
Outcome of Irrigation and Debridement with Topical Antibiotic Delivery Using Antibiotic-Impregnated Calcium Hydroxyapatite for the Management of Periprosthetic Hip Joint Infection

Abstract
:1. Introduction
2. Results
2.1. Pre-Operative Patient Information
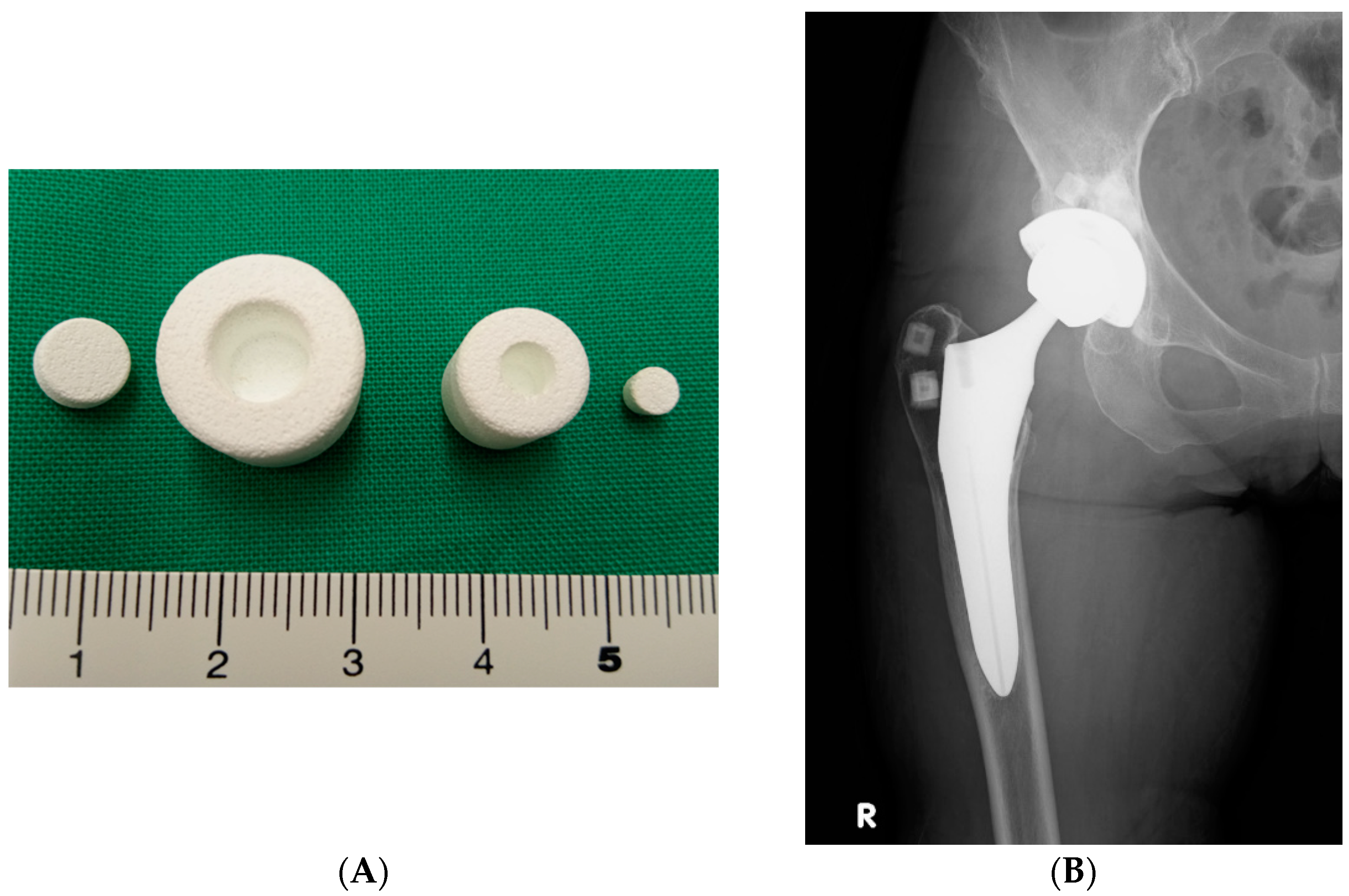
2.2. Surgery
2.3. Antibiotherapy
2.4. Functional Outcomes
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Evaluation of Outcomes
4.3. Success Criterion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kirkpatrick, D.K.; Trachtenberg, L.S.; Mangino, P.D.; Von Fraunhofer, J.A.; Seligson, D. In vitro characteristics of tobramycin-PMMA beads: Comprehensive strength and leaching. Orthopedics 1985, 8, 1130–1133. [Google Scholar] [CrossRef] [PubMed]
- Cerretani, D.; Giorgi, G.; Fornara, P.; Bocchi, L.; Neri, L.; Ceffa, R.; Ghisellini, F.; Ritter, M.A. The in vitro elution characteristics of vancomycin combined with imipenem-cilastatin in acrylic bone-cements. J. Arthroplast. 2002, 17, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Bozic, K.J.; Ries, M.D. The impact of infection after total hip arthroplasty on hospital and surgeon resource utilization. J. Bone Jt. Surg. 2005, 87, 1746–1751. [Google Scholar] [CrossRef]
- Klouche, S.; Sariali, E.; Mamoudy, P. Total hip arthroplasty revision due to infection: A cost analysis approach. Orthop. Traumatol. Surg. Res. 2010, 96, 124–132. [Google Scholar] [CrossRef]
- Fisman, D.N.; Reilly, D.T.; Karchmer, A.W.; Goldie, S.J. Clinical Effectiveness and Cost-Effectiveness of 2 Management Strategies for Infected Total Hip Arthroplasty in the Elderly. Clin. Infect. Dis. 2001, 32, 419–430. [Google Scholar] [CrossRef]
- Hrynyshyn, A.; Simões, M.; Borges, A. Biofilms in Surgical Site Infections: Recent Advances and Novel Prevention and Eradication Strategies. Antibiotics 2022, 11, 69. [Google Scholar] [CrossRef]
- Shinto, Y.; Uchida, A.; Korkusuz, F.; Araki, N.; Ono, K. Calcium hydroxyapatite ceramic used as a delivery system for antibi-otics. J. Bone Jt. Surg. Br. 1992, 74, 600–604. [Google Scholar] [CrossRef]
- Uchida, A.; Shinto, Y.; Araki, N.; Ono, K. Slow release of anticancer drugs from porous calcium hydroxyapatite ceramic. J. Orthop. Res. 1992, 10, 440–445. [Google Scholar] [CrossRef]
- Zimmerli, W.; Trampuz, A.; Ochsner, P.E. Prosthetic-Joint Infections. N. Engl. J. Med. 2004, 14, 1645–1654. [Google Scholar] [CrossRef]
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R. Infectious Diseases Society of America. Executive summary: Diagnosis and management of prosthetic joint infection: Clinical practice guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2013, 56, 1–10. [Google Scholar] [CrossRef]
