Clin. Neurol. Neurosurg. 2013, 115, 72–76. [Google Scholar] [CrossRef]
- Friedrich, M.A.G.; Martins, M.P.; Araújo, M.D.; Klamt, C.; Vedolin, L.; Garicochea, B.; Raupp, E.F.; Sartori El Ammar, J.; Machado, D.C.; Costa, J.C.d.; et al. Intra-Arterial Infusion of Autologous Bone Marrow Mononuclear Cells in Patients with Moderate to Severe Middle Cerebral Artery Acute Ischemic Stroke. Cell Transplant. 2012, 21 (Suppl. 1), S13–S21. [Google Scholar] [CrossRef]
- Azad, T.D.; Veeravagu, A.; Steinberg, G.K. Neurorestoration after Stroke. Neurosurg. Focus 2016, 40, E2. [Google Scholar] [CrossRef]
- Kwak, K.-A.; Kwon, H.-B.; Lee, J.W.; Park, Y.-S. Current Perspectives Regarding Stem Cell-Based Therapy for Ischemic Stroke. Curr. Pharm. Des. 2018, 24, 3332–3340. [Google Scholar] [CrossRef]
- Moniche, F.; Escudero, I.; Zapata-Arriaza, E.; Usero-Ruiz, M.; Prieto-León, M.; de la Torre, J.; Gamero, M.-A.; Tamayo, J.A.; Ochoa-Sepúlveda, J.-J.; Maestre, J.; et al. Intra-Arterial Bone Marrow Mononuclear Cells (BM-MNCs) Transplantation in Acute Ischemic Stroke (IBIS Trial): Protocol of a Phase II, Randomized, Dose-Finding, Controlled Multicenter Trial. Int. J. Stroke Off. J. Int. Stroke Soc. 2015, 10, 1149–1152. [Google Scholar] [CrossRef] [PubMed]
- Palisade Bio. Available online: https://www.palisadebio.com/overview/default.aspx (accessed on 2 May 2021).
- Fang, J.; Guo, Y.; Tan, S.; Li, Z.; Xie, H.; Chen, P.; Wang, K.; He, Z.; He, P.; Ke, Y.; et al. Autologous Endothelial Progenitor Cells Transplantation for Acute Ischemic Stroke: A 4-Year Follow-Up Study. Stem Cells Transl. Med. 2019, 8, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Van Pham, P.; Truong, N.C.; Le, P.T.-B.; Tran, T.D.-X.; Vu, N.B.; Bui, K.H.-T.; Phan, N.K. Isolation and Proliferation of Umbilical Cord Tissue Derived Mesenchymal Stem Cells for Clinical Applications. Cell Tissue Bank. 2016, 17, 289–302. [Google Scholar] [CrossRef]
- Dobrzański, L.A. Biomaterials in Regenerative Medicine; BoD—Books on Demand: Norderstedt, Germany, 2018; ISBN 978-953-51-3776-4. [Google Scholar]
- Weiss, J.N.; Levy, S. Neurologic Stem Cell Treatment Study (NEST) Using Bone Marrow Derived Stem Cells for the Treatment of Neurological Disorders and Injuries: Study Protocol for a Nonrandomized Efficacy Trial. Available online: https://www.clinicaltdd.com/article.asp?issn=2542-3975;year=2016;volume=1;issue=4;spage=176;epage=180;aulast=Weiss (accessed on 2 May 2021).
- Toyoda, K. Epidemiology and Registry Studies of Stroke in Japan. J. Stroke 2013, 15, 21–26. [Google Scholar] [CrossRef]
- Mackie, A.R.; Losordo, D.W. CD34-Positive Stem Cells: In the Treatment of Heart and Vascular Disease in Human Beings. Tex. Heart Inst. J. 2011, 38, 474–485. [Google Scholar] [PubMed]
- Heldring, N.; Mäger, I.; Wood, M.J.A.; Le Blanc, K.; Andaloussi, S.E.L. Therapeutic Potential of Multipotent Mesenchymal Stromal Cells and Their Extracellular Vesicles. Hum. Gene Ther. 2015, 26, 506–517. [Google Scholar] [CrossRef]
- ReNeuron. Available online: http://www.reneuron.com/ (accessed on 2 May 2021).
- Stevanato, L.; Hicks, C.; Sinden, J.D. Differentiation of a Human Neural Stem Cell Line on Three Dimensional Cultures, Analysis of MicroRNA and Putative Target Genes. J. Vis. Exp. JoVE 2015, 12, 52410. [Google Scholar] [CrossRef] [Green Version]
- Athersys, Inc. Available online: https://www.athersys.com/home/default.aspx (accessed on 2 May 2021).
