

Incidence of Drug-Resistant Hospital-Associated Gram-Negative Bacterial Infections, the Accompanying Risk Factors, and Clinical Outcomes with Treatment
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Location and Ethical Considerations
2.2. Study Design and Data Collection
2.3. Identification and Antimicrobial Susceptibility Assay of Bacteria Isolates
2.4. Definition of Infections
2.5. Antimicrobial Treatment Regime Assay and Determination of Clinical Outcomes
2.6. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Bacterial Infections and Antimicrobial Assay
3.3. Duration of Hospital Stay, Patients’ Comorbid Conditions, and Clinical Outcomes after Treatment
3.4. Monotherapy and Combined Therapy Treatment Types for Clinical Bacterial Infections
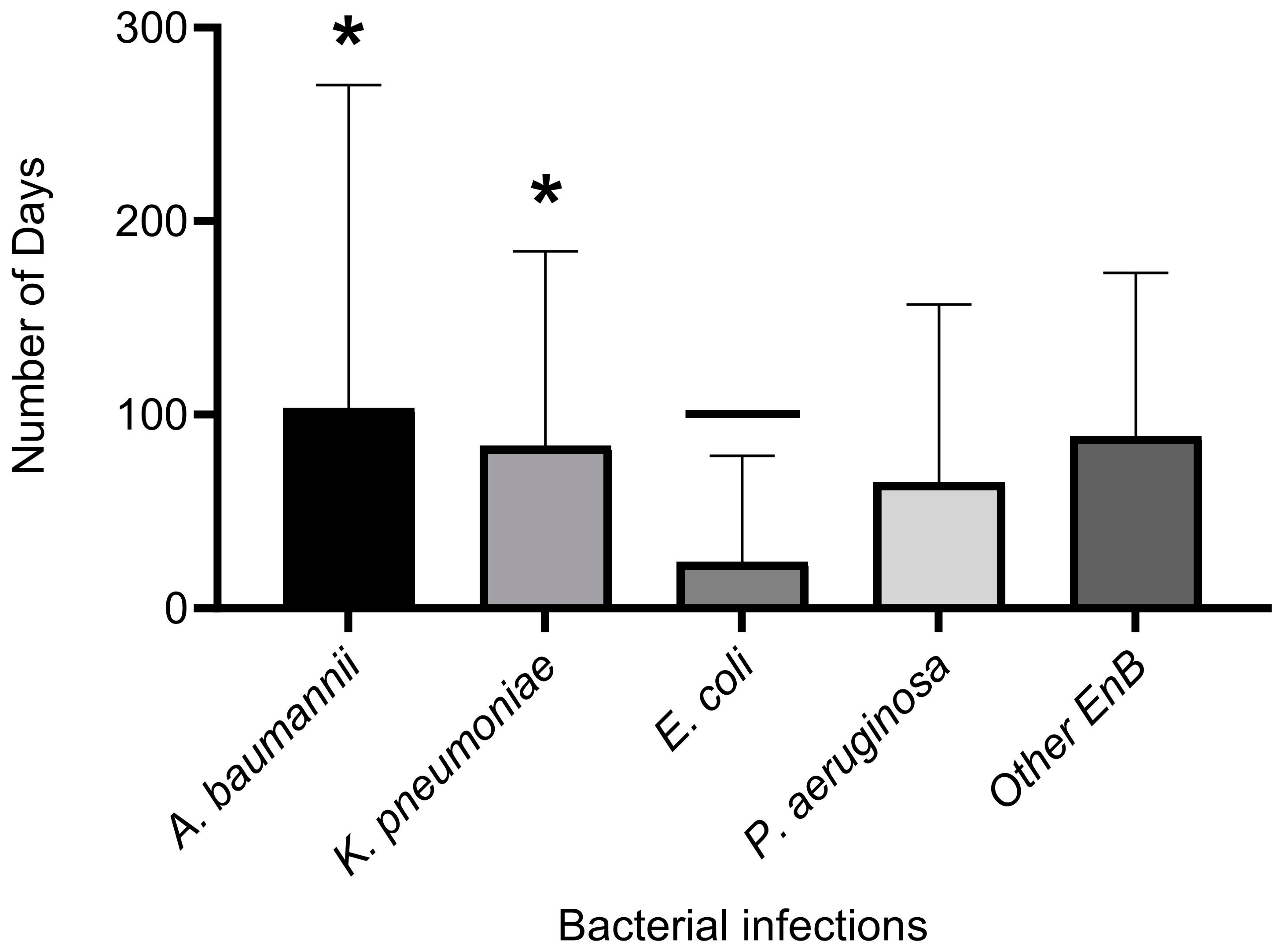
3.5. Comparing the Length of Hospital Stay by Type of Bacterial Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Balasubramanian, R.; Van Boeckel, T.P.; Carmeli, Y.; Cosgrove, S.; Laxminarayan, R. Global incidence in hospital-associated infections resistant to antibiotics: An analysis of point prevalence surveys from 99 countries. PLoS Med. 2023, 20, e1004178. [Google Scholar] [CrossRef]
- Dramowski, A.; Whitelaw, A.; Cotton, M.F. Burden, spectrum, and impact of healthcare-associated infection at a South African children’s hospital. J. Hosp. Infect. 2016, 94, 364–372. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Assessing the Health Burden of Infections with Antibiotic-Resistant Bacteria in the EU/EEA, 2016–2020; ECDC: Stockholm, Sweden, 2022. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Health-burden-infections-antibiotic-resistant-bacteria.pdf (accessed on 1 August 2021).
