
Clinical Features and Outcomes of VAP Due to Multidrug-Resistant Klebsiella spp.: A Retrospective Study Comparing Monobacterial and Polybacterial Episodes

 and
and
Abstract
:1. Introduction
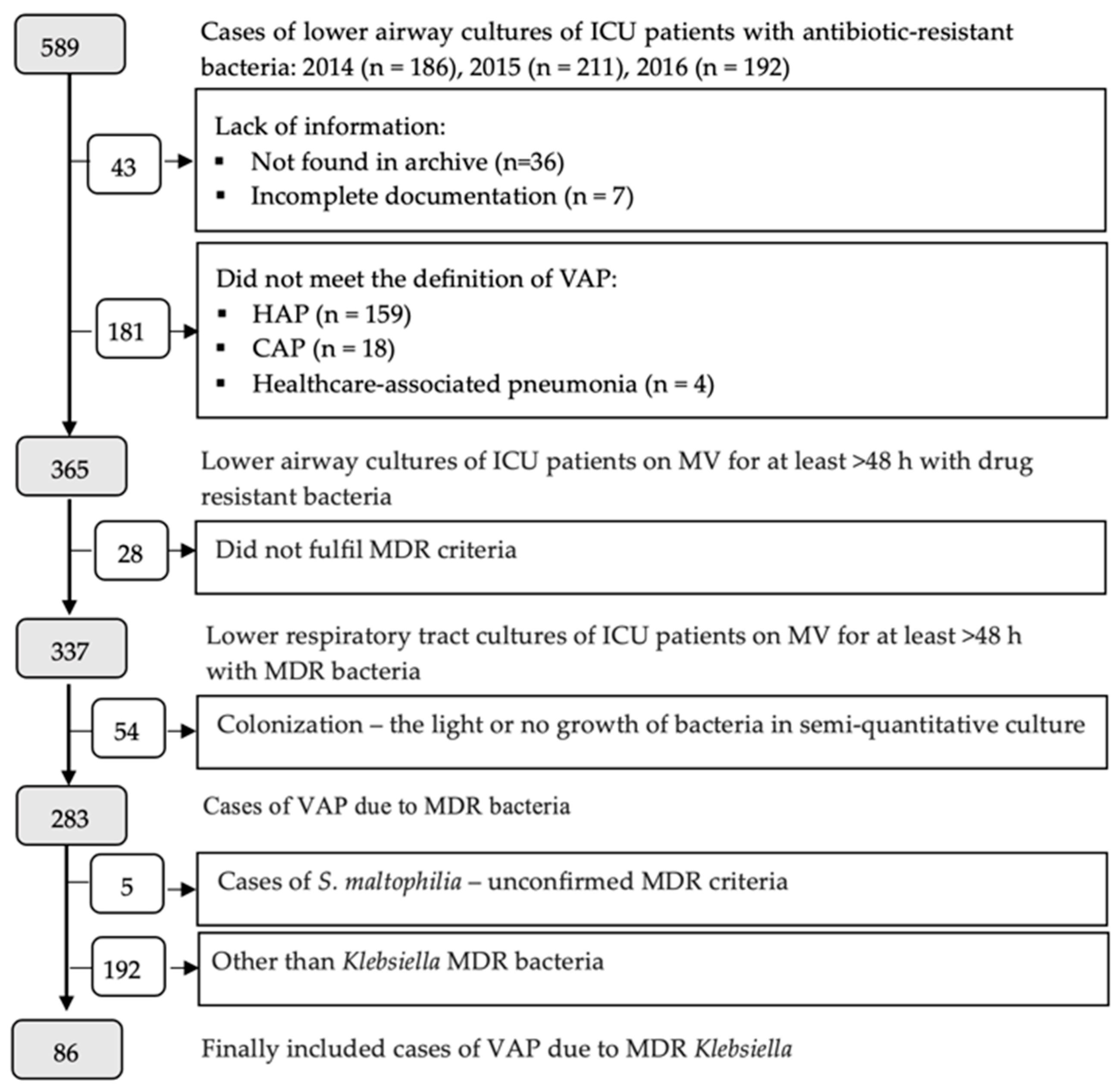
2. Materials and Methods
Statistical Analysis
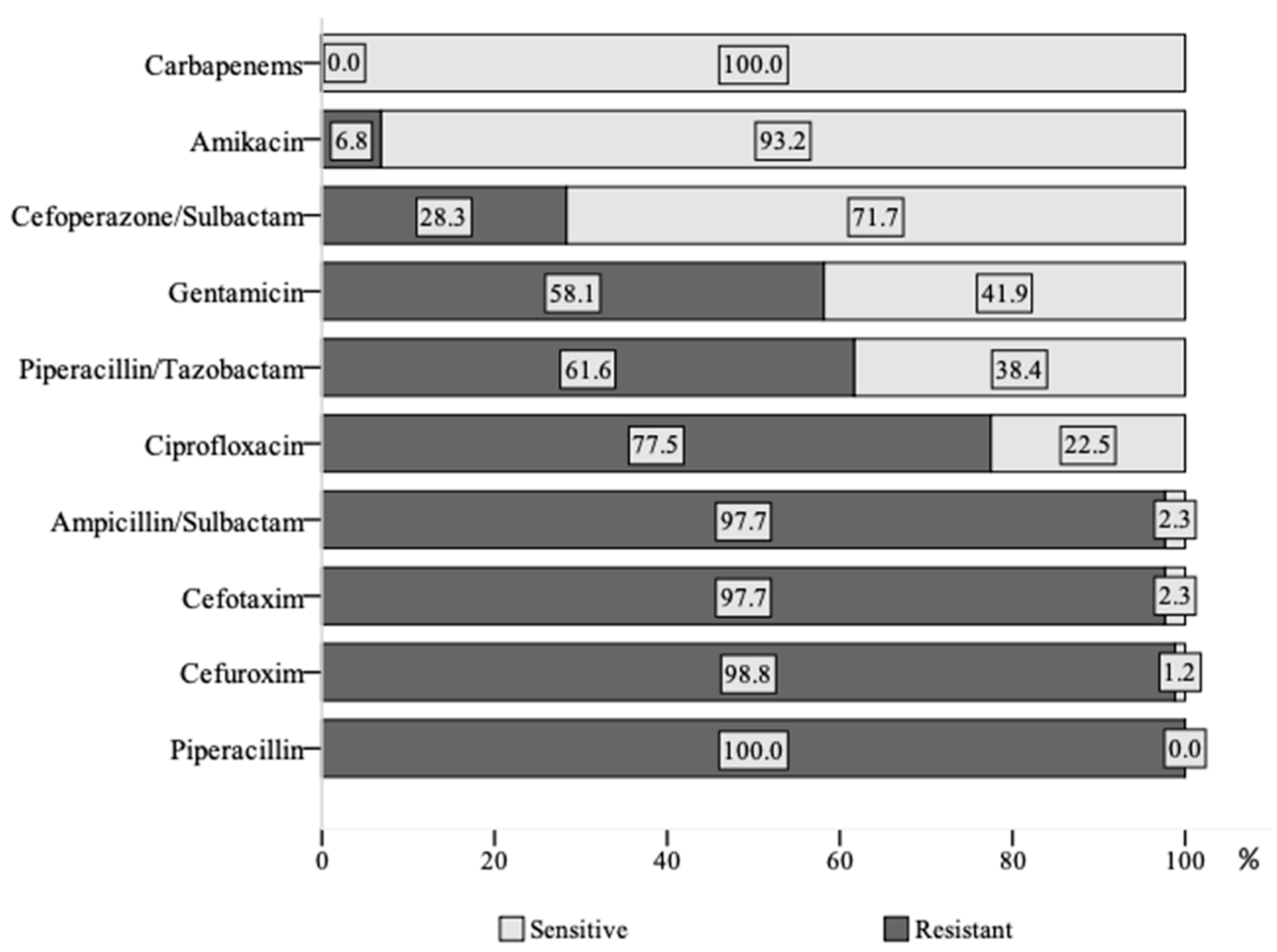
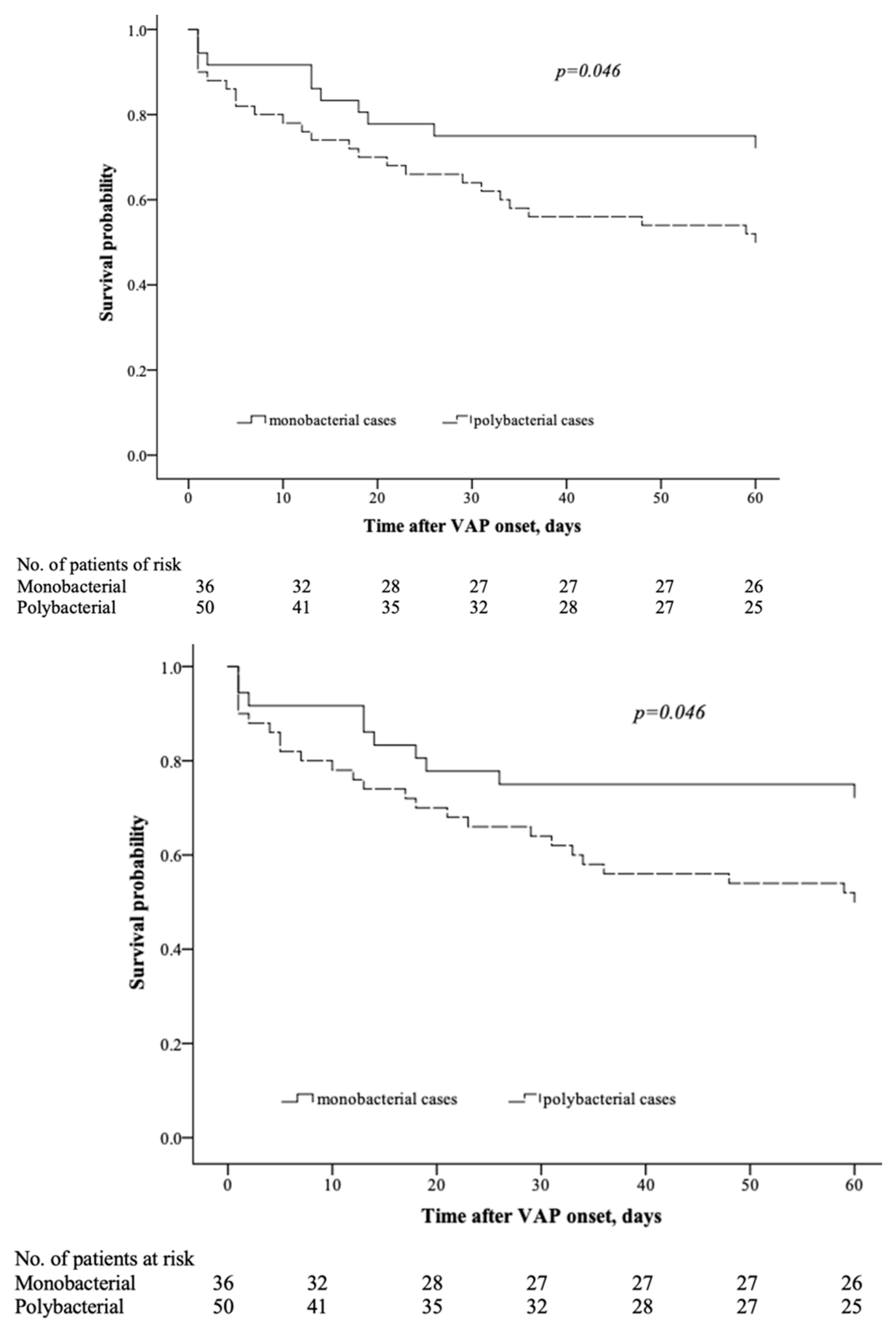
3. Results
4. Discussion
Study Novelties and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Papazian, L.; Klompas, M.; Luyt, C.E. Ventilator-associated pneumonia in adults: Narrative review. Intensive Care Med. 2020, 46, 