

Screening for Tuberculosis Infection among Migrants: A Cost-Effectiveness Analysis in the Italian Context
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Site and Population
2.2. Study Design
2.3. Study Procedures
2.3.1. Arm 1 Procedures
2.3.2. Arm 2 Procedures
2.3.3. Definitions
- -
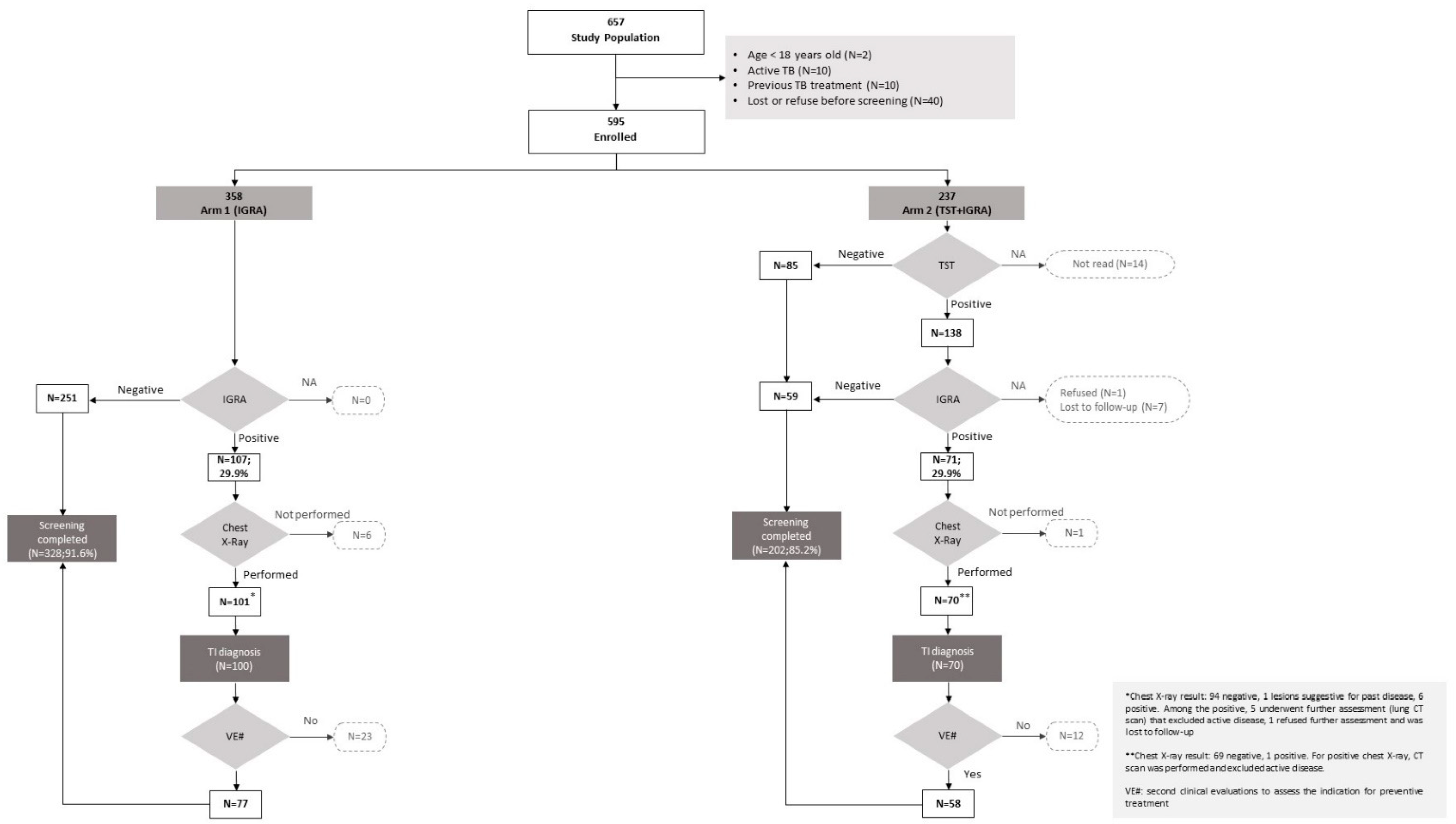
- Arm 1 (IGRA only): in case of a negative IGRA result, screening was considered completed when the IGRA result was communicated; for patients with a positive IGRA test, chest X-ray (VR) and outpatient consultation for preventive therapy (VE) were required.
