
Efficacy and Safety of Antibiotic Impregnated Microporous Nanohydroxyapatite Beads for Chronic Osteomyelitis Treatment: A Multicenter, Open-Label, Prospective Cohort Study

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Demographics and Clinical Characteristics
2.2. Blood Biochemistry and Therapeutic Drug Monitoring
2.3. Treatment Outcome
2.4. Quality of Life by SF-36 Questionnaire
2.5. Adverse Events
3. Discussion
4. Materials and Methods
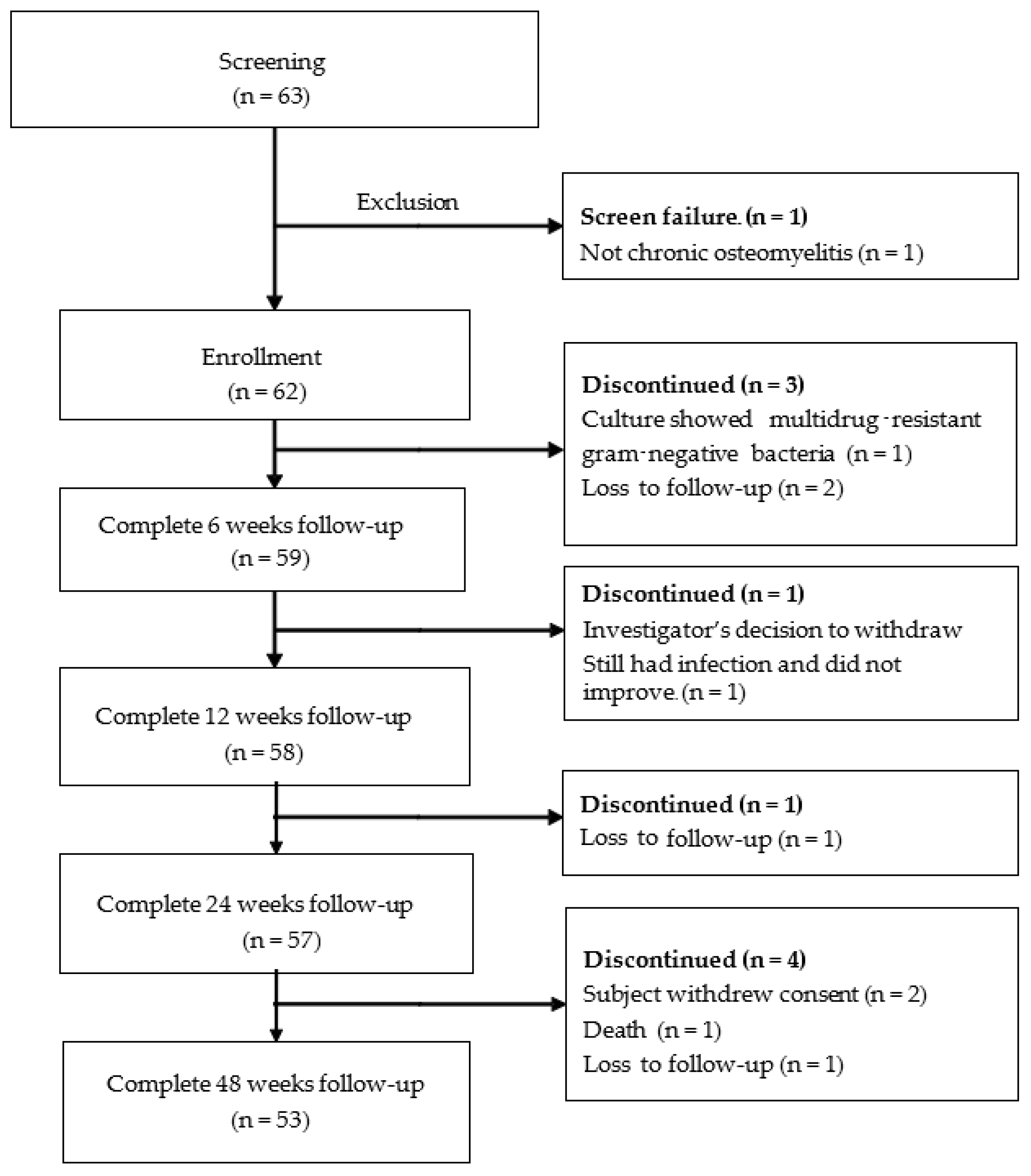
4.1. Patient Enrollment
4.2. Preparation of Antibiotic Impregnated Microporous Nanohydroxyapatite Beads
4.3. Operative Procedure
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- O’Connor, O.; Thahir, A.; Krkovic, M. How much does an infected fracture cost? Arch. Bone Jt. Surg. 2022, 10, 135–140. [Google Scholar] [CrossRef]
- Dartnell, J.; Ramachandran, M.; Katchburian, M. Haematogenous acute and subacute paediatric osteomyelitis. J. Bone Joint Surg. Br. 2012, 94-B, 584–595. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, J.J.; Dormans, J.P.; Kozin, S.H.; Pizzutillo, P.D. Musculoskeletal infections in children. Basic treatment principles and recent advancements. J. Bone Joint Surg. 2004, 86A, 850–863. [Google Scholar] [CrossRef]
- De Boeck, H. Osteomyelitis and septic arthritis in children. Acta Orthop. Belg. 2005, 71, 505–515. [Google Scholar] [PubMed]
- Riise, O.R.; Kirkhus, E.; Handeland, K.S.; Flato, B.; Reiseter, T.; Cvancarova, M.; Nakstad, B.; Wathne, K.-O. Childhood osteomyelitis-Incidence and differentiation from other acute onset musculoskeletal features in a population-based study. BMC Pediatr. 2008, 8, 45. [Google Scholar] [CrossRef] [PubMed]
- Walter, N.; Bärtl, S.; Alt, V.; Rupp, M. The epidemiology of osteomyelitis in children. Children 2021, 8, 1000. [Google Scholar] [CrossRef]
- Walter, N.; Baertl, S.; Alt, V.; Rupp, M. What is the burden of osteomyelitis in Germany? An analysis of inpatient data from 2008 through 2018. BMC Infect. Dis. 2021, 21, 550. [Google Scholar] [CrossRef] [PubMed]
- Henke, P.K.; Blackburn, S.A.; Wainess, R.W.; Cowan, J.; Terando, A.; Proctor, M.; Wakefield, T.W.; Upchurch, G.R.; Stanley, J.C.; Greenfield, L.J. Osteomyelitis of the Foot and Toe in Adults Is a Surgical Disease. Ann. Surg. 2005, 241, 885–894. [Google Scholar] [CrossRef]
- Shone, A.; Burnside, J.; Chipchase, S.; Game, F.; Jeffcoate, W. Probing the validity of the probe-to bone test in the diagnosis of osteomyelitis of the foot in diabetes. Diabetes Care 2006, 29, 945. [Google Scholar] [CrossRef]
- Lavery, L.A.; Armstrong, D.G.; Peters, E.J.; Lipsky, B.A. Probe-to-bone test for diagnosing diabetic foot osteomyelitis: Reliable or relic? Diabetes Care 2007, 30, 270–274. [Google Scholar] [CrossRef]
- Masters, E.A.; Ricciardi, B.F.; Bentley, K.L.D.M.; Moriarty, T.F.; Schwarz, E.M.; Muthukrishnan, G. Skeletal infections: Microbial pathogenesis, immunity and clinical management. Nat. Rev. Microbiol. 2022, 20, 385–400. [Google Scholar] [CrossRef] [PubMed]
- Meroni, G.; Tsikopoulos, A.; Tsikopoulos, K.; Allemanno, F.; Martino, P.A.; Soares Filipe, J.F. A Journey into Animal Models of Human Osteomyelitis: A Review. Microorganisms 2022, 10, 1135. [Google Scholar] [CrossRef]
- Veis, D.J.; Cassat, J.E. Infectious osteomyelitis: Marrying bone biology and microbiology to shed new light on a persistent clinical challenge. J. Bone Miner. Res. 2021, 36, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Wassif, R.K.; Elkayal, M.; Shamma, R.N.; Elkheshen, S.A. Recent advances in the local antibiotics delivery systems for management of osteomyelitis. Drug Deliv. 2021, 28, 2392–2414. [Google Scholar] [CrossRef] [PubMed]
- Cobb, L.H.; McCabe, E.M.; Priddy, L.B. Therapeutics and delivery vehicles for local treatment of osteomyelitis. J. Orthop. Res. 2020, 38, 2091–2103. [Google Scholar] [CrossRef] [PubMed]