- Xie, B.; Chen, M.; Hu, R.; Han, W.; Ding, S. Therapeutic Evidence of Human Mesenchymal Stem Cell Transplantation for Cerebral Palsy: A Meta-Analysis of Randomized Controlled Trials. Stem Cells Int. 2020, 2020, 5701920. [Google Scholar] [CrossRef]
- Pathipati, P.; Lecuyer, M.; Faustino, J.; Strivelli, J.; Phinney, D.G.; Vexler, Z.S. Mesenchymal Stem Cell (MSC)–Derived Extracellular Vesicles Protect from Neonatal Stroke by Interacting with Microglial Cells. Neurotherapeutics 2021, 18, 1939–1952. [Google Scholar] [CrossRef]
- Stonesifer, C.; Corey, S.; Ghanekar, S.; Diamandis, Z.; Acosta, S.A.; Borlongan, C.V. Stem Cell Therapy for Abrogating Stroke-Induced Neuroinflammation and Relevant Secondary Cell Death Mechanisms. Prog. Neurobiol. 2017, 158, 94–131. [Google Scholar] [CrossRef]
- Whitton, P.S. Inflammation as a Causative Factor in the Aetiology of Parkinson’s Disease. Br. J. Pharmacol. 2007, 150, 963–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stolp, H.B. Neuropoietic Cytokines in Normal Brain Development and Neurodevelopmental Disorders. Mol. Cell. Neurosci. 2013, 53, 63–68. [Google Scholar] [CrossRef]
- Raman, D.; Sobolik-Delmaire, T.; Richmond, A. Chemokines in Health and Disease. Exp. Cell Res. 2011, 317, 575–589. [Google Scholar] [CrossRef] [Green Version]
- Barone, F.C.; Feuerstein, G.Z. Inflammatory Mediators and Stroke: New Opportunities for Novel Therapeutics. J. Cereb. Blood Flow Metab. Off. J. Int. Soc. Cereb. Blood Flow Metab. 1999, 19, 819–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinning, C.; Westermann, D.; Clemmensen, P. Oxidative Stress in Ischemia and Reperfusion: Current Concepts, Novel Ideas and Future Perspectives. Biomark. Med. 2017, 11, 11031–11040. [Google Scholar] [CrossRef] [PubMed]
- Vandooren, J.; Van Damme, J.; Opdenakker, G. On the Structure and Functions of Gelatinase B/Matrix Metalloproteinase-9 in Neuroinflammation. Prog. Brain Res. 2014, 214, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Jayaraj, R.L.; Azimullah, S.; Beiram, R.; Jalal, F.Y.; Rosenberg, G.A. Neuroinflammation: Friend and Foe for Ischemic Stroke. J. Neuroinflammation 2019, 16, 142. [Google Scholar] [CrossRef] [Green Version]
- Borlongan, C.V.; Glover, L.E.; Sanberg, P.R.; Hess, D.C. Permeating the Blood Brain Barrier and Abrogating the Inflammation in Stroke: Implications for Stroke Therapy. Curr. Pharm. Des. 2012, 18, 3670–3676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakhan, S.E.; Kirchgessner, A.; Hofer, M. Inflammatory Mechanisms in Ischemic Stroke: Therapeutic Approaches. J. Transl. Med. 2009, 7, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceulemans, A.-G.; Zgavc, T.; Kooijman, R.; Hachimi-Idrissi, S.; Sarre, S.; Michotte, Y. The Dual Role of the Neuroinflammatory Response after Ischemic Stroke: Modulatory Effects of Hypothermia. J. Neuroinflamm. 2010, 7, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iadecola, C.; Anrather, J. The Immunology of Stroke: From Mechanisms to Translation. Nat. Med. 2011, 17, 796–808. [Google Scholar] [CrossRef]
- Park, D.-H.; Borlongan, C.V.; Willing, A.E.; Eve, D.J.; Cruz, L.E.; Sanberg, C.D.; Chung, Y.-G.; Sanberg, P.R. Human Umbilical Cord Blood Cell Grafts for Brain Ischemia. Cell Transplant. 2009, 18, 985–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, D.-H.; Eve, D.J.; Musso, J.; Klasko, S.K.; Cruz, E.; Borlongan, C.V.; Sanberg, P.R. Inflammation and Stem Cell Migration to the Injured Brain in Higher Organisms. Stem Cells Dev. 2009, 18, 693–702. [Google Scholar] [CrossRef]