- -
- Arm 2 (sequential strategy): in case of a negative TST result, participants completed the screening process when the result was evaluated (V2); in case of a positive TST result, screening was defined as completed either when the IGRA result was communicated or when participants underwent chest X-ray (VR) and outpatient consultation for preventive therapy (VE) according to a negative or positive IGRA test result, respectively.
2.4. Statistical Analysis
2.5. Cost-Effectiveness Analysis
2.6. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aldridge, R.W.; Zenner, D.; White, P.J.; Williamson, E.J.; Muzyamba, M.C.; Dhavan, P.; Mosca, D.; Thomas, L.H.; Lalor, M.K.; Abubakar, I.; et al. Tuberculosis in migrants moving from high-incidence to low-incidence countries: A population-based cohort study of 519 955 migrants screened before entry to England, Wales, and Northern Ireland. Lancet 2016, 388, 2510–2518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Centre for Disease Prevention and Control, WHO Regional Office for Europe. Tuberculosis Surveillance and Monitoring in Europe 2022–2020 Data; WHO Regional Office for Europe and Stockholm, European Centre for Disease Prevention and Control: Copenhagen, Demark, 2022; Licence: CC BY 3.0 IGO. [Google Scholar]
- Marchese, V.; Rossi, L.; Formenti, B.; Magoni, M.; Caruana, A.; Sileo, C.; Lanfredini, L.; Castelli, F.; Matteelli, A. Tuberculosis trend among native and foreign-born people over a 17 year period (2004–2020) in a large province in Northern Italy. Sci. Rep. 2021, 11, 23394. [Google Scholar] [CrossRef] [PubMed]
- Pontarelli, A.; Marchese, V.; Scolari, C.; Capone, S.; El-Hamad, I.; Donato, F.; Moioli, R.; Girardi, E.; Cirillo, D.M.; Castelli, F.; et al. Screening for active and latent tuberculosis among asylum seekers in Italy: A retrospective cohort analysis. Travel. Med. Infect. Dis. 2019, 27, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Vanino, E.; Tadolini, M.; Attard, L.; Po, C.; Francia, F.; Giannini, A.; Viale, P. Systematic Tuberculosis Screening in Asylum Seekers in Italy. Clin. Infect. Dis. 2017, 65, 1407–1409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menezes, D.; Zenner, D.; Aldridge, R.; Anderson, S.R.; de Vries, G.; Erkens, C.; Marchese, V.; Matteeli, A.; Muzyamba, M.; Nederby-Öhd, J.; et al. Country differences and determinants of yield in programmatic migrant TB screening in four European countries. Int. J. Tuberc. Lung Dis. 2022, 26, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Barcellini, L.; Borroni, E.; Cimaglia, C.; Girardi, E.; Matteelli, A.; Marchese, V.; Stancanelli, G.; Abubakar, I.; members of the E-Detect TB Consortium; Cirillo, D.M. App-based symptoms screening with Xpert MTB/RIF Ultra assay used for active tuberculosis detection in migrants at point of arrivals in Italy: The E-DETECT TB intervention analysis. PLoS ONE 2019, 14, e0218039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zammarchi, L.; Casadei, G.; Strohmeyer, M.; Bartalesi, F.; Liendo, C.; Matteelli, A.; Bonati, M.; Gotuzzo, E.; Bartoloni, A.; COHEMI project study group. A scoping review of cost-effectiveness of screening and treatment for latent tubercolosis infection in migrants from high-incidence countries. BMC Health Serv. Res. 2015, 15, 412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zenner, D.; Hafezi, H.; Potter, J.; Capone, S.; Matteelli, A. Effectiveness and cost-effectiveness of screening migrants for active tuberculosis and latent tuberculous infection. Int. J. Tuberc. Lung Dis. 2017, 21, 965–976. [Google Scholar] [CrossRef] [PubMed]