- Lorentzen, A.K.; Engel, L.; Gottlieb, H.; Obinah, M.P.B. One-stage treatment of chronic osteomyelitis with an antibiotic-loaded biocomposite and a local or free flap. Eur. J. Plast. Surg. 2021, 44, 367–374. [Google Scholar] [CrossRef]
- Steadman, W.; Chapman, P.R.; Schuetz, M.; Schmutz, B.; Trampuz, A.; Tetsworth, K. Local Antibiotic Delivery Options in Prosthetic Joint Infection. Antibiotics 2023, 12, 752. [Google Scholar] [CrossRef]
- Roos, E.; Bartha, H.; Charles, V.; Hoepelman, A.I.M.; Peters, E.J.G. To bead or not to bead? Treatment of osteomyelitis and prosthetic joint-associated infections with gentamicin bead chains. Int. J. Antimicrob. Agents. 2011, 38, 371–375. [Google Scholar] [CrossRef]
- van Vugt, T.A.G.; Arts, J.J.; Geurts, J.A.P. Antibiotic-loaded polymethylmethacrylate beads and spacers in treatment of orthopedic infections and the role of biofilm formation. Front. Microbiol. 2019, 10, 1626. [Google Scholar] [CrossRef]
- Thomes, B.; Murray, P.; Bouchier-Hayes, D. Development of resistant strains of Staphylococcus epidermidis on gentamicin-loaded bone cement in vivo. J. Bone Joint Surg. Br. 2002, 84, 758–760. [Google Scholar] [CrossRef]
- Neut, D.; van de Belt, H.; Stokroos, I.; van Horn, J.R.; van der Mei, H.C.; Busscher, H.J. Biomaterial-associated infection of gentamicin-loaded PMMA beads in orthopaedic revision surgery. J. Antimicrob. Chemother. 2001, 47, 885–891. [Google Scholar] [CrossRef]
- Hansen, E.N.; Adeli, B.; Kenyon, R.; Parvizi, J. Routine use of antibiotic laden bone cement for primary total knee arthroplasty: Impact on infecting microbial patterns and resistance profiles. J. Arthroplast. 2014, 29, 1123–1127. [Google Scholar] [CrossRef] [PubMed]
- Ene, R.; Nica, M.; Ene, D.; Cursaru, A.; Cirstoiu, C. Review of calcium-sulphate-based ceramics and synthetic bone substitutes used for antibiotic delivery in PJI and osteomyelitis treatment. EFORT Open Rev. 2021, 6, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Kallala, R.; Harris, W.E.; Ibrahim, M.; Dipane, M.; McPherson, E. Use of Stimulan absorbable calcium sulphate beads in revision lower limb arthroplasty. Bone Joint Res. 2018, 7, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Thahir, A.; Lim, J.A.; West, C.; Krkovic, M. The use of calcium sulphate beads in the management of osteomyelitis of femur and tibia: A systematic review. Arch. Bone Jt. Surg. 2022, 10, 320–327. [Google Scholar] [CrossRef]
- Ferguson, J.Y.; Dudareva, M.; Riley, N.D.; Stubbs, D.; Atkins, B.L.; McNally, M.A. The use of a biodegradable antibiotic-loaded calcium sulphate carrier containing tobramycin for the treatment of chronic osteomyelitis. Bone Joint J. 2014, 96-B, 829–836. [Google Scholar] [CrossRef]
- Ali, T.; Mutalik, S.; Venkatesh, M.; Shenoy, D.B.; Acharya, L.; Udupa, U. Biodegradable implants of gentamicin sulfate for effective management of osteomyelitis. Saudi. Pharma. J. 2006, 14, 120–125. [Google Scholar]
- Chang, H.I.; Perrie, Y.; Coombes, A.G.A. Delivery of the antibiotic gentamicin sulphate from precipitation cast matrices of polycaprolactone. J. Control. Release 2006, 110, 414–421. [Google Scholar] [CrossRef]
- Naraharisetti, P.K.; Lee, H.C.G.; Fu, Y.C.; Lee, D.J.; Wang, C.H. In vitro and in vivo release of gentamicin from biodegradable discs. J. Biomed. Mater. Res. Part B Appl. Biomater. 2006, 77B, 329–337. [Google Scholar] [CrossRef]
- Schmidt, C.; Wenz, R.; Nies, B.; Moll, F. Antibiotic in vivo/in vitro release, histocompatibility and biodegradation of gentamicin implants based on lactic acid polymers and copolymers. J. Control. Release 1995, 37, 83–94. [Google Scholar] [CrossRef]
- Aimin, C.; Chunlin, H.; Juliang, B.; Tinyin, Z.; Zhichao, D. Antibiotic loaded chitosan bar. An in vitro, in vivo study of a possible treatment for osteomyelitis. Clin. Orthop. Relate Res. 1999, 366, 239–247. [Google Scholar] [CrossRef]
