
Socioeconomic and Governance Factors Disentangle the Relationship between Temperature and Antimicrobial Resistance: A 10-Year Ecological Analysis of European Countries

Abstract
:1. Introduction
2. Results
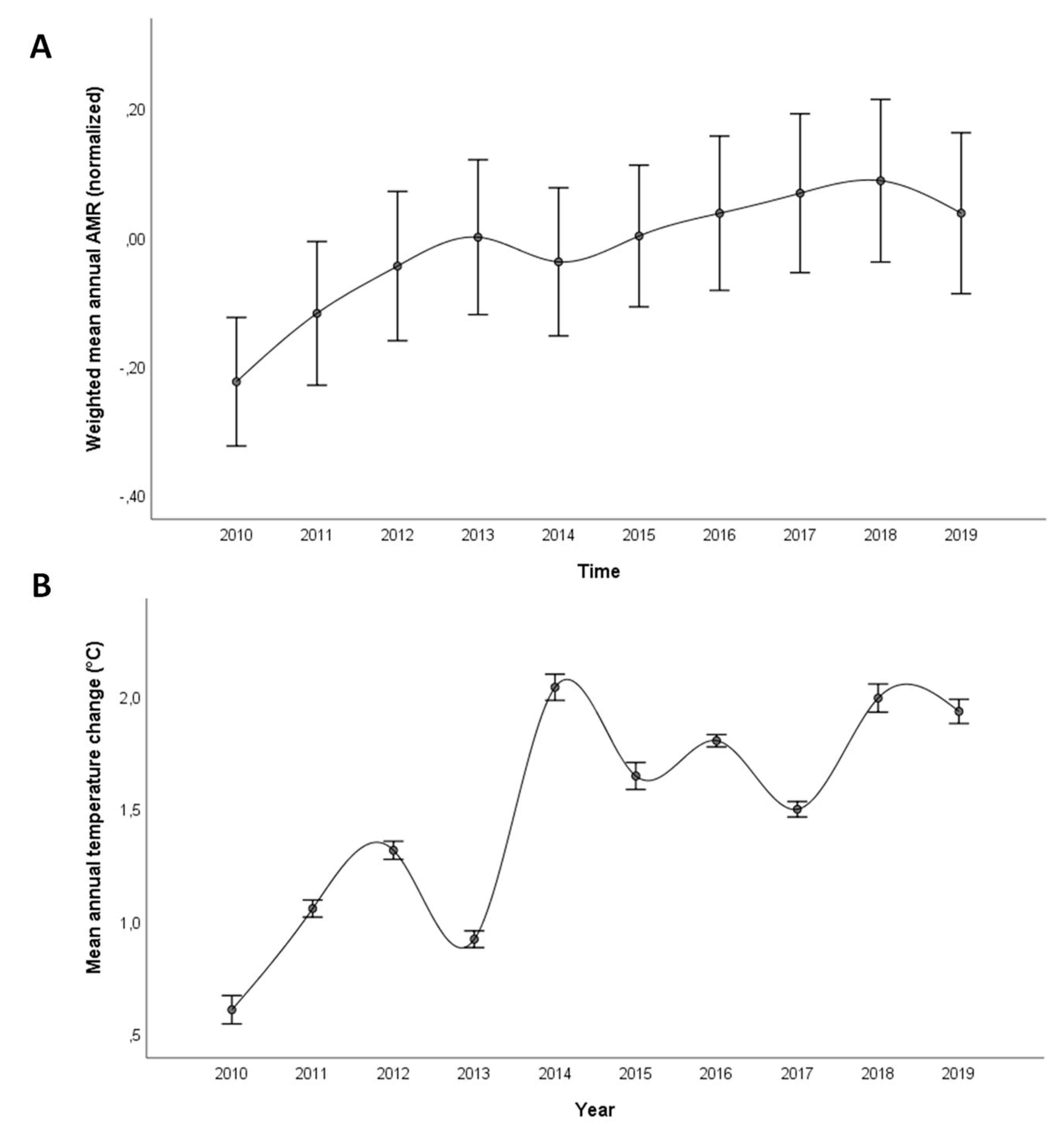
2.1. Trend of AMR and Temperature Changes across European Countries
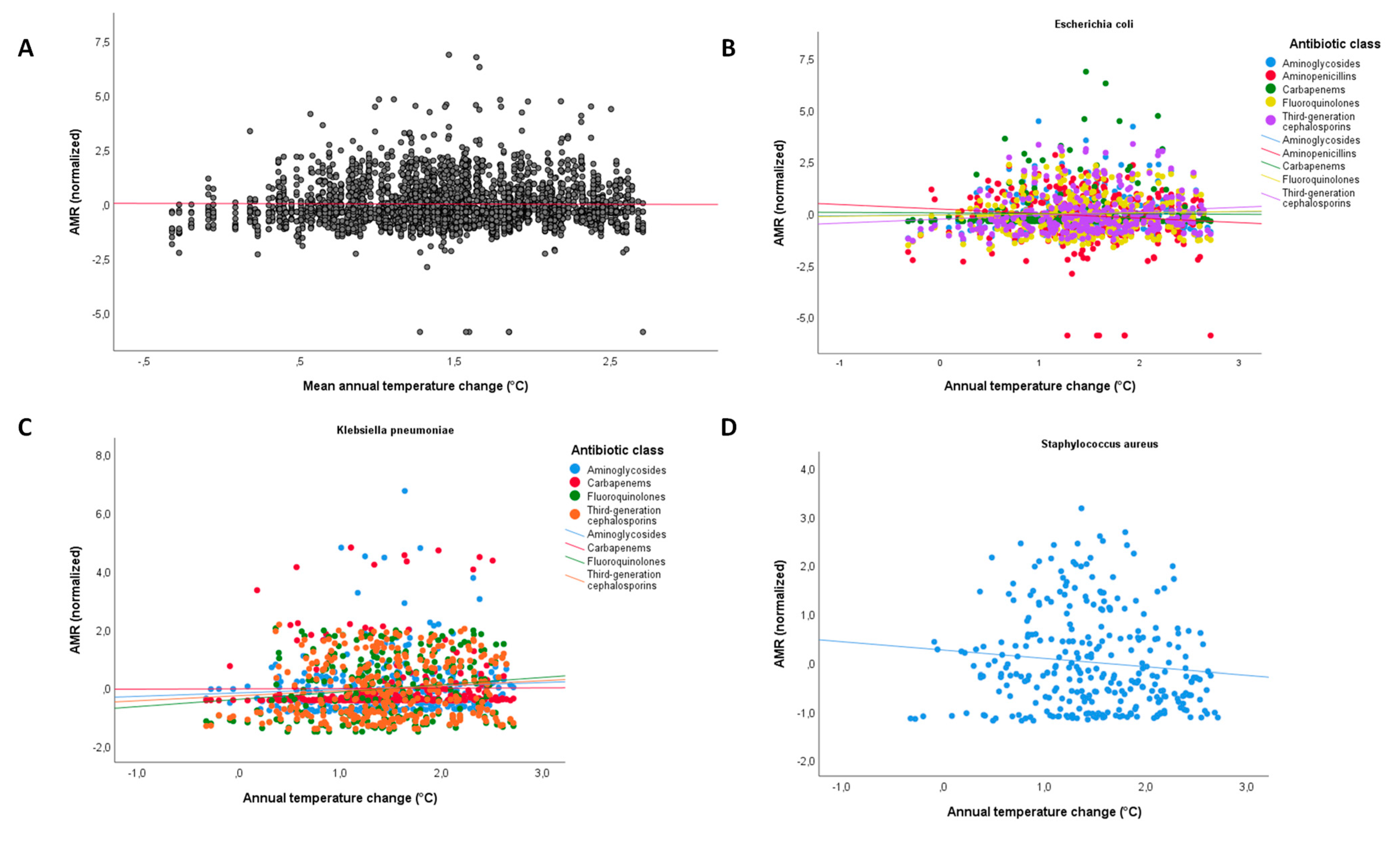
2.2. Relationship between Temperature Change and AMR
2.3. Accounting for the Effect of Gross Domestic Product and Governance
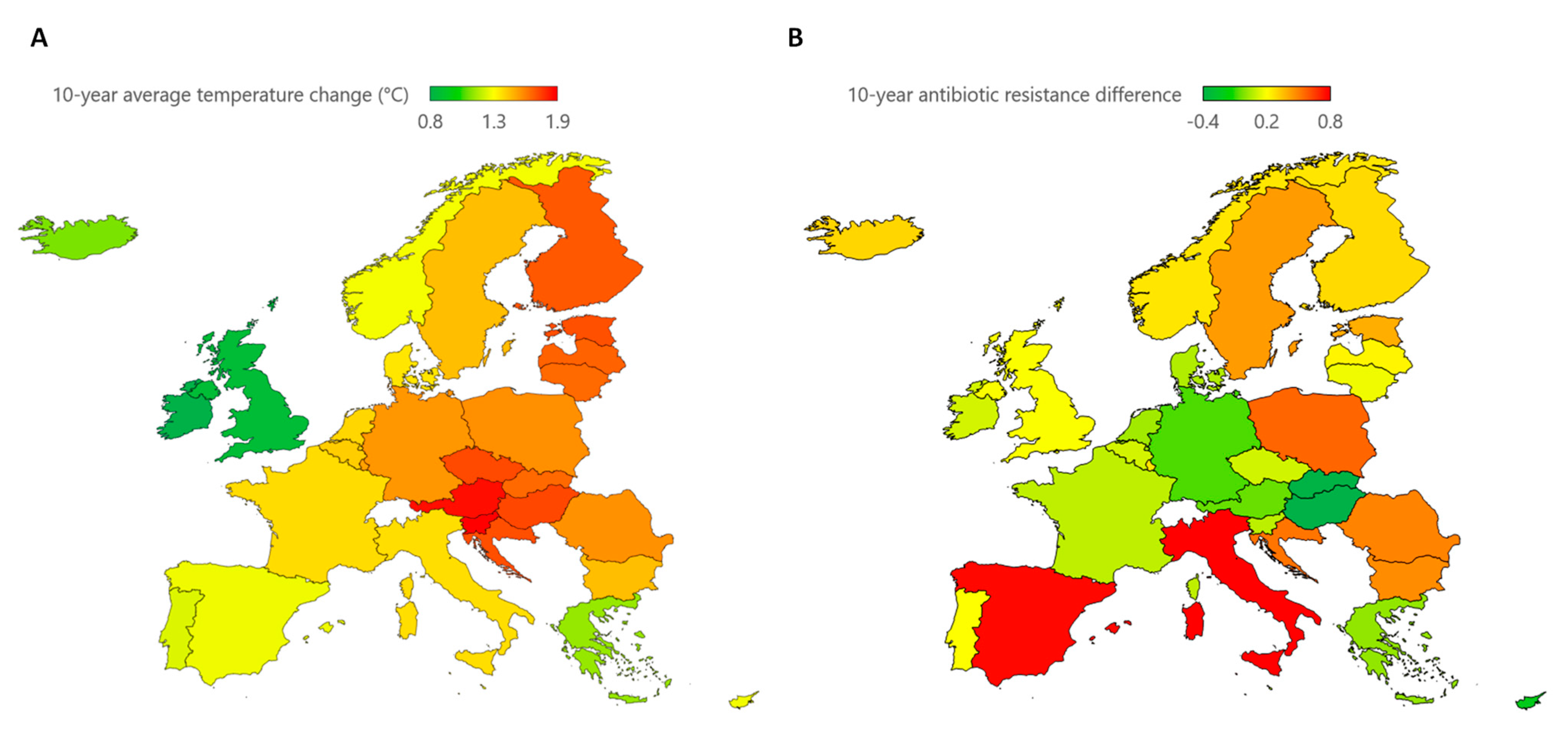
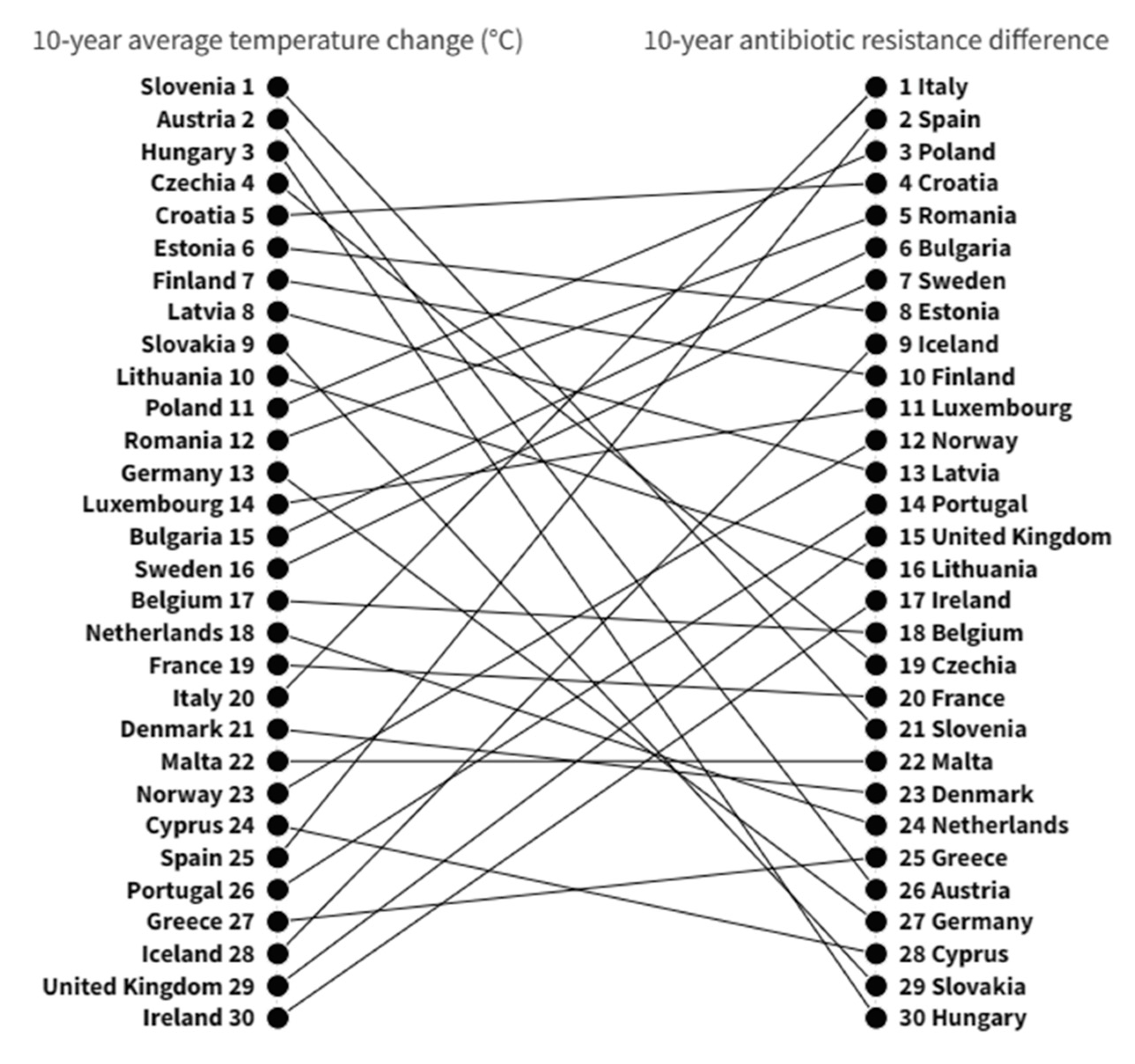
2.4. Evaluating the 10-Year Effect of Temperature Change
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Antimicrobial Resistance
4.3. Temperature Change
4.4. Antibiotic Consumption
4.5. Other Predictors
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed]
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Assessing the Health Burden of Infections with Antibiotic-Resistant Bacteria in the EU/EEA, 2016–2020; European Centre for Disease Prevention and Control: Solna, Sweden, 2022. [Google Scholar]
- World Health Organization. Global Action Plan on Antimicrobial Resistance. Geneva; 2015. Available online: https://www.who.int/publications/i/item/9789241509763 (accessed on 10 February 2023).
- European Commission. A European One Health Action Plan against Antimicrobial Resistance; European Commission: Brussels, Belgium, 2017. [Google Scholar]
- European Centre for Disease Prevention and Control. European Antimicrobial Resistance Surveillance Network (EARS-Net). Available online: https://www.ecdc.europa.eu/en/about-us/partnerships-and-networks/disease-and-laboratory-networks/ears-net (accessed on 10 February 2023).
- Gasser, M.; Zingg, W.; Cassini, A.; Kronenberg, A. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in Switzerland. Lancet Infect. Dis. 2019, 19, 17–18. [Google Scholar] [CrossRef] [PubMed]