- Marx, F.M.; Hauer, B.; Menzies, N.A.; Haas, W.; Perumal, N. Targeting screening and treatment for latent tuberculosis infection towards asylum seekers from high-incidence countries—A model-based cost-effectiveness analysis. BMC Public Health 2021, 21, 2172. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Public Health Guidance on Screening and Vaccination for Infectious Diseases in Newly Arrived Migrants within the EU/EEA; ECDC: Stockholm, Sweden, 2018. [Google Scholar]
- D’Ambrosio, L.; Centis, R.; Dara, M.; Solovic, I.; Sulis, G.; Zumla, A.; Migliori, G.B. European policies in the management of tuberculosis among migrants. Int. J. Infect. Dis. 2017, 56, 85–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Ambrosio, L.; Centis, R.; Dobler, C.C.; Tiberi, S.; Matteelli, A.; Denholm, J.; Zenner, D.; Al-Abri, S.; Alyaquobi, F.; Arbex, M.A.; et al. Screening for Tuberculosis in Migrants: A Survey by the Global Tuberculosis Network. Antibiotics 2021, 10, 1355. [Google Scholar] [CrossRef] [PubMed]
- Kunst, H.; Burman, M.; Arnesen, T.M.; Fiebig, L.; Hergens, M.P.; Kalkouni, O.; Klinkenberg, E.; Orcau, À.; Soini, H.; Sotgiu, G.; et al. Tuberculosis and latent tuberculous infection screening of migrants in Europe: Comparative analysis of policies, surveillance systems and results. Int. J. Tuberc. Lung Dis. 2017, 21, 840–851. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Review of Reviews and Guidelines on Target Groups, Diagnosis, Treatment and Programmatic Issues for Implementation of Latent Tuberculosis Management; ECDC: Stockholm, Sweden, 2018; Available online: https://www.ecdc.europa.eu/en/publications-data/review-reviews-and-guidelines-target-groups-diagnosis-treatment-and-programmatic (accessed on 29 November 2022).
- Berrocal-Almanza, L.C.; Harris, R.J.; Collin, S.M.; Muzyamba, M.C.; Conroy, O.D.; Mirza, A.; O’Connell, A.M.; Altass, L.; Anderson, S.R.; Thomas, H.L.; et al. Effectiveness of nationwide programmatic testing and treatment for latent tuberculosis infection in migrants in England: A retrospective, population-based cohort study. Lancet Public Health 2022, 7, e305–e315. [Google Scholar] [CrossRef]
- WHO Consolidated Guidelines on Tuberculosis. Module 1: Prevention—Tuberculosis Preventive Treatment; World Health Organization: Geneva, Switzerland, 2020; Licence: CC BY-NC-SA 3.0 IGO. [Google Scholar]
- Latent Tuberculosis Infection: Updated and Consolidated Guidelines for Programmatic Management; World Health Organization: Geneva, Switzerland, 2018; Licence: CC BY-NC-SA 3.0 IGO.
- Istituto Nazionale per la Promozione Della Salute Delle Popolazioni Migranti e per il Contrasto delle Malattie della Povertà (INMP); Istituto Superiore di Sanità (ISS); Società Italiana di Medicina delle Migrazioni (SIMM). I Controlli alla Frontiera. La Frontiera dei Controlli. Controlli Sanitari All’arrivo e Percorsi di Tutela per i Migranti Ospiti nei Centri di Accoglienza. Italian. Published online 2017. Available online: https://www.epicentro.iss.it/migranti/pdf/LG_Migranti-web.pdf (accessed on 1 January 2023).
- Lombardy Region. Delibera Giunta Regionale 12 Luglio 2017—N. X/6855 Revisione ed Aggiornamento degli Interventi di Sorveglianza, Prevenzione, Profilassi e Controllo Della Tubercolosi in Regione Lombardia. Italian. Published Online 2017. Available online: http://www.consultazioniburl.servizirl.it/ConsultazioneBurl/temp/16038089248401776997901237012217.pdf#page=3 (accessed on 1 January 2023).
- European Centre for Disease Prevention and Control. Cost-Effectiveness Analysis of Programmatic Screening Strategies for Latent Tuberculosis Infection in the EU/EEA; Stockholm: ECDC; 2018. Available online: https://data.europa.eu/doi/10.2900/938014 (accessed on 29 November 2022).
