

Ceftazidime-Avibactam as Osteomyelitis Therapy: A Miniseries and Review of the Literature


Abstract
:1. Introduction
2. Cases Description
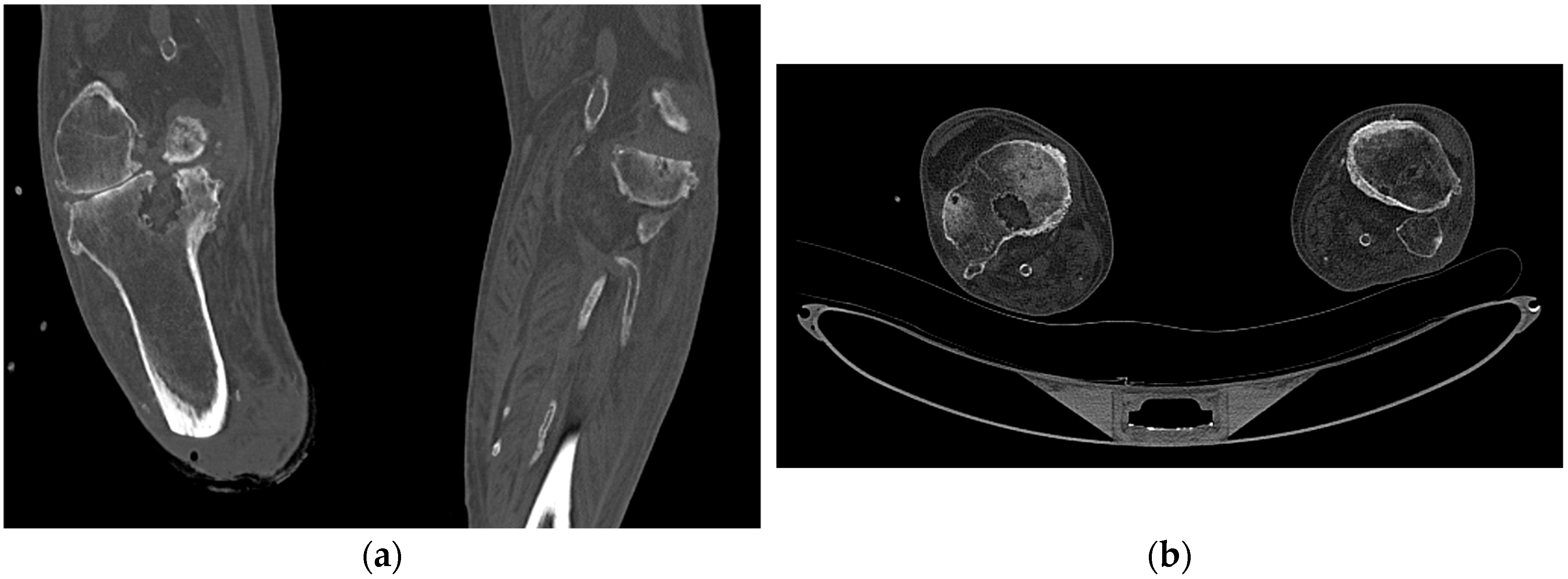
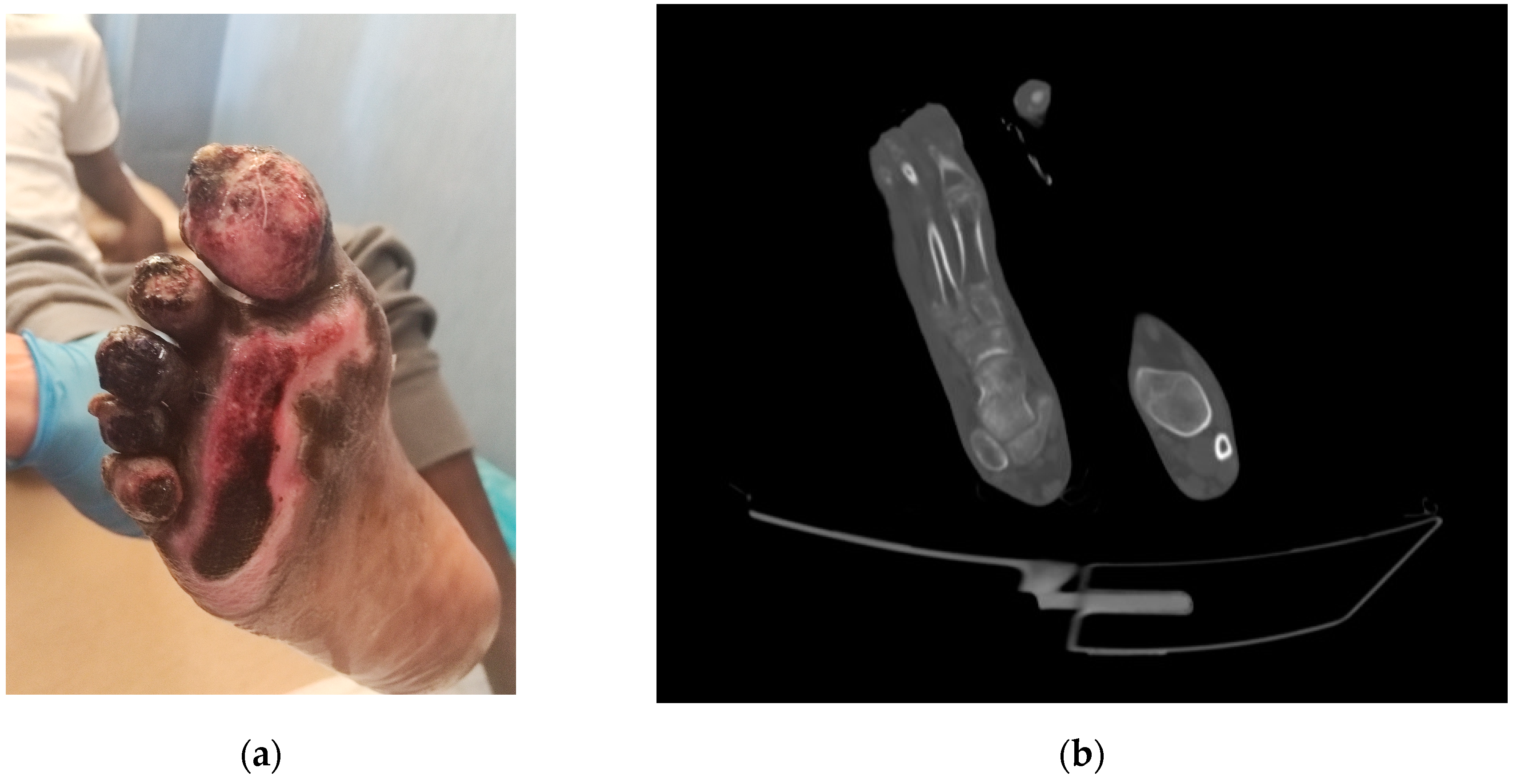
2.1. Patient 1
2.2. Patient 2
2.3. Patient 3
3. Discussion and Review of the Literature
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Urish, K.L.; Cassat, J.E. Staphylococcus aureus Osteomyelitis: Bone, Bugs, and Surgery. Infect. Immun. 2020, 88, e00932-19. [Google Scholar] [CrossRef]
- Titécat, M.; Senneville, E.; Wallet, F.; Dezèque, H.; Migaud, H.; Courcol, R.J.; Loïez, C. Bacterial epidemiology of osteoarticular infections in a referent center: 10-year study. Orthop. Traumatol. Surg. Res. 2013, 99, 653–658. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control and WHO Regional Office for Europe. Surveillance of Antimicrobial Resistance in Europe, 2021 Data: Executive Summary; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2022. [Google Scholar]
- Zhanel, G.G.; Lawson, C.D.; Adam, H.; Schweizer, F.; Zelenitsky, S.; Lagacé-Wiens, P.R.; Denisuik, A.; Rubinstein, E.; Gin, A.S.; Hoban, D.J.; et al. Ceftazidime-avibactam: A novel cephalosporin/β-lactamase inhibitor combination. Drugs 2013, 73, 159–177. [Google Scholar] [CrossRef] [PubMed]
- Mushtaq, S.; Warner, M.; Livermore, D.M. In vitro activity of ceftazidime+NXL104 against Pseudomonas aeruginosa and other non-fermenters. J. Antimicrob. Chemother. 2010, 65, 2376–2381. [Google Scholar] [CrossRef] [PubMed]
- Curcio, D. Activity of a novel combination against multidrug-resistant nonfermenters: Ceftazidime plus NXL104. Expert. Rev. Anti-Infect. Ther. 2011, 9, 173–176. [Google Scholar] [CrossRef]
- National Pressure Ulcer Advisory Panel; European Pressure Ulcer Advisory Panel; Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers: Quick Reference Guide; Haesler, E., Ed.; Cambridge Media: Osborne Park, Australia, 2014. [Google Scholar]