- de Vries, L.; van der Weegen, W.; Neve, W.; Das, H.; Ridwan, B.; Steens, J. The Effectiveness of Debridement, Antibiotics and Irrigation for Periprosthetic Joint Infections after Primary Hip and Knee Arthroplasty. A 15 Years Retrospective Study in Two Community Hospitals in the Netherlands. J. Bone Jt. Infect. 2016, 7, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Zmistowski, B.; Karam, J.A.; Durinka, J.B.; Casper, D.S.; Parvizi, J. Periprosthetic Joint Infection Increases the Risk of One-Year Mortality. J. Bone Jt. Surg. 2013, 95, 2177–2184. [Google Scholar] [CrossRef] [PubMed]
- Natsuhara, K.M.; Shelton, T.J.; Meehan, J.P.; Lum, Z.C. Mortality During Total Hip Periprosthetic Joint Infection. J. Arthroplast. 2019, 34, S337–S342. [Google Scholar] [CrossRef] [PubMed]
- Berend, K.R.; Lombardi, A.V.; Morris, M.J.; Bergeson, A.G.; Adams, J.; Sneller, M.A. Two-stage Treatment of Hip Periprosthetic Joint Infection Is Associated With a High Rate of Infection Control but High Mortality. Clin. Orthop. Relat. Res. 2013, 471, 510–518. [Google Scholar] [CrossRef]
- Leonard, H.A.C.; Liddle, A.D.; Burke; Murray, D.W.; Pandit, H. Single- or Two-stage Revision for Infected Total Hip Arthroplasty? A Systematic Review of the Literature. Clin. Orthop. Relat. Res. 2014, 472, 1036–1042. [Google Scholar] [CrossRef]
- Shohat, N.; Goswami, K.; Tan, T.L.; Fillingham, Y.; Parvizi, J. Increased Failure After Irrigation and Debridement for Acute Hematogenous Periprosthetic Joint Infection. J. Bone Jt. Surg. Am. 2019, 17, 696–703. [Google Scholar] [CrossRef]
- Triantafyllopoulos, G.K.; Poultsides, L.A.; Sakellariou, V.I.; Zhang, W.; Sculco, P.K.; Ma, Y.; Sculco, T.P. Irrigation and debridement for periprosthetic infections of the hip and factors determining outcome. Int. Orthop. 2015, 39, 1203–1209. [Google Scholar] [CrossRef]
- Vilchez, F.; Martínez-Pastor, J.; García-Ramiro, S.; Bori, G.; Maculé, F.; Sierra, J.; Font, L.; Mensa, J.; Soriano, A. Outcome and predictors of treatment failure in early post-surgical prosthetic joint infections due to Staphylococcus aureus treated with debridement. Clin. Microbiol. Infect. 2011, 17, 439–444. [Google Scholar] [CrossRef]
- Odum, S.M.; Fehring, T.K.; Lombardi, A.V.; Zmistowski, B.M.; Brown, N.M.; Luna, J.T.; Fehring, K.A.; The Periprosthetic Infection Consortium. Periprosthetic Infection Consortium. Irrigation and debridement for periprosthetic infections: Does the organism matter? J. Arthroplast. 2011, 26 (Suppl. 6), 114–118. [Google Scholar] [CrossRef]