- Dailey, T.; Metcalf, C.; Mosley, Y.I.; Sullivan, R.; Shinozuka, K.; Tajiri, N.; Pabon, M.; Acosta, S.; Kaneko, Y.; van Loveren, H.; et al. An Update on Translating Stem Cell Therapy for Stroke from Bench to Bedside. J. Clin. Med. 2013, 2, 220–241. [Google Scholar] [CrossRef] [Green Version]
- Borlongan, C.V.; Sanberg, P.R.; Freeman, T.B. Neural Transplantation for Neurodegenerative Disorders. Lancet 1999, 353 (Suppl. 1), SI29–SI30. [Google Scholar] [CrossRef]
- Borlongan, C.V.; Kaneko, Y.; Maki, M.; Yu, S.-J.; Ali, M.; Allickson, J.G.; Sanberg, C.D.; Kuzmin-Nichols, N.; Sanberg, P.R. Menstrual Blood Cells Display Stem Cell-like Phenotypic Markers and Exert Neuroprotection Following Transplantation in Experimental Stroke. Stem Cells Dev. 2010, 19, 439–452. [Google Scholar] [CrossRef]
- Antonucci, I.; Stuppia, L.; Kaneko, Y.; Yu, S.; Tajiri, N.; Bae, E.C.; Chheda, S.H.; Weinbren, N.L.; Borlongan, C.V. Amniotic Fluid as a Rich Source of Mesenchymal Stromal Cells for Transplantation Therapy. Cell Transplant. 2011, 20, 789–795. [Google Scholar] [CrossRef]
- Stevanato, L.; Thanabalasundaram, L.; Vysokov, N.; Sinden, J.D. Investigation of Content, Stoichiometry and Transfer of MiRNA from Human Neural Stem Cell Line Derived Exosomes. PLoS ONE 2016, 11, e0146353. [Google Scholar] [CrossRef]
- Takahashi, K.; Yamanaka, S. Induction of Pluripotent Stem Cells from Mouse Embryonic and Adult Fibroblast Cultures by Defined Factors. Cell 2006, 126, 663–676. [Google Scholar] [CrossRef] [Green Version]
- Drela, K.; Siedlecka, P.; Sarnowska, A.; Domanska-Janik, K. Human Mesenchymal Stem Cells in the Treatment of Neurological Diseases. Acta Neurobiol. Exp. 2013, 73, 38–56. [Google Scholar]
- Kim, S.U.; Lee, H.J.; Kim, Y.B. Neural Stem Cell-Based Treatment for Neurodegenerative Diseases. Neuropathol. Off. J. Jpn. Soc. Neuropathol. 2013, 33, 491–504. [Google Scholar] [CrossRef]
- Tang, S.-C.; Arumugam, T.V.; Xu, X.; Cheng, A.; Mughal, M.R.; Jo, D.G.; Lathia, J.D.; Siler, D.A.; Chigurupati, S.; Ouyang, X.; et al. Pivotal Role for Neuronal Toll-like Receptors in Ischemic Brain Injury and Functional Deficits. Proc. Natl. Acad. Sci. USA 2007, 104, 13798–13803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, Y.; Yasuhara, T.; Hara, K.; Matsukawa, N.; Maki, M.; Yu, G.; Xu, L.; Hess, D.C.; Borlongan, C.V. Transplantation of Bone Marrow-Derived Stem Cells: A Promising Therapy for Stroke. Cell Transplant. 2007, 16, 159–169. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Gu, G.-J.; Shen, X.; Zhang, Q.; Wang, G.-M.; Wang, P.-J. Neural Stem Cell Transplantation Enhances Mitochondrial Biogenesis in a Transgenic Mouse Model of Alzheimer’s Disease-like Pathology. Neurobiol. Aging 2015, 36, 1282–1292. [Google Scholar] [CrossRef] [PubMed]
- Xuan, A.G.; Luo, M.; Ji, W.D.; Long, D.H. Effects of Engrafted Neural Stem Cells in Alzheimer’s Disease Rats. Neurosci. Lett. 2009, 450, 167–171. [Google Scholar] [CrossRef]
- Laroni, A.; de Rosbo, N.K.; Uccelli, A. Mesenchymal Stem Cells for the Treatment of Neurological Diseases: Immunoregulation beyond Neuroprotection. Immunol. Lett. 2015, 168, 183–190. [Google Scholar] [CrossRef]
- Comi, C.; Tondo, G. Insights into the Protective Role of Immunity in Neurodegenerative Disease. Neural Regen. Res. 2017, 12, 64–65. [Google Scholar] [CrossRef] [PubMed]
- Venkataramana, N.K.; Kumar, S.K.V.; Balaraju, S.; Radhakrishnan, R.C.; Bansal, A.; Dixit, A.; Rao, D.K.; Das, M.; Jan, M.; Gupta, P.K.; et al. Open-Labeled Study of Unilateral Autologous Bone-Marrow-Derived Mesenchymal Stem Cell Transplantation in Parkinson’s Disease. Transl. Res. J. Lab. Clin. Med. 2010, 155, 62–70. [Google Scholar] [CrossRef]
