
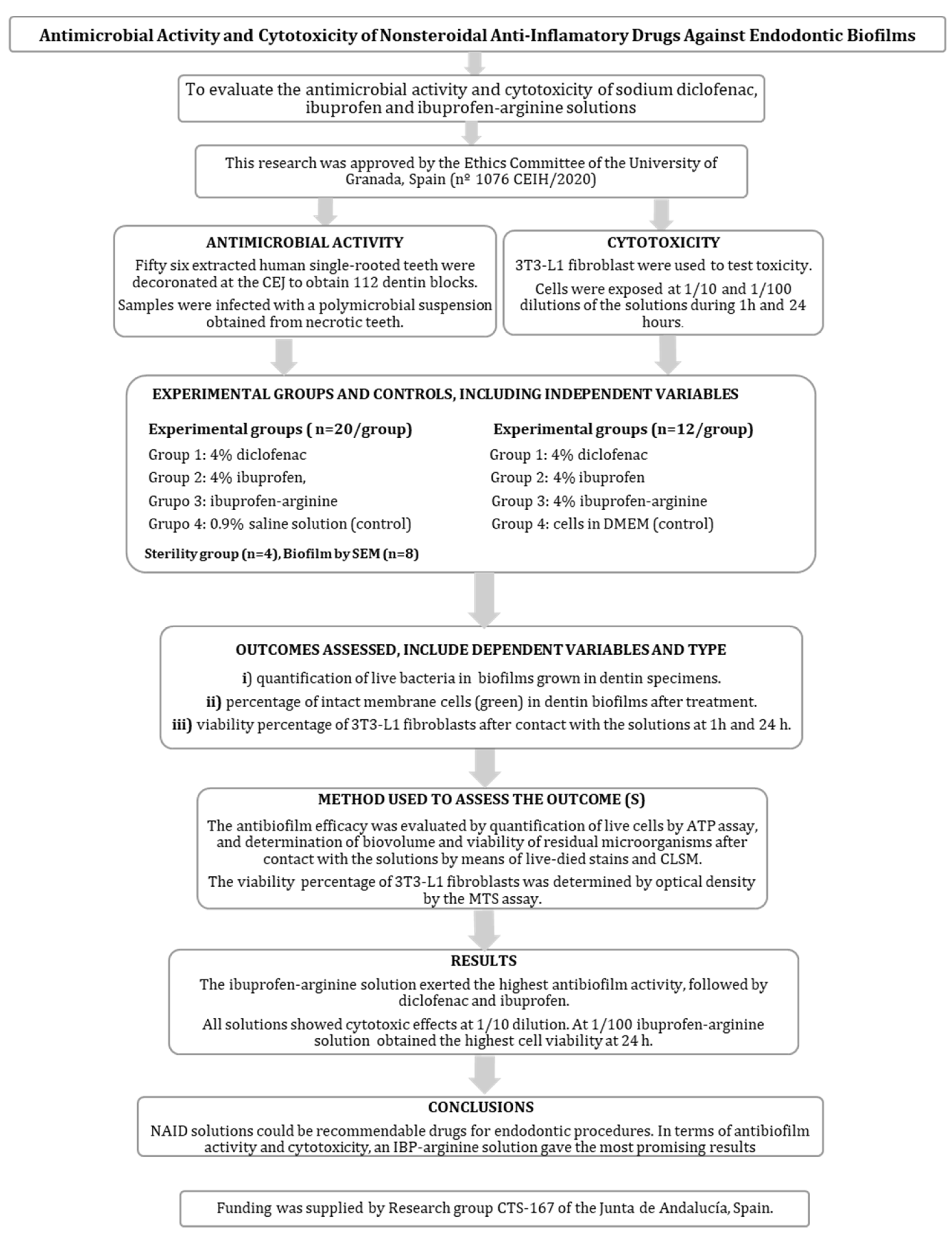
Antimicrobial Activity and Cytotoxicity of Nonsteroidal Anti-Inflammatory Drugs against Endodontic Biofilms
Abstract
:1. Introduction
2. Results
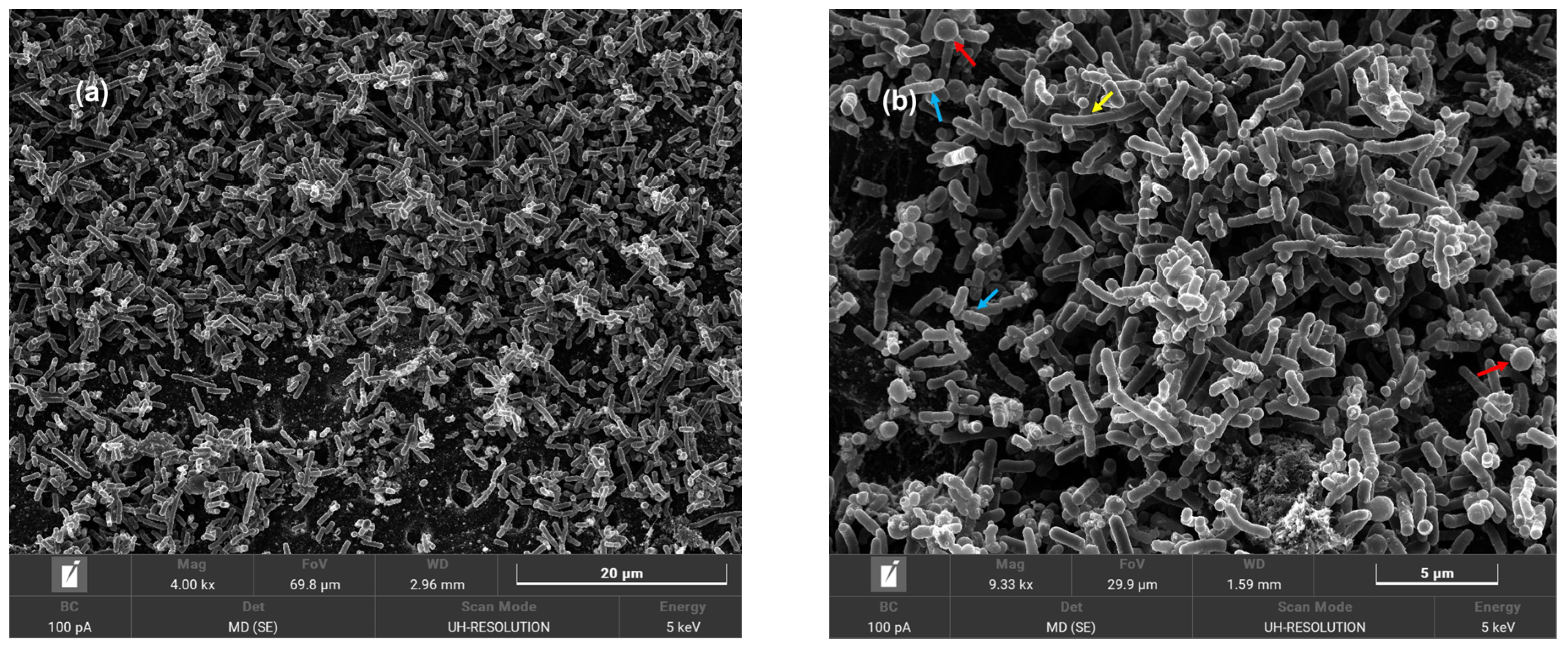
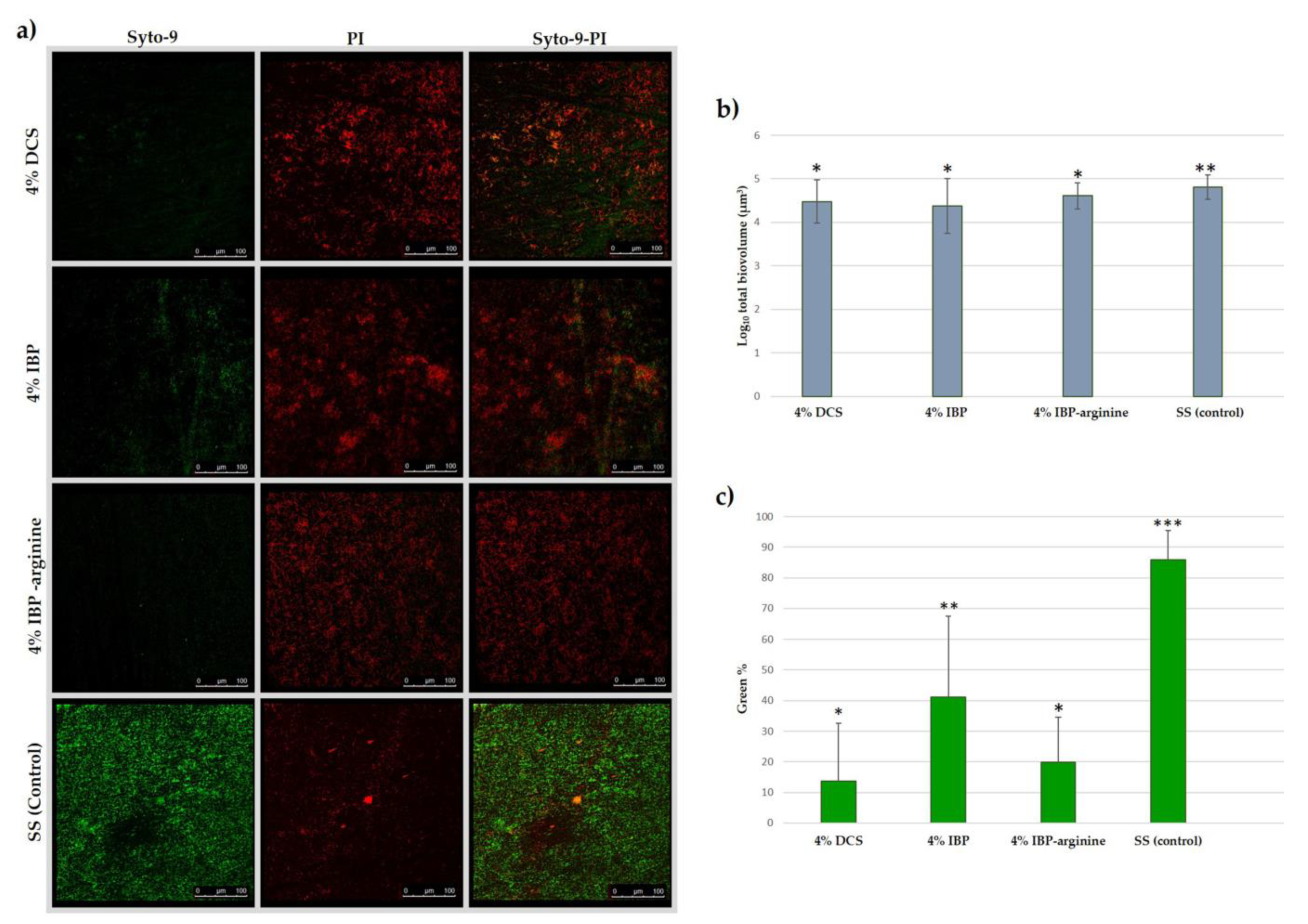
2.1. Antimicrobial Effects
2.2. Cytotoxicity
3. Discussion
4. Materials and Methods
4.1. Antimicrobial Activity Determination
4.1.1. Preparation and Infection of Dentin Specimens
4.1.2. Antimicrobial Test
4.2. Cytotoxicity Assessment
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Neelakantan, P.; Romero, M.; Vera, J.; Daood, U.; Khan, A.U.; Yan, A.; Cheung, G.S.P. Biofilms in Endodontics-Current Status and Future Directions. Int. J. Mol. Sci. 2017, 11, 1748. [Google Scholar] [CrossRef] [Green Version]
- Siqueira, J.F., Jr.; Rôças, I.N. Present status and future directions: Microbiology of endodontic infections. Int. Endod. J. 2022, 55 (Suppl. S3), 512–530. [Google Scholar] [CrossRef]
- Luo, X.; Wan, Q.; Cheng, L.; Xu, R. Mechanisms of bone remodeling and therapeutic strategies in chronic apical periodontitis. Front. Cell. Infect. Microbiol. 2022, 22, 908859. [Google Scholar] [CrossRef]
- Antibiotic Resistance in Dentistry; FDI World Dental Federation. Available online: https://www.fdiworlddental.org/antibiotic-resistance-dentistry (accessed on 24 January 2023).