- Kuiper, J.W.; Vos, S.J.; Saouti, R.; Vergroesen, D.A.; Graat, H.C.; Debets-Ossenkopp, Y.J.; Peters EJ, G.; Nolte, P.A. Prosthetic joint-associated infections treated with DAIR (debridement, antibiotics, irrigation, and retention): Analysis of risk factors and local antibiotic carriers in 91 patients. Acta Orthop. 2013, 84, 380–386. [Google Scholar] [CrossRef]
- Weenders, S.G.M.; Nijhof, M.W.; Schimmel, J.J.P.; Goosen, J.H.M. Debridement, antibiotics and implant retention in early periprosthetic joint infection after primary total hip arthroplasty: 88 percent survival after two years follow-up. Acta Orthop. Belg. 2016, 82, 530–538. [Google Scholar] [PubMed]
- Lebeaux, D.; Ghigo, J.-M.; Beloin, C. Biofilm-Related Infections: Bridging the Gap between Clinical Management and Fundamental Aspects of Recalcitrance toward Antibiotics. Microbiol. Mol. Biol. Rev. 2014, 78, 510–543. [Google Scholar] [CrossRef] [PubMed]
- Davies, D. Understanding biofilm resistance to antibacterial agents. Nat. Rev. Drug Discov. 2003, 2, 114–122. [Google Scholar] [CrossRef]
- Roman, M.D.; Bocea, B.-A.; Ion, N.-I.; Vorovenci, A.E.; Dragomirescu, D.; Birlutiu, R.-M.; Birlutiu, V.; Fleaca, S.R. Are There Any Changes in the Causative Microorganisms Isolated in the Last Years from Hip and Knee Periprosthetic Joint Infections? Antimicrobial Susceptibility Test Results Analysis. Microorganisms 2023, 11, 116. [Google Scholar] [CrossRef]
- Bue, M.; Hanberg, P.; Koch, J.; Jensen, L.K.; Lundorff, M.; Aalbæk, B.; Jensen, H.E.; Søballe, K.; Tøttrup, M. Single-dose bone pharmacokinetics of vancomycin in a porcine implant-associated osteomyelitis model. J. Orthop. Res. 2018, 36, 1093–1098. [Google Scholar] [CrossRef] [PubMed]
- Byren, I.; Bejon, P.; Atkins, B.L.; Angus, B.; Masters, S.; McLardy-Smith, P.; Gundle, R.; Berendt, A. One hundred and twelve infected arthroplasties treated with ‘DAIR’ (debridement, antibiotics and implant retention): Antibiotic duration and outcome. J. Antimicrob. Chemother. 2009, 63, 1264–1271. [Google Scholar] [CrossRef] [PubMed]
- Katakam, A.; Melnic, C.M.; Bedair, H.S. Morbid Obesity Is a Risk Factor for Infection Recurrence Following Debridement, Antibiotics, and Implant Retention for Periprosthetic Joint Infection. J. Arthroplast. 2020, 35, 3710–3715. [Google Scholar] [CrossRef] [PubMed]
- Joseph, T.N.; Chen, A.L.; Di Cesare, P.E. Use of Antibiotic-Impregnated Cement in Total Joint Arthroplasty. J. Am. Acad. Orthop. Surg. 2003, 11, 38–47. [Google Scholar] [CrossRef]
- Sudo, A.; Hasegawa, M.; Fukuda, A.; Uchida, A. Treatment of Infected Hip Arthroplasty With Antibiotic-Impregnated Calcium Hydroxyapatite. J. Arthroplast. 2008, 23, 145–150. [Google Scholar] [CrossRef]
