
Predictors of Mortality in Patients with Infections Due to Carbapenem-Resistant Gram-Negative Bacteria

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AMR | antimicrobial resistance |
| CR | carbapenem-resistant |
| CRE | carbapenem-resistant Enterobacterales |
| CR-GNB | Gram-negative bacteria |
| eCIM | EDTA-modified carbapenem inactivation method |
| HR | hazard ratio |
| ICU | intensive care unit |
| IMV | invasive mechanical ventilation |
| IQR | interquartile range |
| MALDI-TOF | matrix-assisted laser desorption/ionisation time-of-flight |
| mCIM | modified carbapenem inactivation method |
| MDR | multidrug-resistant |
| PCR | polymerase chain reaction |
References
- Zhou, N.; Cheng, Z.; Zhang, X.; Lv, C.; Guo, C.; Liu, H.; Dong, K.; Zhang, Y.; Liu, C.; Chang, Y.; et al. Global Antimicrobial Resistance: A System-Wide Comprehensive Investigation Using the Global One Health Index. Infect. Dis. Poverty 2022, 11, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Nordmann, P.; Naas, T.; Poirel, L. Global Spread of Carbapenemase-Producing Enterobacteriaceae. Emerg. Infect. Dis. 2011, 17, 1791–1798. [Google Scholar] [CrossRef] [PubMed]
- Schwaber, M.J.; Carmeli, Y. Carbapenem-Resistant Enterobacteriaceae: A Potential Threat. JAMA 2008, 300, 2911–2913. [Google Scholar] [CrossRef]
- Martinez-Guerra, B.A.; Gonzalez-Lara, M.F.; De-Leon-Cividanes, N.A.; Tamez-Torres, K.M.; Roman-Montes, C.M.; Rajme-Lopez, S.; Villalobos-Zapata, G.I.; Lopez-Garcia, N.I.; Martínez-Gamboa, A.; Sifuentes-Osornio, J.; et al. Antimicrobial Resistance Patterns and Antibiotic Use during Hospital Conversion in the COVID-19 Pandemic. Antibiotics 2021, 10, 182. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Robles Aguilar, G.