- Coraca-Huber, D.C.; Wurm, A.; Fille, M.; Hausdorfer, J.; Nogler, M.; Vogt, S.; Kuhn, K.D. Antibiotic-loaded calcium carbonate/calcium sulfate granules as co-adjuvant for bone grafting. J. Mater. Sci. Mater. Med. 2015, 26, 5344. [Google Scholar] [CrossRef]
- Fleiter, N.; Walter, G.; Bösebeck, H.; Vogt, S.; Büchner, H.; Hirschberger, W.; Hoffmann, R. Clinical use and safety of a novel gentamicin-releasing resorbable bone graft substitute in the treatment of osteomyelitis/osteitis. Bone Joint Res. 2014, 3, 223–229. [Google Scholar] [CrossRef] [PubMed]
- McKee, M.D.; Wild, L.M.; Schemitsch, E.H.; Waddell, J.P. The use of an antibiotic-impregnated, osteoconductive, bioabsorbable bone substitute in the treatment of infected long bone defects: Early results of a prospective trial. J. Orthop. Trauma 2002, 16, 622–627. [Google Scholar] [CrossRef]
- Prasanna, A.P.S.; Venkatasubbu, G.D. Sustained release of amoxicillin from hydroxyapatite nanocomposite for bone infections. Prog. Biomater. 2018, 7, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Geuli, O.; Metoki, N.; Zada, T.; Reches, M.; Eliaz, N.; Mandler, D. Synthesis, coating, and drug-release of hydroxyapatite nanoparticles loaded with antibiotics. J. Mater. Chem. B 2017, 5, 7819–7830. [Google Scholar] [CrossRef]
- Kaya, M.; Şimşek-Kaya, G.; Gürsan, N.; Kireççi, E.; Dayi, E.; Gündoğdu, B. Local treatment of chronic osteomyelitis with surgical debridement and tigecycline-impregnated calcium hydroxyapatite: An experimental study. Oral Surg. Oral Med. Oral. Pathol. Oral Radiol. 2012, 113, 340–347. [Google Scholar] [CrossRef]
- Kattimani, V.S.; Kondaka, S.; Lingamaneni, K.P. Hydroxyapatite: Past, present, and future in bone regeneration. Bone Tissue Regen Insights 2016, 7, 9. [Google Scholar] [CrossRef]
- Barrère, F.; van Blitterswijk, C.A.; de Groot, K. Bone regeneration: Molecular and cellular interactions with calcium phosphate ceramics. Int. J. Nanomed. 2006, 1, 317–332. [Google Scholar]
- Ogose, A.; Kondo, N.; Umezu, H.; Hotta, T.; Kawashima, H.; Tokunaga, K.; Ito, T.; Kudo, N.; Hoshino, M.; Gu, W.; et al. Histological assessment in grafts of highly purified beta-tricalcium phosphate (OSferion) in human bones. Biomaterials 2006, 27, 1542–1549. [Google Scholar] [CrossRef]
- Suwanprateeb, J.; Suvannapruk, W.; Wasoontararat, K. Low temperature preparation of calcium phosphate structure via phosphorization of 3D-printed calcium sulfate hemihydrate based material. J. Mater. Sci. Mater. Med. 2010, 21, 419–429. [Google Scholar] [CrossRef]
- Suwanprateeb, J.; Thammarakcharoen, F.; Wasoontararat, K.; Suvannapruk, W. Influence of printing parameters on the transformation efficiency of 3D-printed plaster of paris to hydroxyapatite and its properties. Rapid Prototyp. J. 2012, 18, 490–499. [Google Scholar] [CrossRef]
- Suwanprateeb, J.; Thammarakcharoen, F.; Phanphiriya, P.; Chokevivat, W.; Suvannapruk, W.; Chernchujit, B. Preparation and characterizations of antibiotic impregnated microporous nano-hydroxyapatite for osteomyelitis treatment. Biomed. Eng.-Appl. Basis Commun. 2014, 26, 1450041. [Google Scholar] [CrossRef]
- Kijartorn, P.; Wongpairojpanich, J.; Thammarakcharoen, F.; Suwanprateeb, J.; Buranawat, B. Clinical evaluation of 3D printed nano-porous hydroxyapatite bone graft for alveolar ridge preservation: A randomized controlled trial. J. Dent. Sci. 2022, 17, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, Y.; Uchida, A.; Yamakawa, T.; Shinto, Y.; Araki, N.; Kato, K. Treatment of chronic osteomyelitis using calcium hydroxyapatite ceramic implants impregnated with antibiotic. Int. Orthop. 1998, 22, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Itokazu, M.; Aoki, T.; Nonomura, H.; Nishimoto, Y.; Itoh, Y. Antibiotic-loaded porous hydroxyapatite blocks for the treatment of osteomyelitis and postoperative infection. A preliminary report. Bull. Hosp. Jt. Dis. 1998, 57, 125–129. [Google Scholar] [PubMed]