- Choe, H.; Inaba, Y.; Kobayashi, N.; Miyamae, Y.; Ike, H.; Saito, T. Clinical utility of antibiotic-loaded hydroxyapatite block for treatment of intractable periprosthetic joint infection and septic arthritis of the hip. Mod. Rheumatol. 2015, 25, 937–942. [Google Scholar] [CrossRef]
- Korkusuz, F.; Uchida, A.; Shinto, Y.; Araki, N.; Inoue, K.; Ono, K. Experimental implant-related osteomyelitis treated by antibiotic-calcium hydroxyapatite ceramic composites. J. Bone Jt. Surg. Br. 1993, 75, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Klouche, S.; Lhotellier, L.; Mamoudy, P. Infected total hip arthroplasty treated by an irrigation-debridement/component retention protocol. A prospective study in a 12-case series with minimum 2 years’ follow-up. Orthop. Traumatol. Surg. Res. 2011, 97, 134–138. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Case | Sex | Age | Diagnoses | Previous Surgery | Onset Symptom | Organism | Age of THA (Months) | The Time from Surgery to Onset Symptom | Antibiotics in the CHA Blocks (Numbers) | Antibiotics at Interim Period (Weeks) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 65 | ION | Hemi | Hip pain, fever | Escherichia coli | 112 | 8 months | CTM, AMK (5) | CTM, AMK (6) |
| 2 | M | 56 | ION | THA | Hip pain, fever | Streptococcus agalactiae | 8 | 3 months | FMOX (5) | FMOX, FOM, CTM, MINO, IPM/CS, PCG (5) |
| 3 | F | 62 | OA | THA | Chill | MRSA | 31 | 3 months | VCM (2) | ABK, GM (9) |
| 4 | F | 69 | FX | Hemi | Hip pain | Staphylococcus epidermidis | 1 | 1 month | VCM, CTM (5) | FOMX, ABK, AMK, VCM, TEIC (8) |
| 5 | F | 52 | OA | THA | Hip pain | Staphylococcus aureus | 12 | 2 months | IPM/CS, CTM(4) | ABPC, CLDM, PIPC, IPM/CS (6) |
| 6 | F | 71 | OA | THA | Fever, fistula | CNS | 1 | 2 weeks | VCM, AMK (3) | SBTPC, CTM, IPM/CS (8) |
| 7 | M | 57 | RA | THA | Hip pain | MSSA | 78 | 3 days | VCM (2) | CEZ, MEPM, TEIC (7) |
| 8 | M | 71 | RA | THA(rt) | Hip pain | MSSA | 43 | 2 weeks | VCM, FOM (3) | CEZ, PIPC, TEIC, LVFX, CLDM, RFP (6) |
| 8 | M | 71 | RA | THA(lt) | Hip pain | MSSA | 36 | 2 weeks | VCM, FOM (3) | CEZ, PIPC, TEIC, LVFX, CLDM, RFP (6) |
| 9 | F | 63 | OA | THA | Hip pain, fever, fistula | MSSA | 36 | 7 months | VCM, FOM (3) | CLDM, TEIC, VCM, RFP (7) |
| 10 | F | 74 | RA | THA | Swelling | E.coli | 84 | 6 months | VCM, FOM (3) | CEZ, MEPM, IPM/CS, RFP (6) |
| 11 | F | 68 | OA | THA | Hip pain, fistula | MSSA | 20 | 5 months | VCM, FOM (3) | CEZ, ABPC, ABPC/SBT, MINO, RFP (3) |
| 12 | F | 64 | RA | THA | Swelling | - | 48 | 3.5 weeks | VCM (3) | CEZ, LVFX(6) |