- Ventola, C.L. The antibiotic resistance crisis: Part 1: Causes and threats. Pharm. Ther. 2015, 40, 277–283. [Google Scholar]
- WHO. Antimicrobial Resistance: Global Report on Surveillance. 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/112642/9789241564748_eng.pdf;jsessionid=6340DE5721019788DC15BBF4EAD4B8F6?sequence=1 (accessed on 1 August 2021).
- Nørgaard, S.M.; Jensen, C.S.; Aalestrup, J.; Vandenbroucke-Grauls, C.M.J.E.; de Boer, M.G.J.; Pedersen, A.B. Choice of therapeutic interventions and outcomes for the treatment of infections caused by multidrug-resistant gram-negative pathogens: A systematic review. Antimicrob. Resist. Infect. Control 2019, 8, 170. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Peghin, M.; Vena, A.; Giacobbe, D.R. Treatment of Infections Due to MDR Gram-Negative Bacteria. Front. Med. 2019, 6, 74. [Google Scholar] [CrossRef] [PubMed]
- Forster, A.J.; Taljaard, M.; Oake, N.; Wilson, K.; Roth, V.; van Walraven, C. The effect of hospital-acquired infection with Clostridium difficile on length of stay in hospital. CMAJ 2012, 184, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.; Birhane, M.; Bekele, S.; Kibru, G.; Teshager, L.; Yilma, Y.; Ahmed, Y.; Fentahun, N.; Assefa, H.; Gashaw, M.; et al. Healthcare associated infection and its risk factors among patients admitted to a tertiary hospital in Ethiopia: Longitudinal study. Antimicrob. Resist. Infect. Control 2018, 7, 2. [Google Scholar] [CrossRef]
- O’Neill, J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations. 2016. Available online: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf (accessed on 1 August 2021).
