Fused Deposition Modelling as a Potential Tool for Antimicrobial Dialysis Catheters Manufacturing: New Trends vs. Conventional Approaches





Abstract
:1. Introduction
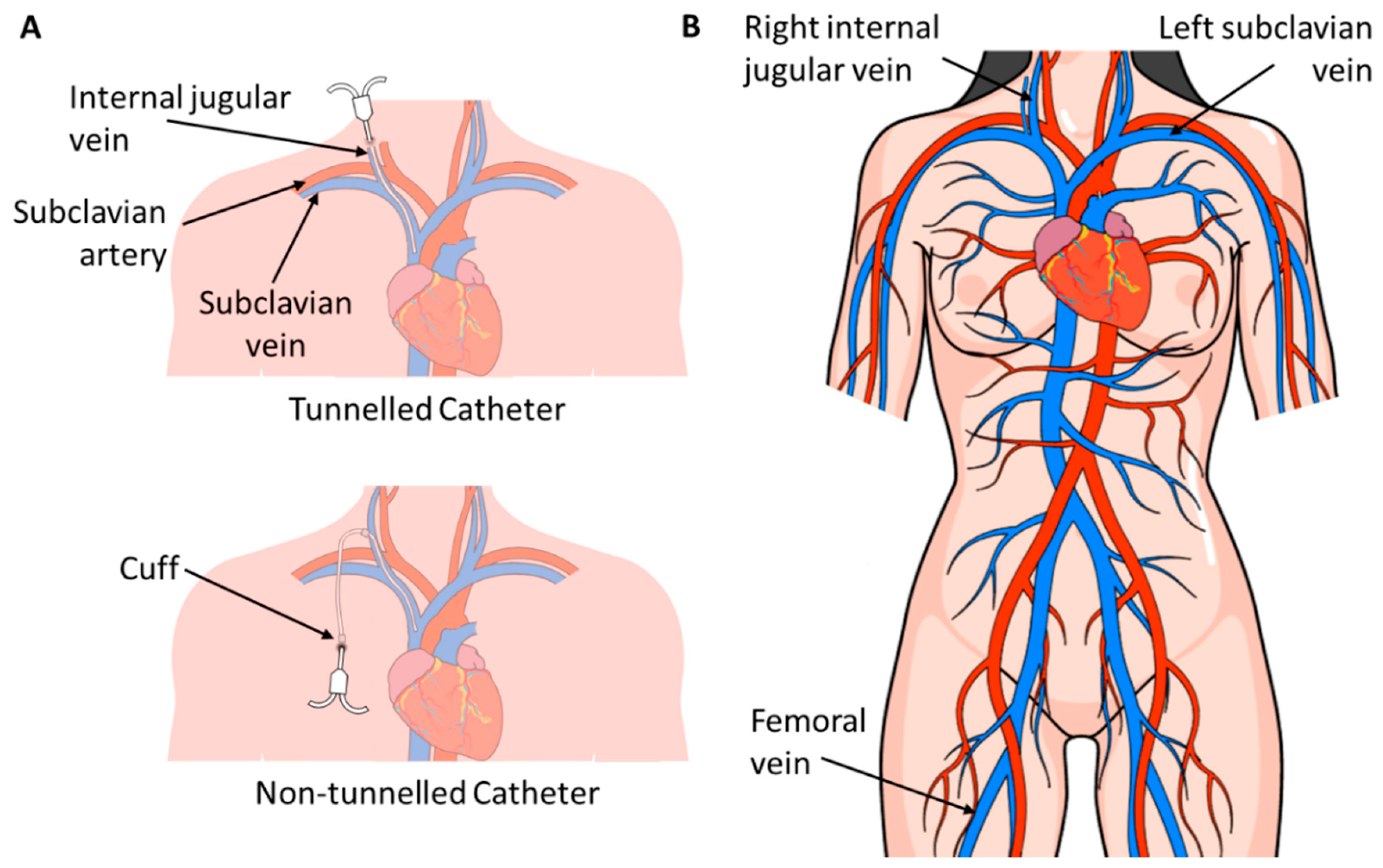
1.1. Infections
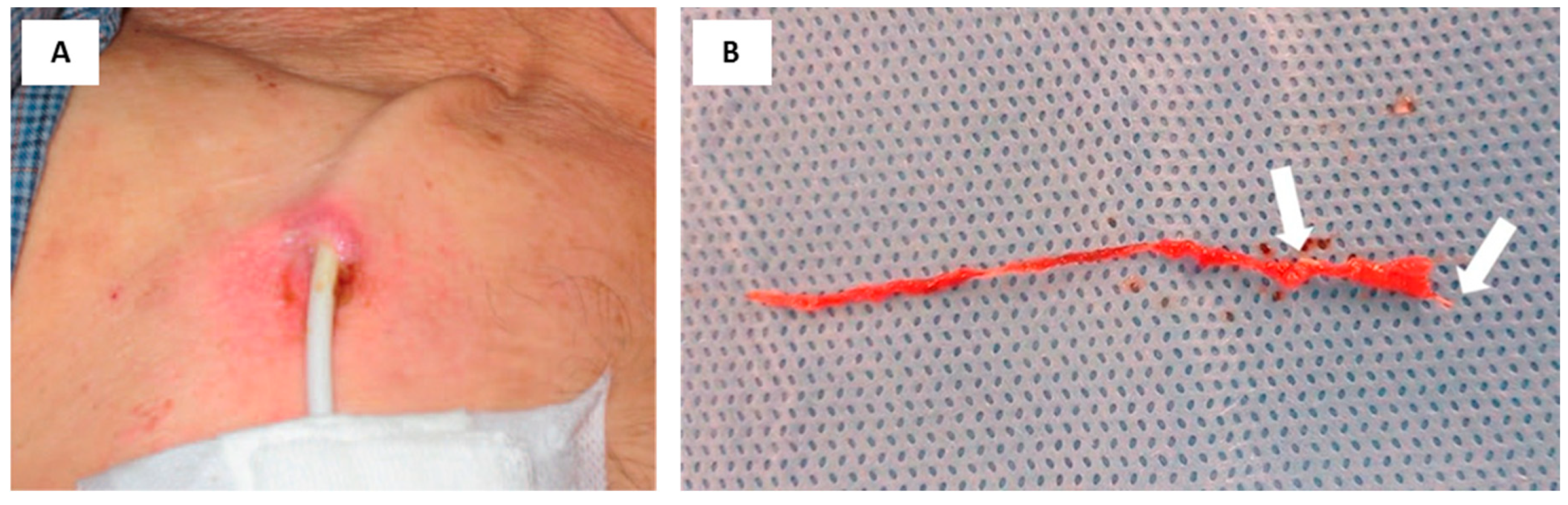
1.2. Fibrin Sheath Formation
2. Current Processes
2.1. Catheter Coatings
2.1.1. Pyrogallol Coating
2.1.2. Heparin Coating
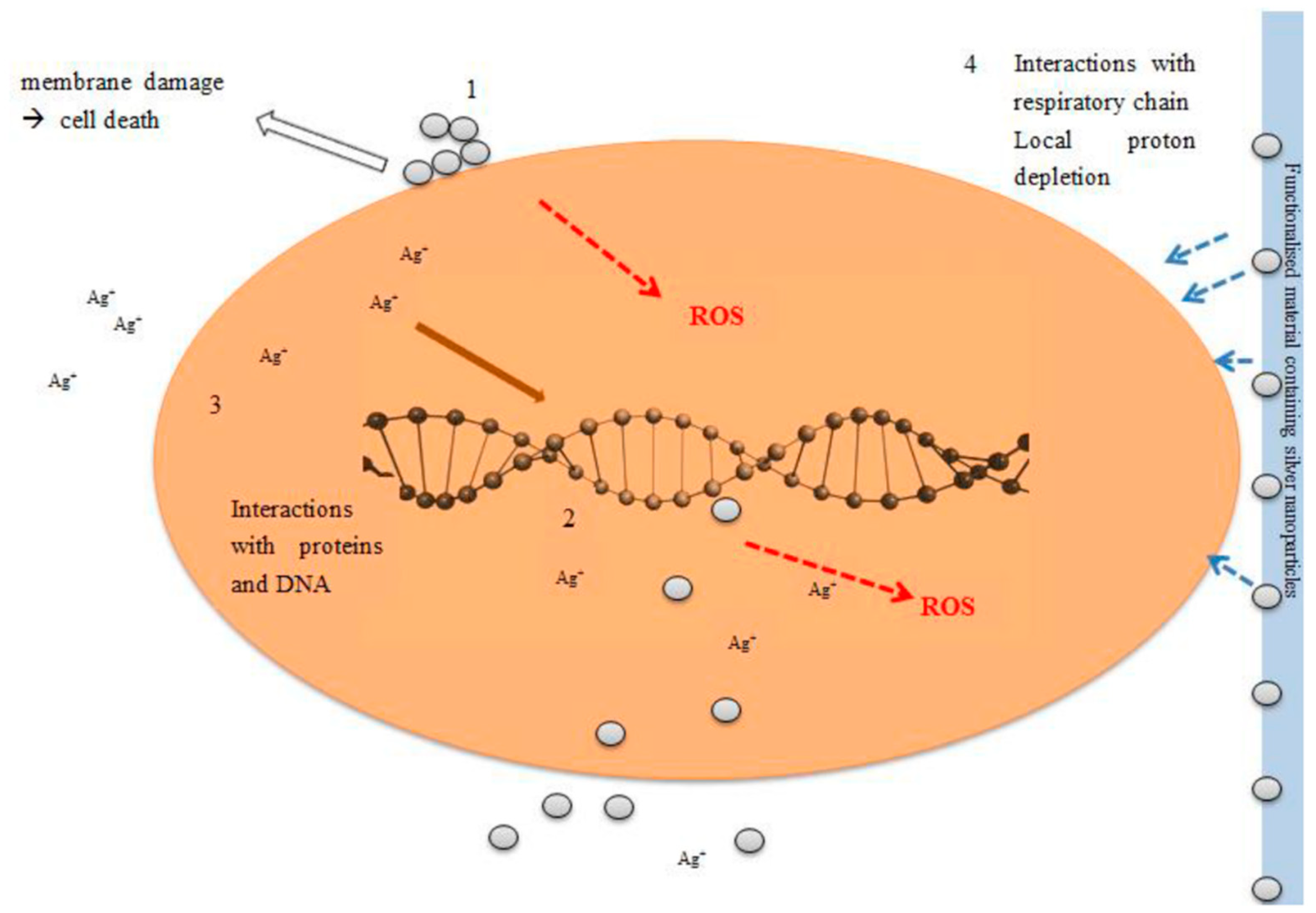
2.1.3. Silver Particles
2.2. Limitations of Coated Catheters