| 13 | F | 90 | OA | THA | Hip pain, fistula | Enterococcus faecalis | 57 | 2 weeks | VCM (2) | CEZ, LVFX(4) |
| Case | Reimplantation | Success/Failure | Treatment of Reinfection | Follow-up | Follow-up Periods after Treatment of PJI (Years) | Final JOA Score |
|---|---|---|---|---|---|---|
| 1 | I&D + exchange | Success | Died of other causes | 5.7 | ||
| 2 | I&D | Success | Died of other causes | 4.7 | ||
| 3 | I&D | Success | Regularly visits | 18.6 | 49 | |
| 4 | I&D + exchange | Failure (Reinfection) | two-stage revision | Regularly visits | 16.4 | 59 |
| 5 | I&D + exchange | Failure (Reinfection) | two-stage revision | Died of other causes | 12.5 | 46 |
| 6 | I&D + exchange | Success | Regularly visits | 11.6 | 42 | |
| 7 | I&D + exchange | Success | Regularly visits | 5.3 | 93 | |
| 8 | I&D + exchange | Success | Regularly visits | 9.0 | 77 | |
| 8 | I&D + exchange | Success | Regularly visits | 9.0 | 78 | |
| 9 | I&D + exchange with cup | Success | Regularly visits | 4.6 | 97 | |
| 10 | I&D + exchange | Success | Died of other causes | 4.0 | 93 | |
| 11 | I&D + exchange with cup/stem | Success | Regularly visits | 6.0 | 70 | |
| 12 | I&D + exchange | Success | Regularly visits | 3.0 | 77 | |
| 13 | I&D + exchange | Success | Regularly visits | 2.9 | 51 |
| Male 5 Hips (4 Patients) Female 9 Hips | |
|---|---|
| Osteoarthritis (OA) | 6 hips |
| Rheumatoid arthritis (RA) | 5 hips (4 patients) |
| Idiopathic osteonecrosis of the femoral head (ION) | 2 hips |
| Neck of femur fracture (FX) | 1 hip |
| Follow-up periods after treatment of PJI | Average 8.1 years (2.9~18.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wakabayashi, H.; Hasegawa, M.; Naito, Y.; Tone, S.; Sudo, A. Outcome of Irrigation and Debridement with Topical Antibiotic Delivery Using Antibiotic-Impregnated Calcium Hydroxyapatite for the Management of Periprosthetic Hip Joint Infection. Antibiotics 2023, 12, 938. https://doi.org/10.3390/antibiotics12050938
Wakabayashi H, Hasegawa M, Naito Y, Tone S, Sudo A. Outcome of Irrigation and Debridement with Topical Antibiotic Delivery Using Antibiotic-Impregnated Calcium Hydroxyapatite for the Management of Periprosthetic Hip Joint Infection. Antibiotics. 2023; 12(5):938. https://doi.org/10.3390/antibiotics12050938
Chicago/Turabian StyleWakabayashi, Hiroki, Masahiro Hasegawa, Yohei Naito, Shine Tone, and Akihiro Sudo. 2023. "Outcome of Irrigation and Debridement with Topical Antibiotic Delivery Using Antibiotic-Impregnated Calcium Hydroxyapatite for the Management of Periprosthetic Hip Joint Infection" Antibiotics 12, no. 5: 938. https://doi.org/10.3390/antibiotics12050938