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global Burden of Bacterial Antimicrobial Resistance in 2019: A Systematic Analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Ben-David, D.; Kordevani, R.; Keller, N.; Tal, I.; Marzel, A.; Gal-Mor, O.; Maor, Y.; Rahav, G. Outcome of Carbapenem Resistant Klebsiella Pneumoniae Bloodstream Infections. Clin. Microbiol. Infect. 2012, 18, 54–60. [Google Scholar] [CrossRef] [Green Version]
- Fraenkel-Wandel, Y.; Raveh-Brawer, D.; Wiener-Well, Y.; Yinnon, A.M.; Assous, M.V. Mortality due to BlaKPC Klebsiella Pneumoniae Bacteraemia. J. Antimicrob. Chemother. 2016, 71, 1083–1087. [Google Scholar] [CrossRef] [Green Version]
- Bartsch, S.M.; McKinnell, J.A.; Mueller, L.E.; Miller, L.G.; Gohil, S.K.; Huang, S.S.; Lee, B.Y. Potential Economic Burden of Carbapenem-Resistant Enterobacteriaceae (CRE) in the United States. Clin. Microbiol. Infect. 2017, 23, 48.e9–48.e16. [Google Scholar] [CrossRef] [Green Version]
- McEwen, S.A.; Collignon, P.J. Antimicrobial Resistance: A One Health Perspective. Microbiol. Spectr. 2018, 6, 521–547. [Google Scholar] [CrossRef] [Green Version]
- Logan, L.K.; Weinstein, R.A. The Epidemiology of Carbapenem-Resistant Enterobacteriaceae: The Impact and Evolution of a Global Menace. J. Infect. Dis. 2017, 215, S28–S36. [Google Scholar] [CrossRef] [Green Version]
- Horan, T.C.; Andrus, M.; Dudeck, M.A. CDC/NHSN Surveillance Definition of Health Care-Associated Infection and Criteria for Specific Types of Infections in the Acute Care Setting. Am. J. Infect. Control 2008, 36, 309–332. [Google Scholar] [CrossRef]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing, 30th ed.; CLSI Supplement M100; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2020. [Google Scholar]
