
β-Lactam Pharmacokinetic/Pharmacodynamic Target Attainment in Intensive Care Unit Patients: A Prospective, Observational, Cohort Study
 , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. Demographic and Clinical Data
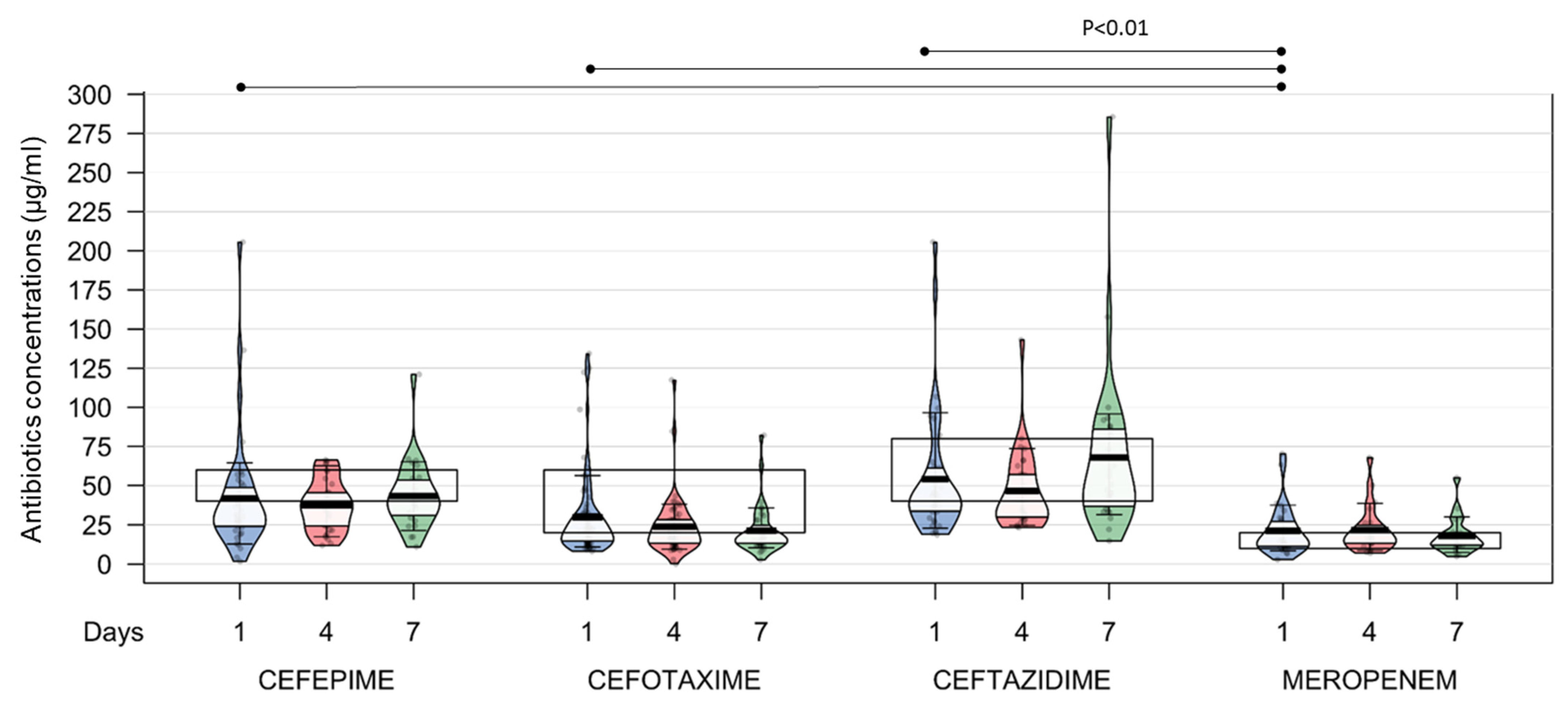
2.2. Target Attainment at D1, D4, and D7
2.3. Covariates Associated with Target Attainment
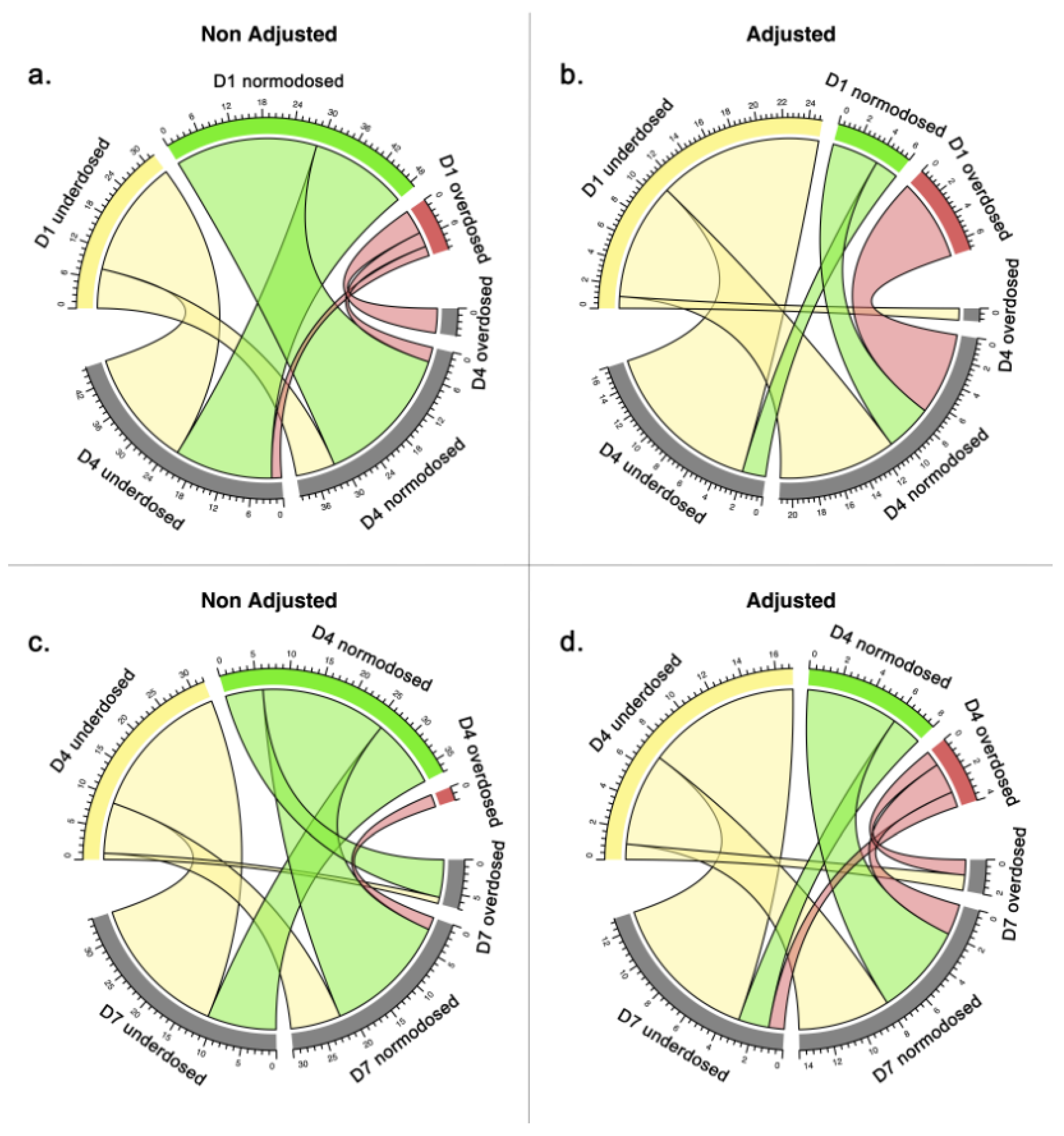
2.4. Impact of Dosage Adjustment on Target Attainment
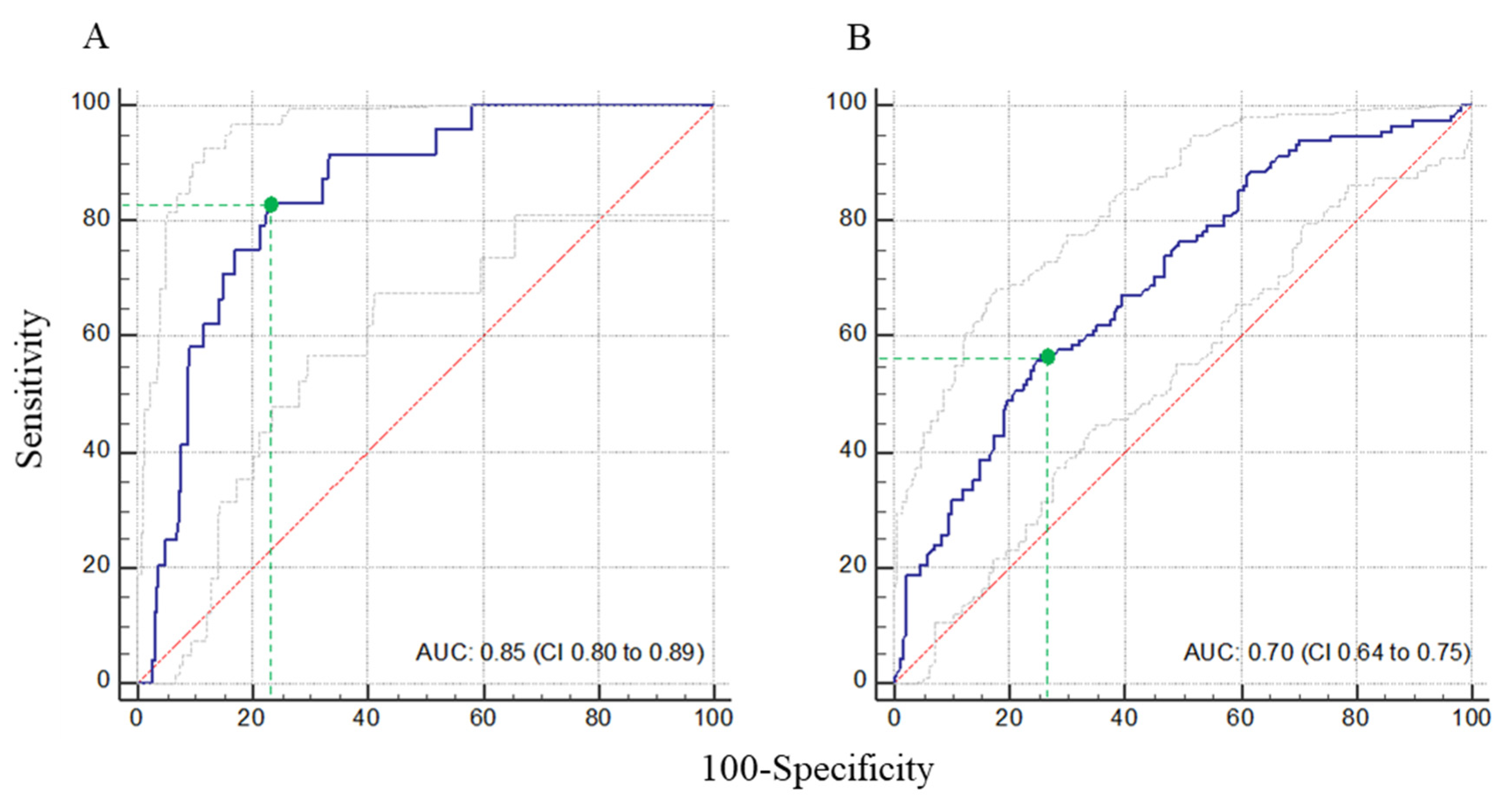
2.5. Impact on Target Non-Attainment on Clinical Outcomes
3. Discussion
4. Patients and Methods
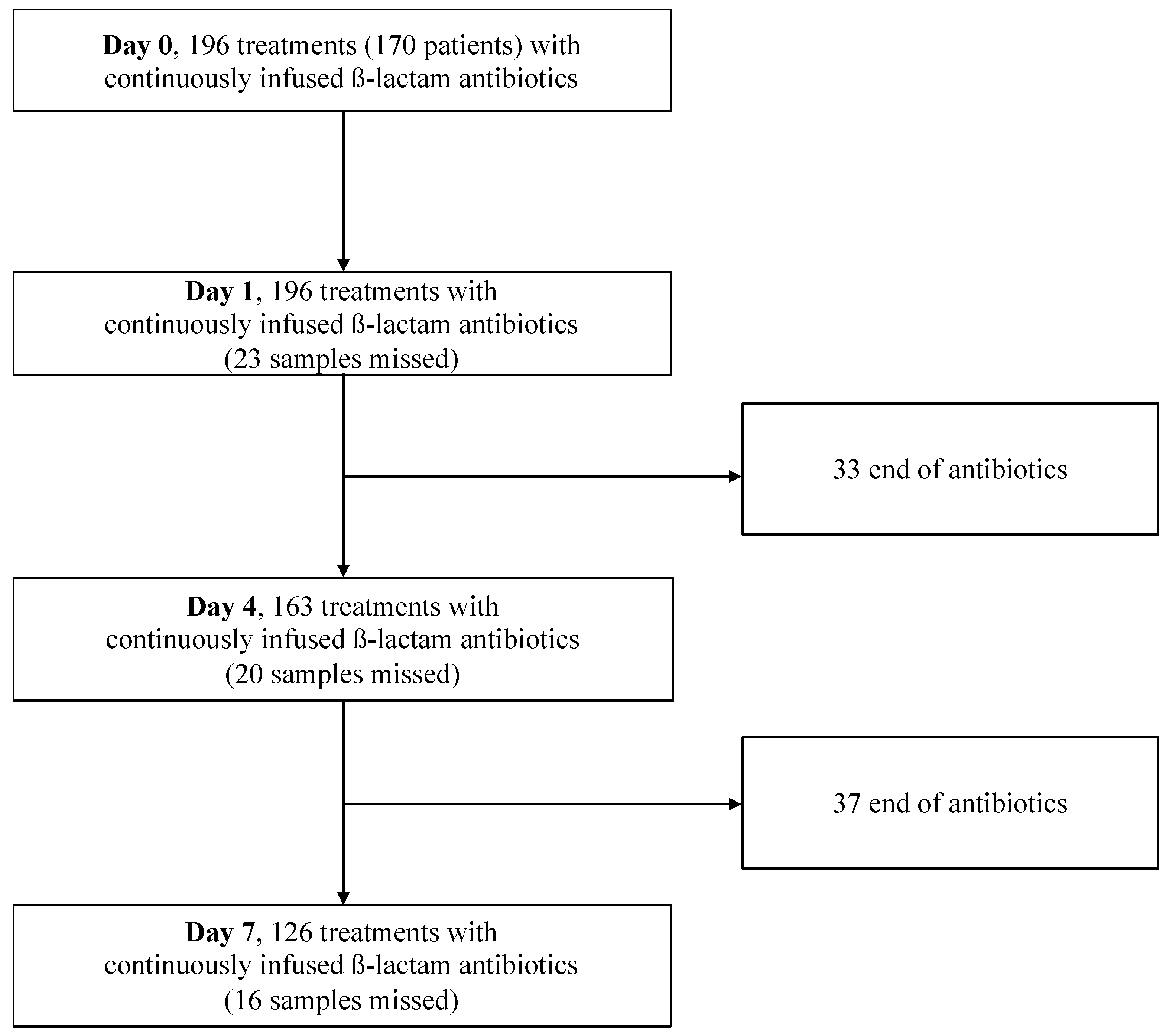
4.1. Study Design
4.2. Target Attainment and Therapeutic Drug Monitoring (TDM)
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Surveillance de la Consommation des Antibiotiques. Réseau ATB-Raisin. Résultats 2015. Available online: https://www.santepubliquefrance.fr/maladies-et-traumatismes/infections-associees-aux-soins-et-resistance-aux-antibiotiques/resistance-aux-antibiotiques/documents/rapport-synthese/surveillance-de-la-consommation-des-antibiotiques.-reseau-atb-raisin.-resultats-2015 (accessed on 18 September 2020).
- Blot, S.I.; Pea, F.; Lipman, J. The effect of pathophysiology on pharmacokinetics in the critically ill patient--concepts appraised by the example of antimicrobial agents. Adv. Drug Deliv. Rev. 2014, 77, 3–11. [Google Scholar] [CrossRef]
- Pea, F.; Viale, P.; Pavan, F.; Furlanut, M. Pharmacokinetic considerations for antimicrobial therapy in patients receiving renal replacement therapy. Clin. Pharmacokinet. 2007, 46, 997–1038. [Google Scholar] [CrossRef]
- Taccone, F.S.; Laterre, P.-F.; Dugernier, T.; Spapen, H.; Delattre, I.; Wittebole, X.; De Backer, D.; Layeux, B.; Wallemacq, P.; Vincent, J.-L.; et al. Insufficient β-lactam concentrations in the early phase of severe sepsis and septic shock. Crit. Care 2010, 14, R126. [Google Scholar] [CrossRef] [Green Version]