- Bessa, L.J.; Botelho, J.; Machado, V.; Alves, R.; Mendes, J.J. Managing Oral Health in the Context of Antimicrobial Resistance. Int. J. Environ. Res. Public Health 2022, 19, 16448. [Google Scholar] [CrossRef]
- Griffith, A.; Mateen, A.; Markowitz, K.; Singer, S.R.; Cugini, C.; Shimizu, E.; Wiedman, G.R.; Kumar, V. Alternative Antibiotics in Dentistry: Antimicrobial. Peptides. Pharmaceutics 2022, 14, 1679. [Google Scholar] [CrossRef]
- Gan, T.J. Diclofenac: An update on its mechanism of action and safety profile. Curr. Med. Res. Opin. 2010, 26, 1715–1731. [Google Scholar] [CrossRef]
- Mazumdar, K.; Dastidar, S.G.; Park, J.H.; Dutta, N.K. The anti-inflammatory non-antibiotic helper compound diclofenac: An antibacterial drug target. Eur. J. Clin. Microbiol. Infect. Dis. 2009, 28, 881–891. [Google Scholar] [CrossRef]
- Leão, C.; Borges, A.; Simões, M. NSAIDs as a Drug Repurposing Strategy for Biofilm Control. Antibiotics 2020, 9, 591. [Google Scholar] [CrossRef]
- Oliveira, I.M.; Borges, A.; Borges, F.; Simões, M. Repurposing ibuprofen to control Staphylococcus aureus biofilms. Eur. J. Med. Chem. 2019, 166, 197–205. [Google Scholar] [CrossRef]
- Lagadinou, M.; Onisor, M.O.; Rigas, A.; Musetescu, D.V.; Gkentzi, D.; Assimakopoulos, S.F.; Panos, G.; Marangos, M. Antimicrobial Properties on Non-Antibiotic Drugs in the Era of Increased Bacterial Resistance. Antibiotics 2020, 9, 107. [Google Scholar] [CrossRef] [Green Version]
- Ørstavik, D. Essential Endodontology: Prevention and Treatment of Apical Periodontitis, 3rd ed.; Blackwell Science: Oxford, UK, 2019; pp. 1–10. [Google Scholar]
- Ferrer-Luque, C.M.; Conde-Ortiz, A.; Arias-Moliz, M.T.; Valderrama, M.J.; Baca, P. Residual activity of chelating agents and their combinations with cetrimide on root canals infected with Enterococcus faecalis. J. Endod. 2012, 38, 826–828. [Google Scholar] [CrossRef]
- Valverde, M.E.; Baca, P.; Ceballos, L.; Fuentes, M.V.; Ruiz-Linares, M.; Ferrer-Luque, C.M. Antibacterial efficacy of several intracanal medicaments for endodontic therapy. Dent. Mater. J. 2017, 36, 319–324. [Google Scholar] [CrossRef] [Green Version]
- Valderrama, P.; Baca, P.; Solana, C.; Ferrer-Luque, C.M. Root Canal Disinfection Articles with the Highest Relative Citation Ratios. A Bibliometric Analysis from 1990 to 2019. Antibiotics 2021, 10, 1412. [Google Scholar] [CrossRef]
- Vasincu, I.M.; Apotrosoaei, M.; Constantin, S.; Butnaru, M.; Vereștiuc, L.; Lupușoru, C.E.; Buron, F.; Routier, S.; Lupașcu, D.; Taușer, R.G.; et al. New ibuprofen derivatives with thiazolidine-4-one scaffold with improved pharmaco-toxicological profile. BMC Pharmacol. Toxicol. 2021, 22, 10. [Google Scholar] [CrossRef]
- Salem-Milani, A.; Balaei-Gajan, E.; Rahimi, S.; Moosavi, Z.; Abdollahi, A.; Zakeri-Milani, P.; Bolourian, M. Antibacterial Effect of Diclofenac Sodium on Enterococcus faecalis. J. Dent. 2013, 10, 16–22. [Google Scholar]