- Cani, E.; Moussavi, F.; Ocheretyaner, E.; Sharma, R.; Brown, C.; Eilertson, B. Carbapenem-resistant Klebsiella pneumoniae vertebral osteomyelitis in a renal transplant recipient treated with ceftazidime-avibactam. Transpl. Infect. Dis. 2018, 20, e12837. [Google Scholar] [CrossRef]
- Rico-Nieto, A.; Moreno-Ramos, F.; Fernández-Baillo, N. Lumbar arthrodesis infection by multi-resistant Klebsiella pneumoniae, successfully treated with implant retention and ceftazidime/avibactam. Rev. Esp. Cir. Ortop. Traumatol. 2018, 62, 471–473. [Google Scholar] [CrossRef]
- De León-Borrás, R.; Álvarez-Cardona, J.; Vidal, J.A.; Guiot, H.M. Ceftazidime/Avibactam for Refractory Bacteremia, Vertebral Diskitis/Osteomyelitis with Pre-Vertebral Abscess and Bilateral Psoas Pyomyositis Secondary to Klebsiella Pneumoniae Carbapenemase-Producing Bacteria (KPC). P. R. Health Sci. J. 2018, 37, 128–131. [Google Scholar]
- Rodríguez-Núñez, O.; Ripa, M.; Morata, L.; de la Calle, C.; Cardozo, C.; Fehér, C.; Pellicé, M.; Valcárcel, A.; Puerta-Alcalde, P.; Marco, F.; et al. Evaluation of ceftazidime/avibactam for serious infections due to multidrug-resistant and extensively drug-resistant Pseudomonas aeruginosa. J. Glob. Antimicrob. Resist. 2018, 15, 136–139. [Google Scholar] [CrossRef]
- Mittal, J.; Szymczak, W.A.; Guo, Y.; Levi, M.H.; Chen, L.; Kreiswirth, B.N.; Riska, P.F.; Nori, P. Two for the price of one: Emerging carbapenemases in a returning traveller to New York City. BMJ Case Rep. 2018, 2018, bcr2018225440. [Google Scholar] [CrossRef]
- Schimmenti, A.; Brunetti, E.; Seminari, E.; Mariani, B.; Cambieri, P.; Orsolini, P. Prosthetic Joint Infection from Carbapenemase-Resistant Klebsiella pneumoniae Successfully Treated with Ceftazidime-Avibactam. Case Rep. Infect. Dis. 2018, 2018, 1854805. [Google Scholar] [CrossRef] [PubMed]
- Alamarat, Z.I.; Babic, J.; Tran, T.T.; Wootton, S.H.; Dinh, A.Q.; Miller, W.R.; Hanson, B.; Wanger, A.; Gary, J.L.; Arias, C.A.; et al. Long-Term Compassionate Use of Cefiderocol To Treat Chronic Osteomyelitis Caused by Extensively Drug-Resistant Pseudomonas aeruginosa and Extended-Spectrum-β-Lactamase-Producing Klebsiella pneumoniae in a Pediatric Patient. Antimicrob. Agents Chemother. 2020, 64, e01872-19. [Google Scholar] [CrossRef] [PubMed]