888–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blot, S.; Ruppé, E.; Harbarth, S.; Asehnoune, K.; Poulakou, G.; Luyt, C.E.; Rello, J.; Klompas, M.; Depuydt, P.; Eckmann, C.; et al. Healthcare-associated infections in adult intensive care unit patients: Changes in epidemiology, diagnosis, prevention and contributions of new technologies. Intensive Crit. Care Nurs. 2022, 70, 103227. [Google Scholar] [CrossRef]
- Ding, X.; Ma, X.; Gao, S.; Su, L.; Shan, G.; Hu, Y.; Chen, J.; Ma, D.; Zhang, F.; Zhu, W.; et al. Effect of ICU quality control indicators on VAP incidence rate and mortality: A retrospective study of 1267 hospitals in China. Crit. Care 2022, 26, 405. [Google Scholar] [CrossRef]
- Sarda, C.; Fazal, F.; Rello, J. Management of ventilator-associated pneumonia (VAP) caused by resistant gram-negative bacteria: Which is the best strategy to treat? Expert Rev. Respir. Med. 2019, 13, 789–798. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Healthcare-Associated Infections Acquired in Intensive Care Units. In Annual Epidemiological Report for 2017; ECDC: Stockholm, Sweden, 2019; Available online: https://www.ecdc.europa.eu/sites/default/files/documents/AER_for_2017-HAI.pdf (accessed on 4 May 2023).