- Bowman, M.; Racke, M.; Kissel, J.; Imitola, J. Responsibilities of Health Care Professionals in Counseling and Educating Patients With Incurable Neurological Diseases Regarding “Stem Cell Tourism”: Caveat Emptor. JAMA Neurol. 2015, 72, 1342–1345. [Google Scholar] [CrossRef]
- Tajiri, N.; Duncan, K.; Antoine, A.; Pabon, M.; Acosta, S.A.; de la Pena, I.; Hernadez-Ontiveros, D.G.; Shinozuka, K.; Ishikawa, H.; Kaneko, Y.; et al. Stem Cell-Paved Biobridge Facilitates Neural Repair in Traumatic Brain Injury. Front. Syst. Neurosci. 2014, 8, 116. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Chopp, M. Neurorestorative Treatment of Stroke: Cell and Pharmacological Approaches. NeuroRx J. Am. Soc. Exp. Neurother. 2006, 3, 466–473. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Ramos, J.; Song, S.; Cardozo-Pelaez, F.; Hazzi, C.; Stedeford, T.; Willing, A.; Freeman, T.B.; Saporta, S.; Janssen, W.; Patel, N.; et al. Adult Bone Marrow Stromal Cells Differentiate into Neural Cells in Vitro. Exp. Neurol. 2000, 164, 247–256. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.G. Embryo-Derived Stem Cells: Of Mice and Men. Annu. Rev. Cell Dev. Biol. 2001, 17, 435–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Stojkovic, P.; Przyborski, S.; Cooke, M.; Armstrong, L.; Lako, M.; Stojkovic, M. Derivation of Human Embryonic Stem Cells from Developing and Arrested Embryos. Stem Cells 2006, 24, 2669–2676. [Google Scholar] [CrossRef] [PubMed]
- Thomson, J.A.; Itskovitz-Eldor, J.; Shapiro, S.S.; Waknitz, M.A.; Swiergiel, J.J.; Marshall, V.S.; Jones, J.M. Embryonic Stem Cell Lines Derived from Human Blastocysts. Science 1998, 282, 1145–1147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reubinoff, B.E.; Pera, M.F.; Fong, C.Y.; Trounson, A.; Bongso, A. Embryonic Stem Cell Lines from Human Blastocysts: Somatic Differentiation in Vitro. Nat. Biotechnol. 2000, 18, 399–404. [Google Scholar] [CrossRef]
- Volarevic, V.; Markovic, B.S.; Gazdic, M.; Volarevic, A.; Jovicic, N.; Arsenijevic, N.; Armstrong, L.; Djonov, V.; Lako, M.; Stojkovic, M. Ethical and Safety Issues of Stem Cell-Based Therapy. Int. J. Med. Sci. 2018, 15, 36–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riley, J.; Glass, J.; Feldman, E.L.; Polak, M.; Bordeau, J.; Federici, T.; Johe, K.; Boulis, N.M. Intraspinal Stem Cell Transplantation in Amyotrophic Lateral Sclerosis: A Phase I Trial, Cervical Microinjection, and Final Surgical Safety Outcomes. Neurosurgery 2014, 74, 77–87. [Google Scholar] [CrossRef] [Green Version]
- Sakata, H.; Narasimhan, P.; Niizuma, K.; Maier, C.M.; Wakai, T.; Chan, P.H. Interleukin 6-Preconditioned Neural Stem Cells Reduce Ischaemic Injury in Stroke Mice. Brain J. Neurol. 2012, 135, 3298–3310. [Google Scholar] [CrossRef] [Green Version]
- Hicks, A.U.; Lappalainen, R.S.; Narkilahti, S.; Suuronen, R.; Corbett, D.; Sivenius, J.; Hovatta, O.; Jolkkonen, J. Transplantation of Human Embryonic Stem Cell-Derived Neural Precursor Cells and Enriched Environment after Cortical Stroke in Rats: Cell Survival and Functional Recovery. Eur. J. Neurosci. 2009, 29, 562–574. [Google Scholar] [CrossRef]
- Wu, P.; Tarasenko, Y.I.; Gu, Y.; Huang, L.-Y.M.; Coggeshall, R.E.; Yu, Y. Region-Specific Generation of Cholinergic Neurons from Fetal Human Neural Stem Cells Grafted in Adult Rat. Nat. Neurosci. 2002, 5, 1271–1278. [Google Scholar] [CrossRef] [PubMed]