- Bogaerts, P.; Rezende de Castro, R.; de Mendonça, R.; Huang, T.-D.; Denis, O.; Glupczynski, Y. Validation of Carbapenemase and Extended-Spectrum β-Lactamase Multiplex Endpoint PCR Assays According to ISO 15189. J. Antimicrob. Chemother. 2013, 68, 1576–1582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riley, R.D.; Ensor, J.; Snell, K.I.E.; Harrell, F.E.; Martin, G.P.; Reitsma, J.B.; Moons, K.G.M.; Collins, G.; van Smeden, M. Calculating the Sample Size Required for Developing a Clinical Prediction Model. BMJ 2020, 368, m441. [Google Scholar] [CrossRef] [Green Version]
- Zhao, S.; Kennedy, S.; Perry, M.R.; Wilson, J.; Chase-Topping, M.; Anderson, E.; Woolhouse, M.E.J.; Lockhart, M. Epidemiology of and Risk Factors for Mortality Due to Carbapenemase-Producing Organisms (CPO) in Healthcare Facilities. J. Hosp. Infect. 2021, 110, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Gualtero, S.; Valderrama, S.; Valencia, M.; Rueda, D.; Munõz-Velandia, O.; Ariza, B.; Cortes, G.; Salgado, D.; Porras, Y.; Ninõ, A. Factors Associated with Mortality in Infections Caused by Carbapenem-Resistant Enterobacteriaceae. J. Infect. Dev. Ctries. 2020, 14, 654–659. [Google Scholar] [CrossRef] [PubMed]
- Bar-Yoseph, H.; Cohen, N.; Korytny, A.; Andrawus, E.R.; Even Dar, R.; Geffen, Y.; Hussein, K.; Paul, M. Risk Factors for Mortality among Carbapenem-Resistant Enterobacteriaceae Carriers with Focus on Immunosuppression. J. Infect. 2019, 78, 101–105. [Google Scholar] [CrossRef]
- Zheng, Y.L.; Wan, Y.F.; Zhou, L.Y.; Ye, M.L.; Liu, S.; Xu, C.Q.; He, Y.Q.; Chen, J.H. Risk Factors and Mortality of Patients with Nosocomial Carbapenem-Resistant Acinetobacter Baumannii Pneumonia. Am. J. Infect. Control 2013, 41, e59–e63. [Google Scholar] [CrossRef]
- Lemos, E.V.; de la Hoz, F.P.; Einarson, T.R.; Mcghan, W.F.; Quevedo, E.; Castañeda, C.; Kawai, K. Carbapenem Resistance and Mortality in Patients with Acinetobacter Baumannii Infection: Systematic Review and Meta-Analysis. Clin. Microbiol. Infect. 2014, 20, 416–423. [Google Scholar] [CrossRef] [Green Version]