3. Future Directions for Catheter Manufacture: Challenges and Expected Impact
3.1. Additive Manufacturing
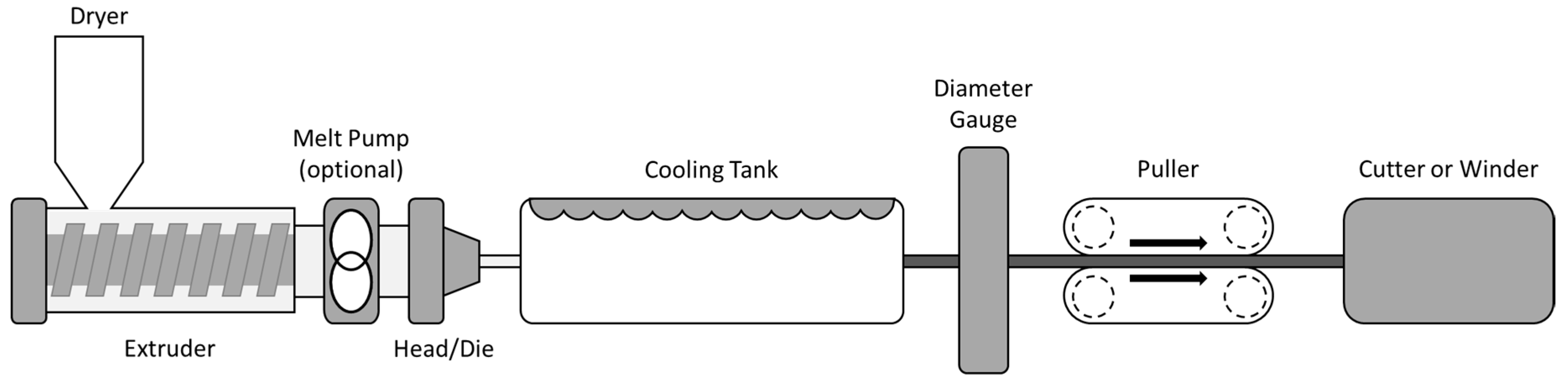
3.2. Hot-Melt Extrusion
4. Suitable Materials for Additive Manufacturing
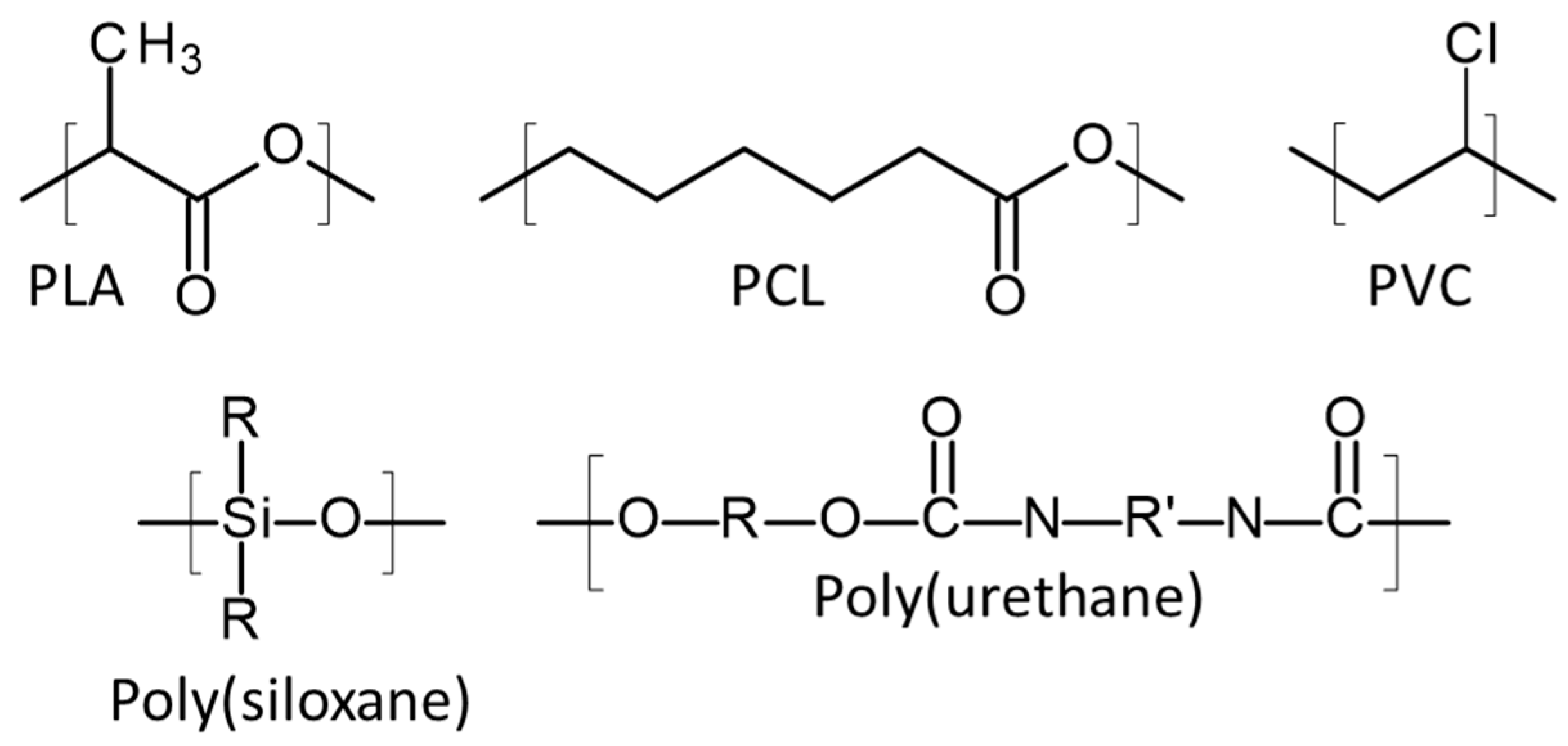
4.1. Poly(Lactic Acid)
4.2. Poly(Caprolactone)
4.3. Poly(Vinyl Chloride)
4.4. Thermoplastic Poly(Urethane)
4.5. Silicone
4.6. Latex
5. Regulatory Considerations on 3D-Printed Medical Devices
Author Contributions
Funding
Conflicts of Interest
References
- Kidney Care UK. Patient Reported Experience of Kidney Care in England and Wales 2017; Kidney Care UK: Alton, UK, 2017. [Google Scholar]
- Couser, W.G.; Remuzzi, G.; Mendis, S.; Tonelli, M. The contribution of chronic kidney disease to the global burden of major noncommunicable diseases. Kidney Int. 2011, 80, 1258–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kidney Care UK. Facts and Stats. Available online: https://www.kidneycareuk.org/news-and-campaigns/facts-and-stats/ (accessed on 7 March 2019).