- Gonçalves-Pereira, J.; Póvoa, P. Antibiotics in critically ill patients: A systematic review of the pharmacokinetics of β-lactams. Crit. Care 2011, 15, R206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, A.; Roberts, D.; Wood, K.E.; Light, B.; Parrillo, J.E.; Sharma, S.; Suppes, R.; Feinstein, D.; Zanotti, S.; Taiberg, L.; et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit. Care Med. 2006, 34, 1589–1596. [Google Scholar] [CrossRef] [PubMed]
- Iregui, M.; Ward, S.; Sherman, G.; Fraser, V.J.; Kollef, M.H. Clinical importance of delays in the initiation of appropriate antibiotic treatment for ventilator-associated pneumonia. Chest 2002, 122, 262–268. [Google Scholar] [CrossRef] [Green Version]
- Leone, M.; Bourgoin, A.; Cambon, S.; Dubuc, M.; Albanèse, J.; Martin, C. Empirical antimicrobial therapy of septic shock patients: Adequacy and impact on the outcome. Crit. Care Med. 2003, 31, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Guilhaumou, R.; Benaboud, S.; Bennis, Y.; Dahyot-Fizelier, C.; Dailly, E.; Gandia, P.; Goutelle, S.; Lefeuvre, S.; Mongardon, N.; Roger, C.; et al. Optimization of the treatment with beta-lactam antibiotics in critically ill patients-guidelines from the French Society of Pharmacology and Therapeutics (Société Française de Pharmacologie et Thérapeutique-SFPT) and the French Society of Anaesthesia and Intensive Care Medicine (Société Française d’Anesthésie et Réanimation-SFAR). Crit. Care 2019, 23, 104. [Google Scholar] [PubMed] [Green Version]
- Roberts, J.A.; Abdul-Aziz, M.-H.; Davis, J.S.; Dulhunty, J.M.; Cotta, M.O.; Myburgh, J.; Bellomo, R.; Lipman, J. Continuous versus Intermittent β-Lactam Infusion in Severe Sepsis. A Meta-analysis of Individual Patient Data from Randomized Trials. Am. J. Respir. Crit. Care Med. 2016, 194, 681–691. [Google Scholar] [CrossRef]
- Lal, A.; Jaoude, P.; El-Solh, A.A. Prolonged versus Intermittent Infusion of β-Lactams for the Treatment of Nosocomial Pneumonia: A Meta-Analysis. Infect. Chemother. 2016, 48, 81–90. [Google Scholar] [CrossRef]
- Lee, Y.R.; Miller, P.D.; Alzghari, S.K.; Blanco, D.D.; Hager, J.D.; Kuntz, K.S. Continuous Infusion Versus Intermittent Bolus of Beta-Lactams in Critically Ill Patients with Respiratory Infections: A Systematic Review and Meta-analysis. Eur. J. Drug Metab. Pharmacokinet. 2018, 43, 155–170. [Google Scholar] [CrossRef]