- Rustage, K.; Lobe, J.; Hayward, S.E.; Kristensen, K.L.; Margineanu, I.; Stienstra, Y.; Goletti, D.; Zenner, D.; Noori, T.; Pareek, M. Initiation and completion of treatment for latent tuberculosis infection in migrants globally: A systematic review and meta-analysis. Lancet Infect. Dis. 2021, 21, 1701–1712. [Google Scholar] [CrossRef]
- World Health Organization. Global Tuberculosis Report 2022; WHO: Geneva, Switzerland, 2022; Licence: CC BY-NC-SA 3.0 IGO. [Google Scholar]
- Lim, R.K.; Talavlikar, R.; Chiazor, O.; Bietz, J.; Gardiner, H.; Fisher, D. Fewer losses in the cascade of care for latent tuberculosis with solo interferon-gamma release assay screening compared to sequential screening. BMC Infect. Dis. 2021, 21, 936. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Programmatic Management of Latent Tuberculosis Infection in the European Union; ECDC: Stockholm, Sweden, 2018. [Google Scholar]
- Zwerling, A.; Behr, M.A.; Verma, A.; Brewer, T.F.; Menzies, D.; Pai, M. The BCG World Atlas: A Database of Global BCG Vaccination Policies and Practices. PLoS Med. 2011, 8, e1001012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abubakar, I.; Lalvani, A.; Southern, J.; Sitch, A.; Jackson, C.; Onyimadu, O.; Lipman, M.; Deeks, J.J.; Griffiths, C.; Bothamley, G.; et al. Two interferon gamma release assays for predicting active tuberculosis: The UK PREDICT TB prognostic test study. Health Technol. Assess. 2018, 22, 1–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, J.R.; Johnston, J.C.; Sadatsafavi, M.; Cook, V.J.; Elwood, R.K.; Marra, F. Cost-effectiveness of post-landing latent tuberculosisinfection control strategies in new migrants toCanada. PLoS ONE 2017, 12, e0186778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahon, J.; Beale, S.; Holmes, H.; Arber, M.; Nikolayevskyy, V.; Alagna, R.; Manissero, D.; Dowdy, D.; Migliori, G.B.; Sotgiu, G.; et al. A systematic review of cost-utility analyses of screening methods in latent tuberculosis infection in high-risk populations. BMC Pulm. Med. 2022, 22, 375. [Google Scholar] [CrossRef] [PubMed]
- Proença, R.; Mattos Souza, F.; Lisboa Bastos, M.; Caetano, R.; Braga, J.U.; Faerstein, E.; Trajman, A. Active and latent tuberculosis in refugees and asylum seekers: A systematic review and meta-analysis. BMC Public Health 2020, 20, 838. [Google Scholar] [CrossRef] [PubMed]
- Istituto Nazionale per la Promozione della Salute delle Popolazioni Migranti e per il Contrasto delle Malattie della Povertà (INMP); Istituto Superiore di Sanità (ISS); Società Italiana di Medicina delle Migrazioni (SIMM). Il controllo della tubercolosi tra gli immigrati in Italia. ISBN 9788898544202. Italian. Published online 2018. Available online: https://www.iss.it/documents/20126/0/LG_tubercolosi.pdf/25b23756-b119-2e08-012b-86d880734fa4?t=1582277492054 (accessed on 1 January 2023).
- Italian Ministry of Health. Linee Guida per il Controllo della Malattia Tubercolare su Proposta del Ministro della Sanità, ai Sensi dell’art. 115, Comma 1, Lettera b) del Decreto Legislativo 31 Marzo 1998, n. 112. Italian. Available online: https://www.salute.gov.it/imgs/C_17_pubblicazioni_615_allegato.pdf (accessed on 1 January 2023).


{kind=link}
| Arm 1 (IGRA Only) | Arm 2 (TST + IGRA) | Total | p-Value | |
|---|---|---|---|---|
| Total population, n | 358 | 237 | 595 | - |
| Sex, n (%) | ||||
| Men | 321 (89.7) | 223 (94.1) | 544 (91.4) | 0.059 |
| Women | 31 (10.3) | 14 (5.9) | 51 (8.6) | |
| Median age at the time of arrival, years (IQR) | 26 (22–33) | 26 (23–32) | 26 (22–32) | 0.955 |
| Age at the time of the first test, n (%) | ||||
