
Evaluating the Counseling Standards and Ability of Pharmacy Staff to Detect Antibiotic-Drugs Interactions: A Simulated Client Study from Pakistan

 , ,
, ,
Abstract
:1. Introduction
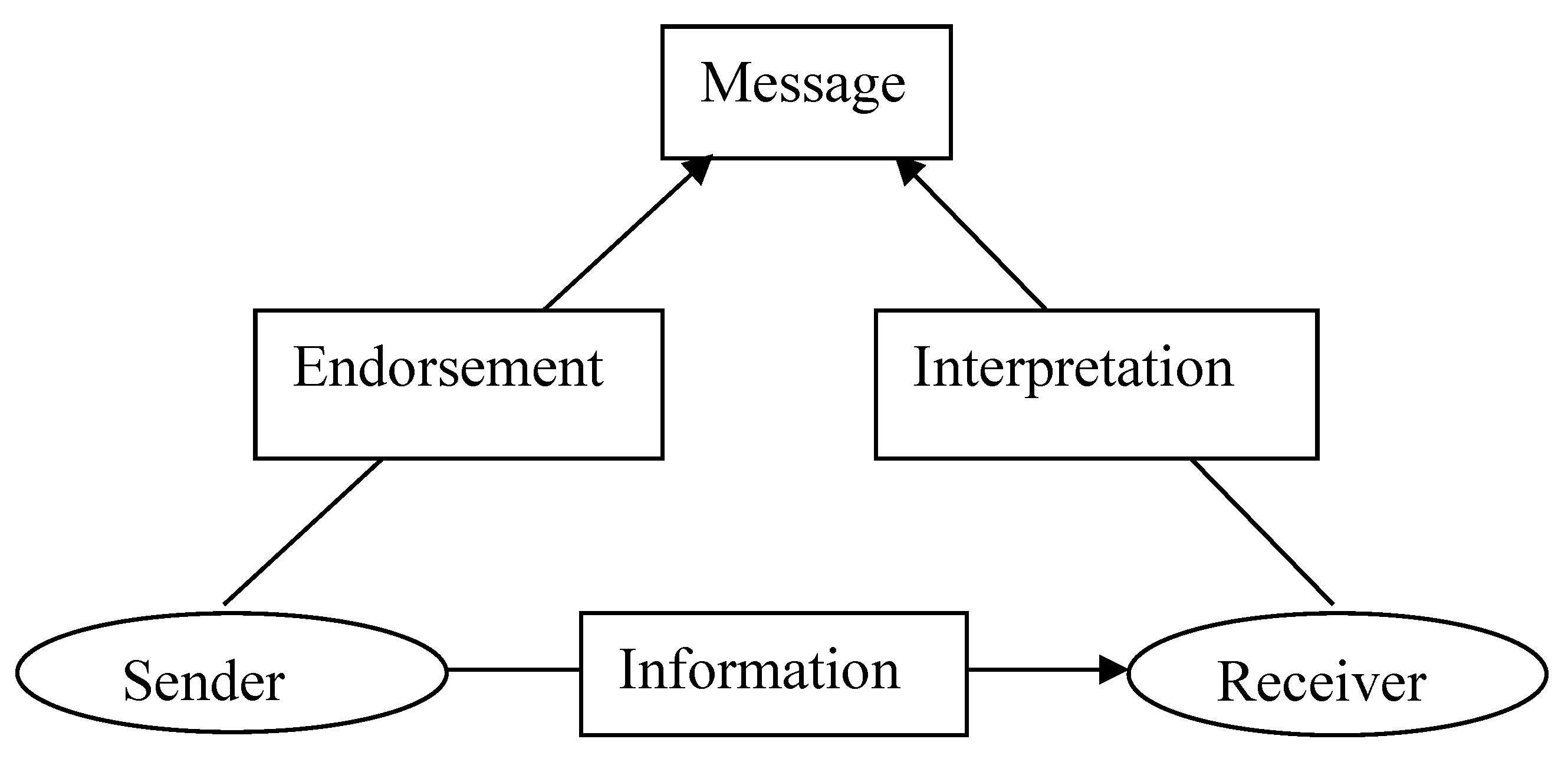
Theories and Conceptual Framework
2. Methods
2.1. Simulated Clients
2.2. Communication Skills Assessment
2.3. Pilot Study
2.4. Documentation of Feedback
2.5. Study Setting
2.6. Pharmacy Selection
2.7. Scenarios
Scenario 1
Scenario 2
2.8. Ethical Considerations
2.9. Data Analysis
3. Results
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yang, S.; Kim, D.; Choi, H.J.; Chang, M.J. A comparison of patients’ and pharmacists’ satisfaction with medication counseling provided by community pharmacies: A cross-sectional survey. BMC Health Serv. Res. 2016, 16, 131. [Google Scholar] [CrossRef]
- Kashour, T.S.; Joury, A.; Alotaibi, A.M.; Althagafi, M.; Almufleh, A.S.; Hersi, A.; Thalib, L. Quality of assessment and counselling offered by community pharmacists and medication sale without prescription to patients presenting with acute cardiac symptoms: A simulated client study. Eur. J. Clin. Pharm. 2015, 72, 321–328. [Google Scholar] [CrossRef]
- Berger, K.; Eickhoff, C.; Schulz, M. Counseling quality in community pharmacies: Implementation of the pseudo customer methodology in Germany. J. Clin. Pharm. Ther. 2005, 30, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, A.T.; Roque, F.; Gonzalez, C.; Soares, S.; Figueiras, A.; Herdeiro, M.T. Improving Antibiotic Use through Educational Interventions. Microbial Pathogens and Strategies For Combating Them: Science, Technology and Education. Available online: www.formatex.info/microbiology4/vol3/1706-1714.pdf (accessed on 12 February 2023).