- Vincent, J.L.; Rello, J.; Marshall, J.; Silva, E.; Anzueto, A.; Martin, C.D.; Moreno, R.; Lipman, J.; Gomersall, C.; Sakr, Y.; et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA 2009, 302, 2323–2329. [Google Scholar] [CrossRef]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and Pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef]
- Alkofide, H.; Alhammad, A.M.; Alruwaili, A.; Aldemerdash, A.; Almangour, T.A.; Alsuwayegh, A.; Almoqbel, D.; Albati, A.; Alsaud, A.; Enani, M. Multidrug-Resistant and Extensively Drug-Resistant Enterobacteriaceae: Prevalence, Treatments, and Outcomes—A Retrospective Cohort Study. Infect. Drug Resist. 2020, 13, 4653–4662. [Google Scholar] [CrossRef]
- Iwuafor, A.A.; Ogunsola, F.T.; Oladele, R.O.; Oduyebo, O.O.; Desalu, I.; Egwuatu, C.C.; Nnachi, A.U.; Akujobi, C.N.; Ita, I.O.; Ogban, G.I. Incidence, Clinical Outcome and Risk Factors of Intensive Care Unit Infections in the Lagos University Teaching hospital (LUTH), Lagos, Nigeria. PLoS ONE 2016, 11, e0165242. [Google Scholar] [CrossRef]
- El-Saed, A.; Balkhy, H.H.; Alshamrani, M.M.; Aljohani, S.; Alsaedi, A.; Al Nasser, W.; El Gammal, A.; Almohrij, S.A.; Alyousef, Z.; Almunif, S.; et al. High contribution and impact of resistant gram-negative pathogens causing surgical site infections at a multi-hospital healthcare system in Saudi Arabia, 2007–2016. BMC Infect. Dis. 2020, 20, 275. [Google Scholar] [CrossRef]
- Friedrich, A.W. Control of hospital acquired infections and antimicrobial resistance in Europe: The way to go. Wien. Med. Wochenschr. 2019, 169, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.K.; Wertheim, H.F.; Sumpradit, N.; Vlieghe, E.; Hara, G.L.; Gould, I.M.; Goossens, H.; et al. Antibiotic resistance-the need for global solutions. Lancet Infect. Dis. 2013, 13, 1057–1098. [Google Scholar] [CrossRef] [PubMed]
- Razine, R.; Azzouzi, A.; Barkat, A.; Khoudri, I.; Hassouni, F.; Chefchaouni, A.C.; Abouqal, R. Prevalence of hospital-acquired infections in the university medical center of Rabat, Morocco. Int. Arch. Med. 2012, 5, 26. [Google Scholar] [CrossRef]
- Balkhy, H.H.; Cunningham, G.; Chew, F.K.; Francis, C.; Al Nakhli, D.J.; Almuneef, M.A.; Memish, Z.A. Hospital- and community-acquired infections: A point prevalence and risk factors survey in a tertiary care center in Saudi Arabia. Int. J. Infect. Dis. 2006, 10, 326–333. [Google Scholar] [CrossRef]
- Endalafer, N.; Gebre-Selassie, S.; Kotiso, B. Nosocomial bacterial infections in a tertiary hospital in Ethiopia. J. Infect. Prev. 2011, 12, 38–43. [Google Scholar] [CrossRef]
- Ige, O.K.; Adesanmi, A.A.; Asuzu, M.C. Hospital-acquired infections in a Nigerian tertiary health facility: An audit of surveillance reports. Niger. Med. J. 2011, 52, 239–243. [Google Scholar] [CrossRef]
- Mutair, A.A.; Alhumaid, S.; Alawi, Z.A.; Zaidi, A.R.Z.; Alzahrani, A.J.; Al-Tawfiq, J.A.; Al-Shammari, H.; Rabaan, A.A.; Khojah, O.; Al-Omari, A. Five-year resistance trends in pathogens causing healthcare-associated infections at a multi-hospital healthcare system in Saudi Arabia, 2015–2019. J. Glob. Antimicrob. Resist. 2021, 25, 142–150. [Google Scholar] [CrossRef]
- Cella, E.; Ciccozzi, M.; Lo Presti, A.; Fogolari, M.; Azarian, T.; Prosperi, M.; Salemi, M.; Equestre, M.; Antonelli, F.; Conti, A.; et al. Multi-drug resistant Klebsiella pneumoniae strains circulating in hospital setting: Whole-genome sequencing and Bayesian phylogenetic analysis for outbreak investigations. Sci. Rep. 2017, 7, 3534. [Google Scholar] [CrossRef]
- Agyepong, N.; Fordjour, F.; Owusu-Ofori, A. Multidrug-resistant Acinetobacter baumannii in healthcare settings in Africa. Front. Trop. Dis. 2023, 4, 1110125. [Google Scholar] [CrossRef]
- Voidazan, S.; Albu, S.; Toth, R.; Grigorescu, B.; Rachita, A.; Moldovan, I. Healthcare Associated Infections-A New Pathology in Medical Practice. Int. J. Environ. Res. Public Health 2020, 17, 760. [Google Scholar] [CrossRef] [PubMed]