- Kerr, M. Chronic Kidney Disease in England: The Human and Financial Cost; Insight Health Economics Ltd.: Twickenham, UK, 2012; p. 10. [Google Scholar]
- Lewis, R. Understanding Chronic Kidney Disease: A Guide for the Non-Specialist; M&K Update Ltd.: Keswick, UK, 2011. [Google Scholar]
- Foreman, K.J.; Marquez, N.; Dolgert, A.; Fukutaki, K.; Fullman, N.; McGaughey, M.; Pletcher, M.A.; Smith, A.E.; Tang, K.; Yuan, C.W.; et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: Reference and alternative scenarios for 2016–40 for 195 countries and territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef]
- Dialysis—NHS. Available online: https://www.nhs.uk/conditions/dialysis/ (accessed on 7 March 2019).
- Miller, D.L.; O’Grady, N.P. Guidelines for the Prevention of Intravascular Catheter-related Infections: Recommendations Relevant to Interventional Radiology for Venous Catheter Placement and Maintenance. J. Vasc. Interv. Radiol. 2012, 23, 997–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kramer, R.D.; Rogers, M.A.M.; Conte, M.; Mann, J.; Saint, S.; Chopra, V. Are antimicrobial peripherally inserted central catheters associated with reduction in central line—associated bloodstream infection? A systematic review and meta-analysis. AJIC Am. J. Infect. Control 2017, 45, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Mendu, M.L.; May, M.F.; Kaze, A.D.; Graham, D.A.; Cui, S.; Chen, M.E.; Shin, N.; Aizer, A.A.; Waikar, S.S. Non-Tunneled versus tunneled dialysis catheters for acute kidney injury requiring renal replacement therapy: A prospective cohort study. BMC Nephrol. 2017, 18, 1–7. [Google Scholar] [CrossRef]
- van Oevelen, M.; Abrahams, A.C.; Weijmer, M.C.; Nagtegaal, T.; Dekker, F.W.; Rotmans, J.I.; Meijvis, S.C.A.; Bijlsma, J.A.; van der Bogt, K.E.A.; van de Brug, A.; et al. Precurved non-tunnelled catheters for haemodialysis are comparable in terms of infections and malfunction as compared to tunnelled catheters: A retrospective cohort study. J. Vasc. Access 2019, 20, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, D.W.; Zhang, X.; Charest, J.L. Water infused surface protection as an active mechanism for fibrin sheath prevention in central venous catheters. Artif. Organs 2017, 41, E155–E165. [Google Scholar] [CrossRef]
- Ripa, M.; Morata, L.; Rodríguez-Núñez, O.; Cardozo, C.; Puerta-Alcalde, P.; Hernández-Meneses, M.; Ambrosioni, J.; Linares, L.; Bodro, M.; Valcárcel, A.; et al. Short-term peripheral venous catheter-related bloodstream infections: Evidence for increasing prevalence of gram-negative microorganisms from a 25-year prospective observational study. Antimicrob. Agents Chemother. 2018, 62, e00892-18. [Google Scholar] [CrossRef]
- Miller, L.M.; Clark, E.; Dipchand, C.; Hiremath, S.; Kappel, J.; Kiaii, M.; Lok, C.; Luscombe, R.; Moist, L. Hemodialysis tunneled catheter noninfectious complications. Can. J. Kidney Health Dis. 2016, 3, 2054358116669130. [Google Scholar] [CrossRef]
- Wiese, L.; Mejer, N.; Schønheyder, H.C.; Westh, H. A nationwide study of comorbidity and risk of reinfection after Staphylococcus aureus bacteraemia. J. Infect. 2013, 67, 199–205. [Google Scholar] [CrossRef]
- Brass, P.; Hellmich, M.; Kolodziej, L.; Schick, G.; Af, S. Ultrasound guidance versus anatomical landmarks for internal jugular vein catheterization. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Tong, H.; Liu, H.; Wang, Y.; Wang, R.; Gao, H.; Yu, P.; Lv, Y.; Chen, S.; Wang, G.; et al. Effectiveness of antimicrobial-coated central venous catheters for preventing catheter-related blood-stream infections with the implementation of bundles: A systematic review and network meta-analysis. Ann. Intensive Care 2018, 8, 71. [Google Scholar] [CrossRef] [PubMed]
- Zanini, S.; Polissi, A.; Maccagni, E.A.; Dell’Orto, E.C.; Liberatore, C.; Riccardi, C. Development of antibacterial quaternary ammonium silane coatings on polyurethane catheters. J. Colloid Interface Sci. 2015, 451, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Schneider, A.; Baldwin, I.; Souweine, B. What’s new: Prevention of acute dialysis catheter-related infection. Intensive Care Med. 2018, 44, 356–358. [Google Scholar] [CrossRef] [PubMed]
- Keum, H.; Kim, J.Y.; Yu, B.; Yu, S.J.; Kim, J.; Jeon, H.; Lee, D.Y.; Im, S.G.; Jon, S. Prevention of bacterial colonization on catheters by a one-step coating process involving an antibiofouling polymer in water. ACS Appl. Mater. Interfaces 2017, 9, 19736–19745. [Google Scholar] [CrossRef]