- Palaian, S.; Prabhu, M.; Shankar, P.R. Patient counseling by pharmacist—A focus on chronic illness. Pak. J. Pharm. Sci. 2006, 19, 65–72. [Google Scholar] [PubMed]
- Okumura, L.M.; Rotta, I.; Correr, C.J. Assessment of pharmacist-led patient counseling in randomized controlled trials: A systematic review. Pharm. Weekbl. 2014, 36, 882–891. [Google Scholar] [CrossRef] [PubMed]
- Alaqeel, S.; Abanmy, N.O. Counseling practices in community pharmacies in Riyadh, Saudi Arabia: A cross-sectional study. BMC Health Serv. Res. 2015, 15, 557. [Google Scholar] [CrossRef]
- Hussain, A.; Ibrahim, M.I.M. Medication counselling and dispensing practices at community pharmacies: A comparative cross sectional study from Pakistan. Pharm. Weekbl. 2011, 33, 859–867. [Google Scholar] [CrossRef] [PubMed]
- Al Aqeel, S.; Abanmy, N.; Alshaya, H.; AlMeshari, A. Interventions for improving pharmacist-led patient counselling in the community setting: A systematic review. Syst. Rev. 2018, 7, 1–13. [Google Scholar] [CrossRef]
- Kheir, N. Pharmacy Practice in Qatar. Elsevier Inc. Available online: https://www.sciencedirect.com/science/article/pii/B9780128017142000125 (accessed on 12 February 2023).
- Medication Errors Cause Half a Million Deaths in Pakistan, Say Pharmacists. Available online: https://www.dawn.com/news/1362951 (accessed on 12 February 2023).
- Del Arco, A.; Tortajada, B.; de la Torre, J.; Olalla, J.; Padra, J.L.; Montiel, N.; García-Alegría, J. Results of a counselling programme in antibiotic treatment in a secondary hospital. Rev. Esp. Quimioter. 2011, 24, 96–98. [Google Scholar] [PubMed]
- WHO 2014. The Role of Pharmacist in Encouraging Prudent Use of Antibiotics and Averting Antimicrobial Resistance: A Review Ofpol-Icy and Experience. Available online: http://apps.who.int/medicinedocs/en/m/abstract/Js22244en/ (accessed on 12 February 2023).