- Kharaba, A.; Abdelaziz Hussein, M.A.; Al-Hameed, F.M.; Mandourah, Y.; Almekhlafi, G.A.; Algethamy, H.; Hamdan, A.; Azem, M.A.; Fatani, J.; Al Beshabshe, A.; et al. Acinetobacter baumannii in Saudi Arabia: The New Growing Threat. Saudi Crit. Care J. 2019, 3, 54–57. Available online: https://www.sccj-sa.org/text.asp?2019/3/1/54/259469 (accessed on 24 June 2023). [CrossRef]
- Aly, M.M.; Abu Alsoud, N.M.; Elrobh, M.S.; Al Johani, S.M.; Balkhy, H.H. High prevalence of the PER-1 gene among carbapenem-resistant Acinetobacter baumannii in Riyadh, Saudi Arabia. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1759–1766. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, M.E. Prevalence of Acinetobacter baumannii in Saudi Arabia: Risk factors, antimicrobial resistance patterns and mechanisms of carbapenem resistance. Ann. Clin. Microbiol. Antimicrob. 2019, 18, 1. [Google Scholar] [CrossRef] [PubMed]
- Abdalhamid, B.; Hassan, H.; Itbaileh, A.; Shorman, M. Characterization of carbapenem-resistant Acinetobacter baumannii clinical isolates in a tertiary care hospital in Saudi Arabia. New Microbiol. 2014, 37, 65–73. [Google Scholar]
- Al-Obeid, S.; Jabri, L.; Al-Agamy, M.; Al-Omari, A.; Shibl, A. Epidemiology of extensive drug resistant Acinetobacter baumannii (XDRAB) at Security Forces hospital (SFH) in Kingdom of Saudi Arabia (KSA). J. Chemother. 2015, 27, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Senok, A.; Garaween, G.; Raji, A.; Khubnani, H.; Kim Sing, G.; Shibl, A. Genetic relatedness of clinical and environmental Acinetobacter baumannii isolates from an intensive care unit outbreak. J. Infect. Dev. Ctries. 2015, 9, 665–669. [Google Scholar] [CrossRef] [PubMed]
- Al-Gethamy, M.M.; Faidah, H.S.; Adetunji, H.A.; Haseeb, A.; Ashgar, S.S.; Mohanned, T.K.; Mohammed, A.H.; Khurram, M.; Hassali, M.A. Risk factors associated with multi-drug-resistant Acinetobacter baumannii nosocomial infections at a tertiary care hospital in Makkah, Saudi Arabia - a matched case-control study. J. Int. Med. Res. 2017, 45, 1181–1189. [Google Scholar] [CrossRef]
- Khan, M.A.; Mahomed, M.F.; Ashshi, A.M. Drug resistance patterns of Acinetobacter baumannii in Makkah, Saudi Arabia. Pak. J. Med. Res. 2012, 51, 127–131. Available online: https://applications.emro.who.int/imemrf/Pak_J_Med_Res/Pak_J_Med_Res_2012_51_4_127_131.pdf (accessed on 24 June 2023).
- Kadri, S.S.; Adjemian, J.; Lai, Y.L.; Spaulding, A.B.; Ricotta, E.; Prevots, D.R.; Palmore, T.N.; Rhee, C.; Klompas, M.; Dekker, J.P.; et al. Difficult-to-Treat Resistance in Gram-negative Bacteremia at 173 US Hospitals: Retrospective Cohort Analysis of Prevalence, Predictors, and Outcome of Resistance to All First-line Agents. Clin. Infect. Dis. 2018, 67, 1803–1814. [Google Scholar] [CrossRef] [PubMed]
- Patolia, S.; Abate, G.; Patel, N.; Patolia, S.; Frey, S. Risk factors and outcomes for multidrug-resistant Gram-negative bacilli bacteremia. Ther. Adv. Infect. Dis. 2018, 5, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Zusman, O.; Avni, T.; Leibovici, L.; Adler, A.; Friberg, L.; Stergiopoulou, T.; Carmeli, Y.; Paul, M. Systematic review and meta-analysis of in vitro synergy of polymyxins and carbapenems. Antimicrob. Agents Chemother. 2013, 57, 5104–5111. [Google Scholar] [CrossRef]
- Walker, M.M.; Roberts, J.A.; Rogers, B.A.; Harris, P.N.A.; Sime, F.B. Current and Emerging Treatment Options for Multidrug Resistant Escherichia coli Urosepsis: A Review. Antibiotics 2022, 11, 1821. [Google Scholar] [CrossRef] [PubMed]
- Zeina, A.K.; MSSouha, S.K. Acinetobacter infection: Treatment and prevention. Official reprint from UpToDate www.uptodate.com 2023. Available online: https://www.uptodate.com/contents/acinetobacter-infection-treatment-and-prevention/print (accessed on 4 June 2023).