- Meschiari, M.; Franconi, I.; Bacca, E.; Bianco, V.; Orlando, G.; Cuomo, G.; Bedini, A.; Mussini, C. Ceftazidime/avibactam and ceftolozane/tazobactam for the treatment of extensively drug-resistant Pseudomonas aeruginosa post-neurosurgical infections: Three cases and a review of the literature. Infection 2021, 49, 549–553. [Google Scholar] [CrossRef]
- Mularoni, A.; Mezzatesta, M.L.; Pilato, M.; Medaglia, A.A.; Cervo, A.; Bongiorno, D.; Aprile, A.; Luca, A.; Stefani, S.; Grossi, P. Combination of aztreonam, ceftazidime-avibactam and amikacin in the treatment of VIM-1 Pseudomonas aeruginosa ST235 osteomyelitis. Int. J. Infect. Dis. 2021, 108, 510–512. [Google Scholar] [CrossRef] [PubMed]
- Ji, Z.; Sun, K.; Li, Z.; Cheng, W.; Yang, J. Carbapenem-Resistant Klebsiella pneumoniae Osteomyelitis Treated with Ceftazidime-Avibactam in an Infant: A Case Report. Infect. Drug Resist. 2021, 14, 3109–3113. [Google Scholar] [CrossRef] [PubMed]
- Eskenazi, A.; Lood, C.; Wubbolts, J.; Hites, M.; Balarjishvili, N.; Leshkasheli, L.; Askilashvili, L.; Kvachadze, L.; van Noort, V.; Wagemans, J.; et al. Combination of pre-adapted bacteriophage therapy and antibiotics for treatment of fracture-related infection due to pandrug-resistant Klebsiella pneumoniae. Nat. Commun. 2022, 13, 302. [Google Scholar] [CrossRef]
- Racenis, K.; Rezevska, D.; Madelane, M.; Lavrinovics, E.; Djebara, S.; Petersons, A.; Kroica, J. Use of Phage Cocktail BFC 1.10 in Combination With Ceftazidime-Avibactam in the Treatment of Multidrug-Resistant Pseudomonas aeruginosa Femur Osteomyelitis-A Case Report. Front. Med. 2022, 9, 851310. [Google Scholar] [CrossRef] [PubMed]
- Rubnitz, Z.A.; Kunkel, V.N.; Baselski, V.S.; Summers, N.A. A Case of New Delhi Metallo-β-Lactamases (NDM) Citrobacter sedlakii Osteomyelitis Successfully Treated With Ceftazidime-Avibactam and Aztreonam. Cureus 2022, 14, e28855. [Google Scholar] [CrossRef]