- Lok, C.E.; Mokrzycki, M.H. Prevention and management of catheter-related infection in hemodialysis patients. Kidney Int. 2011, 79, 587–598. [Google Scholar] [CrossRef] [Green Version]
- Mogi, N.; Nakagawa, M.; Matsumae, H.; Hattori, A.; Shimohira, M.; Shibamoto, Y. Fibrin sheath of a peripherally inserted central catheter undepicted with gray-scale (real-time B-mode) ultrasonography: A case report. Radiol. Case Rep. 2018, 13, 537–541. [Google Scholar] [CrossRef] [PubMed]
- Valliant, A.M.; Chaudhry, M.K.; Yevzlin, A.; Astor, B.; Chan, M.R. Tunneled dialysis catheter exchange with fibrin sheath disruption is not associated with increased rate of bacteremia. J. Vasc. Access 2015, 16, 52–56. [Google Scholar] [CrossRef]
- Wang, L.H.; Wei, F.; Jia, L.; Lu, Z.; Wang, B.; Dong, H.Y.; Yu, H.B.; Sun, G.J.; Yang, J.; Li, B.; et al. Fibrin sheath formation and intimal thickening after catheter placement in dog model: Role of hemodynamic wall shear stress. J. Vasc. Access 2015, 16, 275–284. [Google Scholar] [CrossRef]
- Ahmed, R.; Chapman, S.A.; Tantrige, P.; Hussain, A.; Johnston, E.W.; Fang, C.; Ammar, T.; Huang, D.Y.; Wilkins, C.J.; Garzillo, G.; et al. TuLIP (Tunnelled Line Intraluminal Plasty): An alternative technique for salvaging haemodialysis catheter patency in fibrin sheath formation. Cardiovasc. Interv. Radiol. 2019, 42, 770–774. [Google Scholar] [CrossRef]
- May, R.M.; Brennan, A.B.; Fraser, J.C.; Drinker, M.C.; Mann, E.E.; Reddy, S.T.; Magin, C.M.; Siedlecki, C.A. An engineered micropattern to reduce bacterial colonization, platelet adhesion and fibrin sheath formation for improved biocompatibility of central venous catheters. Clin. Transl. Med. 2015, 4, 1–8. [Google Scholar] [CrossRef]
- UV-CURE SILICONES ENABLE NEW MEDICAL DEVICE DESIGN CONCEPTS AND INCREASE CUSTOMER VALUE. Available online: https://www.freudenbergmedical.com/ecomaXL/files/UV-Cure_Silicones.pdf?download=1 (accessed on 14 August 2019).
- Weisenberg, S.H.; Termaath, S.C.; Seaver, C.E.; Killeffer, J.A. Ventricular catheter development: Past, present, and future. J. Neurosurg. 2016, 125, 1504–1512. [Google Scholar] [CrossRef]
- Yang, S.; Lee, Y.J.; Lin, F.; Yang, J.; Chen, K. Chitosan/Poly (vinyl alcohol) blending hydrogel coating improves the surface characteristics of segmented polyurethane urethral catheters. J. Biomed. Mater. Res. Part B 2007, 83, 304–313. [Google Scholar] [CrossRef]
- Weisman, J.A.; Ballard, D.H.; Jammalamadaka, U.; Tappa, K.; Sumerel, J.; D’Agostino, H.B.; Mills, D.K.; Woodard, P.K. 3D printed antibiotic and chemotherapeutic eluting catheters for potential use in interventional radiology: In vitro proof of concept study. Acad. Radiol. 2019, 26, 270–274. [Google Scholar] [CrossRef]
- Balne, P.K.; Harini, S.; Dhand, C.; Dwivedi, N.; Chalasani, M.L.S.; Verma, N.K.; Barathi, V.A.; Beuerman, R.; Agrawal, R.; Lakshminarayanan, R. Surface characteristics and antimicrobial properties of modified catheter surfaces by polypyrogallol and metal ions. Mater. Sci. Eng. C 2018, 90, 673–684. [Google Scholar] [CrossRef]
- Falk, A. The Role of Surface Coatings on Central Venous and Hemodialysis Catheters. Endovasc. Today 2008, 28–30. [Google Scholar]
- Ps, S.; Shah, N. Heparin-bonded catheters for prolonging the patency of central venous catheters in children. Cochrane Database Syst. Rev. 2014, 3–5. [Google Scholar] [CrossRef]
- Nicolas, D.R.M. Heparin Induced Thrombocytopenia (HIT); StatPearls: Treasure Island, FL, USA, 2018. [Google Scholar]
- Kasirajan, K. Outcomes after heparin-Induced thrombocytopenia in patients with propaten vascular grafts. Ann. Vasc. Surg. 2012, 26, 802–808. [Google Scholar] [CrossRef]
- Franci, G.; Falanga, A.; Galdiero, S.; Palomba, L.; Rai, M.; Morelli, G.; Galdiero, M. Silver nanoparticles as potential antibacterial agents. Molecules 2015, 20, 8856–8874. [Google Scholar] [CrossRef]
- Reidy, B.; Haase, A.; Luch, A.; Dawson, A.K.; Lynch, I. Mechanisms of silver nanoparticle release, transformation and toxicity: A critical review of current knowledge and recommendations for future studies and applications. Materials 2013, 6, 2295–2350. [Google Scholar] [CrossRef]
- Wu, K.; Yang, Y.; Zhang, Y.; Deng, J.; Lin, C. A ntimicrobial activity and cytocompatibility of silver nanoparticles coated catheters via a biomimetic surface functionalization strategy. Int. J. Nanomed. 2015, 10, 7241–7252. [Google Scholar] [CrossRef]