- Naylor, N.R.; Atun, R.; Zhu, N.; Kulasabanathan, K.; Silva, S.; Chatterjee, A.; Knight, G.M.; Robotham, J.V. Estimating the burden of antimicrobial resistance: A systematic literature review. Antimicrob. Resist. Infect. Control 2018, 7, 58. [Google Scholar] [CrossRef]
- Hay, S.I.; Rao, P.C.; Dolecek, C.; Day, N.P.J.; Stergachis, A.; Lopez, A.D.; Murray, C.J.L. Measuring and mapping the global burden of antimicrobial resistance. BMC Med. 2018, 16, 78. [Google Scholar] [CrossRef]
- Cassini, A.; Plachouras, D.; Eckmanns, T.; Abu Sin, M.; Blank, H.P.; Ducomble, T.; Haller, S.; Harder, T.; Klingeberg, A.; Sixtensson, M.; et al. Burden of Six Healthcare-Associated Infections on European Population Health: Estimating Incidence-Based Disability-Adjusted Life Years through a Population Prevalence-Based Modelling Study. PLoS Med. 2016, 13, e1002150. [Google Scholar] [CrossRef]
- Barchitta, M.; Maugeri, A.; La Rosa, M.C.; La Mastra, C.; Murolo, G.; Corrao, G.; Agodi, A. Burden of Healthcare-Associated Infections in Sicily, Italy: Estimates from the Regional Point Prevalence Surveys 2016–2018. Antibiotics 2021, 10, 1360. [Google Scholar] [CrossRef]
- Cassini, A.; Colzani, E.; Pini, A.; Mangen, M.J.; Plass, D.; McDonald, S.A.; Maringhini, G.; van Lier, A.; Haagsma, J.A.; Havelaar, A.H.; et al. Impact of infectious diseases on population health using incidence-based disability-adjusted life years (DALYs): Results from the Burden of Communicable Diseases in Europe study, European Union and European Economic Area countries, 2009 to 2013. Eurosurveill 2018, 23, 17–00454. [Google Scholar] [CrossRef]
- Suetens, C.; Latour, K.; Kärki, T.; Ricchizzi, E.; Kinross, P.; Moro, M.L.; Jans, B.; Hopkins, S.; Hansen, S.; Lyytikäinen, O.; et al. Prevalence of healthcare-associated infections, estimated incidence and composite antimicrobial resistance index in acute care hospitals and long-term care facilities: Results from two European point prevalence surveys, 2016 to 2017. Eurosurveill 2018, 23, 1800516. [Google Scholar] [CrossRef]