- Saito, J.; Shoji, K.; Oho, Y.; Kato, H.; Matsumoto, S.; Aoki, S.; Nakamura, H.; Ogawa, T.; Hasegawa, M.; Yamatani, A.; et al. Population Pharmacokinetics and Pharmacodynamics of Meropenem in Critically Ill Pediatric Patients. Antimicrob. Agents Chemother. 2020, 65, e01909-20. Available online: https://aac.asm.org/content/65/2/e01909-20 (accessed on 1 April 2021). [CrossRef]
- Gatti, M.; Tedeschi, S.; Trapani, F.; Ramirez, S.; Mancini, R.; Giannella, M.; Viale, P.; Pea, F. A Proof of Concept of the Usefulness of a TDM-Guided Strategy for Optimizing Pharmacokinetic/Pharmacodynamic Target of Continuous Infusion Ampicillin-Based Regimens in a Case Series of Patients with Enterococcal Bloodstream Infections and/or Endocarditis. Antibiotics 2022, 11, 1037. [Google Scholar] [CrossRef] [PubMed]
- Hyun, D.G.; Seo, J.; Lee, S.Y.; Ahn, J.H.; Hong, S.B.; Lim, C.M.; Koh, Y.; Huh, J.W. Continuous Piperacillin-Tazobactam Infusion Improves Clinical Outcomes in Critically Ill Patients with Sepsis: A Retrospective, Single-Centre Study. Antibiotics 2022, 11, 1508. [Google Scholar] [CrossRef]
- Abdulla, A.; Ewoldt, T.M.J.; Purmer, I.M.; Muller, A.E.; Gommers, D.; Endeman, H.; Koch, B.C.P. A narrative review of predictors for β-lactam antibiotic exposure during empirical treatment in critically ill patients. Expert Opin. Drug Metab. Toxicol. 2021, 17, 359–368. [Google Scholar] [CrossRef] [PubMed]
- De Waele, J.J.; Carrette, S.; Carlier, M.; Stove, V.; Boelens, J.; Claeys, G.; Leroux-Roels, I.; Hoste, E.; Depuydt, P.; Decruyenaere, J.; et al. Therapeutic drug monitoring-based dose optimisation of piperacillin and meropenem: A randomised controlled trial. Intensive Care Med. 2014, 40, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Huttner, A.; Harbarth, S.; Hope, W.W.; Lipman, J.; Roberts, J.A. Therapeutic drug monitoring of the β-lactam antibiotics: What is the evidence and which patients should we be using it for? J. Antimicrob. Chemother. 2015, 70, 3178–3183. [Google Scholar] [CrossRef] [Green Version]