- Sudo, A.; Hasegawa, M.; Fukuda, A.; Uchida, A. Treatment of infected hip arthroplasty with antibiotic-impregnated calcium hydroxyapatite. J. Arthroplast. 2008, 23, 145–150. [Google Scholar] [CrossRef]
- Takigami, I.; Ito, Y.; Ishimaru, D.; Ogawa, H.; Mori, N.; Shimizu, T.; Terabayashi, N.; Shimizu, K. Two-stage revision surgery for hip prosthesis infection using antibiotic-loaded porous hydroxyapatite blocks. Arch. Orthop. Trauma Surg. 2010, 130, 1221–1226. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, K.; Itokazu, M.; Uemura, S.; Takigami, I.; Naganawa, T.; Shimizu, K. Successful joint arthroplasty after treatment of destructive MRSA arthritis of the knee using antibiotic-loaded hydroxyapatite blocks: A case report. Arch. Orthop. Trauma Surg. 2007, 127, 47–50. [Google Scholar] [CrossRef]
- Bose, D.; Kugan, R.; Stubbs, D.; McNally, M. Management of infected nonunion of the long bones by a multidisciplinary team. Bone Joint J. 2015, 97-B, 814–817. [Google Scholar] [CrossRef]
- Metsemakers, W.J.; Kuehl, R.; Moriarty, T.F.; Richards, R.G.; Verhofstad, M.H.J.; Borens, O.; Kates, S.; Morgenstern, M. Infection after fracture fixation: Current surgical and microbiological concepts. Injury 2018, 49, 511–522. [Google Scholar] [CrossRef] [PubMed]
- Klemn, K. The use of antibiotic-containing beads chain in the treatment of chronic bone infections. Clin. Microbial. Infect. 2001, 7, 28–31. [Google Scholar] [CrossRef] [PubMed]
- Gauland, C. Managing lower-extremity osteomyelitis locally with surgical debridement and synthetic calcium sulfate antibiotic tablets. Adv. Skin Wound Care 2011, 24, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Calhoun, J.H.; Henry, S.L.; Anger, D.M.; Cobos, J.A.; Mader, J.T. The treatment of infected nonunions with gentamicin-polymethylmethacrylate antibiotic beads. Clin. Orthop. Relat. Res. 1993, 295, 23–27. [Google Scholar] [CrossRef]
- Patzakis, M.J.; Mazur, K.; Wilkins, J.; Sherman, R.; Holtom, P. Septopal beads and autogenous bone grafting for bone defects in patients with chronic osteomyelitis. Clin. Orthop. Relat. Res. 1993, 295, 112–118. [Google Scholar] [CrossRef]
- McNally, M.A.; Ferguson, J.Y.; Scarborough, M.; Ramsden, A.; Stubbs, D.A.; Atkins, B.L. Mid- to long-term results of single-stage surgery for patients with chronic osteomyelitis using a bioabsorbable gentamicin-loaded ceramic carrier. Bone Joint J. 2022, 104-B, 1095–1100. [Google Scholar] [CrossRef]
- Cierny, G., III. Surgical treatment of osteomyelitis. Plast. Reconstr. Surg. 2011, 127 (Suppl. S1), 190S–204S. [Google Scholar] [CrossRef] [PubMed]
- Walenkamp, G.H.; Kleijn, L.L.; de Leeuw, M. Osteomyelitis treated with gentamicin-PMMA beads: 100 patients followed for 1–12 years. Acta Orthop. Scand. 1998, 69, 518–522. [Google Scholar] [CrossRef]
- Kallala, R.; Haddad, F.S. Hypercalcaemia following the use of antibiotic-eluting absorbable calcium sulphate beads in revision arthroplasty for infection. Bone Joint J. 2015, 97-B, 1237–1241. [Google Scholar] [CrossRef]
- Lum, Z.C.; Pereira, G.C. Local bio-absorbable antibiotic delivery in calcium sulfate beads in hip and knee arthroplasty. J. Orthop. 2018, 15, 676–678. [Google Scholar] [CrossRef]
- McPherson, E.; Dipane, M.; Sherif, S. Dissolvable antibiotic beads in treatment of periprosthetic joint infection and revision arthroplasty—The use of synthetic pure calcium sulfate (Stimulan®) impregnated with vancomycin & tobramycin. Reconstr. Rev. 2013, 3, 32–43. [Google Scholar] [CrossRef]
- Chang, W.; Colangeli, M.; Colangeli, S.; Di Bella, C.; Gozzi, E.; Donati, D. Adult osteomyelitis: Debridement versus debridement plus Osteoset T pellets. Acta Orthop. Belg. 2007, 73, 238–243. [Google Scholar]
- Zhao, Z.; Wang, G.; Zhang, Y.; Luo, W.; Liu, S.; Liu, Y.; Zhou, Y.; Zhang, Y. The effect of calcium sulfate/calcium phosphate composite for the treatment of chronic osteomyelitis compared with calcium sulfate. Ann. Palliat. Med. 2020, 9, 1821–1833. [Google Scholar] [CrossRef] [PubMed]