- Collignon, P.; Beggs, J.J. Socioeconomic Enablers for Contagion: Factors Impelling the Antimicrobial Resistance Epidemic. Antibiotics 2019, 8, 86. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Antimicrobial Consumption in the EU/EEA (ESAC-Net)—Annual Epidemiological Report 2021. Stockholm: ECDC; 2022. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-consumption-europe-2021 (accessed on 10 February 2023).
- Collignon, P. Antibiotic resistance: Are we all doomed? Intern. Med. J. 2015, 45, 1109–1115. [Google Scholar] [CrossRef] [PubMed]
- Klein, E.Y.; Van Boeckel, T.P.; Martinez, E.M.; Pant, S.; Gandra, S.; Levin, S.A.; Goossens, H.; Laxminarayan, R. Global increase and geographic convergence in antibiotic consumption between 2000 and 2015. Proc. Natl. Acad. Sci. USA 2018, 115, E3463–E3470. [Google Scholar] [CrossRef] [PubMed]
- Collignon, P.; Beggs, J.J.; Walsh, T.R.; Gandra, S.; Laxminarayan, R. Anthropological and socioeconomic factors contributing to global antimicrobial resistance: A univariate and multivariable analysis. Lancet Planet Health 2018, 2, e398–e405. [Google Scholar] [CrossRef] [PubMed]
- Barchitta, M.; Maugeri, A.; Vinci, R.; Agodi, A. The Inverse Relationship between Influenza Vaccination and Antimicrobial Resistance: An Ecological Analysis of Italian Data. Vaccines 2022, 10, 554. [Google Scholar] [CrossRef]
- Maugeri, A.; Barchitta, M.; Agodi, A. Vaccination coverage in Italian children and antimicrobial resistance: An ecological analysis. Antimicrob. Resist. Infect. Control 2022, 11, 136. [Google Scholar] [CrossRef]
- Li, W.; Liu, C.; Ho, H.C.; Shi, L.; Zeng, Y.; Yang, X.; Huang, Q.; Pei, Y.; Huang, C.; Yang, L. Association between antibiotic resistance and increasing ambient temperature in China: An ecological study with nationwide panel data. Lancet Reg. Health West. Pac. 2023, 30, 100628. [Google Scholar] [CrossRef] [PubMed]