- Cienfuegos-Gallet, A.V.; Ocampo De Los Ríos, A.M.; Sierra Viana, P.; Ramirez Brinez, F.; Restrepo Castro, C.; Roncancio Villamil, G.; Del Corral Londoño, H.; Jiménez, J.N. Risk Factors and Survival of Patients Infected with Carbapenem-Resistant Klebsiella Pneumoniae in a KPC Endemic Setting: A Case-Control and Cohort Study. BMC Infect. Dis. 2019, 19, 830. [Google Scholar] [CrossRef] [Green Version]
- Kohler, P.P.; Volling, C.; Green, K.; Uleryk, E.M.; Shah, P.S.; McGeer, A. Carbapenem Resistance, Initial Antibiotic Therapy, and Mortality in Klebsiella Pneumoniae Bacteremia: A Systematic Review and Meta-Analysis. Infect. Control. Hosp. Epidemiol. 2017, 38, 1319–1328. [Google Scholar] [CrossRef] [Green Version]
- Van Duin, D.; Lok, J.J.; Earley, M.; Cober, E.; Richter, S.S.; Perez, F.; Salata, R.A.; Kalayjian, R.C.; Watkins, R.R.; Doi, Y.; et al. Colistin Versus Ceftazidime-Avibactam in the Treatment of Infections Due to Carbapenem-Resistant Enterobacteriaceae. Clin. Infect. Dis. 2018, 66, 163–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassetti, M.; Echols, R.; Matsunaga, Y.; Ariyasu, M.; Doi, Y.; Ferrer, R.; Lodise, T.P.; Naas, T.; Niki, Y.; Paterson, D.L.; et al. Efficacy and Safety of Cefiderocol or Best Available Therapy for the Treatment of Serious Infections Caused by Carbapenem-Resistant Gram-Negative Bacteria (CREDIBLE-CR): A Randomised, Open-Label, Multicentre, Pathogen-Focused, Descriptive, Phase 3 Trial. Lancet Infect. Dis. 2021, 21, 226–240. [Google Scholar] [CrossRef] [PubMed]
- Wunderink, R.G.; Giamarellos-Bourboulis, E.J.; Rahav, G.; Mathers, A.J.; Bassetti, M.; Vazquez, J.; Cornely, O.A.; Solomkin, J.; Bhowmick, T.; Bishara, J.; et al. Effect and Safety of Meropenem-Vaborbactam versus Best-Available Therapy in Patients with Carbapenem-Resistant Enterobacteriaceae Infections: The TANGO II Randomized Clinical Trial. Infect. Dis. Ther. 2018, 7, 439–455. [Google Scholar] [CrossRef] [Green Version]