- Karataş, E.; Baltacı, M.Ö.; Uluköylü, E.; Adıgüzel, A. Antibacterial effectiveness of calcium hydroxide alone or in combination with Ibuprofen and Ciprofloxacin in teeth with asymptomatic apical periodontitis: A randomized controlled clinical study. Int. Endod. J. 2020, 53, 742–753. [Google Scholar] [CrossRef]
- Altman, R.; Bosch, B.; Brune, K.; Patrignani, P.; Young, C. Advances in NSAID development: Evolution of diclofenac products using pharmaceutical technology. Drugs 2015, 75, 859–877. [Google Scholar] [CrossRef] [Green Version]
- Lane, N.E. Pain management in osteoarthritis: The role of COX-2 inhibitors. J. Rheumatol. Suppl. 1997, 49, 20–24. [Google Scholar]
- Ferrer-Luque, C.M.; Baca, P.; Solana, C.; Rodríguez-Archilla, A.; Arias-Moliz, M.T.; Ruiz-Linares, M. Antibiofilm Activity of Diclofenac and Antibiotic Solutions in Endodontic Therapy. J. Endod. 2021, 47, 1138–1143. [Google Scholar] [CrossRef]
- De Freitas, R.P.; Greatti, V.R.; Alcalde, M.P.; Cavenago, B.C.; Vivan, R.R.; Duarte, M.A.; Weckwerth, A.C.; Weckwerth, P.H. Effect of the Association of Nonsteroidal Anti-inflammatory and Antibiotic Drugs on Antibiofilm Activity and pH of Calcium Hydroxide Pastes. J. Endod. 2017, 43, 131–134. [Google Scholar] [CrossRef] [Green Version]
- Da Silva, G.F.; Cesário, F.; Garcia, A.M.R.; Weckwerth, P.H.; Duarte, M.A.H.; de Oliveira, R.C.; Vivan, R.R. Effect of association of non-steroidal anti-inflammatory and antibiotic agents with calcium hydroxide pastes on their cytotoxicity and biocompatibility. Clin. Oral Investig. 2020, 24, 757–763. [Google Scholar] [CrossRef]
- Ruiz-Linares, M.; Solana, C.; Baca, P.; Arias-Moliz, M.T.; Ferrer-Luque, C.M. Antibiofilm potential over time of a tricalcium silicate material and its association with sodium diclofenac. Clin. Oral Investig. 2022, 26, 2661–2669. [Google Scholar] [CrossRef]
- Ruiz-Linares, M.; Monroy-Rojas, J.F.; Solana, C.; Baca, P.; Aguado, B.; Soriano-Lerma, A.; Arias-Moliz, M.T.; Ferrer-Luque, C.M. Antimicrobial potential of new diclofenac hydrogels for disinfection in regenerative endodontics: An in vitro and ex vivo study. Int. Endod. J. 2022, 56, 103–117. [Google Scholar] [CrossRef]
- Barbarossa, A.; Rosato, A.; Corbo, F.; Clodoveo, M.L.; Fracchiolla, G.; Carrieri, A.; Carocci, A. Non-Antibiotic Drug Repositioning as an Alternative Antimicrobial Approach. Antibiotics 2022, 11, 816. [Google Scholar] [CrossRef]
- He, J.; Hwang, G.; Liu, Y.; Gao, L.; Kilpatrick-Liverman, L.; Santarpia, P.; Zhou, X.; Koo, H. l-Arginine Modifies the exopolysaccharide Matrix and Thwarts Streptococcus mutans Outgrowth within Mixed-Species Oral Biofilms. J Bacteriol. 2016, 198, 2651–2661. [Google Scholar] [CrossRef] [Green Version]
- Zaura, E.; Twetman, S. Critical Appraisal of Oral Pre- and Probiotics for Caries Prevention and Care. Caries Res. 2019, 53, 514–526. [Google Scholar] [CrossRef]
- Huang, X.; Zhang, K.; Deng, M.; Exterkate, R.; Liu, C.; Zhou, X.; Cheng, L.; Ten Cate, J.M. Effect of arginine on the growth and biofilm formation of oral bacteria. Arch. Oral Biol. 2017, 82, 256–262. [Google Scholar] [CrossRef]