- Bock, L.; Aguilar-Bultet, L.; Egli, A.; Battegay, M.; Kronenberg, A.; Vogt, R.; Kaufmann, C.; Tschudin-Sutter, S. Air temperature and incidence of extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae. Environ. Res. 2022, 215, 114146. [Google Scholar] [CrossRef]
- Kaba, H.E.J.; Kuhlmann, E.; Scheithauer, S. Thinking outside the box: Association of antimicrobial resistance with climate warming in Europe—A 30 country observational study. Int. J. Hyg. Environ. Health 2020, 223, 151–158. [Google Scholar] [CrossRef]
- McGough, S.F.; MacFadden, D.R.; Hattab, M.W.; Mølbak, K.; Santillana, M. Rates of increase of antibiotic resistance and ambient temperature in Europe: A cross-national analysis of 28 countries between 2000 and 2016. Eurosurveill 2020, 25, 1900414. [Google Scholar] [CrossRef]
- MacFadden, D.R.; McGough, S.F.; Fisman, D.; Santillana, M.; Brownstein, J.S. Antibiotic Resistance Increases with Local Temperature. Nat. Clim. Chang. 2018, 8, 510–514. [Google Scholar] [CrossRef]
- Rodríguez-Verdugo, A.; Lozano-Huntelman, N.; Cruz-Loya, M.; Savage, V.; Yeh, P. Compounding Effects of Climate Warming and Antibiotic Resistance. iScience 2020, 23, 101024. [Google Scholar] [CrossRef] [PubMed]
- Magnano San Lio, R.; Favara, G.; Maugeri, A.; Barchitta, M.; Agodi, A. How Antimicrobial Resistance Is Linked to Climate Change: An Overview of Two Intertwined Global Challenges. Int. J. Environ. Res. Public Health 2023, 20, 1681. [Google Scholar] [CrossRef] [PubMed]
- Larsson, D.G.J.; Flach, C.F. Antibiotic resistance in the environment. Nat. Rev. Microbiol. 2022, 20, 257–269. [Google Scholar] [CrossRef] [PubMed]
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.K.; Wertheim, H.F.; Sumpradit, N.; Vlieghe, E.; Hara, G.L.; Gould, I.M.; Goossens, H.; et al. Antibiotic resistance-the need for global solutions. Lancet Infect. Dis. 2013, 13, 1057–1098. [Google Scholar] [CrossRef] [PubMed]