- Kwong, F.N.; Porter, R.M.; Griffin, D.R.; Evans, C.H. Effect of tobramycin on the osteogenesis of stem cells derived from human bone marrow. J. Bone Joint Surg. [Br]. 2009, 91-B (Suppl. SI), 130–131. [Google Scholar]
- Francesca, D.B.; Bancroft, L.W.; Peterson, J.J.; Kransdorf, M.J.; Menke, D.M.; DeOrio, J.K. Imaging characteristics of bone graft materials. RadioGraphics. 2006, 26, 373–388. [Google Scholar] [CrossRef]
- Lavery, L.A.; Ahn, J.; Ryan, E.C.; Bhavan, K.; Oz, O.K.; La Fontaine, J.; Wukich, D.K. What are the optimal cutoff values for ESR and CRP to diagnose osteomyelitis in patients with diabetes-related foot infections? Clin. Orthop. Relat. Res. 2019, 477, 1594–1602. [Google Scholar] [CrossRef]
- Easton, C.R.; Junho, A.; Wukich, D.K.; Kim, P.J.; Fontaine, J.L.; Lavery, L.A. Diagnostic utility of erythrocyte sedimentation rate and C-reactive protein in osteomyelitis of the foot in persons without diabetes. J. Foot Ankle Surg. 2019, 58, 484–488. [Google Scholar] [CrossRef]
- Ghanem, E.; Antoci, V., Jr.; Pulido, L.; Joshi, A.; Hozack, W.; Parvizi, J. The use of receiver operating characteristics analysis in determining erythrocyte sedimentation rate and C-reactive protein levels in diagnosing periprosthetic infection prior to revision total hip arthroplasty. Int. J. Infect. Dis. 2009, 13, e444–e449. [Google Scholar] [CrossRef]
- Greidanus, N.V.; Masri, B.A.; Garbuz, D.S.; Wilson, S.D.; McAlinden, M.G.; Xu, M.; Duncan, C.P. Use of erythrocyte sedimentation rate and C-reactive protein level to diagnose infection before revision total knee arthroplasty. A prospective evaluation. J. Bone Joint Surg. Am. 2007, 89, 1409–1416. [Google Scholar] [CrossRef]
- Lammin, K.; Taylor, J.; Zenios, M. The usefulness of CRP and ESR In diagnosing long bone osteomyelitis in children—Are we being falsely reassured? Orthop. Procs. 2012, 94-B (Suppl. SXXXIX), 156. [Google Scholar]
- Chiang, H.Y.; Chung, C.W.; Kuo, C.C.; Lo, Y.C.; Chang, W.S.; Chi, C.Y. First-4-week erythrocyte sedimentation rate variability predicts erythrocyte sedimentation rate trajectories and clinical course among patients with pyogenic vertebral osteomyelitis. PLoS ONE 2019, 14, e0225969. [Google Scholar] [CrossRef]
- Cohen, G.; Lager, S.; Cece, D.; Rubel, I.F. The social impact associated with chronic osteomyelitis. A grading system for the most frequent complication. Osteosynth. Trauma Care 2004, 12, 74–76. [Google Scholar] [CrossRef]
- Yagdiran, A.; Otto-Lambertz, C.; Lingscheid, K.M.; Sircar, K.; Samel, C.; Scheyerer, M.J.; Zarghooni, K.; Eysel, P.; Sobottke, R.; Jung, N.; et al. Quality of life and mortality after surgical treatment for vertebral osteomyelitis (VO): A prospective study. Eur. Spine J. 2020, 30, 1721–1731. [Google Scholar] [CrossRef]
- Zayzan, K.R.; Yusof, N.M.; Sulong, A.F.; Zakaria, Z.; Rahman, J.A. Functional outcome and quality of life following treatment for post-traumatic osteomyelitis of long bones. Singap. Med. J. 2022, 63, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Wahlig, H.; Dingeldein, E.; Bergmann, R.; Reuss, K. The release of gentamicin from polymethylmethacrylate beads. An experimental and pharmacokinetic study. J. Bone Joint Surg. Br. 1978, 60-B, 270–275. [Google Scholar] [CrossRef]
- Jenny, J.Y.; Jenny, G.; Lambert, J.; Gaudias, J.; Kempf, I. Utility of measurement of gentamicin release from PMMA beads in wound drainage fluid after in-vivo implantation. Acta Orthop. Belg. 1995, 61, 10–13. [Google Scholar]
- Salvati, E.A.; Callaghan, J.J.; Brause, B.D.; Klein, R.F.; Small, R.D. Reimplantation in infection. Elution of gentamicin from cement and beads. Clin. Orthop. 1986, 207, 83–93. [Google Scholar] [CrossRef]
- Livio, F.; Wahl, P.; Csajka, C.; Gautier, E.; Buclin, T. Tobramycin exposure from active calcium sulfate bone graft substitute. BMC Pharmacol Toxicol. 2014, 15, 12. [Google Scholar] [CrossRef]