- Paul, M.; Daikos, G.L.; Durante-Mangoni, E.; Yahav, D.; Carmeli, Y.; Benattar, Y.D.; Skiada, A.; Andini, R.; Eliakim-Raz, N.; Nutman, A.; et al. Colistin Alone versus Colistin plus Meropenem for Treatment of Severe Infections Caused by Carbapenem-Resistant Gram-Negative Bacteria: An Open-Label, Randomised Controlled Trial. Lancet Infect. Dis. 2018, 18, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Li, X.; Li, W.; Du, X.; He, J.Q.; Tao, C.; Feng, Y. Influence of Carbapenem Resistance on Mortality of Patients with Pseudomonas Aeruginosa Infection: A Meta-Analysis. Sci. Rep. 2015, 5, 11715. [Google Scholar] [CrossRef] [Green Version]
- Poston, J.T.; Koyner, J.L. Sepsis Associated Acute Kidney Injury. BMJ 2019, 364, k4891. [Google Scholar] [CrossRef]
- Khairoun, M.; Uffen, J.W.; Ocak, G.; Koopsen, R.; Haitjema, S.; Oosterheert, J.J.; Kaasjager, K. The Incidence, Mortality and Renal Outcomes of Acute Kidney Injury in Patients with Suspected Infection at the Emergency Department. PLoS ONE 2021, 16, e0260942. [Google Scholar] [CrossRef]
- Kadri, S.S.; Adjemian, J.; Lai, Y.L.; Spaulding, A.B.; Ricotta, E.; Rebecca Prevots, D.; Palmore, T.N.; Rhee, C.; Klompas, M.; Dekker, J.P.; et al. Difficult-to-Treat Resistance in Gram-Negative Bacteremia at 173 US Hospitals: Retrospective Cohort Analysis of Prevalence, Predictors, and Outcome of Resistance to All First-Line Agents. Clin. Infect. Dis. 2018, 67, 1803–1814. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
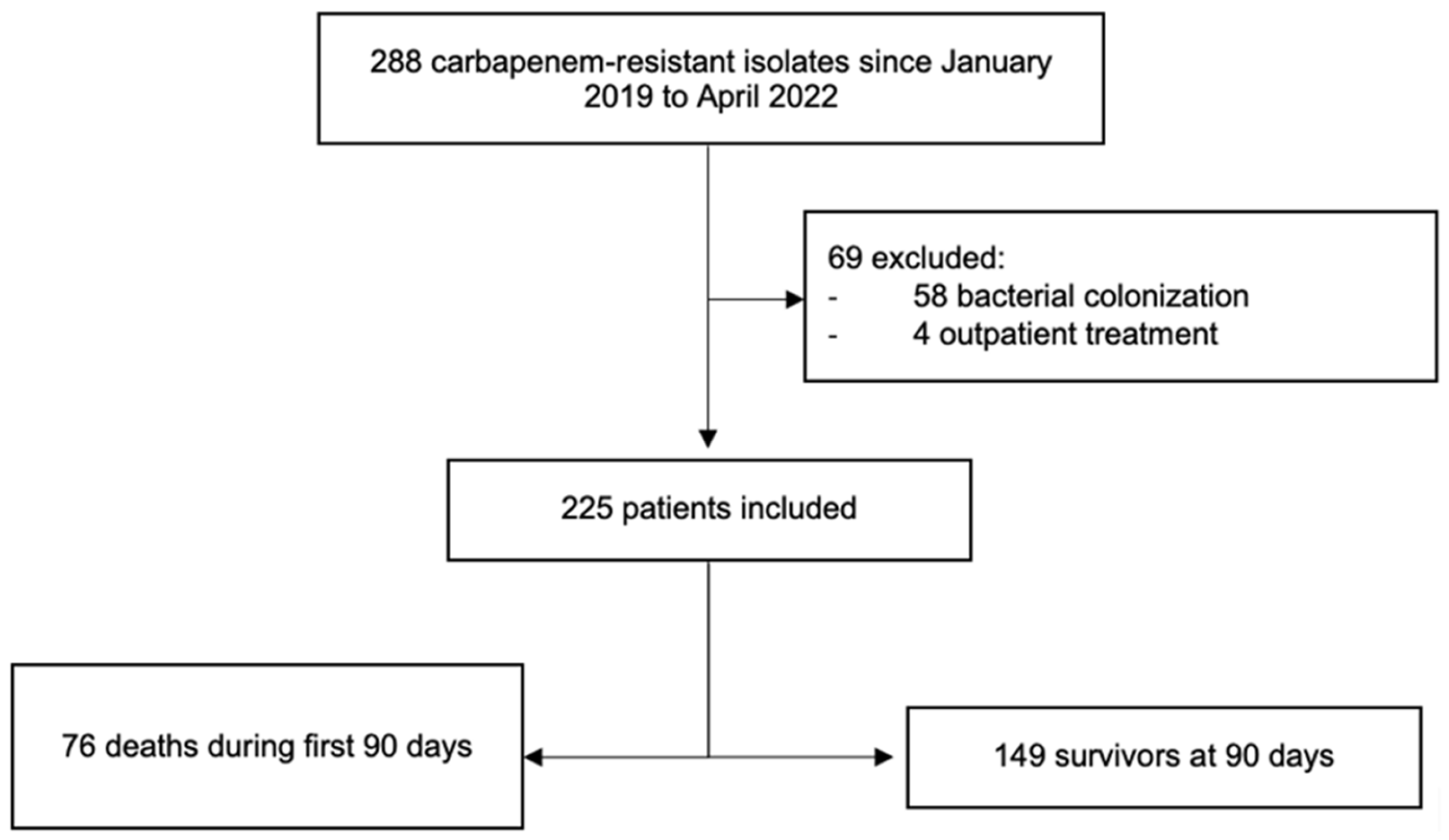
| Variable | Total n = 225 (100%) | Deaths at 90 Days n = 76 (33.8%) | Survivors at 90 Days n = 149 (66.2%) | p |
|---|---|---|---|---|
| Male, n (%) | 145 (64.4) | 53 (69.7) | 92 (61.7) | 0.236 |
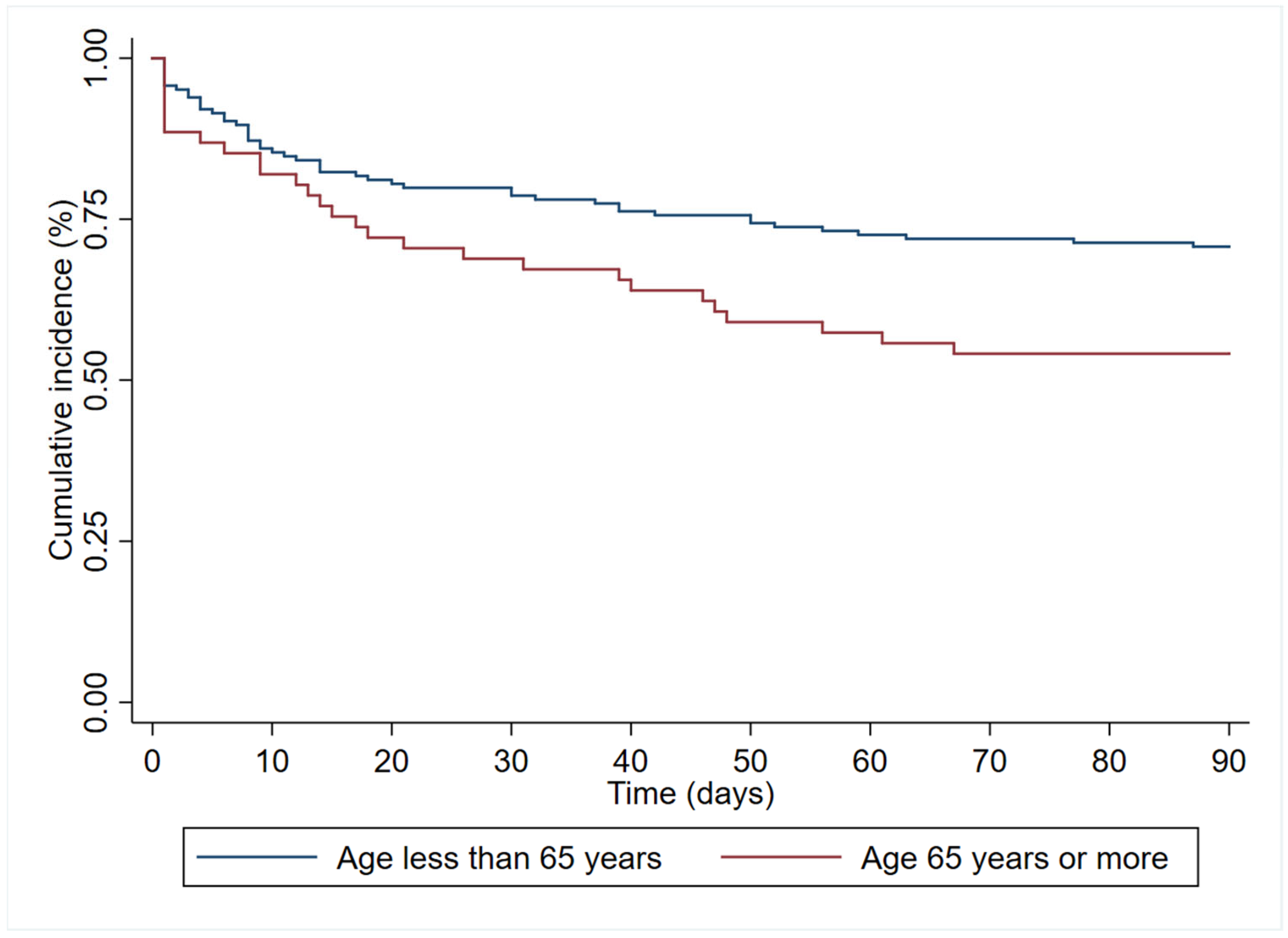