- Collignon, P.; Athukorala, P.C.; Senanayake, S.; Khan, F. Antimicrobial resistance: The major contribution of poor governance and corruption to this growing problem. PLoS ONE 2015, 10, e0116746. [Google Scholar] [CrossRef]
- Maugeri, A.; Barchitta, M.; Puglisi, F.; Agodi, A. Socio-economic, governance and health indicators shaping antimicrobial resistance: An ecological analysis of 30 european countries. Glob. Health 2023, 19, 12. [Google Scholar] [CrossRef] [PubMed]
- Laxminarayan, R.; Sridhar, D.; Blaser, M.; Wang, M.; Woolhouse, M. Achieving global targets for antimicrobial resistance. Science 2016, 353, 874–875. [Google Scholar] [CrossRef] [PubMed]
- Food and Agriculture Organization. Temperature Change Statistics 1961–2021. 2022. Available online: https://www.fao.org/3/cb9051en/cb9051en.pdf (accessed on 10 February 2023).
- Ratkowsky, D.A.; Olley, J.; McMeekin, T.A.; Ball, A. Relationship between temperature and growth rate of bacterial cultures. J. Bacteriol. 1982, 149, 1–5. [Google Scholar] [CrossRef]
- Holmes, A.H.; Moore, L.S.; Sundsfjord, A.; Steinbakk, M.; Regmi, S.; Karkey, A.; Guerin, P.J.; Piddock, L.J. Understanding the mechanisms and drivers of antimicrobial resistance. Lancet 2016, 387, 176–187. [Google Scholar] [CrossRef]
- Relman, D.A. Microbial genomics and infectious diseases. N. Engl. J. Med. 2011, 365, 347–357. [Google Scholar] [CrossRef]
- Surette, M.D.; Wright, G.D. Lessons from the Environmental Antibiotic Resistome. Annu. Rev. Microbiol. 2017, 71, 309–329. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, M.G.; Wackernagel, W. Bacterial gene transfer by natural genetic transformation in the environment. Microbiol. Rev. 1994, 58, 563–602. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.R.; Weeks, J.; Livermore, D.M.; Toleman, M.A. Dissemination of NDM-1 positive bacteria in the New Delhi environment and its implications for human health: An environmental point prevalence study. Lancet Infect. Dis. 2011, 11, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Uria, G.; Midde, M. Trends and factors associated with antimicrobial resistance of Acinetobacter spp. invasive isolates in Europe: A country-level analysis. J. Glob. Antimicrob. Resist. 2018, 14, 29–32. [Google Scholar] [CrossRef]
- Robinson, T.P.; Bu, D.P.; Carrique-Mas, J.; Fèvre, E.M.; Gilbert, M.; Grace, D.; Hay, S.I.; Jiwakanon, J.; Kakkar, M.; Kariuki, S.; et al. Antibiotic resistance is the quintessential One Health issue. Trans. R. Soc. Trop. Med. Hyg. 2016, 110, 377–380. [Google Scholar] [CrossRef]
- Kaier, K.; Frank, U.; Conrad, A.; Meyer, E. Seasonal and ascending trends in the incidence of carriage of extended-spectrum ß-lactamase-producing Escherichia coli and Klebsiella species in 2 German hospitals. Infect. Control Hosp. Epidemiol. 2010, 31, 1154–1159. [Google Scholar] [CrossRef]
- Titley, M.A.; Butchart, S.H.M.; Jones, V.R.; Whittingham, M.J.; Willis, S.G. Global inequities and political borders challenge nature conservation under climate change. Proc. Natl. Acad. Sci. USA 2021, 118, e2011204118. [Google Scholar] [CrossRef]
- Liobikienė, G.; Butkus, M. The challenges and opportunities of climate change policy under different stages of economic development. Sci. Total Environ. 2018, 642, 999–1007. [Google Scholar] [CrossRef]
- Zhou, N.; Cheng, Z.; Zhang, X.; Lv, C.; Guo, C.; Liu, H.; Dong, K.; Zhang, Y.; Liu, C.; Chang, Y.F.; et al. Global antimicrobial resistance: A system-wide comprehensive investigation using the Global One Health Index. Infect. Dis. Poverty 2022, 11, 92. [Google Scholar] [CrossRef]
- Our World in Data. CO₂ Emissions per Capita vs GDP per Capita. 2018. Available online: https://ourworldindata.org/grapher/co2-emissions-vs-gdp (accessed on 10 February 2023).