- Rempenault, C.; Pagis, V.; Noussair, L.; Berbescu, S.; Duran, C.; Bouchand, F.; de Laroche, M.; Salomon, E.; Nich, C.; Bauer, T.; et al. Treatment of bone and joint infections by ceftazidime/avibactam and ceftolozane/tazobactam: A cohort study. J. Glob. Antimicrob. Resist. 2021, 25, 282–286. [Google Scholar] [CrossRef]
- Davido, B.; Crémieux, A.C.; Vaugier, I.; Gatin, L.; Noussair, L.; Massias, L.; Laurent, F.; Saleh-Mghir, A. Efficacy of ceftazidime-avibactam in various combinations for the treatment of experimental osteomyelitis due to Klebsiella pneumoniae carbapenemase (KPC)-producing Klebsiella pneumoniae. Int. J. Antimicrob. Agents 2023, 61, 106702. [Google Scholar] [CrossRef]
- Davido, B.; Crémieux, A.C.; Vaugier, I.; De Truchis, P.; Hamami, K.; Laurent, F.; Saleh-Mghir, A. Efficacy of ceftazidime/avibactam in various combinations for the treatment of experimental osteomyelitis in rabbits caused by OXA-48-/ESBL-producing Escherichia coli. J. Antimicrob. Chemother. 2023, 78, 1211–1218. [Google Scholar] [CrossRef] [PubMed]
- Montero, M.M.; Domene Ochoa, S.; López-Causapé, C.; Luque, S.; Sorlí, L.; Campillo, N.; López Montesinos, I.; Padilla, E.; Prim, N.; Angulo-Brunet, A.; et al. Time-Kill Evaluation of Antibiotic Combinations Containing Ceftazidime-Avibactam against Extensively Drug-Resistant Pseudomonas aeruginosa and Their Potential Role against Ceftazidime-Avibactam-Resistant Isolates. Microbiol. Spectr. 2021, 9, e0058521. [Google Scholar] [CrossRef] [PubMed]
- Papp-Wallace, K.M.; Zeiser, E.T.; Becka, S.A.; Park, S.; Wilson, B.M.; Winkler, M.L.; D’Souza, R.; Singh, I.; Sutton, G.; Fouts, D.E.; et al. Ceftazidime-Avibactam in Combination with Fosfomycin: A Novel Therapeutic Strategy Against Multidrug-Resistant Pseudomonas aeruginosa. J. Infect. Dis. 2019, 220, 666–676. [Google Scholar] [CrossRef] [PubMed]