- Fournier, A.; Eggimann, P.; Pagani, J.-L.; Revelly, J.-P.; Decosterd, L.A.; Marchetti, O.; Pannatier, A.; Voirol, P.; Que, Y.-A. Impact of the introduction of real-time therapeutic drug monitoring on empirical doses of carbapenems in critically ill burn patients. Burns 2015, 41, 956–968. [Google Scholar] [CrossRef]
- Delannoy, M.; Agrinier, N.; Charmillon, A.; Degand, N.; Dellamonica, J.; Leone, M.; Pulcini, C.; Novy, E. Implementation of antibiotic stewardship programmes in French ICUs in 2018: A nationwide cross-sectional survey. J. Antimicrob. Chemother. 2019, 74, 2106–2114. [Google Scholar] [CrossRef]
- Dhaese, S.A.M.; Thooft, A.D.J.; Farkas, A.; Lipman, J.; Verstraete, A.G.; Stove, V.; Roberts, J.A.; De Waele, J.J. Early target attainment of continuous infusion piperacillin/tazobactam and meropenem in critically ill patients: A prospective observational study. J. Crit. Care 2019, 52, 75–79. [Google Scholar] [CrossRef]
- Abdulla, A.; Dijkstra, A.; Hunfeld, N.G.M.; Endeman, H.; Bahmany, S.; Ewoldt, T.M.J.; Muller, A.E.; Van Gelder, T.; Gommers, D.; Koch, B.C.P. Failure of target attainment of beta-lactam antibiotics in critically ill patients and associated risk factors: A two-center prospective study (EXPAT). Crit. Care 2020, 24, 558. [Google Scholar] [CrossRef]
- Payne, L.E.; Gagnon, D.J.; Riker, R.R.; Seder, D.B.; Glisic, E.K.; Morris, J.G.; Fraser, G.L. Cefepime-induced neurotoxicity: A systematic review. Crit. Care 2017, 21, 276. [Google Scholar] [CrossRef] [Green Version]
- Huwyler, T.; Lenggenhager, L.; Abbas, M.; Ing Lorenzini, K.; Hughes, S.; Huttner, B.; Karmime, A.; Uçkay, I.; von Dach, E.; Lescuyer, P.; et al. Cefepime plasma concentrations and clinical toxicity: A retrospective cohort study. Clin. Microbiol. Infect. 2017, 23, 454–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klastrup, V.; Thorsted, A.; Storgaard, M.; Christensen, S.; Friberg, L.E.; Öbrink-Hansen, K. Population Pharmacokinetics of Piperacillin following Continuous Infusion in Critically Ill Patients and Impact of Renal Function on Target Attainment. Antimicrob. Agents Chemother. 2020, 64, e02556-19. Available online: https://aac.asm.org/content/64/7/e02556-19 (accessed on 1 April 2021). [CrossRef] [PubMed]