- Koulenti, D.; Tsigou, E.; Rello, J. Nosocomial pneumonia in 27 ICUs in Europe: Perspectives from the EU-VAP/CAP study. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 1999–2006. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Xu, J.; Wei, Y.; Xu, J.; Li, Y.; Xue, R. Clinical and molecular characteristics of Klebsiella pneumoniae ventilator-associated pneumonia in mainland China. BMC Infect. Dis. 2016, 16, 608. [Google Scholar] [CrossRef] [Green Version]
- Surveillance of Healthcare-Associated Infections in Intensive Care Units. Annual Epidemiological Report for 2015 [Hospitalinių Infekcijų Epidemiologinės Priežiūros Padidintos Rizikos Skyriuose 2015 m. Ataskaita]. Available online: https://www.hi.lt/uploads/pdf/padaliniai/VSTC%20IS/RITS/RITS_2022_m._ataskaita.pdf (accessed on 4 May 2023).
- Rello, J.; Kalwaje Eshwara, V.; Conway-Morris, A.; Lagunes, L.; Alves, J.; Alp, E.; Zhang, Z.; Mer, M.; TOTEM Study Investigators. Perceived differences between intensivists and infectious diseases consultants facing antimicrobial resistance: A global cross-sectional survey. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2019, 38, 1235–1240. [Google Scholar] [CrossRef]
- Rello, J.; Kalwaje Eshwara, V.; Lagunes, L.; Alves, J.; Wunderink, R.G.; Conway-Morris, A.; Rojas, J.N.; Alp, E.; Zhang, Z. A global priority list of the TOp TEn resistant Microorganisms (TOTEM) study at intensive care: A prioritization exercise based on multi-criteria decision analysis. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2019, 38, 319–323. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Surveillance of Antimicrobial Resistance in Europe 2019. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/surveillance-antimicrobial-resistance-Europe-2019.pdf (accessed on 4 May 2023).
- Sharma, A.; Thakur, A.; Thakur, N.; Kumar, V.; Chauchan, A.; Bhardwa, N. Changing trend in the antibiotic resistance pattern of Klebsiella pneumonia isolated from endotracheal aspirate samples of ICU patients of a tertiary care hospital in North India. Cureus 2023, 15, e36317. [Google Scholar] [CrossRef]
- Tacconelli, E.; Magrini, N. Global Priority List of Antibiotic-Resistant Bacteria to Guide Research, Discovery, and Development of New Antibiotics. Available online: http://www.who.int/medicines/publications/global-priority-list-antibiotic-resistant-bacteria/en/ (accessed on 4 May 2023).
- Mahjobipoor, H.; Sajadi, M.; Honarmand, A.; Rahimi-Varposhti, M.; Yadegari, S.; Fattahpour, S.; Soleimani, M. Prevalence incidence and clinical outcome of Klebsiella and Acinetobacter ventilator-associated pneumonia. Immunopathol. Persa 2023, 9, e34412. [Google Scholar] [CrossRef]
- Gupta, A.; Agrawal, A.; Mehrotra, S.; Singh, A.; Malik, S.; Khanna, A. Incidence, risk stratification, antibiogram of pathogens isolated and clinical outcome of ventilator associated pneumonia. Indian J. Crit. Care Med. 2011, 15, 96–101. [Google Scholar] [CrossRef] [Green Version]
- Lakbar, I.; Medam, S.; Ronflé, R.; Cassir, N.; Delamarre, L.; Hammad, E.; Lopez, A.; Lepape, A.; Machut, A.; Boucekine, M.; et al. Association between mortality and highly antimicrobial-resistant bacteria in intensive care unit-acquired pneumonia. Sci. Rep. 2021, 11, 16497. [Google Scholar] [CrossRef]
- Serra-Burriel, M.; Keys, M.; Campillo-Artero, C.; Agodi, A.; Barchitta, M.; Gikas, A.; Polos, C.; Lopez-Casasnovas, G. Impact of multi-drug resistant bacteria on economic and clinical outcomes of healthcare-associated infections in adults: Systematic review and meta-analysis. PLoS ONE 2020, 15, e0227139. [Google Scholar] [CrossRef]