| Age—yr, median (IQR) | 54 (40–66) | 60 (47–70) | 52 (38–63) | 0.0055 |
| Days from admission to diagnosis, median (IQR) | 13 (4–28) | 17 (5–32) | 12 (4–27) | 0.3421 |
| Admission diagnosis, n (%) | 0.468 | |||
| Bacterial infection | 125 (55.6) | 42 (55.3) | 83 (55.7) | |
| COVID-19 | 45 (20.0) | 13 (17.1) | 32 (21.5) | |
| Neoplasm | 24 (10.7) | 12 (15.8) | 12 (8.1) | |
| Elective surgery | 18 (8.0) | 4 (5.3) | 14 (9.4) | |
| Urgent surgery | 8 (3.6) | 3 (4.0) | 5 (3.4) | |
| Other | 5 (2.2) | 2 (2.6) | 3 (2.1) | |
| Patient location at diagnosis, n (%) | ||||
| ICU | 81 (36.0) | 37 (48.7) | 44 (29.5) | 0.005 |
| Hospital ward | 144 (64.0) | 39 (51.3) | 105 (70.5) | |
| Type of CR-GNB infection, n (%) | ||||
| Bloodstream infection | 19 (8.4) | 8 (10.5) | 11 (7.4) | 0.422 |
| Respiratory tract infection | 88 (39.1) | 39 (51.3) | 49 (32.9) | 0.007 |
| Intraabdominal infection | 85 (37.8) | 16 (21.1) | 69 (46.3) | <0.001 |
| Urinary tract infection | 28 (12.5) | 5 (6.6) | 23 (15.5) | 0.055 |
| Bone and soft tissues infections | 18 (8.0) | 10 (13.2) | 8 (5.4) | 0.042 |
| Others | 4 (1.8) | 0 (0) | 4 (2.7) | 0.303 |
| Secondary bacteraemia | 59 (26.2) | 18 (23.7) | 41 (31.5) | 0.536 |
| Comorbidities, n (%) | ||||
| Charlson index >3 | 88 (39.1) | 41 (54.0) | 47 (31.5) | 0.001 |
| COVID-19 | 56 (24.9) | 17 (22.4) | 39 (26.2) | 0.532 |
| Obesity | 50 (22.4) | 15 (19.7) | 35 (23.8) | 0.489 |
| Diabetes | 55 (24.4) | 20 (26.3) | 35 (23.5) | 0.641 |
| Heart disease | 45 (20) | 22 (29.0) | 23 (15.4) | 0.017 |
| Hypertension | 78 (34.7) | 29 (38.2) | 49 (32.9) | 0.432 |
| COPD | 5 (2.2) | 3 (4.0) | 2 (1.3) | 0.339 |
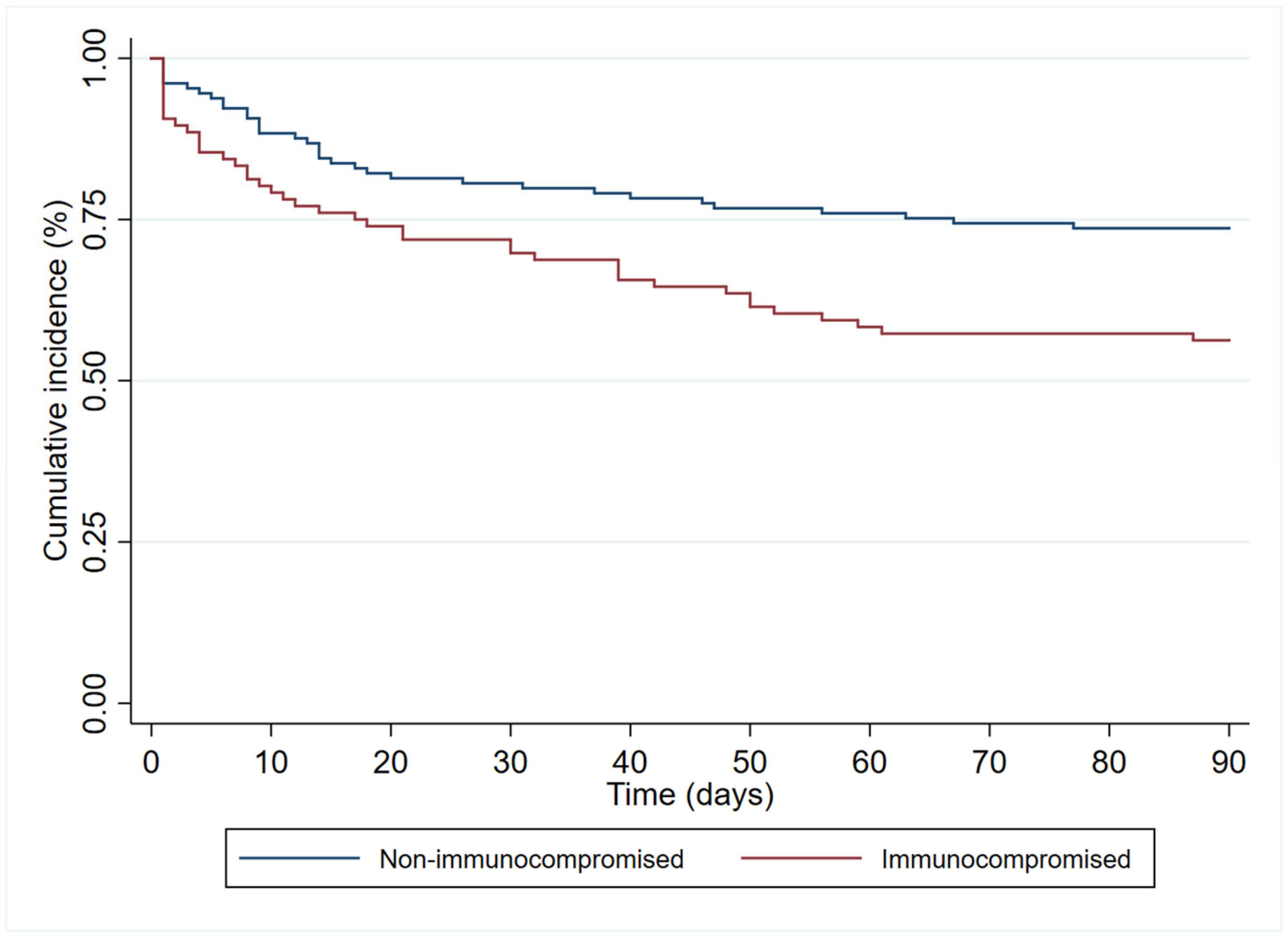
| Immunosuppression | 96 (42.7) | 42 (55.3) | 54 (36.2) | 0.006 |
| Iatrogenic bile duct injury | 34 (15.1) | 7 (9.3) | 27 (18.1) | 0.078 |
| Liver cirrhosis | 13 (5.8) | 3 (4.0) | 10 (6.7) | 0.551 |