| ≤26 years | 196 (54.8) | 127 (53.6) | 323 (54.3) | 0.781 |
| >26 years | 657 (45.3) | 110 (46.4) | 272 (45.7) | |
| Year of arrival * | ||||
| ≤2020 | 171 (47.8) | 160 (67.5) | 331 (55.6) | <0.001 |
| >2020 | 179 (50.0) | 46 (19.4) | 225 (37.8) | |
| TB incidence in the country of origin, n (%) ^ | ||||
| <150/100,000 | 118 (33.0) | 90 (38.0) | 208 (35.0) | 0.209 |
| ≥150/100,000 | 240 (67.0) | 147 (62.0) | 387 (65.0) |
| Screening Completed/Tot | Univariable | Multivariable | |||
|---|---|---|---|---|---|
| (530/595) | IRR (95% CI) | p-Value | aIRR (95% CI) | p-Value | |
| SEX | |||||
| Men | 485/544 | Ref. | Ref. | ||
| Women | 45/51 | 0.99 (0.89–1.10) | 0.846 | 0.97 (0.88–1.09) | 0.669 |
| Age at first test, by 5-year increase | 1.00 (0.99–1.02) | 0.657 | 1.00 (0.99–1.02) | 0.712 | |
| ARM | |||||
| 1 (IGRA) | 328/358 | 1.07 (1.01–1.14) | 0.022 | 1.08 (1.01–1.14) | 0.019 |
| 2 (TST + IGRA) | 202/237 | Ref. | Ref. | ||
| TB INCIDENCE IN THE COUNTRY OF ORIGIN ^ | |||||
| <150/100,0000 | 185/208 | Ref. | |||
| ≥150/100,0000 | 345/387 | 1.00 (0.94–1.06) | 0.939 | 1.00 (0.94–1.06) | 0.969 |
| Treatment Initiation/Tot | Univariable | Multivariable | |||
|---|---|---|---|---|---|
| (117/595) | IRR (95% CI) | p-Value | aIRR (95% CI) | p-Value | |
| SEX | |||||
| Men | 111/544 | Ref | Ref | ||
| Women | 6/51 | 0.58 (0.27–1.25) | 0.161 | 0.59 (0.29–1.28) | 0.181 |
| Age at the first test, by 5-year increase | 1.01 (0.93–1.11) | 0.766 | 1.03 (0.94–1.14) | 0.523 | |
| ARM | |||||
| 1 (IGRA) | 65/358 | 0.83 (0.60–1.14) | 0.255 | 0.83 (0.60–1.15) | 0.272 |
| 2 (TST + IGRA) | 52/237 | Ref | Ref | Ref | |
| TB INCIDENCE IN THE COUNTRY OF ORIGIN ^ | |||||
| <150/100,0000 | 37/208 | Ref | Ref | ||
| ≥150/100,0000 | 80/387 | 1.16 (0.82–1.65) | 0.402 | 1.17 (0.82–1.67) | 0.400 |
| Cost per Unit | Arm 1 (IGRA) | Arm 2 (TST + IGRA) | ||||
|---|---|---|---|---|---|---|
| N. | Costs (€) | N. | Costs (€) | |||
| TST * | - | 237 | 1374.60 | |||
| IGRA | 358 | 18,705.50 | 130 | 6792.50 | ||
| Chest X-ray # | 162 | 2818.80 | 81 | 1409.40 | ||
| VE (performed as distinct from VT) | 40 | 900.00 | 26 | 585.00 | ||
| VT (performed as distinct from VE) | 28 | 630.00 | 20 | 450.00 | ||
| VE + VT (performed at a single time point) | 37 | 832.50 | 32 | 720.00 | ||
| Blood tests | 65 | 2905.50 | 52 | 2324.40 | ||
| Total | 26,792.30 | 13,655.90 | ||||
| Costs per subject undergoing TBI screening | 74.84 | 57.62 | ||||
| Costs for 100 subjects undergoing TBI screening | 7483.88 | 5761.98 | ||||
| ACER § | 412.19 | 262.61 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Russo, G.; Marchese, V.; Formenti, B.; Cimaglia, C.; Di Rosario, G.; Cristini, I.; Magro, P.; El-Hamad, I.; Cirillo, D.M.; Girardi, E.; et al. Screening for Tuberculosis Infection among Migrants: A Cost-Effectiveness Analysis in the Italian Context. Antibiotics 2023, 12, 631. https://doi.org/10.3390/antibiotics12040631
Russo G, Marchese V, Formenti B, Cimaglia C, Di Rosario G, Cristini I, Magro P, El-Hamad I, Cirillo DM, Girardi E, et al. Screening for Tuberculosis Infection among Migrants: A Cost-Effectiveness Analysis in the Italian Context. Antibiotics. 2023; 12(4):631. https://doi.org/10.3390/antibiotics12040631
Chicago/Turabian StyleRusso, Giulia, Valentina Marchese, Beatrice Formenti, Claudia Cimaglia, Gianluca Di Rosario, Irene Cristini, Paola Magro, Issa El-Hamad, Daniela Maria Cirillo, Enrico Girardi, and et al. 2023. "Screening for Tuberculosis Infection among Migrants: A Cost-Effectiveness Analysis in the Italian Context" Antibiotics 12, no. 4: 631. https://doi.org/10.3390/antibiotics12040631