- Agnello, M.; Cen, L.; Tran, N.C.; Shi, W.; McLean, J.S.; He, X. Arginine Improves pH Homeostasis via Metabolism and Microbiome Modulation. J. Dent. Res. 2017, 96, 924–930. [Google Scholar] [CrossRef]
- Bijle, M.N.; Pichika, M.R.; Mak, K.K.; Parolia, A.; Babar, M.G.; You, C.; Daood, U. Concentration-Dependent Multi-Potentiality of L-Arginine: Antimicrobial Effect, Hydroxyapatite Stability, and MMPs Inhibition. Molecules 2021, 26, 6605. [Google Scholar] [CrossRef]
- Bijle, M.N.; Ashraf, U.; Abdalla, M.M.; Neelakantan, P.; Yiu, C.K.Y. Biofilm modulatory response of arginine-fluoride varnish on multi-species biofilm. J. Dent. 2022, 122, 104096. [Google Scholar] [CrossRef]
- Paes Leme, R.C.; da Silva, R.B. Antimicrobial Activity of Non-steroidal Anti-inflammatory Drugs on Biofilm: Current Evidence and Potential for Drug Repurposing. Front. Microbiol. 2021, 12, 707629. [Google Scholar] [CrossRef]
- Nair, P.N.; Henry, S.; Cano, V.; Vera, J. Microbial status of apical root canal system of human mandibular first molars with primary apical periodontitis after “one-visit” endodontic treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 99, 231–252. [Google Scholar] [CrossRef]
- Kim, S.H.; Semenya, D.; Castagnolo, D. Antimicrobial drugs bearing guanidine moieties: A review. Eur. J. Med. Chem. 2021, 216, 113293. [Google Scholar] [CrossRef]
- Vukomanovic, M.; Gazvoda, L.; Kurtjak, M.; Hrescak, J.; Jaklic, B.; Moya-Andérico, L.; Cendra, M.D.M.; Torrents, E. Development of a ternary cyclodextrin-arginine-ciprofloxacin antimicrobial complex with enhanced stability. Commun. Biol. 2022, 5, 1234. [Google Scholar] [CrossRef]
- Dan Córdoba, A.V.; Aiassa, V.; Dimmer, J.A.; Barrionuevo, C.N.; Quevedo, M.A.; Longhi, M.R.; Zoppi, A. Development and Characterization of Pharmaceutical Systems Containing Rifampicin. Pharmaceutics 2023, 5, 198. [Google Scholar] [CrossRef]
- Lee, T.H.; Hu, C.C.; Lee, S.S.; Chou, M.Y.; Chang, Y.C. Cytotoxicity of chlorhexidine on human osteoblastic cells is related to intracellular glutathione levels. Int. Endod. J. 2010, 43, 430–435. [Google Scholar] [CrossRef]
- Karanikola, T.; Cheva, A.; Sarafidou, K.; Myronidou-Tzouveleki, M.; Tsavdaridis, I.; Kontonasaki, E.; Tsirlis, A. Effect of Diclofenac and Simvastatin on Bone Defect Healing-An In Vivo Animal Study. Biomimetics 2022, 7, 143. [Google Scholar] [CrossRef]
- Oliveira, M.C.G.; Queiroz, Í.O.A.; Machado, T.; Garrido, L.M.A.; Oliveira, S.H.P.; Duarte, M.A.H. Effect of nonsteroidal anti-inflammatory drugs (NSAIDs) association on physicochemical and biological properties of tricalcium silicate-based cement. Braz. Dent. J. 2022, 33, 47–54. [Google Scholar] [CrossRef]
- De Castro Kruly, P.; Alenezi, H.E.H.M.; Manogue, M.; Devine, D.A.; Dame-Teixeira, N.; Garcia, F.C.P.; Do, T. Residual Bacteriome after Chemomechanical Preparation of Root Canals in Primary and Secondary Infections. J. Endod. 2022, 48, 855–863. [Google Scholar] [CrossRef]