- Sangla, F.; Marti, P.E.; Verissimo, T.; Pugin, J.; de Seigneux, S.; Legouis, D. Measured and Estimated Glomerular Filtration Rate in the ICU: A Prospective Study. Crit. Care Med. 2020, 48, e1232–e1241. [Google Scholar] [CrossRef]
- Roberts, J.A.; Lipman, J. Pharmacokinetic issues for antibiotics in the critically ill patient. Crit. Care Med. 2009, 37, 840–851; quiz 859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zander, J.; Döbbeler, G.; Nagel, D.; Scharf, C.; Huseyn-Zada, M.; Jung, J.; Frey, L.; Vogeser, M.; Zoller, M. Variability of piperacillin concentrations in relation to tazobactam concentrations in critically ill patients. Int. J. Antimicrob. Agents 2016, 48, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Aziz, M.H.; Alffenaar, J.-W.C.; Bassetti, M.; Bracht, H.; Dimopoulos, G.; Marriott, D.; Neely, M.N.; Paiva, J.-A.; Pea, F.; Sjovall, F.; et al. Antimicrobial therapeutic drug monitoring in critically ill adult patients: A Position Paper. Intensive Care Med. 2020, 46, 1127–1153. [Google Scholar] [CrossRef]
- Roberts, J.A.; Hope, W.W.; Lipman, J. Therapeutic drug monitoring of beta-lactams for critically ill patients: Unwarranted or essential? Int. J. Antimicrob. Agents 2010, 35, 419–420. [Google Scholar] [CrossRef]
- Jacobs, A.; Taccone, F.S.; Roberts, J.A.; Jacobs, F.; Cotton, F.; Wolff, F.; Creteur, J.; Vincent, J.-L.; Hites, M. β-Lactam Dosage Regimens in Septic Patients with Augmented Renal Clearance. Antimicrob. Agents Chemother. 2018, 62, e02534-17. Available online: https://aac.asm.org/content/62/9/e02534-17 (accessed on 1 April 2021). [CrossRef] [Green Version]
- Al-Shaer, M.H.; Rubido, E.; Cherabuddi, K.; Venugopalan, V.; Klinker, K.; Peloquin, C. Early therapeutic monitoring of β-lactams and associated therapy outcomes in critically ill patients. J. Antimicrob. Chemother. 2020, 75, 3644–3651. [Google Scholar] [CrossRef] [PubMed]