- Bassetti, M.; Righi, E.; Carnelutti, A.; Graziano, E.; Russo, A. Multidrug-resistant Klebsiella pneumoniae: Challenges for treatment, prevention and infection control. Expert Rev. Anti-Infect. Ther. 2018, 16, 749–761. [Google Scholar] [CrossRef] [PubMed]
- Combes, A.; Figliolini, C.; Trouillet, J.L.; Kassis, N.; Wolff, M.; Gibert, C.; Chastre, J. Incidence and outcomes of polymicrobial ventilator-associated pneumonia. Chest 2002, 121, 1618–1623. [Google Scholar] [CrossRef]
- Ferrer, M.; Difrancesco, L.F.; Liapikou, A.; Rinaudo, M.; Carbonara, M.; Li Bassi, G.; Gabarrus, A.; Torres, A. Polymicrobial intensive care unit-acquired pneumonia: Prevalence, microbiology and outcome. Crit. Care 2015, 19, 450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardak, E.; Avivi, I.; Berkun, L.; Raz-Pasteur, A.; Lavi, N.; Geffen, Y.; Yigla, M.; Oren, I. Polymicrobial pulmonary infection in patients with hematological malignancies: Prevalence, co-pathogens, course and outcome. Infection 2016, 44, 491–497. [Google Scholar] [CrossRef]
- Karakonstantis, S.; Kritsotakis, E.I. Systematic review and meta-analysis of the proportion and associated mortality of polymicrobial (vs monomicrobial) pulmonary and bloodstream infections by Acinetobacter baumannii complex. Infection 2021, 49, 1149–1161. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Fusco, P.; Morrone, H.L.; Trecarichi, E.M.; Torti, C. New advances in management and treatment of multidrug-resistant Klebsiella pneumoniae. Expert Rev. Anti-Infect. Ther. 2023, 21, 41–55. [Google Scholar] [CrossRef]
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am. J. Respir. Crit. Care Med. 2005, 171, 388–416. [Google Scholar] [CrossRef] [Green Version]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 6.0. 2016. Available online: http://www.eucast.org (accessed on 4 May 2023).
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Ollson-Liljequist; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dellinger, R.F.; Levy, M.M.; Rhodes, A.; Annane, D.; Gerlach, H.; Opal, S.M.; Sevransky, J.E.; Sprung, C.L.; Douglas, I.S.; Jaeschke, R.; et al. Surviving Sepsis Campaign: International guidelines for management of sepsis and septic shock: 2012. Crit. Care Med. 2013, 41, 580–637. [Google Scholar] [CrossRef]
- Cilloniz, C.; Civljak, R.; Nicolini, A.; Torres, A. Polymicrobial community-acquired pneumonia: An emerging entity. Respirology 2016, 21, 65–75. [Google Scholar] [CrossRef]
- Brogden, K.A.; Guthmiller, J.M.; Taylor, C.E. Human polymicrobial infections. Lancet 2005, 365, 253–255. [Google Scholar] [CrossRef]
- Brewer, S.C.; Wunderink, R.G.; Jones, C.B.; Leeper, K.V. Ventilator-associated pneumonia due to Pseudomonas aeruginosa. Chest 1996, 109, 1019–1029. [Google Scholar] [CrossRef]
- Adukauskiene, D.; Ciginskiene, A.; Adukauskaite, A.; Koulenti, D.; Rello, J. Clinical features and outcomes of monobacterial and polybacterial episodes of ventilator-associated pneumonia due to multidrug-resistant Acinetobacter baumannii. Antibiotics 2022, 11, 892. [Google Scholar] [CrossRef]
- Hwang, J.H.; Handigund, M.; Hwang, J.H.; Cho, Y.G.; Kim, D.S.; Lee, J. Clinical features and risk factors associated with 30-day mortality in patients with pneumonia caused by hypervirulent Klebsiella pneumoniae (hvKP). Ann. Lab. Med. 2020, 40, 481–487. [Google Scholar] [CrossRef]
- Puech, B.; Canivet, C.; Teysseyre, L.; Miltgen, G.; Aujoulat, T.; Caron, M.; Combe, C.; Jabot, J.; Martinet, O.; Allyn, J.; et al. Effect of antibiotic therapy on the prognosis of ventilator-associated pneumonia caused by Stenotrophomonas maltophilia. Ann. Intensive Care 2021, 11, 160. [Google Scholar] [CrossRef]