- Darsalia, V.; Kallur, T.; Kokaia, Z. Survival, Migration and Neuronal Differentiation of Human Fetal Striatal and Cortical Neural Stem Cells Grafted in Stroke-Damaged Rat Striatum. Eur. J. Neurosci. 2007, 26, 605–614. [Google Scholar] [CrossRef]
- Faiz, M.; Sachewsky, N.; Gascón, S.; Bang, K.W.A.; Morshead, C.M.; Nagy, A. Adult Neural Stem Cells from the Subventricular Zone Give Rise to Reactive Astrocytes in the Cortex after Stroke. Cell Stem Cell 2015, 17, 624–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Péron, S.; Berninger, B. Imported Stem Cells Strike against Stroke. Cell Stem Cell 2015, 17, 501–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sirko, S.; Behrendt, G.; Johansson, P.A.; Tripathi, P.; Costa, M.; Bek, S.; Heinrich, C.; Tiedt, S.; Colak, D.; Dichgans, M.; et al. Reactive Glia in the Injured Brain Acquire Stem Cell Properties in Response to Sonic Hedgehog. Cell Stem Cell 2013, 12, 426–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, G.-L.; Zhu, Z.-H.; Wang, Y.-Z. Neural Stem Cell Transplantation Therapy for Brain Ischemic Stroke: Review and Perspectives. World J. Stem Cells 2019, 11, 817–830. [Google Scholar] [CrossRef] [PubMed]
- Gögel, S.; Gubernator, M.; Minger, S.L. Progress and Prospects: Stem Cells and Neurological Diseases. Gene Ther. 2011, 18, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Yoo, J.; Kim, H.-S.; Hwang, D.-Y. Stem Cells as Promising Therapeutic Options for Neurological Disorders. J. Cell. Biochem. 2013, 114, 743–753. [Google Scholar] [CrossRef] [PubMed]
- Le Blanc, K.; Rasmusson, I.; Sundberg, B.; Götherström, C.; Hassan, M.; Uzunel, M.; Ringdén, O. Treatment of Severe Acute Graft-versus-Host Disease with Third Party Haploidentical Mesenchymal Stem Cells. Lancet 2004, 363, 1439–1441. [Google Scholar] [CrossRef]
- Burt, R.K.; Traynor, A.E.; Oyama, Y.; Barr, W.G. Plasticity of Hematopoietic Stem Cells: Enough to Induce Tolerance and Repair Tissue? Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 2002, 46, 855–858. [Google Scholar] [CrossRef]
- Burt, R.K.; Verda, L.; Kim, D.-A.; Oyama, Y.; Luo, K.; Link, C. Embryonic Stem Cells As an Alternate Marrow Donor Source: Engraftment without Graft-Versus-Host Disease. J. Exp. Med. 2004, 199, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Siniscalco, D.; Kannan, S.; Semprún-Hernández, N.; Eshraghi, A.A.; Brigida, A.L.; Antonucci, N. Stem Cell Therapy in Autism: Recent Insights. Stem Cells Cloning Adv. Appl. 2018, 11, 55–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, A.; Gokulchandran, N.; Sane, H.; Nagrajan, A.; Paranjape, A.; Kulkarni, P.; Shetty, A.; Mishra, P.; Kali, M.; Biju, H.; et al. Autologous Bone Marrow Mononuclear Cell Therapy for Autism: An Open Label Proof of Concept Study. Stem Cells Int. 2013, 2013, 623875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herberts, C.A.; Kwa, M.S.; Hermsen, H.P. Risk Factors in the Development of Stem Cell Therapy. J. Transl. Med. 2011, 9, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hough, R.E.; Snowden, J.A.; Wulffraat, N.M. Haemopoietic Stem Cell Transplantation in Autoimmune Diseases: A European Perspective. Br. J. Haematol. 2005, 128, 432–459. [Google Scholar] [CrossRef] [PubMed]
- Cao, Q.; Benton, R.L.; Whittemore, S.R. Stem Cell Repair of Central Nervous System Injury. J. Neurosci. Res. 2002, 68, 501–510. [Google Scholar] [CrossRef]




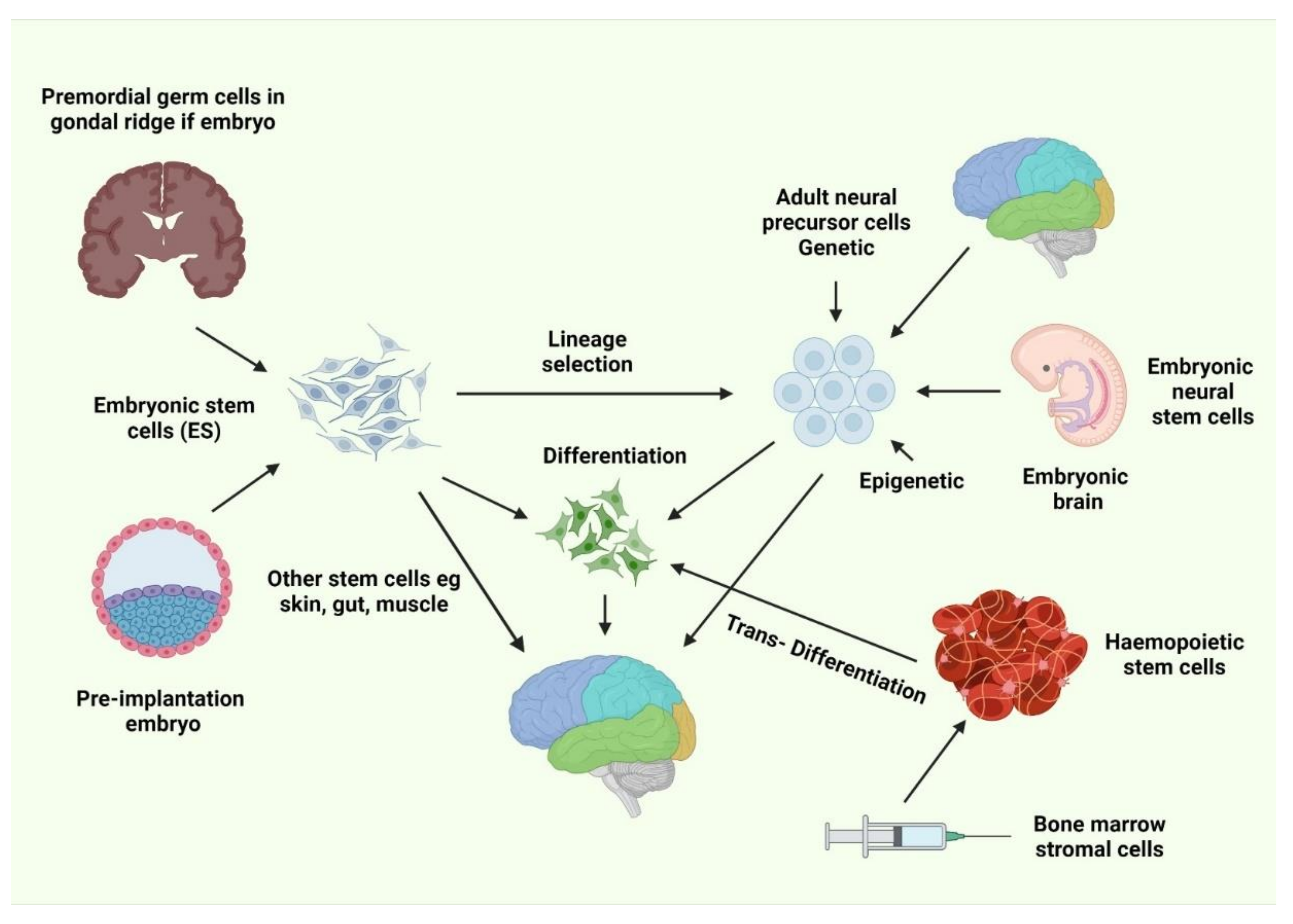{kind=link}
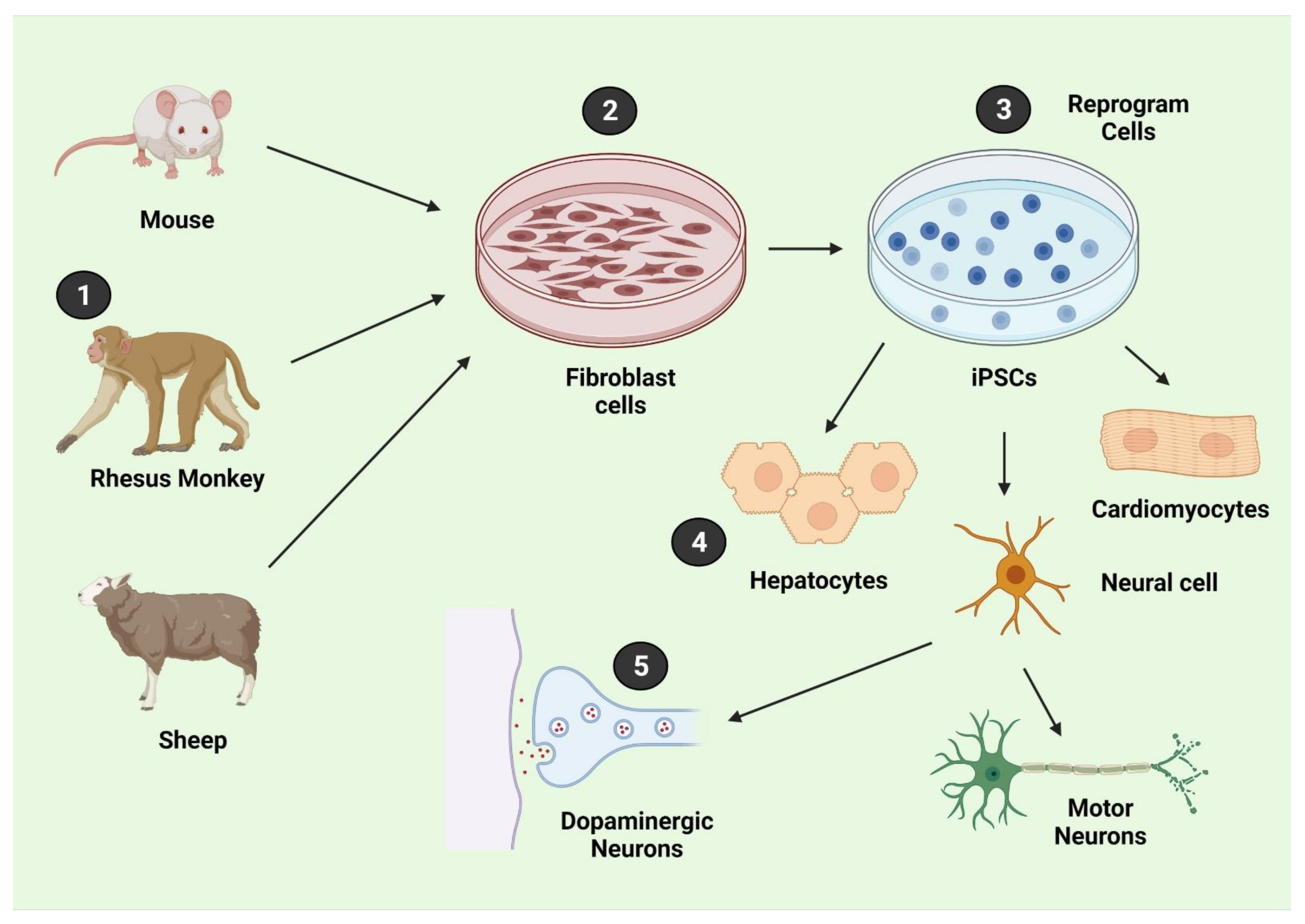{kind=link}
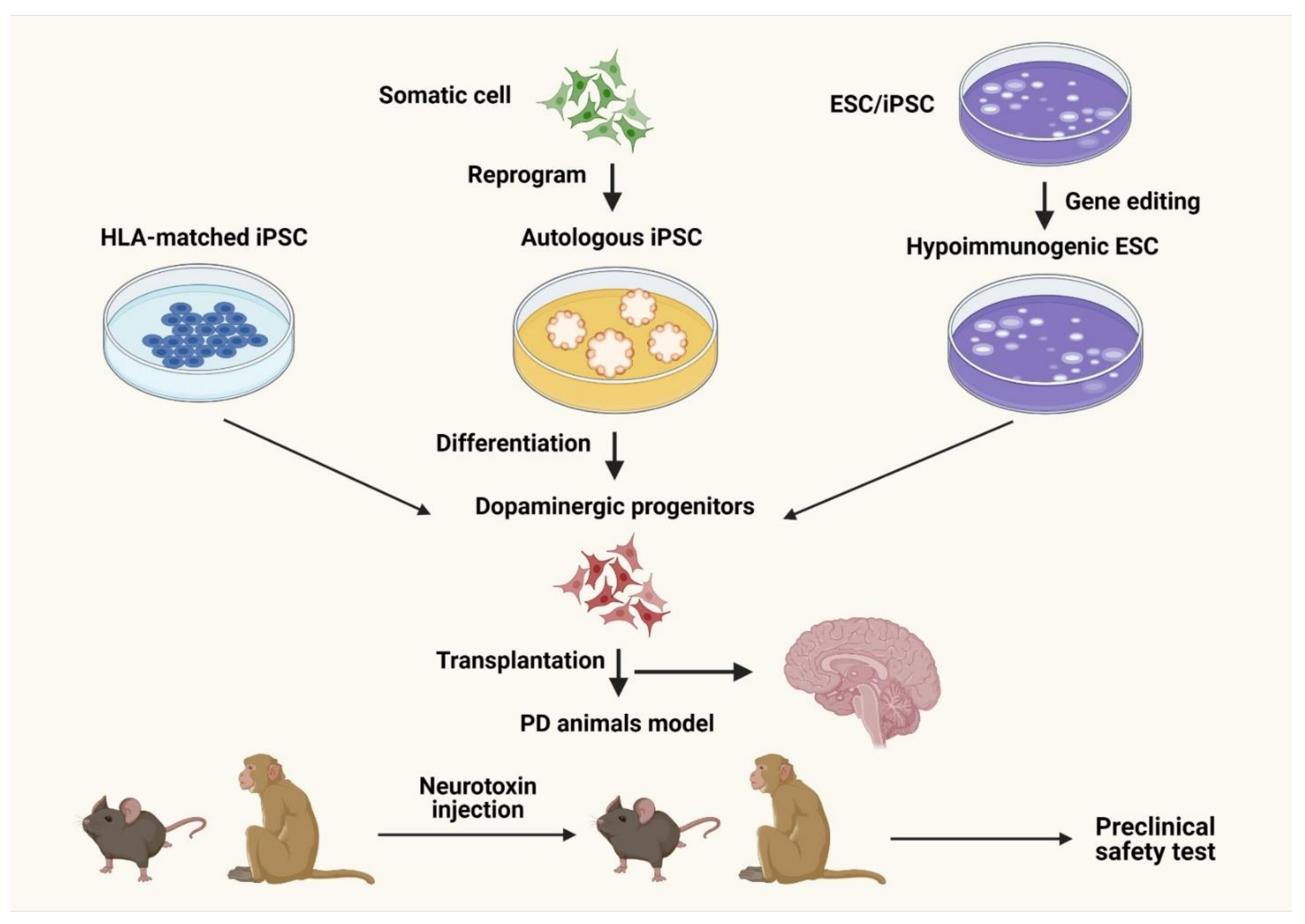{kind=link}