- Zhong, H.; Zhao, X.Y.; Zhang, Z.L.; Gu, Z.C.; Zhang, C.; Gao, Y.; Cui, M. Evaluation of the efficacy and safety of ceftazidime/avibactam in the treatment of Gram-negative bacterial infections: A systematic review and meta-analysis. Int. J. Antimicrob. Agents 2018, 52, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Sternbach, N.; Leibovici Weissman, Y.; Avni, T.; Yahav, D. Efficacy and safety of ceftazidime/avibactam: A systematic review and meta-analysis. J. Antimicrob. Chemother. 2018, 73, 2021–2029. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Susceptibility Profile (MIC) | |||
|---|---|---|---|
| Antimicrobial | Patient 1 | Patient 2 | Patient 3 |
| Piperacillin–tazobactam | R | R (64/4) | R (64/4) |
| Ceftazidime | I | R (16) | R (>16) |
| Ceftazidime–avibactam | S | S (8/4) | S (4/4) |
| Cefepime | I | R (>8) | R (>8) |
| Ceftolozane–tazobactam | R | R (>4/4) | R (>4/4) |
| Imipenem | R | R (>8) | R (>8) |
| Meropenem | R | R (>16) | R (>16) |
| Meropenem–vaborbactam | R | R (>8/8) | R (>8/8) |
| Aztreonam | I | R (>16) | I (8) |
| Amikacin | R | R (>16) | S (16) |
| Tobramycin | R | R (>4) | S (≤1) |
| Ciprofloxacin | R | R (>1) | I (0.25) |
| Colistin | N/A | S (1) | S (2) |
| Laboratory examination | Patient 1 | Patient 2 | Patient 3 |
|---|---|---|---|
| White blood cell (cells/μL) | 6400 | 10,900 | 5700 |
| Haemoglobin (g/dL) | 9.6 | 12.6 | 12.1 |
| Platelet (cells/μL) | 346,000 | 217,000 | 314,000 |
| Serum creatinine (mg/dL) | 0.81 | 0.62 | 0.64 |
| ALT (U/L) | 11 | 22 | 12 |
| AST (U/L) | 14 | 15 | 17 |
| C-reactive protein (mg/L) | 10.57 | 22 | 0.6 |
| Ceftazidime/Avibactam | Outcome | |||||||
|---|---|---|---|---|---|---|---|---|
| First Author and Year | Bacterium | Mechanism of Resistance | Dosage | Antibiotics Combination | Treatment (days) | Surgical Treatment | Clinical Cure | Microbiological Cure |
| Cani E, 2017 [8] | K. pneumoniae | N/A | 2.5 g t.i.d. | Amikacin | 42 | Yes | Yes | N/A |
| Rico-Nieto A, 2018 [9] | K. pneumoniae | OXA-48 | 2.5 g t.i.d. | Colistin | 56 | Yes | Yes | N/A |
| De León-Borrás R, 2018 [10] | K. pneumoniae | KPC | N/A | Amikacin, polymyxin B | 42 | No | Yes | N/A |
| Rodríguez-Núñez O, 2018 [11] | P. aeruginosa | N/A | N/A | Tobramycin, ciprofloxacin | 34 | Yes | No | Yes |