| Renal replacement therapy for CKD | 21 (9.3) | 11 (14.5) | 10 (6.7) | 0.058 |
| Cerebrovascular disease | 7 (3.1) | 4 (5.3) | 3 (2.0) | 0.230 |
| Urological disorders | 24 (10.7) | 4 (5.3) | 20 (13.4) | 0.061 |
| Tracheostomy carrier | 31 (13.8) | 9 (11.8) | 22 (14.8) | 0.547 |
| Bacterial coinfection | 120 (53.3) | 41 (54.0) | 79 (53.0) | 0.895 |
| Disease presentation severity, n (%) | ||||
| Mechanical ventilation at diagnosis | 67 (29.8) | 29 (38.2) | 38 (25.5) | 0.050 |
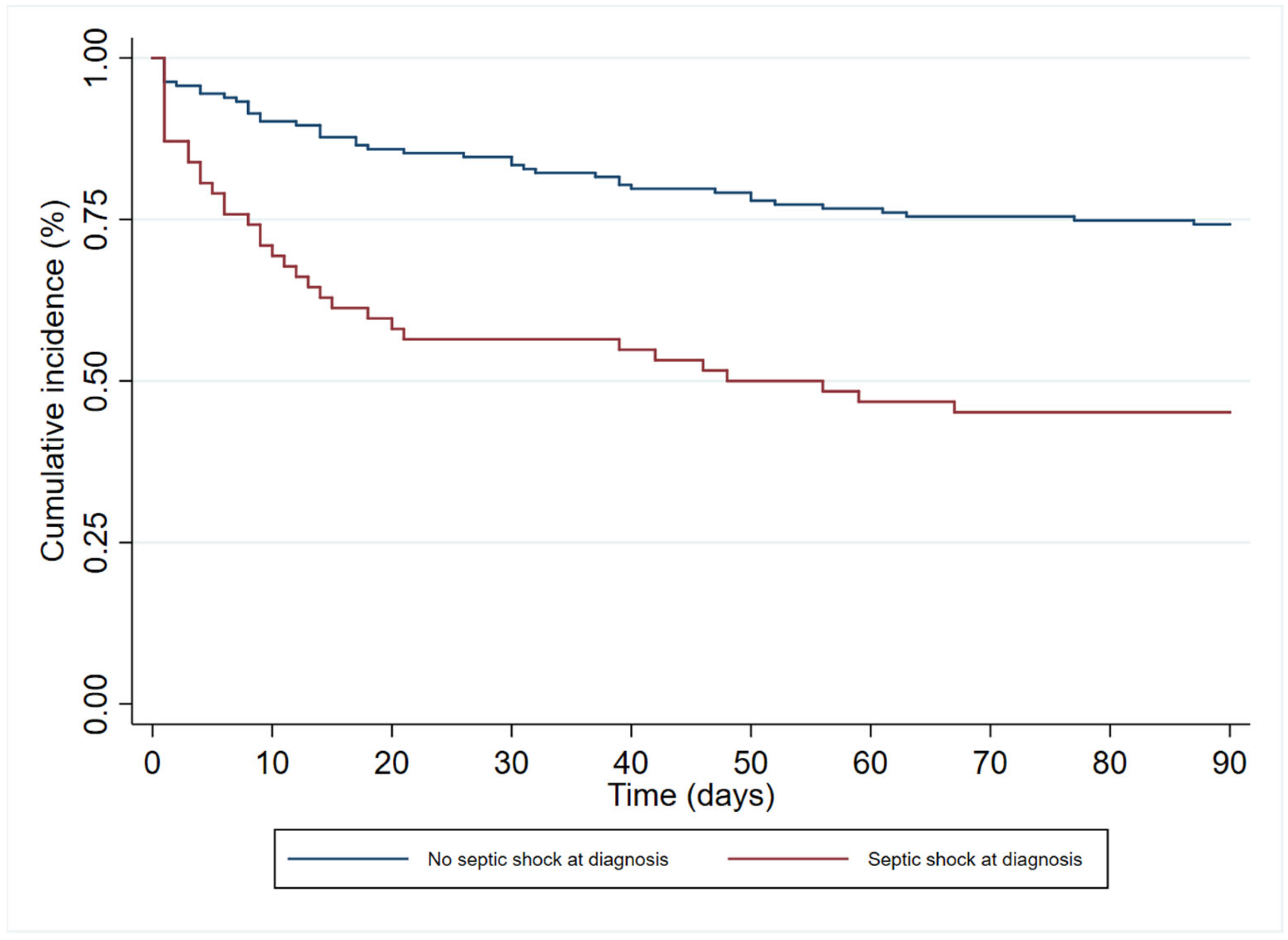
| Septic shock at time of infection | 62 (27.6) | 34 (44.7) | 28 (18.8) | <0.001 |
| Outcome | Total n = 225 (100%) | Deaths at 90 Days n = 76 (33.8%) | Survivors at 90 Days n = 149 (66.2%) | p |
|---|---|---|---|---|
| Mechanical ventilation after diagnosis, n (%) | 19 (8.4) | 13 (17.1) | 6 (4.0) | 0.002 |
| ICU stay after diagnosis, n (%) | 25 (11.1) | 16 (21.1) | 9 (6.0) | 0.001 |
| Infection relapse, n (%) | 41 (18.2) | 8 (10.5) | 33 (22.2) | 0.033 |
| Rehospitalisation for any cause, n (%) n = 224 * | 41 (18.2) | 8 (10.5) | 33 (22.2) | 0.033 |
| C. difficile infection, n (%) | 9 (4.0) | 3 (4.0) | 6 (4.0) | 1.000 |
| Antibiotic-related renal replacement therapy, n (%) | 2 (0.9) | 1 (1.3) | 1 (0.7) | 1.000 |
| Acute kidney injury within the first 10 days of appropriate treatment, n (%) n = 181 | 40 (22.1) | 21 (41.2) | 19 (14.6) | <0.001 |
| Days from diagnosis to death, median (IQR) | - | 13 (4–38) | - | - |
| Variable | aHR (CI 95%), p |
|---|---|
| Male gender | 1.08 (0.64–1.83), 0.779 |
| Age * | 1.19 (1.00–1.83), 0.048 |
| Bloodstream infection | 1.55 (0.60–4.00), 0.364 |
| Respiratory tract infection | 1.25 (0.54–2.94), 0.599 |
| Intraabdominal infection | 0.57 (0.22–1.47), 0.245 |
| Urinary tract infection | 0.33 (0.10–1.10), 0.072 |
| Bone and soft tissue infections | 1.61 (0.59–4.38), 0.347 |
| Obesity | 0.84 (0.46–1.53), 0.564 |