- Economou, C.J.P.; Wong, G.; McWhinney, B.; Ungerer, J.P.J.; Lipman, J.; Roberts, J.A. Impact of β-lactam antibiotic therapeutic drug monitoring on dose adjustments in critically ill patients undergoing continuous renal replacement therapy. Int. J. Antimicrob. Agents 2017, 49, 589–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, B.M.; Paratz, J.; See, N.C.; Muller, M.J.; Rudd, M.; Paterson, D.; Briscoe, S.E.M.; Ungerer, J.F.; McWhinney, B.C.M.; Lipman, J.M.; et al. Therapeutic drug monitoring of beta-lactam antibiotics in burns patients—A one-year prospective study. Ther. Drug Monit. 2012, 34, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Blondiaux, N.; Wallet, F.; Favory, R.; Onimus, T.; Nseir, S.; Courcol, R.J.; Durocher, A.; Roussel-Delvallez, M. Daily serum piperacillin monitoring is advisable in critically ill patients. Int. J. Antimicrob. Agents 2010, 35, 500–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdulla, A.; Ewoldt, T.M.J.; Hunfeld, N.G.M.; Muller, A.E.; Rietdijk, W.J.R.; Polinder, S.; van Gelder, T.; Endeman, H.; Koch, B.C.P. The effect of therapeutic drug monitoring of beta-lactam and fluoroquinolones on clinical outcome in critically ill patients: The DOLPHIN trial protocol of a multi-centre randomised controlled trial. BMC Infect. Dis. 2020, 20, 57. Available online: https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-020-4781-x (accessed on 1 April 2021). [CrossRef]
- Mangalore, R.P.; Ashok, A.; Lee, S.J.; Romero, L.; Peel, T.N.; Udy, A.A.; Peleg, A.Y. Beta-Lactam Antibiotic Therapeutic Drug Monitoring in Critically Ill Patients: A Systematic Review and Meta-Analysis. Clin. Infect. Dis. 2022, 75, 1848–1860. [Google Scholar] [CrossRef]
- Toulouse, E.; Lafont, B.; Granier, S.; Mcgurk, G.; Bazin, J.E. French legal approach to patient consent in clinical research. Anaesth. Crit. Care Pain Med. 2020, 39, 883–885. [Google Scholar] [CrossRef]