- Sarkar, P.; Samaddar, S.; Ammanathan, V.; Yarlagadda, V.; Ghosh, C.; Shukla, M.; Kaul, G.; Manjithaya, R.; Chopra, S.; Haldar, J. Vancomycin Derivative Inactivates Carbapenem-Resistant Acinetobacter baumannii and Induces Autophagy. ACS Chem. Biol. 2020, 15, 884–889. [Google Scholar] [CrossRef] [PubMed]
- Schmid, A.; Wolfensberger, A.; Nemeth, J.; Schreiber, P.W.; Sax, H.; Kuster, S.P. Monotherapy versus combination therapy for multidrug-resistant Gram-negative infections: Systematic Review and Meta-Analysis. Sci. Rep. 2019, 9, 15290. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group | Frequency (N) | Percentage (%) | p-Value | |
|---|---|---|---|---|
| Age | 0-10 10-20 21-30 31-40 41-50 51-60 61-70 71-80 81-90 91-100 | 8 1 13 11 10 18 17 10 12 1 | 7.92 0.99 12.8 10.9 9.9 17.8 16.8 9.9 12 0.99 | 0.00 a |
| Gender | Females | 51 | 50 | |
| Males | 45 | 45 | 0.91 b | |
| NS | 5 | 5 | ||
| Departments (Hospital wards) | Cardiology ENT ER Family medicine General surgery Geriatric medicine ICU Infectious diseases Internal medicine Nephrology Neurology Neurosurgery NS ObGYNE Oncology Orthopaedic Paediatrics Urology | 2 4 15 2 9 2 25 1 10 1 11 4 5 3 2 2 2 1 | 2 4 14.9 * 2 8.9 2 24.7 * 1 9.9 1 10.9 4 5 3 1.9 1.9 1.9 1 | 0.07672 c |
| Type of specimens | Wound swabs Blood Catheter urine Cephalic wound culture Ear swab Gluteal wound Incision Drainage NS Peritoneal fluid Rectal Swab Right maxillary sinus Sputum Tissue Culture Stool Tracheostomy Swab Transtracheal Aspirate Swab Urine | 15 4 3 1 3 1 4 5 2 1 1 4 2 1 1 14 38 | 15 * 4 3 1 3 1 4 5 2 1 1 4 2 1 1 14 38 * | 0.00024 d |
| Case No. | Age | Clinical Diagnosis | Therapeutic Description (Antibiotics) | Susceptibility Pattern | CLO | LOHS |
|---|---|---|---|---|---|---|
| 4 | 72 | Pneumonia, Pulmonary edema | Combined (MER, VAN) * | XDR | Died | 3 |
| 14 | 33 | Chest and abdomen necrotizing fasciitis | Combined (TAZ, TG) | MDR | AI | 18 |
| 16 | 54 | Necrotizing fasciitis and Multiple comorbidities | Mono therapy (MER) | MDR | ANI | 54 |
| 17 | NI | NI | NI | XDR | NI | NI |
| 20 | 79 | Tumour | Mono therapy (VAN) * | XDR | Died | 46 |
| 23 | 27 | Chronic ulcer of skin | Mono therapy (TAZ) | MDR | AI | 817 |
| 29 | 24 | Pneumonia and Bacteraemia | Combined (TZP, TG) | MDR | AI | 52 |
| 30 | NI | NI | NI | XDR | NI | NI |
| 34 | 66 | Pneumonia, Urosepsis | Combined (TAZ, LEVO) | MDR | Died | 135 |
| 36 | 64 | Stroke, UTI | Mono therapy (TAZ) | XDR | AI | 57 |
| 40 | 56 | Benign neoplasm of pituitary gland | Mono therapy (MER) | XDR | Died | 30 |
| 42 | 59 | Myocardial infraction | Mono therapy (MER) | XDR | Died | 49 |
| 44 | NI | NI | NI | MDR | NI | NI |