- Nagendrababu, V.; Murray, P.E.; Ordinola-Zapata, R.; Peters, O.A.; Rôças, I.N.; Siqueira, J.F., Jr.; Priya, E.; Jayaraman, J.; Pulikkotil, S.J.; Camilleri, J.; et al. PRILE 2021 guidelines for reporting laboratory studies in Endodontology: A consensus-based development. Int. Endod. J. 2021, 54, 1482–1490. [Google Scholar] [CrossRef]
- Ruiz-Linares, M.; Baca, P.; Arias-Moliz, M.T.; Ternero, F.J.; Rodríguez, J.; Ferrer-Luque, C.M. Antibacterial and antibiofilm activity over time of GuttaFlow Bioseal and AH Plus. Dent. Mater. J. 2019, 38, 701–706. [Google Scholar] [CrossRef] [Green Version]
- Chavez de Paz, L.E. Image analysis software based on color segmentation for characterization of viability and physiological activity of biofilms. Appl. Environ. Microbiol. 2009, 75, 1734–1739. [Google Scholar] [CrossRef] [Green Version]
- Solana, C.; Ferrer-Luque, C.M.; Wang, X.; Baca, P.; Ruiz-Linares, M.; Cabrera, T. Cytotoxic effects of alkaline tetrasodium EDTA irrigating solutions. J. Oral Sci. 2020, 62, 285–287. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Solutions | Relative Light Units n = 20 Samples/Group | Biovolume Log10 n = 20 Stack/Group | Green Percentage |
|---|---|---|---|
| 4% DCS | 42,519.35 (35,611.49) a | 4.48 (0.50) a | 13.66 (19.01) a |
| 4% IBP | 78,835.60 (35,920.70) b | 4.37 (0.63) a | 41.19 (26.33) b |
| 4% IBP-arginine | 12,053.65 (3482.41) c | 4.61 (0.30) a | 19.84 (14.68) a |
| 0.9% SS (control) | 361,297.90 (189,230.83) d | 4.81 (0.28) b | 85.91 (9.60) c |
| Comparison p value * | <0.001 | 0.031 | <0.001 |
| Time | Dilutions | Diclofenac | Ibuprofen | Ibuprofen Arginine | p-Value * |
|---|---|---|---|---|---|
| 1 h | 1/10 | 35.14 ± 11.73 a | 38.35 ± 11.35 a | 37.95 ± 11.83 a | 0.758 |
| 1/100 | 41.93 ± 11.48 1,A | 78.89 ± 12.44 2,A | 62.14 ± 11.71 3,A | <0.001 | |
| p-value ** | 0.163 | <0.001 | <0.001 | ||
| 24 h | 1/10 | 29.95 ± 9.1 a | 31.25 ± 9.59 a | 30.38 ± 9.28 a | 0.943 |
| 1/100 | 30.1 ± 8.97 1,B | 50.31 ± 12.283 2,B | 60.18 ± 9.59 2,A | <0.001 | |
| p-value ** | 0.963 | <0.001 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferrer-Luque, C.M.; Solana, C.; Aguado, B.; Ruiz-Linares, M. Antimicrobial Activity and Cytotoxicity of Nonsteroidal Anti-Inflammatory Drugs against Endodontic Biofilms. Antibiotics 2023, 12, 450. https://doi.org/10.3390/antibiotics12030450
Ferrer-Luque CM, Solana C, Aguado B, Ruiz-Linares M. Antimicrobial Activity and Cytotoxicity of Nonsteroidal Anti-Inflammatory Drugs against Endodontic Biofilms. Antibiotics. 2023; 12(3):450. https://doi.org/10.3390/antibiotics12030450
Chicago/Turabian StyleFerrer-Luque, Carmen María, Carmen Solana, Beatriz Aguado, and Matilde Ruiz-Linares. 2023. "Antimicrobial Activity and Cytotoxicity of Nonsteroidal Anti-Inflammatory Drugs against Endodontic Biofilms" Antibiotics 12, no. 3: 450. https://doi.org/10.3390/antibiotics12030450