
Real-World Clinical Outcomes of Molnupiravir for the Treatment of Mild to Moderate COVID-19 in Adult Patients during the Dominance of the Omicron Variant: A Meta-Analysis


Abstract
:1. Introduction
2. Method
2.1. Data Search and Extraction
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Definitions
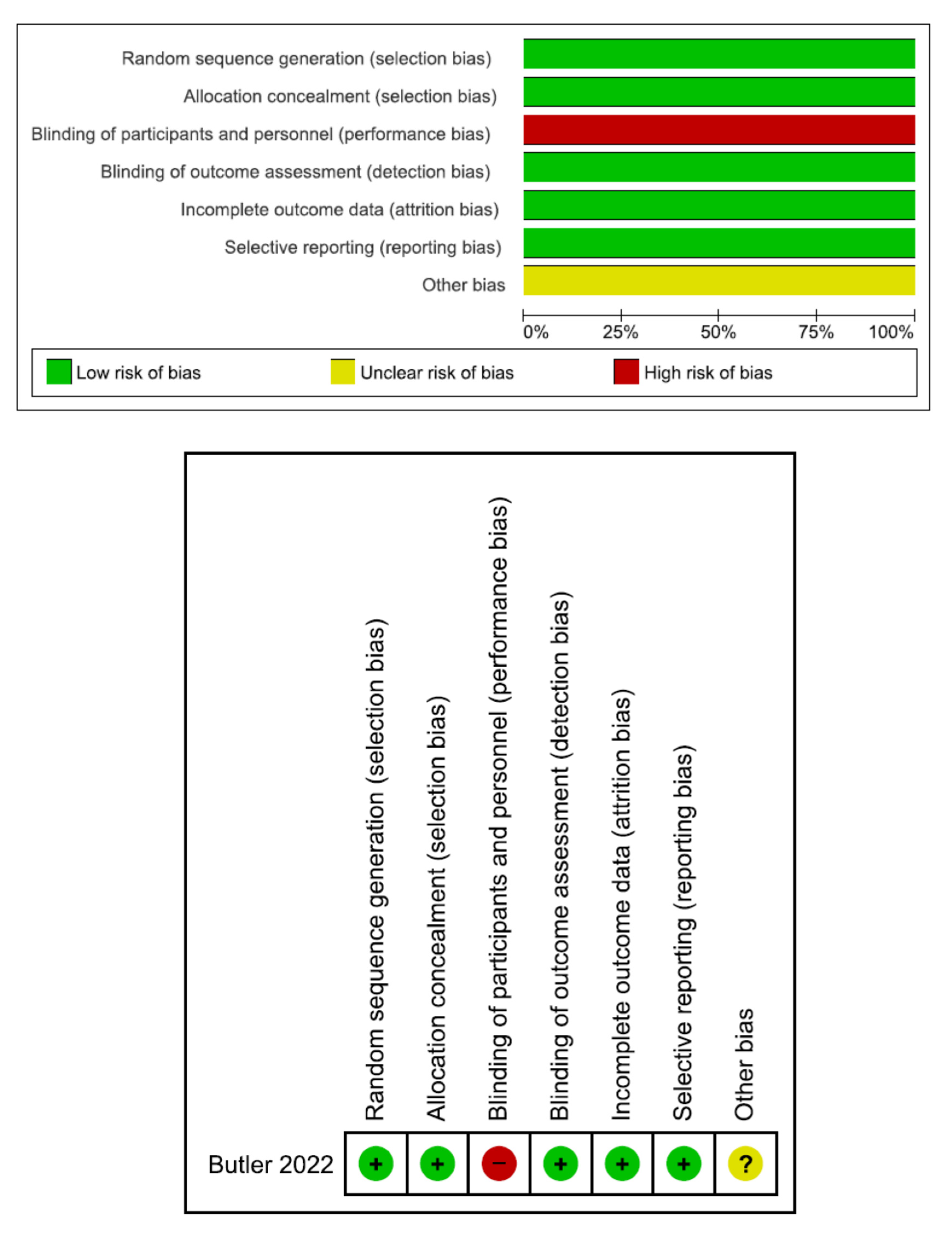
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
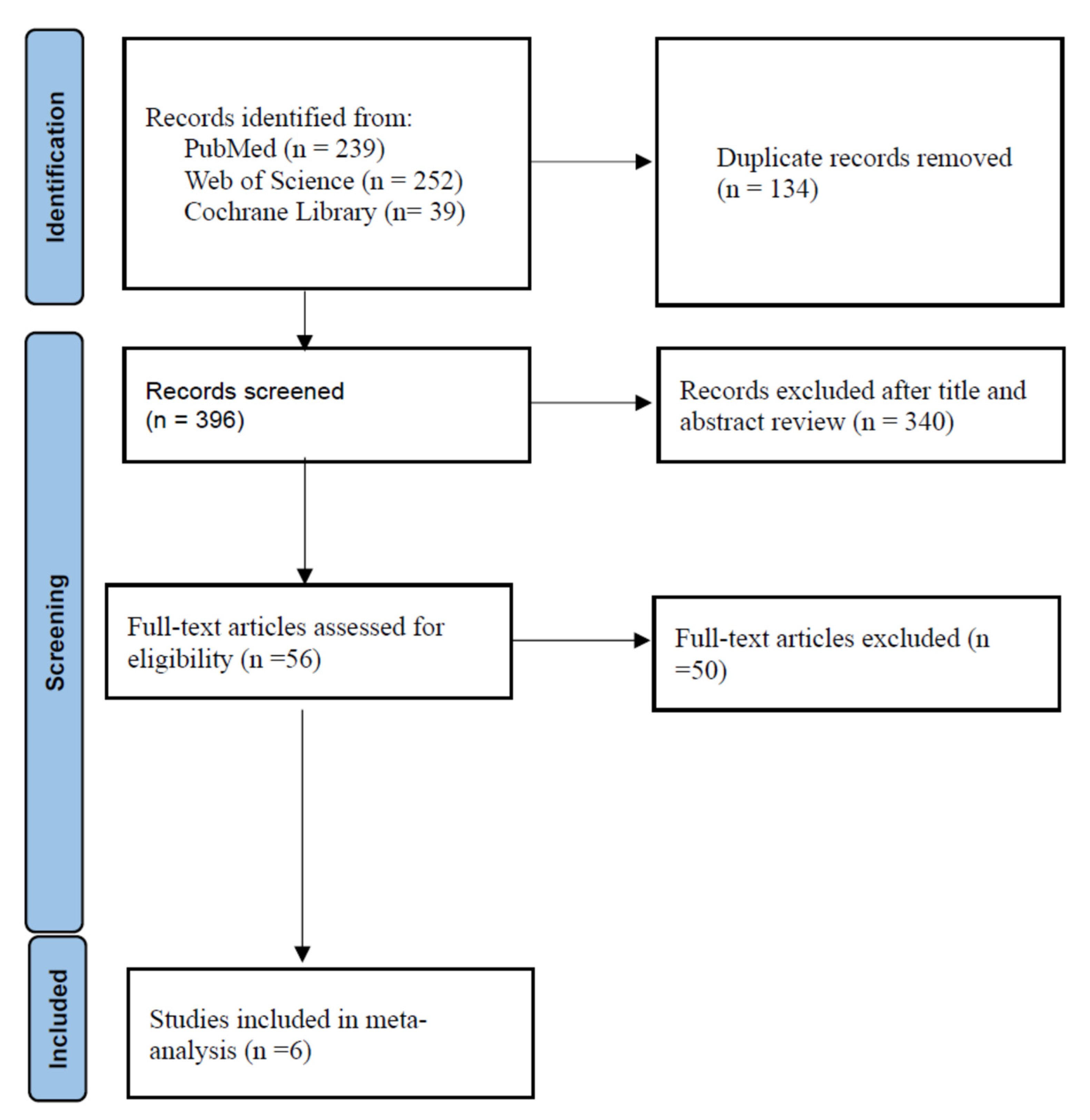