- Bradley, J.; Langford, A.M. Morris. Is it time to stop counselling patients to “finish the course of antibiotics”? Can. Pharm. J. 2017, 150, 349–350. [Google Scholar]
- Pai, M.P.; Momary, K.M.; Rodvold, K.A. Antibiotic drug interactions. Med. Clin. N. Am. 2006, 90, 1223–1255. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.H.; Coombes, I. Mortality from common drug interactions systems, knowledge and clinical reasoning to optimise prescribing. Intern. Med. J. 2014, 44, 621–622. [Google Scholar] [CrossRef]
- Ashdown, H.F.; Räisänen, U.; Wang, K.; Ziebland, S.; Harnden, A. Prescribing antibiotics to ‘at-risk’ children with influenza-like illness in primary care: Qualitative study. BMJ Open 2016, 6, e011497. [Google Scholar] [CrossRef] [PubMed]
- Beckett, C.; Harbarth, S.; Huttner, B. Special considerations of antibiotic prescription in the geriatric population. Clin. Microbiol. Infect. 2015, 21, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Ansari, J. Drug Interaction and Pharmacist. J. Young -Pharm. 2010, 2, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Aziz, M.M.; Masood, I.; Yousaf, M.; Saleem, H.; Ye, D.; Fang, Y. Pattern of medication selling and self-medication practices: A study from Punjab, Pakistan. PLoS ONE 2018, 13, e0194240. [Google Scholar] [CrossRef]
- Babar, Z.D.; Jamshed, S. Social pharmacy strengthening clinical pharmacy: Why pharmaceutical policy research is needed in Paki-stan? Pharm. World Sci. 2008, 30, 617–619. [Google Scholar] [CrossRef]
- Hussain, A.; Malik, M.; Toklu, H.Z. A literature review: Pharmaceutical care an evolving role at community pharmacies in Pakistan. Pharmacol. Pharm. 2013, 4, 425–630. [Google Scholar] [CrossRef]
- Khalid, L.; Mahsood, N.; Ali, I. The public health problem of OTC antibiotics in developing nations. Res. Soc. Adm. Pharm. 2016, 12, 801–802. [Google Scholar] [CrossRef]
- Rabbani, F.; Cheema, F.H.; Talati, N.; Siddiqui, S.; Syed, S.; Bashir, S.; Zuberi, L.Z.; Shamim, A.; Mumtaz, Q. Behind the counter: Pharmacies and dispensing patterns of pharmacy attendants in Karachi. J. Pak. Med. Assoc. 2001, 51, 149–153. [Google Scholar] [PubMed]
- Tully, M.P.; Beckman-Gyllenstrand, A.; Bernsten, C.B. Factors predicting poor counselling about prescription medicines in Swedish community pharmacies. Patient Educ. Couns. 2011, 83, 3–6. [Google Scholar] [CrossRef]
- Shah, B.; Chewning, B. Conceptualizing and measuring pharmacist-patient communication: A review of published studies. Res. Soc. Adm. Pharm. 2006, 2, 153–185. [Google Scholar] [CrossRef] [PubMed]
- Puspitasari, H.P.; Aslani, P.; Krass, I. A review of counseling practices on prescription medicines in community pharmacies. Res. Soc. Adm. Pharm. 2009, 5, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Airaksinen, M. The role of communication skills: Developing patient-centred practice in community pharmacies. Chronic III 2004, 8, 10–14. [Google Scholar]
- Watson, M.C.; Norris, P.; Granas, A.G. A systematic review of the use of simulated patients and pharmacy practice research. Int. J. Pharm. Pr. 2006, 14, 83–93. [Google Scholar] [CrossRef]
- Specialized Healthcare & Medical Education Department (SHMED). Available online: http://health.punjab.gov.pk/ (accessed on 12 February 2023).
- Raosoft Inc. RaoSoft Sample Size Calculator. 2004. Available online: http://www.raosoft.com/samplesize.html (accessed on 1 June 2020).