- Chang, Y.; Jeon, K.; Lee, S.M.; Cho, Y.J.; Kim, Y.S.; Chong, Y.P.; Hong, S.B. The distribution of multidrug-resistant microorganisms and treatment status of hospital-acquired pneumonia/ventilator-associated pneumonia in adult Intensive Care units: A prospective cohort observational study. J. Korean Med. Sci. 2021, 36, e251. [Google Scholar] [CrossRef] [PubMed]
- Kadri, S.S.; Lai, Y.L.; Warner, S.; Strich, J.R.; Babiker, A.; Ricotta, E.E.; Demirkale, C.Y.; Dekker, J.P.; Palmore, T.N.; Rhee, C.; et al. Inappropriate empirical antibiotic therapy for bloodstream infections based on discordant in-vitro susceptibilities: A retrospective cohort analysis of prevalence, predictors, and mortality risk in US hospitals. Lancet Infect. Dis. 2021, 21, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Chong, K.K.; Kline, K.A. Polymicrobial-host interactions during infection. J. Mol. Biol. 2016, 428, 3355–3371. [Google Scholar] [CrossRef]
- Hodak, H. Down to the molecular mechanisms of host-pathogen interactions. J. Mol. Biol. 2016, 428, 3353–3354. [Google Scholar] [CrossRef]
- Peters, B.M.; Jabra-Rizk, M.A.; O’May, G.A.; Costerton, J.W.; Shirtliff, M.E. Polymicrobial interactions: Impact on pathogenesis and human disease. Clin. Microbiol. Rev. 2012, 25, 193–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, Y.T.; Kuo, S.C.; Lee, Y.T.; Chen, C.P.; Lin, S.W.; Shen, L.J.; Fung, C.P.; Cho, W.L.; Chen, T.L. Sheltering effect and indirect pathogenesis of carbapenem-resistant Acinetobacter baumannii in polymicrobial infection. Antimicrob. Agents Chemother. 2014, 58, 3983–3990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verway, M.; Brown, K.A.; Marchand-Austin, A.; Diong, C.; Lee, S.; Langford, B.; Schwartz, K.L.; MacFadden, D.R.; Patel, S.N.; Sander, B.; et al. Prevalence and mortality associated with bloodstream organisms: A population-wide retrospective cohort study. J. Clin. Microbiol. 2022, 60, e0242921. [Google Scholar] [CrossRef] [PubMed]
- Mohd Asri, N.A.; Ahmad, S.; Mohamud, R.; Mohd Hanafi, N.; Mohd Zaidi, N.F.; Irekeola, A.A.; Shueb, R.H.; Yee, L.C.; Mohd Noor, N.; Mustafa, F.H.; et al. Global prevalence of nosocomial multidrug-resistant Klebsiella pneumoniae: A systematic review and meta-analysis. Antibiotics 2021, 10, 1508. [Google Scholar] [CrossRef] [PubMed]
- Maczynska, B.; Paleczny, J.; Oleksy-Wawrzyniak, M.; Choroszy-Krol, I.; Bartoszewicz, M. In vitro susceptibility of multi-drug resistant Klebsiella pneumoniae strains causing nosocomial infections to Fosfomycin. A comparison of determination methods. Pathogens 2021, 10, 512. [Google Scholar] [CrossRef]
- Kot, B.; Piechota, M.; Szweda, P.; Mitrus, J.; Wicha, J.; Gruzewska, A.; Witeska, M. Virulence analysis and antibiotic resistance of Klebsiella pneumoniae isolates from hospitalised patients in Poland. Sci. Rep. 2023, 13, 4448. [Google Scholar] [CrossRef]
- Spadar, A.; Phelan, J.; Elias, R.; Modesto, A.; Caneiras, C.; Marques, C.; Lito, L.; Pinto, M.; Cavaco-Silva, P.; Ferreira, H.; et al. Genomic epidemiological analysis of Klebsiella pneumoniae from Portuguese hospitals reveals insights into circulating antimicrobial resistance. Sci. Rep. 2022, 12, 13791. [Google Scholar] [CrossRef]
- Motsch, J.; Murta de Oliveira, C.; Stus, V.; Köksal, I.; Lyulko, O.; Boucher, H.W.; Kaye, K.S.; File, T.M.; Brown, M.L.; Khan, I.; et al. RESTORE-IMI 1: A multicenter, randomized, double-blind trial comparing efficacy and safety of Imipenem/Relebactam vs Colistin plus Imipenem in patients with Imipenem-nonsusceptible bacterial infections. Clin. Infect. Dis. 2020, 70, 1799–1808. [Google Scholar] [CrossRef] [Green Version]
- Titov, I.; Wunderink, R.G.; Roquilly, A.; Rodríguez Gonzalez, D.; David-Wang, A.; Boucher, H.W.; Kaye, K.S.; Losada, M.C.; Du, J.; Tipping, R.; et al. A randomized, double-blind, multicenter trial comparing efficacy and safety of Imipenem/Cilastatin/Relebactam versus Piperacillin/Tazobactam in adults with hospital-acquired or ventilator-associated bacterial pneumonia (RESTORE-IMI 2 Study). Clin. Infect. Dis. 2021, 73, e4539–e4548. [Google Scholar] [CrossRef]