- Shen, L.; Dong, Y.; Zhang, C.; Guo, Q. Chronic osteomyelitis treatment: A clinical and pharmaco-kinetic study of vancomycin impregnated calcium sulphate. J. Med. Imaging Health Inform. 2014, 5, 36–42. [Google Scholar] [CrossRef]
- Cresswell, T.; Shahane, S.; Stockley, I. Irreducible dislocation of a hip total prosthesis: The risk of gentamicin beads. Orthopedics 2000, 23, 1095–1096. [Google Scholar] [CrossRef]
- Fiddian, N.; Sudlow, R.; Browett, J. Ruptured femoral vein. A complication of the use of gentamicin beads in an infected excision arthroplasty of the hip. J. Bone Joint Surg. Br. 1984, 66, 493–494. [Google Scholar] [CrossRef] [PubMed]
- Clarke, J.; Shalhoub, J.; Das, S.K. Ceramic gentamicin beads in vascular graft infection—A cautionary note. Vasc. Endovasc. Surg. 2013, 47, 76–77. [Google Scholar] [CrossRef] [PubMed]
- Tarar, M.; Khalid, A.; Usman, M.; Javed, K.; Shah, N.; Abbas, M.W. Wound leakage with the use of calcium sulphate beads in prosthetic joint surgeries: A systematic review. Cureus 2021, 13, e19650. [Google Scholar] [CrossRef] [PubMed]
- Ziran, B.H.; Smith, W.R.; Morgan, S.J. Use of calcium-based demineralized bone matrix/allograft for nonunions and posttraumatic reconstruction of the appendicular skeleton: Preliminary results and complications. J. Trauma. 2007, 63, 1324–1328. [Google Scholar] [CrossRef] [PubMed]
- Kelly, C.M.; Wilkins, R.M.; Gitelis, S.; Hartjen, C.; Watson, J.T.; Kim, P.T. The use of a surgical grade calcium sulfate as a bone graft substitute: Results of a multicenter trial. Clin. Orthop. Relat. Res. 2001, 382, 42–50. [Google Scholar] [CrossRef]
- Borrelli, J., Jr.; Prickett, W.D.; Ricci, W.M. Treatment of nonunions and osseous defects with bone graft and calcium sulfate. Clin. Orthop. Relat. Res. 2003, 411, 245–254. [Google Scholar] [CrossRef]
- Smith, I. Convulsions and coma associated with iatrogenically elevated CSF calcium levels post spinal surgery: A case report. Crit. Care Resusc. 2005, 7, 173–176. [Google Scholar]
- Zhou, C.H.; Ren, Y.; Ali, A.; Meng, X.Q.; Zhang, H.A.; Fang, J.; Qin, C.H. Single-stage treatment of chronic localized tibial osteomyelitis with local debridement and antibiotic loaded calcium sulfate implantation: A retrospective study of 42 patients. J. Orthop. Surg. Res. 2020, 15, 201. [Google Scholar] [CrossRef]
- Panteli, M.; Giannoudis, P.V. Chronic osteomyelitis: What the surgeon needs to know. EFORT Open Rev. 2016, 1, 128–135. [Google Scholar] [CrossRef]
- Cunha, B.A. Osteomyelitis in Elderly Patients. Clin. Infect. Dis. 2002, 35, 287–293. [Google Scholar] [CrossRef]
- Leurmarnkul, W.; Meetam, P. Properties testing of the retranslated SF-36 (Thai version). Thai J. Pharm. Sci. 2005, 29, 69–88. [Google Scholar]
- Common Terminology Criteria for Adverse Events (CTCAE). Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm#ctc_60 (accessed on 15 April 2023).




{kind=link}
{kind=link}
{kind=link}
| Characteristics n = 62 | n (%) |
|---|---|
| Sex | |
| Male | 49 (79.0) |
| Female | 13 (21.0) |
| Age (Mean ± SD) | 47.2 ± 14.7 |
| Location | |
| Tibia | 34 (54.8) |
| Femur | 19 (30.6) |
| Humerus | 4 (6.5) |
| Calcaneus | 2 (3.2) |
| Clavicle | 1 (1.6) |
| Forearm | 1 (1.6) |
| Fibula | 1 (1.6) |
| Cierny-Mader Grade | |
| Type I Medullary osteomyelitis | 11 (17.7) |
| Type II Superficial osteomyelitis | 3 (4.8) |
| Type III Localized osteomyelitis | 37 (59.7) |
| Type IV Diffuse osteomyelitis | 11 (17.7) |
| Physiological class | |
| Class A Good immune system and delivery | 47 (75.8) |
| Class B Compromised locally or systemically risk factors | 15 (24.2) |
| Class C requires suppressive or no treatment; minimal disability | 0 (0) |
| Causes | |
| Post-traumatic | 48 (77.4) |
| Hematogones (non-trauma, sepsis) | 14 (22.6) |
| Previous surgery for this condition | |
| 0 | 15 (24.2) |
| 1 | 19 (30.6) |
| 2 | 13 (21.0) |
| 3 | 8 (12.9) |
| 4 | 2 (3.2) |