- Kuehl, R.; Brunetto, P.S.; Woischnig, A.K.; Varisco, M.; Rajacic, Z.; Vosbeck, J.; Terracciano, L.; Fromm, K.M.; Khanna, N. Preventing implant-associated infections by silver coating. Antimicrob. Agents Chemother. 2016, 60, 2467–2475. [Google Scholar] [CrossRef]
- Freitas, P.D. Incorporation of Silver Nanoparticles by the Irradiation Process in Central Venous Catheter (CVC) of Polyurethane Coated with Titanium Oxide for Antimicrobial Activity. Master’s Thesis, Instituto de Pesquisas Energéticas e Nucleares, Sao Paulo, Brazil, July 2018. [Google Scholar]
- Chen, Y.M.; Dai, A.P.; Shi, Y.; Liu, Z.J.; Gong, M.F.; Yin, X.B. Effectiveness of silver-impregnated central. venous catheters for preventing catheter-related blood stream infections: A meta-analysis. Int. J. Infect. Dis. 2014, 29, e279–e286. [Google Scholar] [CrossRef]
- Iqtedar, M.; Aslam, M.; Akhyar, M.; Shehzaad, A.; Abdullah, R.; Kaleem, A. Extracellular biosynthesis, characterization, optimization of silver nanoparticles (AgNPs) using Bacillus mojavensis BTCB15 and its antimicrobial activity against multidrug resistant pathogens. Prep. Biochem. Biotechnol. 2019, 49, 136–142. [Google Scholar] [CrossRef]
- Roe, D.; Karandikar, B.; Bonn-Savage, N.; Gibbins, B.; Roullet, J. baptiste Antimicrobial surface functionalization of plastic catheters by silver nanoparticles. J. Antimicrob. Chemother. 2008, 61, 869–876. [Google Scholar] [CrossRef]
- Kubo, A.L.; Capjak, I.; Vrček, I.V.; Bondarenko, O.M.; Kurvet, I.; Vija, H.; Ivask, A.; Kasemets, K.; Kahru, A. Antimicrobial potency of differently coated 10 and 50 nm silver nanoparticles against clinically relevant bacteria Escherichia coli and Staphylococcus aureus. Colloids Surf. B Biointerfaces 2018, 170, 401–410. [Google Scholar] [CrossRef]
- Kim, S.H.; Lee, H.S.; Ryu, D.S.; Choi, S.J.; Lee, D.S. Antibacterial activity of silver-nanoparticles against Staphylococcus aureus and Escherichia coli. Korean J. Microbiol. Biotechnol. 2011, 39, 77–85. [Google Scholar]
- Chopra, I. The increasing use of silver-based products as antimicrobial agents: A useful development or a cause for concern? J. Antimicrob. Chemother. 2007, 59, 587–590. [Google Scholar] [CrossRef]
- Percival, S.L.; Bowler, P.G.; Russell, D. Bacterial resistance to silver in wound care. J. Hosp. Infect. 2005, 60, 1–7. [Google Scholar] [CrossRef]
- Silver, S. Bacterial silver resistance: Molecular biology and uses and misuses of silver compounds. FEMS Microbiol. Rev. 2003, 27, 341–353. [Google Scholar] [CrossRef]
- Korani, M.; Ghazizadeh, E.; Korani, S.; Hami, Z.; Mohammadi-Bardbori, A. Effects of silver nanoparticles on human health. Eur. J. Nanomed. 2015, 7, 51–62. [Google Scholar] [CrossRef]
- Stenger, M.; Klein, K.; Grønnemose, R.B.; Klitgaard, J.K.; Kolmos, H.J.; Lindholt, J.S.; Alm, M.; Thomsen, P.; Andersen, T.E. Co-release of dicloxacillin and thioridazine from catheter material containing an interpenetrating polymer network for inhibiting device-associated Staphylococcus aureus infection. J. Control. Release 2016, 241, 125–134. [Google Scholar] [CrossRef]
- Zanwar, S.; Jain, P.; Gokarn, A.; Kumar, S.; Punatar, S.; Khurana, S.; Bonda, A.; Pruthy, R.; Bhat, V.; Qureshi, S.; et al. Antibiotic lock therapy for salvage of tunneled central venous catheters with catheter colonization and catheter-related bloodstream infection. Transpl. Infect. Dis. 2019, 21, e13017. [Google Scholar] [CrossRef]
- Melocchi, A.; Parietti, F.; Maroni, A.; Foppoli, A.; Gazzaniga, A.; Zema, L. Hot-melt extruded filaments based on pharmaceutical grade polymers for 3D printing by fused deposition modeling. Int. J. Pharm. 2016, 509, 255–263. [Google Scholar] [CrossRef]
- Weisman, J.A.; Nicholson, J.C.; Tappa, K.; Jammalamadaka, U.; Wilson, C.G.; Mills, D.K. Antibiotic and chemotherapeutic enhanced three-dimensional printer filaments and constructs for biomedical applications. Int. J. Nanomed. 2015, 10, 357–370. [Google Scholar] [CrossRef]
- Sousa, C.; Teixeira, P.; Oliveira, R. Influence of surface properties on the adhesion of staphylococcus epidermidis to acrylic and silicone. Int. J. Biomater. 2009, 2009, 1–9. [Google Scholar] [CrossRef]
- Lalehpour, A.; Janeteas, C.; Barari, A. Surface roughness of FDM parts after post-processing with acetone vapor bath smoothing process. Int. J. Adv. Manuf. Technol. 2018, 95, 1505–1520. [Google Scholar] [CrossRef]