- Natarajan, R.; Ramanathan, V.; Sistla, S. Poor sensorium at the time of intubation predicts polymicrobial ventilator associated pneumonia. Ther. Clin. Risk Manag. 2022, 18, 125–133. [Google Scholar] [CrossRef]
- Doualeh, M.; Payne, M.; Litton, E.; Raby, E.; Currie, A. Molecular methodologies for improved polymicrobial sepsis diagnosis. Int. J. Mol. Sci. 2022, 23, 4484. [Google Scholar] [CrossRef] [PubMed]
- Kadri, S.S.; Adjemian, J.; Lai, Y.L.; Spaulding, A.B.; Ricotta, E.; Prevots, D.R.; Palmore, T.N.; Rhee, C.; Klompas, M.; Dekker; et al. National Institutes of Health Antimicrobial Resistance Outcomes Research Initiative (NIH–ARORI). Difficult-to-Treat Resistance in Gram-negative Bacteremia at 173 US Hospitals: Retrospective Cohort Analysis of Prevalence, Predictors, and Outcome of Resistance to All First-line Agents. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2018, 67, 1803–1814. [Google Scholar] [CrossRef] [Green Version]
- El-Sokkary, R.; Uysal, S.; Erdem, H.; Kullar, R.; Pekok, A.U.; Amer, F.; Grgić, S.; Carevic, B.; El-Kholy, A.; Liskova, A.; et al. Profiles of multidrug-resistant organisms among patients with bacteremia in intensive care units: An international ID-IRI survey. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2021, 40, 2323–2334. [Google Scholar] [CrossRef] [PubMed]
- Maertens, B.; Lin, F.; Chen, Y.; Rello, J.; Lathyris, D.; Blot, S. Effectiveness of Continuous Cuff Pressure Control in Preventing Ventilator-Associated Pneumonia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Crit. Care Med. 2022, 50, 1430–1439. [Google Scholar] [CrossRef]
- Boisson, M.; Bouglé, A.; Sole-Lleonart, C.; Dhanani, J.; Arvaniti, K.; Rello, J.; Rouby, J.J.; Mimoz, O.; European Investigator Network for Nebulized Antibiotics in Ventilator-Associated Pneumonia (ENAVAP). Nebulized Antibiotics for Healthcare- and Ventilator-Associated Pneumonia. Semin. Respir. Crit. Care Med. 2022, 43, 255–270. [Google Scholar] [CrossRef] [PubMed]
- Campogiani, L.; Tejada, S.; Ferreira-Coimbra, J.; Restrepo, M.I.; Rello, J. Evidence supporting recommendations from international guidelines on treatment, diagnosis, and prevention of HAP and VAP in adults. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2020, 39, 483–491. [Google Scholar] [CrossRef]
- Peña-López, Y.; Ramirez-Estrada, S.; Eshwara, V.K.; Rello, J. Limiting ventilator-associated complications in ICU intubated subjects: Strategies to prevent ventilator-associated events and improve outcomes. Expert Rev. Respir. Med. 2018, 12, 1037–1050. [Google Scholar] [CrossRef]
- Azak, E.; Sertcelik, A.; Ersoz, G.; Celebi, G.; Eser, F.; Batirel, A.; Cag, Y.; Ture, Z.; Ozturk Engin, D.; Yetkin, M.A.; et al. THIRG, Turkish Hospital Infection Research Group. Evaluation of the implementation of WHO infection prevention and control core components in Turkish health care facilities: Results from a WHO infection prevention and control assessment framework (IPCAF)-based survey. Antimicrob. Resist. Infect. Control 2023, 12, 11. [Google Scholar] [CrossRef]
- Rello, J.; Paiva, J.A. Antimicrobial stewardship at the emergency department: Dead bugs do not mutate! Eur. J. Intern. Med. 2023, 109, 30–32. [Google Scholar] [CrossRef] [PubMed]
- El-Sokkary, R.; Erdem, H.; Kullar, R.; Pekok, A.U.; Amer, F.; Grgić, S.; Carevic, B.; El-Kholy, A.; Liskova, A.; Özdemir, M.; et al. Self-reported antibiotic stewardship and infection control measures from 57 intensive care units: An international ID-IRI survey. J. Infect. Public Health. 2022, 15, 950–954. [Google Scholar] [CrossRef] [PubMed]