- Newell, R.G.; Prest, B.C.; Sexton, S.E. The GDP-Temperature relationship: Implications for climate change damages. J. Environ. Econ. Manag. 2021, 108, 102445. [Google Scholar] [CrossRef]
- Rosen, R.A. Temperature impact on GDP growth is overestimated. Proc. Natl. Acad. Sci. USA 2019, 116, 16170. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, D.; Kraay, A.; Mastruzzi, M. The Worldwide Governance Indicators: Methodology and Analytical Issues. Hague J. Rule Law 2010, 3, 220–246. [Google Scholar] [CrossRef]
- Krieger, N. Climate crisis, health equity, and democratic governance: The need to act together. J. Public Health Policy 2020, 41, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Bronen, R.; Chapin, F.S., 3rd. Adaptive governance and institutional strategies for climate-induced community relocations in Alaska. Proc. Natl. Acad. Sci. USA 2013, 110, 9320–9325. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Surveillance Atlas of Infectious Diseases. Available online: https://www.ecdc.europa.eu/en/surveillance-atlas-infectious-diseases (accessed on 10 February 2023).
- Food and Agriculture Organization. FAOSTAT Database: Temperature Change. Available online: https://www.fao.org/faostat/en/#data/ET (accessed on 10 February 2023).
- European Centre for Disease Prevention and Control. Antimicrobial Consumption Database (ESAC-Net). Available online: https://www.ecdc.europa.eu/en/antimicrobial-consumption/surveillance-and-disease-data/database (accessed on 10 February 2023).
- European Centre for Disease Prevention and Control. ESAC-Net Reporting Protocol 2022; European Centre for Disease Prevention and Control: Solna, Sweden, 2022. [Google Scholar]
- World Bank. World DataBank: World Development Indicators. Washington, DC. Available online: https://databank.worldbank.org/source/world-development-indicators (accessed on 10 February 2023).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pathogens and Predictors | Coefficient (95% Confidence Interval) a | ||||||
|---|---|---|---|---|---|---|---|
| E. coli | Overall | Aminoglycosides | Aminopenicillins | Carbapenems | Fluoroquinolones | Third-Generation Cephalosporins | Methicillin |
| Mean annual temperature change (°C) | 0.034 (−0.087; 0.155) | 0.168 (−0.055; 0.390) | −0.250 (−0.556; 0.057) | 0.068 (−0.230; 0.365) | 0.116 (−0.097; 0.329) | 0.070 (−0.163; 0.304) | - |
| Year | 0.059 (0.020; 0.098) ** | 0.071 (−0.001; 0.142) | 0.034 (−0.064; 0.133) | 0.062 (−0.033; 0.158) | 0.060 (−0.008; 0.129) | 0.066 (−0.009; 0.141) | - |
| Interaction | −0.024 (−0.048; −0.001) * | −0.047 (−0.090; −0.003) * | −0.003 (−0.063; 0.057) | −0.031 (−0.089; 0.027) | −0.028 (−0.069; 0.014) | −0.013 (−0.058; 0.033) | - |
| Antibiotic consumption in the community (DDD/1000 inhabitants/day) | 0.654 (0.469; 0.840) *** | 0.335 (−0.005; 0.676) | 1.210 (0.741; 1.679) *** | 0.578 (0.123; 1.033) * | 0.729 (0.403; 1.054) *** | 0.419 (0.061; 0.777) * | - |
| Population density (persons/km2) | 0.147 (0.111; 0.183) *** | 0.099 (0.033; 0.165) ** | 0.328 (0.236; 0.419) *** | −0.041 (−0.130; 0.047) | 0.279 (0.215; 0.342) *** | 0.073 (0.003; 0.142) * | - |