| Intervention Model | Route of Administration | Cell Source | Disease Condition | Number of Patients | Clinical Trial Phase | Primary Outcome | Clinical Trial Identifier | References |
|---|---|---|---|---|---|---|---|---|
| Single group assignment | Intravenous | Human umbilical cord blood-derived mesenchymal stem cell (MSC) | Dementia of the Alzheimer’s disease (AD) type | 9 | Phase I | Number of participants with adverse event | NCT01297218 | [195] |
| Single group assignment | Intravenous | Human umbilical cord blood-derived MSC | AD | 30 | Phase Ⅰ/Ⅱ | Number of participants with adverse event | NCT01547689 | [195] |
| Crossover assignment | Subcutaneous | Filgrastim | AD | 8 | Phase I/II | Change in ADAS-Cog and Selected CANTABS tests | NCT01617577 | [196] |
| Case-Control | Brain surgery | Human umbilical cord blood-derived MSC | AD, Dementia, Brain diseases, Central nervous system diseases, Nervous system diseases, Tauopathies, Neurodegenerative Diseases, Delirium, Dementia, Amnestic, Cognitive Disorders, Mental disorders | 14 | Phase I | Incidence rate of adverse events | NCT01696591 | [197] |
| Parallel assignment | Intraventricular | Human umbilical cord blood-derived MSC | AD | 45 | Phase I/II | Number of subjects with adverse events | NCT02054208 | [198] |
| Parallel assignment | Peripheral intravenous | Longeveron MSC | AD | 33 | Phase I | Incidence of treatment-emergent serious adverse events | NCT02600130 | [199] |
| Parallel assignment | Intravenous | Human umbilical cord blood-derived MSC | AD | 16 | Phase I/II | Change in ADAS-Cog score | NCT02672306 | [200] |
| Parallel assignment | Intravenous | Human umbilical cord blood-derived MSC | AD | 45 | Phase I/II | Change from the baseline in ADAS-Cog | NCT03172117 | [201] |
| Parallel assignment | Peripheral intravenous | Longeveron allogeneic human MSC | AD | 33 | Phase I | Incidence of treatment-emergent serious adverse events | NCT02600130 | [199] |
| Parallel assignment | Peripheral intravenous | Autologous bone marrow-derived stem cells | AD, Vascular dementia, Lewy body disease, Lewy body dementia with behavioral disturbance, Mixed dementia, Parkinson-dementia syndrome, Chronic traumatic encephalopathy, Huntington’s dementia, Wernicke Korsakoff syndrome, Traumatic brain injury, Multi-Infarct dementia, Autism, Autism spectrum disorder Autistic behavior, Autistic disorder, Cadasil, LATE limbic-predominant age-related TDP-43 encephalopathy | 100 | Not Applicable | Running | NCT03724136 | [202] |
| Administration Route | Initiation Time Point | Cell Type/Dose | Species/Model | Outcome | Mechanism | References |
|---|---|---|---|---|---|---|
| Intracerebral | One month | NT2N line/0.8 m | Rat/tMCAO | Motor purpose retrieval | Biobridge, cell standby, persuaded evolution, and trophic provision | [247,248] |
| Seven days | hBMSC | Rat/tMCAO | Sensorimotor salvage | Tempted progress and trophic backing | [249,250] | |
| Fourteen days | MHP36 line/0.2 m/8 μL | Rat/tMCAO | Sensorimotor recapture | Cubicle additional | [251,252] | |
| Seven days | hBMSC | Rat/ICH | Sensorimotor repossession | Made increase and trophic issues | [253] | |
| Seven days | hNSC/ | Mouse/ICH | Motor role regaining | Cell spare | [254] | |
| Seven days | hNSC/0.8 m/2 μL | Rat/Endothelin | Motor role regaining | Cell auxiliary | [255] | |
| Seven days | hES/0.2 m/4 μL | Stroke Mouse/Barrel Stroke | Sensorimotor recuperation | Cell additional | [256] | |
| Seven days | rESC/0.1 m | Rat/MCAO | Endurance and diversity of implants | Cell renewal | [257] | |