- Tabah, A.; Bassetti, M.; Kollef, M.H.; Zahar, J.R.; Paiva, J.A.; Timsit, J.F.; Roberts, J.A.; Schouten, J.; Giamarellou, H.; Rello, J.; et al. Antimicrobial de-escalation in critically ill patients: A position statement from a task force of the European Society of Intensive Care Medicine (ESICM) and European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Critically Ill Patients Study Group (ESGCIP). Intensive Care Med. 2020, 46, 245–265. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Sarda, C.; Mokart, D.; Arvaniti, K.; Akova, M.; Tabah, A.; Azoulay, E.; Nine-I study Group. Antimicrobial Stewardship in Hematological Patients at the intensive care unit: A global cross-sectional survey from the Nine-i Investigators Network. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2020, 39, 385–392. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | VAP Origin | ||
|---|---|---|---|
| Monobacterial n = 36 | Polybacterial n = 50 | p Value | |
| Age, years, median (IQR) | 67.0 (55.0–75.0) | 71.0 (57.5–76.5) | 0.813 |
| Sex, male, n (%) | 32.0 (88.9) | 44.0 (88.0) | 0.899 |
| Prior hospitalization within 90 days, n (%) | 22 (61.1) | 20 (40.0) | 0.053 |
| Hospitalisation to ICU from, n (%): | |||
| 14 (38.9) 14 (38.9) 8 (22.2) | 23 (46.0) 17 (34.0) 10 (20.0) | 0.805 |
| Admission, n (%): | |||
| 11 (30.6) 25 (69.4) | 27 (54.0) 23 (46.0) | 0.148 |
| Chronic illness, n (%): | |||
| 31 (86.1) 28 (77.8) 4 (11.1) 5 (13.9) 18 (30.6) 11 (30.6) | 38 (76.0) 35 (70.0) 3 (6.0) 11 (22.0) 5 (5.8) 4 (4.7) | 0.245 0.421 0.392 0.340 0.01 0.007 |
| The use of intravenous antibiotic within 90 days, n (%): | 28 (77.8) | 26 (52.0) | 0.015 |
| 12 (33.3) 24 (66.7) 4 (11.1) 4 (11.1) 3 (3.5) | 12 (24.0) 8 (36.0) 4 (8.0) 3 (6.0) 2 (2.3) | 0.341 0.005 0.715 0.446 0.645 |
| Disease severity at VAP onset, median (IQR): | |||
| 45.0 (35.25–51.0) 7.5 (6–9.75) | 50.0 (40.5–60.75) 7.0 (5.0–8.25) | 0.033 0.149 |
| Organ failure at VAP onset, n (%): | |||
| 28 (77.8) 16 (44.4) 8 (22.2) | 36 (72.0) 5 (10.0) 26 (52.0) | 0.545 <0.001 0.005 |
| Variable | 60-Day Mortality | ||
|---|---|---|---|
| VAP Origin | p Value | ||
| Monobacterial, n/Total (%) * | Polybacterial, n/Total (%) * | ||
| All samples | 10//36 (27.8) | 25/50 (50.0) | 0.039 |
| Severity at VAP diagnosis | |||
| 3/20 (15.0) 7/416 (43.8) | 15/33 (45.5) 10/17 (58.8) | 0.023 0.387 |
| Appropriate treatment and severity at VAP diagnosis | |||
| 2/16 (12.5) 6/15 (40.0) | 10/26 (41.7) 6/13 (46.2) | 0.049 0.743 |
| Antibacterial resistance profile of Klebsiella spp. strains | |||
| 7/19 (36.8) 3/17 (17.6) | 12/21 (57.1) 13/28 (46.4) | 0.199 0.051 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adukauskiene, D.; Ciginskiene, A.; Adukauskaite, A.; Koulenti, D.; Rello, J. Clinical Features and Outcomes of VAP Due to Multidrug-Resistant Klebsiella spp.: A Retrospective Study Comparing Monobacterial and Polybacterial Episodes. Antibiotics 2023, 12, 1056. https://doi.org/10.3390/antibiotics12061056
Adukauskiene D, Ciginskiene A, Adukauskaite A, Koulenti D, Rello J. Clinical Features and Outcomes of VAP Due to Multidrug-Resistant Klebsiella spp.: A Retrospective Study Comparing Monobacterial and Polybacterial Episodes. Antibiotics. 2023; 12(6):1056. https://doi.org/10.3390/antibiotics12061056
Chicago/Turabian StyleAdukauskiene, Dalia, Ausra Ciginskiene, Agne Adukauskaite, Despoina Koulenti, and Jordi Rello. 2023. "Clinical Features and Outcomes of VAP Due to Multidrug-Resistant Klebsiella spp.: A Retrospective Study Comparing Monobacterial and Polybacterial Episodes" Antibiotics 12, no. 6: 1056. https://doi.org/10.3390/antibiotics12061056