| 45 | 17 | Surgical site infection | Combined (VAN, MER) * | XDR | AI | 28 |
| 46 | 58 | Sepsis, Infected diabetic foot | Mono therapy (AUG) | MDR | AI | 54 |
| 50 | 60 | Bed sore | Combined (CAV-AVI, VAN) * | XDR | ANI | 171 |
| 55 | 58 | Intracranial haemorrhage | Combined (CAZ, VAN) * | XDR | Died | 13 |
| 57 | NI | NI | NI | MDR | NI | NI |
| 58 | 61 | Post gastric Sleeve peritonitis | Combined (GM, TG). | XDR | AI | 62 |
| 66 | 41 | Cephalic wound Infection | Combined (MER, VAN) * | MDR | AI | 307 |
| 68 | 85 | Complicated UTI | Combined (VAN, CIP) * | XDR | AI | 16 |
| 72 | 27 | Fever of Unknown origin | Combined (TAZ, TG). | XDR | AI | 69 |
| 78 | 63 | Bacterial pneumonia, Multiple comorbidities | Combined (CAV-AVI, TG). | XDR | ANI | 59 |
| 82 | 87 | Acute pulmonary edema | Combined (TG, CS) | XDR | Died | 180 |
| 83 | 33 | Tracheal perforation | Combined (MER, VAN) * | XDR | ANI | 48 |
| 88 | 54 | DM II, infective endocarditis | Mono therapy (CIP) | XDR | ANI | 17 |
| 89 | 55 | Sepsis | Combined (MER, CS) | XDR | ANI | 135 |
| 91 | 27 | Health care associated meningitis. | Combined (MER, VAN) * | MDR | ANI | 65 |
| Case No. | Age | Clinical Diagnosis | Therapeutic Description (Antibiotics) | Resistance Pattern | CLO | LOHS (Days) |
|---|---|---|---|---|---|---|
| 1 | 35 | Tumour and HAI Meningitis | Combined (MER, CIP) | CRE | Died | 316 |
| 2 | 60 | MMA adenocarcinoma | Monotherapy (AUG) | SS | AI | 14 |
| 5 | 26 | UTI | Monotherapy (CIP) | SS | AI | 1 |
| 13 | 56 | Nasal polyp | Monotherapy (AUG) | SS | AI | 1 |
| 15 | 49 | Leg chronic ulcer | Monotherapy (TAZ) | MDR | AI | 117 |
| 18 | 78 | UTI catheter, Bedsore, comorbidities | Combined (CIP, TAZ) | CRE | AI | 3 |
| 21 | 83 | Multiple comorbidities | Combined (CLOXA, CAZ-AVI, TAZ) | CRE | Died | 7 |
| 27 | 55 | UTI | Combined (GM, CAZ-AVI) | CRE | AI | 13 |
| 31 | 60 | UTI | Combined (CAV-AVI, VAN) * | CRE | ANI | 171 |
| 39 | 3 mths | Perforated auns, UTI | Monotherapy (MER) | CRE | AI | 14 |
| 52 | 45 | UTI | Combined (CEF, VAN) * | CRE | ANI | 1 |
| 59 | 82 | Septic shock and Pyelonephritis | Combined (CAV-AVI) | CRE | Died | 73 |
| 64 | 85 | Complicated UTI | Combined (VAN, CIP) * | CRE | Died | 16 |
| 67 | 62 | Infected Bedsore | Monotherapy (TG) | CRE | Died | 279 |
| 69 | 88 | Infected Bedsore | Monotherapy (MER) | CRE | Died | 16 |
| 70 | 61 | Pneumonia | Combined (CIP, TG) | CRE | AI | 14 |
| 76 | 63 | Bacterial pneumonia, UTI | Combined (CAV-AVI, TG) | CRE | ANI | 59 |
| 85 | 40 | UTI | Combined (AUG, AMP) | SS | AI | 1 |
| 86 | 77 | UTI | Combined (TAZ, GM) | CRE | ANI | 264 |
| 87 | 41 | UTI | Monotherapy (CIP) | MDR | AI | 1 |
| 93 | 55 | Sepsis | Combined (MER, CS) | CRE | ANI | 135 |