- Adepu, R.; Nagavi, B. Attitudes and behaviors of practicing community pharmacists towards patient counselling. Indian J. Pharm. Sci. 2009, 71, 285–289. [Google Scholar] [CrossRef]
- Offor, I.; Enato, E. Patients’ Assessment of Pharmacists’ Medication Counseling in a Psychiatric Hospital in Nigeria. Trop. J. Pharm. Res. 2011, 10, 507–516. [Google Scholar] [CrossRef]
- Ibrahim, M.I.; Palaian, S.; Al-Sulaiti, F.; El-Shami, S. Evaluating community pharmacy practice in Qatar using simulated patient method: Acute gastroenteritis management. Pharm. Pract. 2016, 14, 1–8. [Google Scholar] [CrossRef]
- Horvat, N.; Koder, M.; Kos, M. Using the Simulated Patient Methodology to Assess Paracetamol-Related Counselling for Headache. PLoS ONE 2012, 7, e52510. [Google Scholar] [CrossRef]
- Chua, S.S.; Ramachandran, C.D.; Paraidathathu, T.T. Response of community pharmacists to the presentation of back pain: A simulated patient study. Int. J. Pharm. Pract. 2006, 14, 171–178. [Google Scholar] [CrossRef]
- Kline, J.M.; Wietholter, J.P.; Kline, V.T.; Confer, J. Pediatric Antibiotic Use: A focused review of Fluoroquinolones and Tetracyclines. US Pharm. 2012, 37, 59. Available online: https://www.uspharmacist.com/article/pediatric-antibiotic-use-a-focused-review-of-fluoroquinolones-and-tetracyclines (accessed on 12 February 2023).
- Masters, K.P.; Carr, B.M. Survey of pharmacists and physicians on drug interactions between combined oral contraceptives and broad-spectrum antibiotics. Pharm. Pract. 2009, 7, 139–144. [Google Scholar] [CrossRef]
- Weller, T.M.A.; Jamieson, C.E. The expanding role of the antibiotic pharmacist. J. Antimicrob. Chemother. 2004, 54, 295–298. [Google Scholar] [CrossRef]
- Alfadl, A.A.; Musaad, A.A.; Alhassun, S. Evaluation of medication counseling practice at community pharmacies in Qassim region, Saudi Arabia. Saudi Pharm. J. 2018, 26, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.; McCombs, J.S.; Cheng, R.A.; Johnson, K.A. Pharmacist time requirements for counseling in an outpatient pharmacy. Am. J. Health Pharm. 2002, 59, 2346–2355. [Google Scholar] [CrossRef] [PubMed]
- Anwar, K.; Antibiotic Resistance: It’s Bug-ging. The Express Tribune. 26 April 2015. Available online: https://tribune.com.pk/story/874147/antibiotic-resistance-its-bug-ging/ (accessed on 12 February 2023).
- Tips for Proper Storage of Medications (TPSM). Available online: https://www.opatoday.com/medication-storage-tips (accessed on 12 February 2023).
- WHO 2003, Guidelines for the Storage of Essential Medicines and Other Health Commodities. Available online: http://apps.who.int/medicinedocs/en/d/Js4885e/6.5.html (accessed on 12 February 2023).
- Hawke, K.L.; McGuire, T.; Ranmuthugala, G.; Van Driel, M.L. What do consumers want to know about antibiotics? Analysis of a medicines call centre database. Fam. Pract. 2015, 33, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Ayalew, M. Medication Counseling Practice in Ethiopia: A Systematic Review. J. Basic Clin. Pharm. 2017, 8, 1–5. [Google Scholar]