- Pérez, M.; Medina-Sánchez, G.; García-Collado, A.; Gupta, M.; Carou, D. Surface quality enhancement of fused deposition modeling (FDM) printed samples based on the selection of critical printing parameters. Materials 2018, 11, 1382. [Google Scholar] [CrossRef]
- Keating, A.V.; Soto, J.; Tuleu, C.; Forbes, C.; Zhao, M.; Craig, D.Q.M. Solid state characterisation and taste masking efficiency evaluation of polymer based extrudates of isoniazid for paediatric administration. Int. J. Pharm. 2018, 536, 536–546. [Google Scholar] [CrossRef]
- Verstraete, G.; Van Renterghem, J.; Van Bockstal, P.-J.; Kasmi, S.; De Geest, B.; De Beer, T.; Remon, J.P.; Vervaet, C. Hydrophilic thermoplastic polyurethanes for the manufacturing of highly dosed oral sustained release matrices via hot melt extrusion and injection molding. Int. J. Pharm. 2016, 506, 214–221. [Google Scholar] [CrossRef] [Green Version]
- Muwaffak, Z.; Goyanes, A.; Clark, V.; Basit, A.W.; Hilton, S.T.; Gaisford, S. Patient-specific 3D scanned and 3D printed antimicrobial polycaprolactone wound dressings. Int. J. Pharm. 2017, 527, 161–170. [Google Scholar] [CrossRef]
- Tan, D.K.; Maniruzzaman, M.; Nokhodchi, A. Advanced pharmaceutical applications of hot-melt extrusion coupled with fused deposition modelling (FDM) 3D printing for personalised drug delivery. Pharmaceutics 2018, 10, 203. [Google Scholar] [CrossRef]
- Alhijjaj, M.; Belton, P.; Qi, S. An investigation into the use of polymer blends to improve the printability of and regulate drug release from pharmaceutical solid dispersions prepared via fused deposition modeling (FDM) 3D printing. Eur. J. Pharm. Biopharm. 2016, 108, 111–125. [Google Scholar] [CrossRef] [Green Version]
- Tappa, K.; Jammalamadaka, U. Novel biomaterials used in medical 3D printing techniques. J. Funct. Biomater. 2018, 9, 17. [Google Scholar] [CrossRef]
- Stewart, A.S.; Domínguez-Robles, J.; Donnelly, F.R.; Larrañeta, E. Implantable polymeric drug delivery devices: Classification, manufacture, materials, and clinical applications. Polymers 2018, 10, 1379. [Google Scholar] [CrossRef]
- Domínguez-Robles, J.; Martin, K.N.; Fong, L.M.; Stewart, A.S.; Irwin, J.N.; Rial-Hermida, I.M.; Donnelly, F.R.; Larrañeta, E. Antioxidant PLA composites containing lignin for 3d printing applications: A potential material for healthcare applications. Pharmaceutics 2019, 11, 165. [Google Scholar] [CrossRef]
- Pawar, R.P.; Tekale, S.U.; Shisodia, S.U.; Totre, J.T.; Domb, A.J. Biomedical applications of Poly (Lactic Acid). Rec. Pat. Regen. Med. 2014, 4, 40–51. [Google Scholar] [CrossRef]
- Jacobi, C.; Friedrich, T.; Lüdtke-Buzug, K. Synthesis and characterisation of superparamagnetic polylactic acid based polymers. Int. J. Magn. Part. Imaging 2017, 3, 1710001. [Google Scholar]
- Masutani, K.; Kimura, Y. PLA Synthesis and Polymerization. In Poly(Lactic Acid) Science and Technology: Processing, Properties, Additives and Applications; Jiménez, A., Peltzer, M., Ruseckaite, R., Eds.; Royal Society of Chemistry: London, UK, 2014; ISBN 9781782624806. [Google Scholar]
- Farah, S.; Anderson, D.G.; Langer, R. Physical and mechanical properties of PLA, and their functions in widespread applications—A comprehensive review. Adv. Drug Deliv. Rev. 2016, 107, 367–392. [Google Scholar] [CrossRef]
- Romanov, V.; Samuel, R.; Chaharlang, M.; Jafek, A.R.; Frost, A.; Gale, B.K. FDM 3D printing of high-pressure, heat-resistant, transparent microfluidic devices. Anal. Chem. 2018, 90, 10450–10456. [Google Scholar] [CrossRef]
- Guerra, A.J.; Cano, P.; Rabionet, M.; Puig, T.; Ciurana, J. 3D-printed PCL/PLA composite stents: Towards a new solution to cardiovascular problems. Materials 2018, 11, 1679. [Google Scholar] [CrossRef]
- Li, D.; Guo, G.; Fan, R.; Liang, J.; Deng, X.; Luo, F.; Qian, Z. PLA/F68/Dexamethasone implants prepared by hot-melt extrusion for controlled release of anti-inflammatory drug to implantable medical devices: I. Preparation, characterization and hydrolytic degradation study. Int. J. Pharm. 2013, 441, 365–372. [Google Scholar] [CrossRef]
- Li, D.; Guo, G.; Deng, X.; Fan, R.; Guo, Q.; Fan, M.; Liang, J.; Luo, F.; Qian, Z. PLA/PEG-PPG-PEG/Dexamethasone implant prepared by hot-melt extrusion for controlled release of immunosuppressive drug to implantable medical devices, part 2: In vivo evaluation. Drug Deliv. 2013, 20, 134–142. [Google Scholar] [CrossRef]
- Visscher, L.E.; Dang, H.P.; Knackstedt, M.A.; Hutmacher, D.W.; Tran, P.A. 3D printed Polycaprolactone scaffolds with dual macro-microporosity for applications in local delivery of antibiotics. Mater. Sci. Eng. C 2018, 87, 78–89. [Google Scholar] [CrossRef] [Green Version]