| 95 | 64 | Spine Infection, and Brucella | Combined (CIP, DOX) | CRE | ANI | 173 |
| 96 | 12 mths | Bacterial meningitis | Monotherapy (MER) | CRE | Died | 167 |
| 97 | 60 | Urosepsis and Aspiration pneumonia | Combined (CAV-AVI, CS, GM) | CRE | Died | 159 |
| Case No. | Age | Infection and Clinical Diagnosis | Therapeutic Description (Antibiotics) | Antibiotics Profile | CLO | LOHS |
|---|---|---|---|---|---|---|
| 3 | 47 | VZS and secondary Bacterial infection | Combined (CIP, LZD) | MDR | AI | 18 |
| 7 | 34 | UTI | Monotherapy (CIP) | SS | AI | 1 |
| 8 | 64 | UTI | Combined (CIP, T/S) | SS | AI | 1 |
| 11 | 44 | UTI | Combined (AUG, T/S) | SS | AI | 1 |
| 19 | 72 | UTI and Multiple comorbidities | Combined (BAC, CIP) | MDR | AI | 1 |
| 22 | 49 | Acute cystitis with Multiple comorbidities | Monotherapy (AUG) | MDR | AI | 1 |
| 26 | 27 | Acute cystitis | Monotherapy (NIT) | MDR | AI | 1 |
| 28 | 80 | Stage 4 Bed sore | Monotherapy (CEF) | MDR | Died | 80 |
| 32 | 39 | Sepsis and bilateral thigh abscess | Combined (VAN. TAZ) * | SS | AI | 21 |
| 35 | 72 | UTI | Monotherapy (NIT) | MDR | AI | 1 |
| 37 | 64 | Left PCA stroke, UTI | Monotherapy (TAZ) | MDR | AI | 57 |
| 38 | 87 | Infected Bed sore and UTI | Combined (CRO, CAZ) | MDR | Died | 31 |
| 41 | 24 | Ileocecal stricture | Monotherapy (AUG) | MDR | AI | 30 |
| 47 | 36 | UTI | Monotherapy (CTX) | SS | AI | 1 |
| 48 | 37 | UTI | Monotherapy (CRO) | MDR | AI | 1 |
| 49 | 82 | UTI | Monotherapy (TAZ) | MDR | ANI | 1 |
| 54 | 90 | Complicated UTI | Combined (AUG, NIT) | MDR | ANI | 1 |
| 61 | 23 | UTI | No antibiotic given | MDR | ANI | 1 |
| 71 | 31 | Hydronephrosis, Sepsis | Monotherapy (CIP) | MDR | AI | 17 |
| 74 | 57 | Viral pneumonia and UTI | Monotherapy (TAZ) | MDR | ANI | 30 |
| 77 | 12 mths | UTI | Monotherapy (AUG) | MDR | ANI | 1 |
| 79 | 65 | Post gastric bypass leak | Combined (IMI, VAN) * | CRE | ANI | 60 |
| 94 | 29 | UTI (case of Sickle Cell Disease) | Monotherapy (T/S) | MDR | ANI | 1 |
| 98 | 72 | UTI | Monotherapy (CIP) | MDR | ANI | 1 |
| 99 | 54 | UTI | Monotherapy (AUG) | MDR | ANI | 2 |
| 100 | 77 | UTI | Monotherapy (CS) | CRE | Died | 264 |
| Case No. | Age | Infection and Clinical Diagnosis | Therapeutic Description (Antibiotics) | Susceptibility Profile | CLO | LOHS (Days) |
|---|---|---|---|---|---|---|
| 6 | 40 | UTI with Vaso occlusive crisis | Monotherapy (LEVO) | SS | AI | 1 |
| 12 | 22 | Bilateral otitis externa | Monotherapy (GM) | SS | AI | 1 |
| 24 | 44 | Nasal Polyp, Chronic otitis media | Combine (TobraDex, AUG) | XDR | AI | 1 |
| 25 | 93 | Right MCA stroke | Combine (CRO, CAZ) | XDR | AI | NI |
| 33 | 25 | Bacterial meningitis | Monotherapy (MER) | MDR | Died | 166 |