| Mittal J, 2018 [12] | K. pneumoniae | NDM, OXA-181 | 2.5 g t.i.d. | Aztreonam | 46 | Yes | Yes | Yes |
| Schimmenti A, 2018 [13] | K. pneumoniae | KPC | 2.5 g t.i.d. | None | 14 | Yes | Yes | Yes |
| Alamarat ZI, 2020 [14] | P. aeruginosa K. pneumoniae | NDM-1 KPC | 2.5 g t.i.d. | Aztreonam | 14 | Yes | No | N/A |
| Meschiari A, 2021 [15] | P. aeruginosa K. pneumoniae P. aeruginosa | N/A KPC N/A | 2.5 g q.i.d. 2.5 g t.i.d. | Aztreonam Aztreonam | 42 56 | Yes Yes | Yes Yes | N/A N/A |
| Mularoni A, 2021 [16] | P. aeruginosa | VIM-1 | 2.5 g t.i.d. | Amikacin, aztreonam | 42 | Yes | Yes | Yes |
| Ji Z, 2021 [17] | K. pneumoniae | N/A | 2.5 g t.i.d. | None | 21 | Yes | Yes | Yes |
| Eskenazi A, 2022 [18] | K. pneumoniae | OXA-48 | 2.5 g t.i.d. | Moxifloxacin, phage | 88 | Yes | Yes | Yes |
| Racenis K, 2022 [19] | P. aeruginosa | KPC | 2.5 g t.i.d. | Phage | 15 | Yes | No | No |
| Rubnitz ZA, 2022 [20] | C. sedlakii | NDM | 2.5 g t.i.d. | Aztreonam | 42 | Yes | No | Yes |
| Present cases, 2023 | P. aeruginosa P. aeruginosa P. aeruginosa | N/A N/A N/A | 2.5 g t.i.d. 2.5 g t.i.d. 2.5 g t.i.d. | None Fosfomycin Amikacin | 42 42 42 | No Yes Yes | Yes Yes Yes | N/A N/A N/A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mancuso, A.; Pipitò, L.; Rubino, R.; Distefano, S.A.; Mangione, D.; Cascio, A. Ceftazidime-Avibactam as Osteomyelitis Therapy: A Miniseries and Review of the Literature. Antibiotics 2023, 12, 1328. https://doi.org/10.3390/antibiotics12081328
Mancuso A, Pipitò L, Rubino R, Distefano SA, Mangione D, Cascio A. Ceftazidime-Avibactam as Osteomyelitis Therapy: A Miniseries and Review of the Literature. Antibiotics. 2023; 12(8):1328. https://doi.org/10.3390/antibiotics12081328
Chicago/Turabian StyleMancuso, Alessandro, Luca Pipitò, Raffaella Rubino, Salvatore Antonino Distefano, Donatella Mangione, and Antonio Cascio. 2023. "Ceftazidime-Avibactam as Osteomyelitis Therapy: A Miniseries and Review of the Literature" Antibiotics 12, no. 8: 1328. https://doi.org/10.3390/antibiotics12081328