- Ejeta, F.; Feyisa, D.; Kebede, O.; Aferu, T.; Siraj, J.; Feyissa, D.; Wodajo, E.; Tamiru, A. Medication Counseling Practices in Medicine Retail Outlets Found in Bench Sheko Zone, Southern Nations, Nationalities, and Peoples’ Region, South West Ethiopia. Pragmatic Obs. Res. 2021, 12, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.K.; Edelman, A.; Jensen, J. Patient satisfaction and the impact of written material about postpartum contraceptive decisions. Am. J. Obstet. Gynecol. 2003, 188, 1202–1204. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Category | Scenario 1 (n = 554) | Scenario 2 (n = 465) | Overall % |
|---|---|---|---|---|
| n (%) | n (%) | |||
| Class of pharmacy (Number of the sale counters reported by SCs) | 1 | 334 (60.3) | 287 (61.7) | 61 |
| 2–5 | 204 (36.8) | 164 (35.3) | 36.1 | |
| >5 | 16 (2.9) | 14 (3.0) | 2.9 | |
| Number of employees at the time of visit as reported by SCs | 1–5 | 389 (70.2) | 335 (72.1) | 71.2 |
| 6–10 | 156 (28.1) | 125 (26.8) | 27.5 | |
| >10 | 9 (1.6) | 5 (1.1) | 1.4 | |
| Gender of pharmacy retailers (contacted) | Male | 554 (100.0) | 465 (100.0) | 100.0 |
| Female | 0 (0.0) | 0 (0.0) | 0.0 | |
| Age of contacted retailer (years), estimated by SC | <25 | 19 (3.4) | 21 (4.5) | 3.9 |
| 25–35 | 164 (29.6) | 153 (32.9) | 31.3 | |
| 36–45 | 112 (20.2) | 140 (30.1) | 25.2 | |
| 46–55 | 202 (36.5) | 123 (26.5) | 31.5 | |
| >55 | 57 (10.3) | 28 (6.0) | 8.2 | |
| Day of the visit | Monday | 38 (6.8) | 65 (13.9) | 10.4 |
| Tuesday | 59 (10.6) | 42 (9.0) | 9.8 | |
| Wednesday | 110 (19.8) | 86 (18.5) | 19.1 | |
| Thursday | 79 (14.2) | 32 (6.9) | 10.6 | |
| Friday | 58 (10.5) | 101 (21.7) | 16.1 | |
| Saturday | 66 (11.9) | 70 (15.2) | 13.6 | |
| Sunday | 144 (25.9) | 69 (14.8) | 20.4 | |
| Time of visit | 8:00–12:00 | 146 (26.4) | 167 (35.9) | 31.1 |
| 12:00–14:00 | 35 (6.3) | 67(14.4) | 10.4 | |
| 14:00–22:00 | 373 (67.3) | 231 (49.7) | 58.5 | |
| Number of waiting customers | 0–5 | 361 (65.2) | 338 (72.7) | 68.9 |
| 6–10 | 184 (33.2) | 120 (25.8) | 29.5 | |
| >10 | 9 (1.6) | 7 (1.5) | 1.6 | |
| Waiting time (mints) | 1–5 | 224 (40.4) | 232 (49.9) | 45.2 |
| >5 | 330 (59.6) | 233 (50.1) | 54.8 | |
| Total time of conversation (talk about medication) (mints) | ≤2 | 311 (56.1) | 284 (61.0) | 58.6 |
| 3–5 | 234 (42.2) | 175 (37.6) | 39.9 | |
| >5 | 9 (1.7) | 6 (1.3) | 1.5 | |
| Privacy during conversation | Full provided | 1 (0.2) | 0 (0.0) | 0.09 |
| Semi provided | 17 (3.1) | 4 (0.9) | 2.0 | |
| Not provided | 536 (96.7) | 461 (99.1) | 97.9 |
| Response | Scenario 1 (n = 554) n (%) | Scenario 2 (n = 465) n (%) | Overall % | |
|---|---|---|---|---|
| Counseling without demand | 2 (0.3) | 32 (6.8) | 3.6 | |
| On demand counseling | Provided | 256 (46.2) | 204 (43.8) | 45 |
| Questioning and advised to contact a doctor | 179 (32.3) | 184 (39.5) | 35.9 | |
| Directly advised to contact a doctor | 117 (21.1) | 45 (9.6) | 15.4 | |
| Questions Asked | Scenario 1 (n = 437) n (%) | Scenario 2 (n = 420) n (%) | Overall % |
|---|---|---|---|
| Duration of disease or therapy | 301 (68.8) | 97 (23.0) | 45.9 |
| Whether had taken medicine before | 195 (44.6) | 161 (38.3) | 45.5 |
| Why the medicine was prescribed | - | 91 (21.6) | 21.6 *1 |