- Longuet, P.; Lecapitaine, A.L.; Cassard, B.; Batista, R.; Gauzit, R.; Lesprit, P.; Haddad, R.; Vanjak, D.; Diamantis, S. Preparing and administering injectable antibiotics: How to avoid playing God. Med. Mal. Infect. 2016, 46, 242–268. [Google Scholar] [CrossRef]
- Beumier, M.; Casu, G.S.; Hites, M.; Wolff, F.; Cotton, F.; Vincent, J.L.; Jacobs, F.; Taccone, F.S. Elevated β-lactam concentrations associated with neurological deterioration in ICU septic patients. Minerva Anestesiol. 2015, 81, 497–506. [Google Scholar]
- Verdier, M.-C.; Tribut, O.; Tattevin, P.; Le Tulzo, Y.; Michelet, C.; Bentué-Ferrer, D. Simultaneous Determination of 12 β-Lactam Antibiotics in Human Plasma by High-Performance Liquid Chromatography with UV Detection: Application to Therapeutic Drug Monitoring. Antimicrob. Agents Chemother. 2011, 55, 4873–4879. [Google Scholar] [CrossRef] [Green Version]
- EMA. Guideline-Bioanalytical-Method-Validation. Available online: https://wwwemaeuropaeu/en/documents/scientificguideline/guideline-bioanalytical-method-validation (accessed on 31 September 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics (n = 170) | |
| Age in years, median (IQR) | 56.0 (53.6–58.4) |
| Male, n (%) | 110 (64.7) |
| Weight in kg, mean ± SD | 75 ± 19 |
| Height in cm, median (IQR) | 170 (165–178) |
| Body surface area in m2, median (IQR) | 1.9 (1.7–2.0) |
| Body mass index in kg/m2, median (IQR) | 25.4 (22.0–27.8) |
| Severity scores | |
| SAPS-2 score at ICU admission, median (IQR) | 39 (38.5–51) |
| Modified SOFA score at day 1, median (IQR) | 4 (2–5) |
| Renal replacement therapy, n (%) | 12 (6) |
| Extra corporeal life support, n (%) | 6 (3) |
| Biological data at day 0 (n = 196), median (IQR) | |
| Hematocrit in % | 29 (26–34) |
| Serum albumin in g/L | 29 (25–33) |
| Serum creatinine in μmol/L | 65 (48–104) |
| Indexed creatinine clearance in mL/min/1.73 m2 | 71.4 (31.5–111.0) |
| Infection (n = 196) | |
| Documented, n (%) | 136 (69.4) |
| Respiratory tract | 70 (51.5) |
| Primary bacteremia | 35 (25.7) |
| Urinary tract | 21 (15.5) |
| Intra-abdominal | 1 (0.7) |
| Central nervous system | 3 (2.2) |
| Other sites | 6 (4.4) |
| Not documented, n (%) | 60 (30.6) |