| 5 | 2 (3.2) |
| 6 | 1 (1.6) |
| >7 | 2 (3.2) |
| Risk factor | |
| No risk factor | 41 (66.1) |
| Risk | 21 (33.9) |
| Major risk factor: cellulitis or abscess formation | 5 (23.8) |
| Minor systemic risk factor: subject had smoking history | 7 (33.3) |
| Minor systemic risk factor: diabetes mellitus | 3 (14.3) |
| Minor systemic risk factor: anemia | 2 (9.5) |
| Minor systemic risk factor: chronic lung disease | 1 (4.8) |
| Minor local risk factor: poor soft tissue requiring flap | 9 (42.9) |
| Minor local risk factor: adjacent joint stiff/arthritic | 7 (33.3) |
| Minor local risk factor: heterotopic ossification | 1 (4.8) |
| Surgery Data | Quantity (Median, IQR (Min-Max)) |
|---|---|
| d | 93, 57 |
| Number of antibiotics loaded hydroxyapatite beads used | 60, 54 (6–180) |
| Gentamicin beads | 20, 18 (2–60) |
| Vancomycin beads | 20, 20 (2–60) |
| Fosfomycin beads | 20, 20 (2–60) |
| Cultured organism | n (%) |
| No | 3 (4.8) |
| Yes | 59 (95.2) |
| No growth | 28 (47.5) |
| Cultured organism (2 organisms found) | 7 (11.9) |
| Acinetobactor baumannii and E. coli (ESBL-Producing) | 1 (14.3) |
| Acinetobactor baumannii and Pseudomonas aeruginosa | 1 (14.3) |
| Morganella morganii and Klebsiella pneumoniae (MDR) | 1 (14.3) |
| Pseudomonas aeruginosa (MDR) and Staphylococcus haemolyticus (MR-CoNS) | 1 (14.3) |
| Pseudomonas aeruginosa and Enterococcus avium | 1 (14.3) |
| Pseudomonas aeruginosa and Shewanella putrefaciens | 1 (14.3) |
| Staphylococcus aureus and Staphylococcus epidermidis | 1 (14.3) |
| Cultured organism (1 organism found) | 24 (40.7) |
| Pseudomonas aeruginosa | 9 (37.5) |
| Staphylococcus aureus | 4 (16.7) |
| Staphylococcus aureus (MRSA) | 1 (4.2) |
| Aerobic culture | 1 (4.2) |
| Aerococcus viridans | 1 (4.2) |
| Coagulase Negative Staphylococci | 2 (8.4) |
| Enterobacter cloacae | 1 (4.2) |
| Enterococcus faecalis | 1 (4.2) |
| Serratia marcescens | 1 (4.2) |
| Staphylococcus cohnii | 1 (4.2) |
| Staphylococcus haemolyticus | 1 (4.2) |
| Staphylococcus hominis | 1 (4.2) |
| Vancomycin sensitivity (n = 38) | |
| Sensitive | 8 (21.1) |
| Intermediate | 0 (0) |
| Resistant | 0 (0) |
| Results not reported by hospital lab | 30 (78.9) |
| Gentamicin sensitivity (n = 38) | |
| Sensitive | 19 (50) |
| Intermediate | 1 (2.6) |
| Resistant | 4 (10.5) |
| Results not reported by hospital lab | 14 (36.8) |
| Fosfomycin sensitivity (n = 38) | |
| Sensitive | 9 (23.7) |
| Intermediate | 1 (2.6) |
| Resistant | 2 (5.3) |
| Results not reported by hospital lab | 26 (68.4) |
| Results | Baseline Mean ± SD | 8 Weeks Mean ± SD | 12 Weeks Mean ± SD | 24 Weeks Mean ± SD | 48 Weeks Mean ± SD |
|---|---|---|---|---|---|
| Liver function test | |||||
| AST (SGOT) (U/L) | 29.31 ± 13.85 | 30.25 ± 16.02 | 27.53 ± 12.04 | 31.08 ± 14.85 | 29.37 ± 14.75 |
| ALT (SGPT) (U/L) | 32.78 ± 29.95 | 34.5 ± 29.32 | 28.81 ± 24.86 | 31.67 ± 22.80 | 27.07 ± 19.47 |
| Alkaline Phosphatase (ALP) (U/L) | 103.36 ± 47.29 | 103.81 ± 34.84 | 97.96 ± 32.60 | 94.37 ± 33.25 | 83.44 ± 25.98 |
| Renal function test | |||||
| Serum Creatinine (mg/dL) | 0.81 ± 0.20 | 0.85 ± 0.25 | 1.13 ± 1.74 | 0.85 ± 0.21 | 0.88 ± 0.20 # |
| eGFR (ml/min/1.73 m2) | 103.11 ± 21.84 | 97.67 ± 25.52 # | 98.55 ± 23.59 # | 100.46 ± 19.9 | 96.58 ± 20.86 # |
| BUN (mg/dL) | 14.03 ± 13.28 | 12.24 ± 4.47 | 11.65 ± 3.64 | 13.22 ± 4.28 | 12.90 ± 3.80 |
| C-reactive protein (CRP) (mg/dL) | 12.30 ± 27.82 | 3.96 ± 4.86 | 3.12 ± 4.52 # | 2.7 ± 4.11 # | 2.45 ± 2.65 # |
| Erythrocyte sedimentation rate (ESR) (mm/hour) | 45.11 ± 32.83 | 40.09 ± 26.53 | 27.37 ± 21.68 # | 26.72 ± 27.67 # | 25.13 ± 26.70 # |
| Antibiotics | Duration (h) | Concentration (µg/mL) Mean ± SD | |
|---|---|---|---|
| Wound drainage fluid | Vancomycin | 24 | 128.64 ± 134.49 |
| 48 | 175.79 ± 153.96 | ||
| 72 | 125.43 ± 159.87 | ||
| Gentamicin | 24 | 412.04 ± 646.01 | |
| 48 | 53.03 ± 74.06 | ||
| 72 | 58.41 ± 97.81 | ||