| Any co-morbidity or its treatment? | 287 (65.6) | 81 (19.2) | 42.4 |
| Any allergy to medicine in history? | 79 (18.0) | 55 (13.0) | 15.5 |
| Do you know how to take medicine? | 15 (3.4) | 76 (18.0) | 10.7 |
| You want to ask anything else? | 3 (0.7) | 18 (4.2) | 2.5 |
| Information Provided | Scenario 1 (n = 258) n (%) | Scenario 2 (n = 236) n (%) | Overall% |
|---|---|---|---|
| The name of the medicine discussed | - | 13 (5.5) | 5.5 *1 |
| Drug storage | 0 (0.0) | 0 (0.0) | 0.0 |
| How to take the medication (e.g., with/before/after meal) | 7 (2.7) | 12 (5.1) | 3.9 |
| Discussed root of drug administration | 0 (0.0) | 9 (3.8) | 1.9 |
| Dose of therapy | 219 (84.9) | 185 (78.4) | 81.6 |
| Duration of therapy | 107 (41.4) | 173 (73.3) | 57.4 |
| Possible side effects of therapy | 2 (0.8) | 3 (1.3) | 1.1 |
| Possible drug-drug interaction | 4 (1.5) | 3 (1.3) | 1.4 |
| Life style modification or dietary instruction | 113 (43.8) | 153 (64.8) | 54.3 |
| Any other special warnings or precautions about medication | 4 (1.5) | 3 (1.3) | 1.4 |
| Non compliance to medication and its effect | 0 (0.0) | 0 (0.0) | 0.0 |
| Effect of medicine withdrawal | 0(0.0) | 0(0.0) | 0.0 |
| Other medication during this therapy | 0 (0.0) | 0 (0.0) | 0.0 |
| Reinsured that client understand all instructions | 49 (18.9) | 16 (6.8) | 12.8 |
| Advice to change medication | 4 (1.5) | 3 (1.2) | 1.4 |
| Skill Used | Scenario 1 (n = 258) | Scenario 2 (n = 236) | Overall (n = 494) |
|---|---|---|---|
| Eye contact | 2.3 ± 0.4 | 2.2 ± 0.5 | 2.25 ± 0.4 |
| Attention to customer | 2.5 ± 0.4 | 2.3 ± 0.4 | 2.4 ± 0.4 |
| Engagement of customer | 2.2 ± 0.3 | 2.2 ± 0.3 | 2.2 ± 0.3 |
| Non-verbal expressions used | 1.4 ± 0.2 | 1.4 ± 0.3 | 1.4 ± 0.2 |
| Provided written information | 1.1 ± 0.3 | 1.1 ± 0.4 | 1.1 ± 0.3 |
| Factors | Scenario 1 | Scenario 2 |
|---|---|---|
| Number of employees at the time of visit | 0.294 | 0.387 |
| Age of pharmacy retailer (contacted) | 0.013 | 0.656 |
| Day of visit | 0.178 | 0.614 |
| Time of visit | 0.627 | 0.952 |
| Number of waiting customers | 0.834 | 0.043 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aziz, M.M.; Rasool, M.F.; Alanazi, M.; Alharby, T.N.; Alanazi, J.; Huwaimel, B. Evaluating the Counseling Standards and Ability of Pharmacy Staff to Detect Antibiotic-Drugs Interactions: A Simulated Client Study from Pakistan. Antibiotics 2023, 12, 931. https://doi.org/10.3390/antibiotics12050931
Aziz MM, Rasool MF, Alanazi M, Alharby TN, Alanazi J, Huwaimel B. Evaluating the Counseling Standards and Ability of Pharmacy Staff to Detect Antibiotic-Drugs Interactions: A Simulated Client Study from Pakistan. Antibiotics. 2023; 12(5):931. https://doi.org/10.3390/antibiotics12050931
Chicago/Turabian StyleAziz, Muhammad Majid, Muhammad Fawad Rasool, Muteb Alanazi, Tareq Nafea Alharby, Jowaher Alanazi, and Bader Huwaimel. 2023. "Evaluating the Counseling Standards and Ability of Pharmacy Staff to Detect Antibiotic-Drugs Interactions: A Simulated Client Study from Pakistan" Antibiotics 12, no. 5: 931. https://doi.org/10.3390/antibiotics12050931