| GDP per capita (current USD) | 0.148 (−0.005; 0.301) | 0.147 (−0.134; 0.429) | −0.023 (−0.411; 0.365) | 0.255 (−0.122; 0.631) | 0.262 (−0.008; 0.531) | 0.100 (−0.196; 0.396) | - |
| Governance Index | −1.291 (−1.508; −1.073) *** | −1.559 (−1.959; −1.158) *** | −1.127 (−1.678; −0.575) *** | −0.982 (−1.517; −0.447) *** | −1.378 (−1.761; −0.996) *** | −1.406 (−1.827; −0.985) *** | - |
| K. Pneumoniae | - | ||||||
| Mean annual temperature change (°C) | 0.006 (−0.149; 0.161) | −0.071 (−0.379; 0.237) | - | −0.084 (−0.410; 0.241) | 0.101 (−0.083; 0.285) | 0.078 (−0.085; 0.242) | - |
| Year | 0.051 (0.001; 0.101) * | 0.167 (0.068; 0.266) ** | - | 0.049 (−0.056; 0.154) | −0.010 (−0.069; 0.049) | −0.002 (−0.055; 0.051) | - |
| Interaction | −0.006 (−0.036; 0.024) | −0.035 (−0.095; 0.026) | - | −0.003 (−0.067; 0.061) | 0.012 (−0.024; 0.048) | 0.001 (−0.031; 0.033) | - |
| Antibiotic consumption in the community (DDD/1000 inhabitants/day) | 0.097 (−0.140; 0.334) | −0.479 (−0.950; 0.007) | - | −0.225 (−0.724; 0.274) | 0.531 (0.250; 0.813) *** | 0.560 (0.309; 0.811) *** | - |
| Population density (persons/km2) | 0.111 (0.065; 0.157) *** | 0.195 (0.103; 0.287) *** | - | 0.138 (0.041; 0.234) ** | 0.075 (0.020; 0.129) ** | 0.036 (−0.013; 0.085) | - |
| GDP per capita (current USD) | 0.086 (−0.110; 0.282) | 0.652 (0.262; 1.042) ** | - | 0.162 (−0.251; 0.574) | −0.187 (−0.420; 0.046) | −0.284 (−0.492; −0.076) ** | - |
| Governance Index | −0.804 (−1.083; −0.525) *** | −0.657 (−1.212; −0.103) *** | - | 0.075 (−0.512; 0.661) | −1.328 (−1.659; −0.997) *** | −1.304 (−1.599; −1.009) *** | - |
| S. aureus | |||||||
| Mean annual temperature change (°C) | - | - | - | - | - | - | 0.075 (−0.122; 0.272) |
| Year | - | - | - | - | - | - | 0.015 (−0.048; 0.078) |
| Interaction | - | - | - | - | - | - | −0.029 (−0.067; 0.010) |
| Antibiotic consumption in the community (DDD/1000 inhabitants/day) | - | - | - | - | - | - | 1.401 (1.100; 1.702) *** |
| Population density (persons/km2) | - | - | - | - | - | - | 0.251 (0.193; 0.310) *** |
| GDP per capita (current USD) | - | - | - | - | - | - | −0.149 (−0.398; 0.100) |
| Governance Index | - | - | - | - | - | - | −0.765 (−1.119; −0.412) *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maugeri, A.; Barchitta, M.; Magnano San Lio, R.; Agodi, A. Socioeconomic and Governance Factors Disentangle the Relationship between Temperature and Antimicrobial Resistance: A 10-Year Ecological Analysis of European Countries. Antibiotics 2023, 12, 777. https://doi.org/10.3390/antibiotics12040777
Maugeri A, Barchitta M, Magnano San Lio R, Agodi A. Socioeconomic and Governance Factors Disentangle the Relationship between Temperature and Antimicrobial Resistance: A 10-Year Ecological Analysis of European Countries. Antibiotics. 2023; 12(4):777. https://doi.org/10.3390/antibiotics12040777
Chicago/Turabian StyleMaugeri, Andrea, Martina Barchitta, Roberta Magnano San Lio, and Antonella Agodi. 2023. "Socioeconomic and Governance Factors Disentangle the Relationship between Temperature and Antimicrobial Resistance: A 10-Year Ecological Analysis of European Countries" Antibiotics 12, no. 4: 777. https://doi.org/10.3390/antibiotics12040777