| 51 | 89 | Pneumonia | Monotherapy (TAZ) | XDR | Died | 139 |
| 60 | 87 | Urosepsis | Monotherapy (GM) | XDR | AI | 7 |
| 65 | 69 | Leg cellulitis, UTI | Combine (IMI, CIP) | MDR | AI | 46 |
| 73 | 61 | Sepsis | Combine (GM, TG) | XDR | AI | 62 |
| 75 | 62 | UTI | Combine (AUG, TG) | MDR | Died | 279 |
| 84 | 61 | Diabetic foot infection with gangrene | Combine (MER, VAN, TG) * | XDR | Died | 14 |
| 90 | 45 | Chronic suppurative otitis media | Monotherapy (LEVO) | XDR | ANI | 1 |
| Case No. | Age | Clinical Diagnosis | Antibiotic Treatment | Infecting Bacteria | Antibiotics Profile | CLO | LOHS (Days) |
|---|---|---|---|---|---|---|---|
| 9 | 45 | UTI, multiple comorbidities | Monotherapy (CEF) | Proteus mirabilis | MDR | ANI | 1 |
| 10 | 58 | Stroke | Combined (VAN, CEF) * | Enterobacter Cloacae | SS | ANI | 236 |
| 43 | 35 | Bacterial meningitis | Monotherapy (BAC) | Providencia stuartii | MDR | AI | NI |
| 53 | 80 | Stroke (Bed ridden) | No antibiotic given | Providencia stuartii | MDR | Died | 202 |
| 56 | 27 | Bloody Diarrhoea | Monotherapy (MET) | Shigella flexneri | MDR | ANI | 1 |
| 63 | 60 | Urosepsis and aspiration Pneumonia | Combined (CAV-AVI, CS, GM) | Proteus mirabilis | MDR | Died | 159 |
| 80 | 63 | Bacterial pneumonia, Multiple comorbidities | Combined (CAV-AVI, TG) | Serratia marcescens | CRE | ANI | 59 |
| 81 | 82 | UTI, sepsis | Combined (CAV-AVI, VAN) * | Proteus mirabilis | CRE | ANI | 73 |
| 92 | 27 | HA-pneumonia/ventilatory associated pneumonia. | Monotherapy (TAZ) | Providencia stuartii | MDR | ANI | 69 |
| 101 | 65 | UTI | Monotherapy (SXT) | Proteus mirabilis | MDR | AI | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Badger-Emeka, L.; Al Rashed, A.S.; Aljindan, R.Y.; Emeka, P.M.; Quadri, S.A.; Almutairi, H.H. Incidence of Drug-Resistant Hospital-Associated Gram-Negative Bacterial Infections, the Accompanying Risk Factors, and Clinical Outcomes with Treatment. Antibiotics 2023, 12, 1425. https://doi.org/10.3390/antibiotics12091425
Badger-Emeka L, Al Rashed AS, Aljindan RY, Emeka PM, Quadri SA, Almutairi HH. Incidence of Drug-Resistant Hospital-Associated Gram-Negative Bacterial Infections, the Accompanying Risk Factors, and Clinical Outcomes with Treatment. Antibiotics. 2023; 12(9):1425. https://doi.org/10.3390/antibiotics12091425
Chicago/Turabian StyleBadger-Emeka, Lorina, Abdullatif S. Al Rashed, Reem Y. Aljindan, Promise Madu Emeka, Sayed A. Quadri, and Hayfa Habes Almutairi. 2023. "Incidence of Drug-Resistant Hospital-Associated Gram-Negative Bacterial Infections, the Accompanying Risk Factors, and Clinical Outcomes with Treatment" Antibiotics 12, no. 9: 1425. https://doi.org/10.3390/antibiotics12091425