| Intracranial | Seven days | miPS/0.4 m/4 μL | Rat/Barrel Stroke | Sensorimotor retaking | Cell replacing | [258] |
| Intravenous | rBMSC/1 m/1 mL | Rat/tMCAO | Dipping alteration, motor recouping | Hinder endothelial disfunction | [259] | |
| Twenty-four hours | hUCBC | Rat/tMCAO | Sensorimotor replevin | Cell substitution | [260] | |
| Twenty-four hours | rMSC/3 m | Rat/tMCAO | Sensorimotor reclamation | Red-reducing cell death | [261] | |
| - | hNSC | Rat | Sensorimotor recovery | Cell replacement | [262] | |
| hNSC/5 m/500 μL | Rat/ICH | |||||
| Intra-arterial | One hour | rBMSC/1 m/1 mL | Rat/tMCAO | Relying reducing infarction | Induced growth and trophic item | [263] |
| Twenty-four hours | hBMSC/1000 | Sensorimotor recapture | Decreasing swelling | [264] | ||
| Intranasal | Six hours | rBMSC/1 m/100 μL | Rat/Barrel Stroke | Dipping infarction, sensorimotor recovery, better-quality olfactive roles, and neuropsychiatric aids | Prompt germination and trophic factors | [265] |
| Trails | Initiation Year and Country | Cell Source and Administration Route | Population | Outcome | Status | References |
|---|---|---|---|---|---|---|
| Safety | - | NT2/D1 and Intracerebral | Basal ganglia stroke | Feasible | Completed | [266,271] |
| 2001, USA | NT2/D1 and Intracerebral | Stroke patients | Feasible with small risk of seizure | Completed | [272] | |
| - | MSC and Intravenous | MCA | - | - | [273] | |
| 2005, USA | ES and Intracerebral | Ischemic stroke patients | 2/5 patients showed improvements | Terminated | [274] | |
| 2008, India | BMMNC and Intrathecal | Stroke patients | - | Completed | [275] | |
| 2009, Cuba | BMSC and Intracerebral | Stroke patients | Good tolerance and safety | Completed | [276] | |
| 2010, Brazil | BMMNC and Intra-arterial | Nonacute ischemic stroke | Feasible and safe | Completed | [277] | |
| 2011, Japan | MSC and Intravenous | Stroke patients | Feasible and safe | Completed | [278] | |
| 2012, Hong Kong | UCBMC and Intracranial | Stroke in the middle cerebral artery territory and stable hemiplegia or hemiparesis | N/A | Completed | [279] | |
| 2012, Brazil | BMMNC and Intra-arterial | MCA acute ischemic stroke | Safe | Completed | [280] | |
| 2010, UK | NSC and Intracranial | Stroke patients | Ongoing | [231] | ||
| 2011, Taiwan | OEC and Intracerebral | Thromboembolic Stroke | - | - | [281] | |
| 2012, China | HSC and Intra-arterial | Internal carotid artery territory infarction | N/A | Recruiting | [282] | |
| 2014, Spain | BMMNC/2m/kg or 5m/kg and Intra-arterial | Moderate-to-severe acute ischemic stroke patients | Appears to be safe; 30% clinical improvement at 90 days | Recruiting | [283] | |
| 2014, China | NSC and Intracerebral | Chronic ischemia stroke | - | Completed | [284] | |
| 2014, China | EPC and Intravenous | Chronic ischemia stroke | - | Recruiting | [285] | |
| 2015, China | UCMSC/20m and Intravenous | ICH | - | Ongoing | [286] | |
| 2016, China | UCMSC and Intravenous | Intracerebral ischemic stroke | - | - | [287] | |
| 2016, Taiwan | ADSC and Intracerebral | Stroke patients | - | - | NCT02813512 [288] | |
| Efficacy | 2008, Japan | BMMNC/25 mL and Intravenous | Stroke patients | - | Completed | [289] |
| 2009, Taiwan | CD34+ Stem Cell and Intracerebral | Chronic stroke adult patient | - | Completed | [290] | |
| 2011, USA | BMSC/2.5m 5.0m or 10m and Intracranial | Chronic stroke patients | No serious adverse events attributable and significant improvements in motor impairment | Completed | [291] | |