| Antibiotic treatments (n = 196) | |
| Empirical treatment, n (%) | |
| Cefotaxime | 80 (40.8) |
| Cefepime | 45 (23.0) |
| Ceftazidime | 41 (20.9) |
| Meropenem | 30 (15.3) |
| Duration of antibiotic therapy in days, median (IQR) | 7 (5–10) |
| Outcome (n = 170) | |
| Length of ICU stay in days, median (IQR) | 33 (17–67) |
| Alive at day 28, n (%) | 143 (84.1) |
| Patient Target Attainment (%) | |||||||
|---|---|---|---|---|---|---|---|
| Day 1 | n | Day 4 | n | Day 7 | n | ||
| Cefepime | underdosed | 66 | 38 | 62 | 34 | 52 | 27 |
| normodosed | 24 | 38 | 44 | ||||
| overdosed | 10 | - | 4 | ||||
| Cefotaxime | underdosed | 43 | 69 | 51 | 56 | 71 | 36 |
| normodosed | 51 | 45 | 26 | ||||
| overdosed | 6 | 4 | 3 | ||||
| Ceftazidime | underdosed | 47 | 37 | 48 | 30 | 30 | 27 |
| normodosed | 42 | 48 | 59 | ||||
| overdosed | 11 | 4 | 11 | ||||
| Meropenem | underdosed | 14 | 29 | 17 | 23 | 20 | 20 |
| normodosed | 57 | 57 | 60 | ||||
| overdosed | 29 | 26 | 20 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guilhaumou, R.; Chevrier, C.; Setti, J.L.; Jouve, E.; Marsot, A.; Julian, N.; Blin, O.; Simeone, P.; Lagier, D.; Mokart, D.; et al. β-Lactam Pharmacokinetic/Pharmacodynamic Target Attainment in Intensive Care Unit Patients: A Prospective, Observational, Cohort Study. Antibiotics 2023, 12, 1289. https://doi.org/10.3390/antibiotics12081289
Guilhaumou R, Chevrier C, Setti JL, Jouve E, Marsot A, Julian N, Blin O, Simeone P, Lagier D, Mokart D, et al. β-Lactam Pharmacokinetic/Pharmacodynamic Target Attainment in Intensive Care Unit Patients: A Prospective, Observational, Cohort Study. Antibiotics. 2023; 12(8):1289. https://doi.org/10.3390/antibiotics12081289
Chicago/Turabian StyleGuilhaumou, Romain, Constance Chevrier, Jean Loup Setti, Elisabeth Jouve, Amélie Marsot, Nathan Julian, Olivier Blin, Pierre Simeone, David Lagier, Djamel Mokart, and et al. 2023. "β-Lactam Pharmacokinetic/Pharmacodynamic Target Attainment in Intensive Care Unit Patients: A Prospective, Observational, Cohort Study" Antibiotics 12, no. 8: 1289. https://doi.org/10.3390/antibiotics12081289