| Diabetes | 0.97 (0.51–1.82), 0.919 |
| Heart disease | 1.51 (0.83–2.73), 0.179 |
| Hypertension | 0.69 (0.39–1.21), 0.193 |
| Immunosuppression | 1.84 (1.06–3.18), 0.030 |
| Cirrhosis | 1.37 (0.40–4.72), 0.618 |
| Renal replacement therapy | 1.65 (0.75–3.62), 0.212 |
| Mechanical ventilation at diagnosis | 1.26 (0.65–2.41), 0.493 |
| Septic shock at time of infection | 2.40 (1.41–4.08), 0.001 |
| Non-fermenting Gram-negative bacilli | 0.84 (0.50–1.42), 0.519 |
| Antibiogram guided appropriate treatment | 0.25 (0.14–0.46), <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rivera-Villegas, H.O.; Martinez-Guerra, B.A.; Garcia-Couturier, R.; Xancal-Salvador, L.F.; Esteban-Kenel, V.; Jaimes-Aquino, R.A.; Mendoza-Rojas, M.; Cervantes-Sánchez, A.; Méndez-Ramos, S.; Alonso-Montoya, J.E.; et al. Predictors of Mortality in Patients with Infections Due to Carbapenem-Resistant Gram-Negative Bacteria. Antibiotics 2023, 12, 1130. https://doi.org/10.3390/antibiotics12071130
Rivera-Villegas HO, Martinez-Guerra BA, Garcia-Couturier R, Xancal-Salvador LF, Esteban-Kenel V, Jaimes-Aquino RA, Mendoza-Rojas M, Cervantes-Sánchez A, Méndez-Ramos S, Alonso-Montoya JE, et al. Predictors of Mortality in Patients with Infections Due to Carbapenem-Resistant Gram-Negative Bacteria. Antibiotics. 2023; 12(7):1130. https://doi.org/10.3390/antibiotics12071130
Chicago/Turabian StyleRivera-Villegas, Hector Orlando, Bernardo Alfonso Martinez-Guerra, Rosalia Garcia-Couturier, Luis Fernando Xancal-Salvador, Veronica Esteban-Kenel, Ricardo Antonio Jaimes-Aquino, Miguel Mendoza-Rojas, Axel Cervantes-Sánchez, Steven Méndez-Ramos, Jorge Eduardo Alonso-Montoya, and et al. 2023. "Predictors of Mortality in Patients with Infections Due to Carbapenem-Resistant Gram-Negative Bacteria" Antibiotics 12, no. 7: 1130. https://doi.org/10.3390/antibiotics12071130