| 2014, UK | NSC and Intracerebral | Stroke patient Phase II | Strongly positive results for 12 months; Well-tolerated/no serious adverse events | Ongoing | [292] | |
| 2014, India | BMMNC and Intravenous | Ischemic stroke Phase II | Safe but no beneficial effect | Recruiting | [293] | |
| 2016, US/UK | Multi stem cells and Intravenous | Ischemic stroke Phase II | Excellent; 12-month functional improvement | Completed | [294] | |
| 2016, Europe | ADSC/1m/kg and Intravenous | Hemispheric ischemic stroke | - | Recruiting | [281] | |
| Effectiveness | 2013, China | MSC and Intrathecal | Cerebral palsy | - | Recruiting | [295] |
| Family | Types | Produced By | Role | References | |
|---|---|---|---|---|---|
| Cytokines | Pleiotropic polypeptides (glycoproteins) | Tumor necrosis factor-α (TNF-α), IL-1β, IL-6, IL-20, IL-10, and transforming growth factor (TGF)-β | Microglia | Neuroinflammation (TNF-α, IL-1β, IL-6, IL-20) | [298,299] |
| Astrocytes | Neuroprotection (IL-10 and TGF-β) | ||||
| Neurons and Endothelial cells | |||||
| Invading leukocytes | |||||
| Chemokines | Small cytokines (classified into subgroups according to variations in cysteine residues) | Monocyte chemoattractant protein 1 (MCP-1), macrophage inflammatory protein-1α (MIP-1α), and fractalkine | Microglia | Pro-inflammatory as chemoattractants for invading leukocytes | [300] |
| Astrocytes | |||||
| Injured neurons | |||||
| Cellular adhesion molecules (CAMs) | Cell surface proteins (often transmembrane receptors) | Immunoglobulin superfamily (IgSF), integrins, cadherins, selectins | Endothelial cells | Pro-inflammatory by facilitating extravasation of invading leukocytes | [301] |
| Epithelial cells | |||||
| Leukocytes | |||||
| Reactive oxygen species | Free oxygen radicals | Superoxide anion radical (O2•−), singlet oxygen (1O2), hydroxyl radical (·OH) and perhydroxyl radical (HO2·), nitric oxide (NO) | Neuronal, endothelial* and inducible NO synthases (n−, e−, iNOS, respectively), Oxidative imbalance | Ischemic cell death | [302] |
| Endothelial NO production can have a neuroprotective effect | |||||
| Matrix metalloproteases | Zinc-containing endopeptidases | MMP-2 (gelatinase A) and MMP-9 (gelatinase-B) | Endothelial cells | Pro-inflammatory via degradation of BBB to facilitate invasion of peripheral leukocytes | [303] |
| Neutrophils | |||||
| Macrophages | |||||
| Regulatory T cells | Lymphocytes | CD4+CD25+ | Dendritic or antigen-presenting cell | Immunosuppressive | [304] |
| Mediate microglial/astrocytic activation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahman, M.M.; Islam, M.R.; Islam, M.T.; Harun-Or-Rashid, M.; Islam, M.; Abdullah, S.; Uddin, M.B.; Das, S.; Rahaman, M.S.; Ahmed, M.; et al. Stem Cell Transplantation Therapy and Neurological Disorders: Current Status and Future Perspectives. Biology 2022, 11, 147. https://doi.org/10.3390/biology11010147
Rahman MM, Islam MR, Islam MT, Harun-Or-Rashid M, Islam M, Abdullah S, Uddin MB, Das S, Rahaman MS, Ahmed M, et al. Stem Cell Transplantation Therapy and Neurological Disorders: Current Status and Future Perspectives. Biology. 2022; 11(1):147. https://doi.org/10.3390/biology11010147
Chicago/Turabian StyleRahman, Md. Mominur, Md. Rezaul Islam, Mohammad Touhidul Islam, Md. Harun-Or-Rashid, Mahfuzul Islam, Sabirin Abdullah, Mohammad Borhan Uddin, Sumit Das, Md. Saidur Rahaman, Muniruddin Ahmed, and et al. 2022. "Stem Cell Transplantation Therapy and Neurological Disorders: Current Status and Future Perspectives" Biology 11, no. 1: 147. https://doi.org/10.3390/biology11010147