- Fu, J.; Yu, X.; Jin, Y. 3D printing of vaginal rings with personalized shapes for controlled release of progesterone. Int. J. Pharm. 2018, 539, 75–82. [Google Scholar] [CrossRef]
- Johansson, K.; Greis, G.; Johansson, B.; Grundtmann, A.; Pahlby, Y.; Törn, S.; Axelberg, H.; Carlsson, P. Evaluation of a new PVC-free catheter material for intermittent catheterization: A prospective, randomized, crossover study. Scand. J. Urol. 2013, 47, 33–37. [Google Scholar] [CrossRef]
- Sharma, R.; Singh, R.; Penna, R.; Fraternali, F. Investigations for mechanical properties of Hap, PVC and PP based 3D porous structures obtained through biocompatible FDM filaments. Compos. Part B Eng. 2018, 132, 237–243. [Google Scholar] [CrossRef]
- Rusu, M.; Ursu, M.; Rusu, D. Poly(vinyl chloride) and poly(e-caprolactone) blends for medical use. J. Thermoplast. Compos. Mater. 2006, 19, 173–190. [Google Scholar] [CrossRef]
- Simons, F.J.; Wagner, K.G. Modeling, design and manufacture of innovative floating gastroretentive drug delivery systems based on hot-melt extruded tubes. Eur. J. Pharm. Biopharm. 2019, 137, 196–208. [Google Scholar] [CrossRef]
- Haryńska, A.; Gubanska, I.; Kucinska-Lipka, J.; Janik, H. Fabrication and characterization of flexible medical-grade tpu filament for fused deposition modeling 3dp technology. Polymers 2018, 10, 1304. [Google Scholar] [CrossRef]
- Gupta, S.; Ramamurthy, P.C.; Madras, G. Synthesis and characterization of silicone polymer/functionalized mesostructured silica composites. Polym. Chem. 2011, 2, 2643–2650. [Google Scholar] [CrossRef]
- Thermal Analysis of Silicone Rubber. Available online: https://www.hitachi-hightech.com/file/global/pdf/products/science/appli/ana/thermal/application_TA_018e.pdf (accessed on 14 August 2018).
- Plott, J.; Shih, A. The extrusion-based additive manufacturing of moisture-cured silicone elastomer with minimal void for pneumatic actuators. Addit. Manuf. 2017, 17, 1–14. [Google Scholar] [CrossRef]
- Hamidi, A.; Jain, S.; Tadesse, Y. 3D printing PLA and silicone elastomer structures with sugar solution support material. In Proceedings of the SPIE, Portland, OR, USA, 17 April 2017; Volume 10163. [Google Scholar]
- Feneley, R.C.L.; Hopley, I.B.; Wells, P.N.T. Urinary catheters: History, current status, adverse events and research agenda. J. Med. Eng. Technol. 2015, 39, 459–470. [Google Scholar] [CrossRef]
- Khatri, P.; Shah, M.K.; Vora, N. Formulation strategies for solid oral dosage form using 3D printing technology: A mini-review. J. Drug Deliv. Sci. Technol. 2018, 46, 148–155. [Google Scholar] [CrossRef]
- Adamo, J.E.; Grayson, W.L.; Hatcher, H.; Swanton, J.; Thomas, A.; Hollister, S.; Steele, S.J. Regulatory interfaces surrounding the growing field of additive manufacturing of medical devices and biologic products. J. Clin. Transl. Sci. 2018, 2, 301–304. [Google Scholar] [CrossRef] [Green Version]
- U.S. Food and Drug Administration. Technical Considerations for Additive Manufactured Medical Devices. Guidance for Industry and Food and Drug Administration Staff; U.S. Food and Drug Administration: Silver Spring, MD, USA, 2017.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Advantages | Disadvantages |
|---|---|
| Rapid Manufacture | Drug needs to have similar or higher melting point to polymer |
| Less expensive | Small range of thermoplastic polymers |
| On-demand Fabrication | Lower resolution than stereolithography |
| Patient Matched Device | Difficult to produce small diameter filament |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mathew, E.; Domínguez-Robles, J.; Larrañeta, E.; Lamprou, D.A. Fused Deposition Modelling as a Potential Tool for Antimicrobial Dialysis Catheters Manufacturing: New Trends vs. Conventional Approaches. Coatings 2019, 9, 515. https://doi.org/10.3390/coatings9080515
Mathew E, Domínguez-Robles J, Larrañeta E, Lamprou DA. Fused Deposition Modelling as a Potential Tool for Antimicrobial Dialysis Catheters Manufacturing: New Trends vs. Conventional Approaches. Coatings. 2019; 9(8):515. https://doi.org/10.3390/coatings9080515
Chicago/Turabian StyleMathew, Essyrose, Juan Domínguez-Robles, Eneko Larrañeta, and Dimitrios A. Lamprou. 2019. "Fused Deposition Modelling as a Potential Tool for Antimicrobial Dialysis Catheters Manufacturing: New Trends vs. Conventional Approaches" Coatings 9, no. 8: 515. https://doi.org/10.3390/coatings9080515