| Serum | Vancomycin | 24 | 4.00 ± 0.00 |
| 48 | 2.67 ± 2.31 | ||
| 72 | 6.94 ± 4.16 | ||
| Gentamicin | 24 | 0.38 ± 0.17 | |
| 48 | 0.36 ± 0.12 | ||
| 72 | 0.40 ± 0.00 |
| Results | Baseline Mean ± SD | 6 Weeks Mean ± SD | 12 Weeks Mean ± SD | 24 Weeks Mean ± SD |
|---|---|---|---|---|
| Physical health | 37.14 ± 4.23 | 47.94 ± 14.77 # | 55.51 ± 13.78 # | 60.63 ± 14.64 # |
| Physical functioning | 46.86 ± 26.10 | 50.49 ± 26.91 | 63.98 ± 26.12 # | 72.93 ± 23.49 # |
| Role-physical | 5.27 ± 8.14 | 11.52 ± 10.71 # | 14.29 ± 10.67 # | 16.98 ± 9.65 # |
| Bodily pain | 46.96 ± 26.56 | 64.39 ± 20.34 # | 73.47 ± 18.29 # | 78.89 ± 19.95 # |
| General health | 49.45 ± 19.50 | 65.35 ± 17.69 # | 70.31 ± 16.84 # | 73.72 ± 17.99 # |
| Mental health | 47.44 ± 17.48 | 58.99 ± 14.12 # | 64.81 ± 12.83 # | 67.21 ± 13.63 # |
| Vitality | 66.79 ± 24.48 | 80.76 ± 21.24 | 87.88 ± 19.53 # | 91.44 ± 20.89 # |
| Social function | 56.62 ± 25.54 | 67.40 ± 20.78 | 75.00 ± 19.09 # | 80.16 ± 19.82 # |
| Role- emotional | 7.35 ± 9.67 | 15.03 ± 10.41 # | 17.01 ± 10.06 # | 18.12 ± 10.14 # |
| Mental health | 58.98 ± 21.99 | 72.78 ± 14.24 # | 79.35 ± 12.09 # | 79.13 ± 13.38 # |
| Relations to nHA-ATB Beads | Adverse Events (n = 20) | ||
|---|---|---|---|
| SAE or Non-SAE | Severity | Events | |
| Definitely related | |||
| - HA exposed from wound dehiscence | Non-SAE | Grade I | 1 |
| Possibly related | |||
| - Serum oozing from the surgical wound | Non- SAE | Grade I | 1 |
| - Acute on-top chronic left tibia osteomyelitis | SAE | Grade III | 1 |
| Unlikely | |||
| - Anterior shoulder dislocation | Non-SAE | Grade II | 1 |
| - Loosening of external fixator | SAE | Grade I | 1 |
| - Gastrointestinal hemorrhage, unspecified | SAE | Grade II | 1 |
| Not related | |||
| - Leg pain | Non-SAE | Grade I | 1 |
| - Wrist drop due to radial nerve palsy | Non-SAE | Grade II | 1 |
| - Acute pyelonephritis | SAE | Grade I | 1 |
| - Adjust external fixation | SAE | Grade I | 1 |
| - Bone fracture | SAE | Grade I | 1 |
| - Prolonged hospitalization of chronic osteomyelitis of left distal femur due to financial problem | SAE | Grade I | 1 |
| - Revised external fixation | SAE | Grade I | 1 |
| - Wound dehiscence | SAE | Grade I | 2 |
| - Surgical wound with drainage | SAE | Grade II | 1 |
| - Wound dehiscence after debridement and switch HA-ATB to cement ATB | SAE | Grade II | 1 |
| - Broken Steinman Pin | SAE | Grade III | 1 |
| - Nonunion of the fracture site | SAE | Grade IV | 1 |
| - Death from other causes | SAE | Grade V | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiamton, C.; Apivatgaroon, A.; Aunaramwat, S.; Chawalitrujiwong, B.; Chuaychoosakoon, C.; Suwannaphisit, S.; Jirawison, C.; Iamsumang, C.; Kongmalai, P.; Sukvanich, P.; et al. Efficacy and Safety of Antibiotic Impregnated Microporous Nanohydroxyapatite Beads for Chronic Osteomyelitis Treatment: A Multicenter, Open-Label, Prospective Cohort Study. Antibiotics 2023, 12, 1049. https://doi.org/10.3390/antibiotics12061049
Jiamton C, Apivatgaroon A, Aunaramwat S, Chawalitrujiwong B, Chuaychoosakoon C, Suwannaphisit S, Jirawison C, Iamsumang C, Kongmalai P, Sukvanich P, et al. Efficacy and Safety of Antibiotic Impregnated Microporous Nanohydroxyapatite Beads for Chronic Osteomyelitis Treatment: A Multicenter, Open-Label, Prospective Cohort Study. Antibiotics. 2023; 12(6):1049. https://doi.org/10.3390/antibiotics12061049
Chicago/Turabian StyleJiamton, Chittawee, Adinun Apivatgaroon, Saree Aunaramwat, Banchai Chawalitrujiwong, Chaiwat Chuaychoosakoon, Sitthiphong Suwannaphisit, Choen Jirawison, Chonlathan Iamsumang, Pinkawas Kongmalai, Pawaris Sukvanich, and et al. 2023. "Efficacy and Safety of Antibiotic Impregnated Microporous Nanohydroxyapatite Beads for Chronic Osteomyelitis Treatment: A Multicenter, Open-Label, Prospective Cohort Study" Antibiotics 12, no. 6: 1049. https://doi.org/10.3390/antibiotics12061049