3.1. Characteristics of the Included Studies
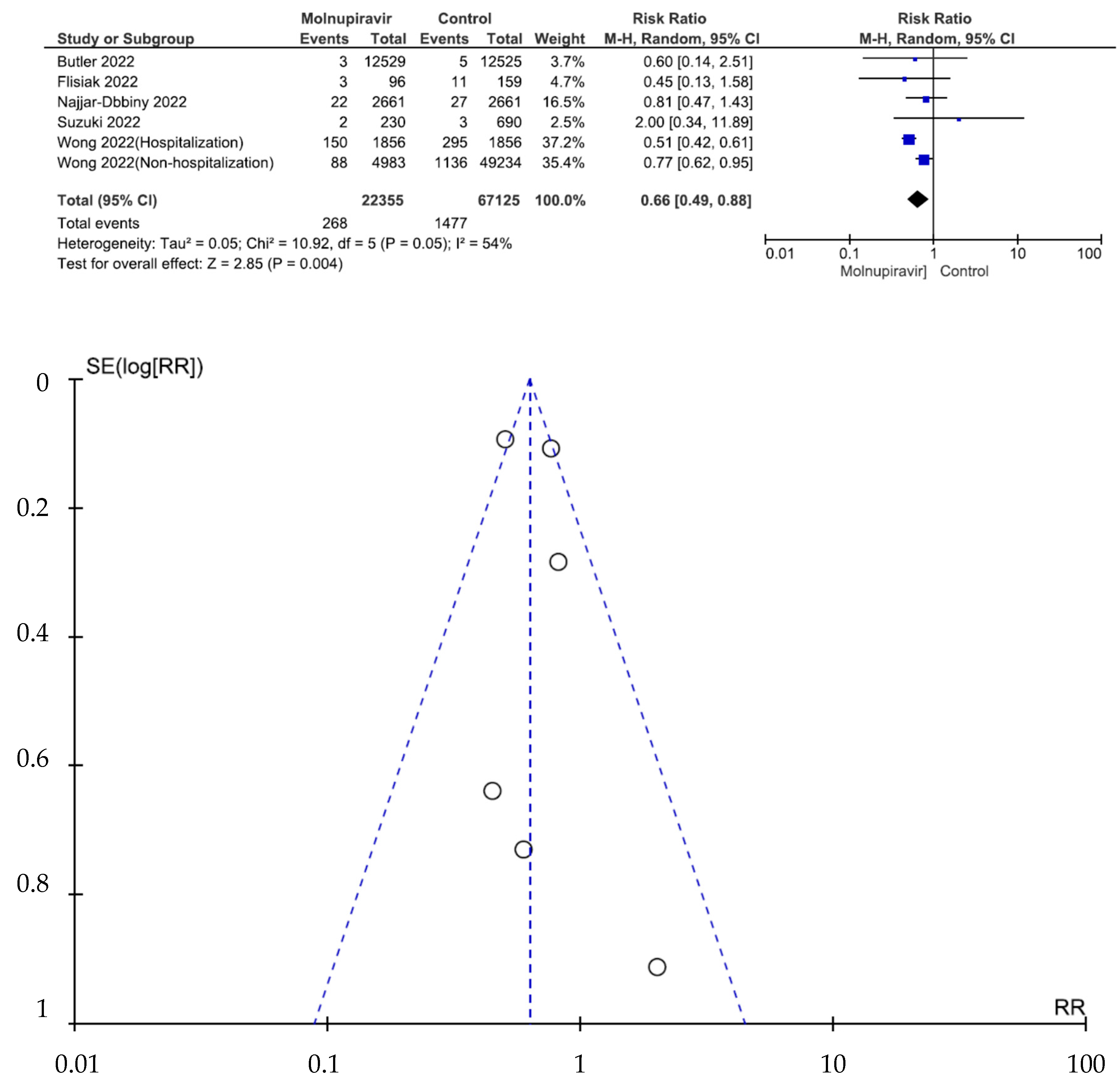
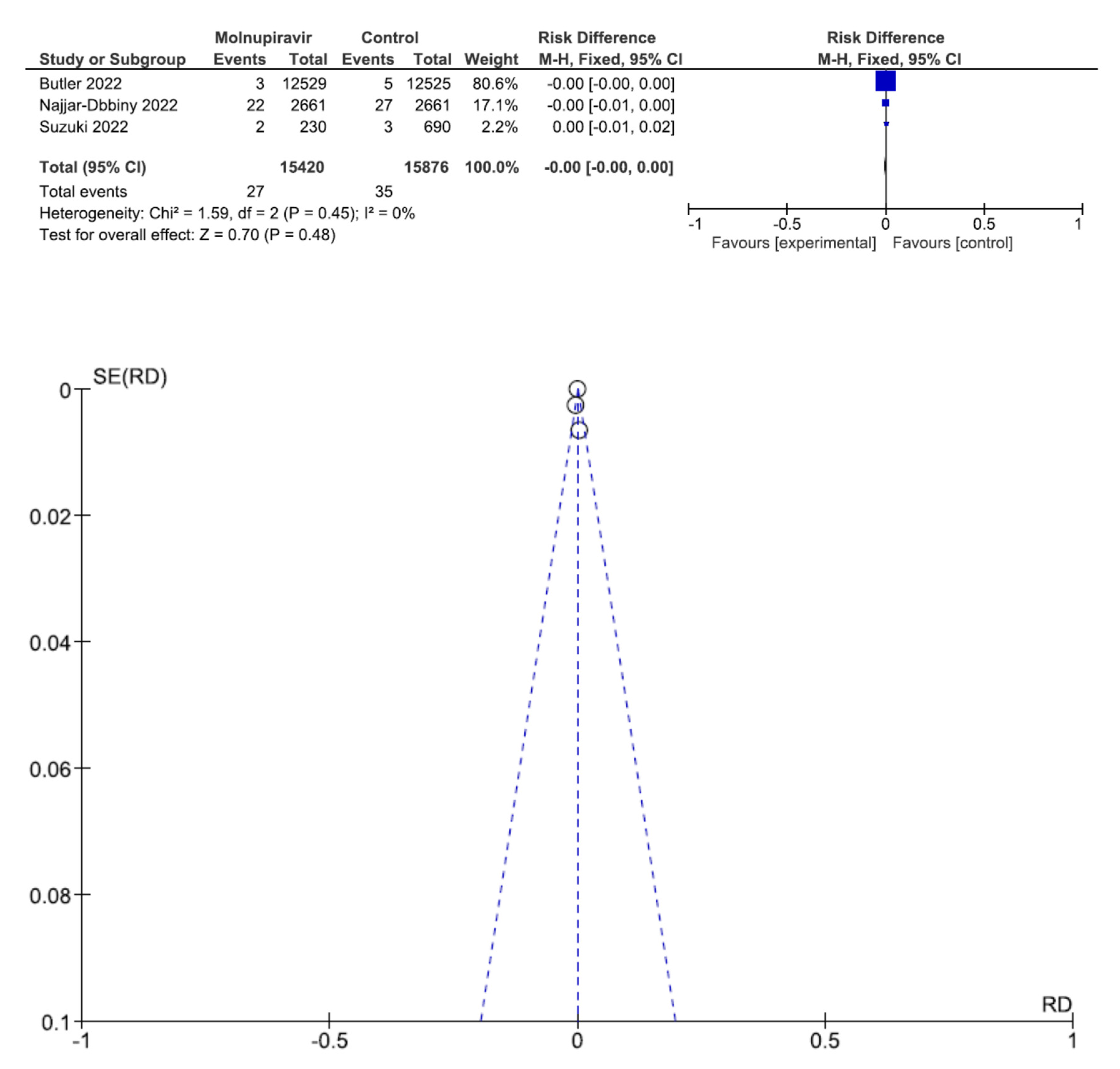
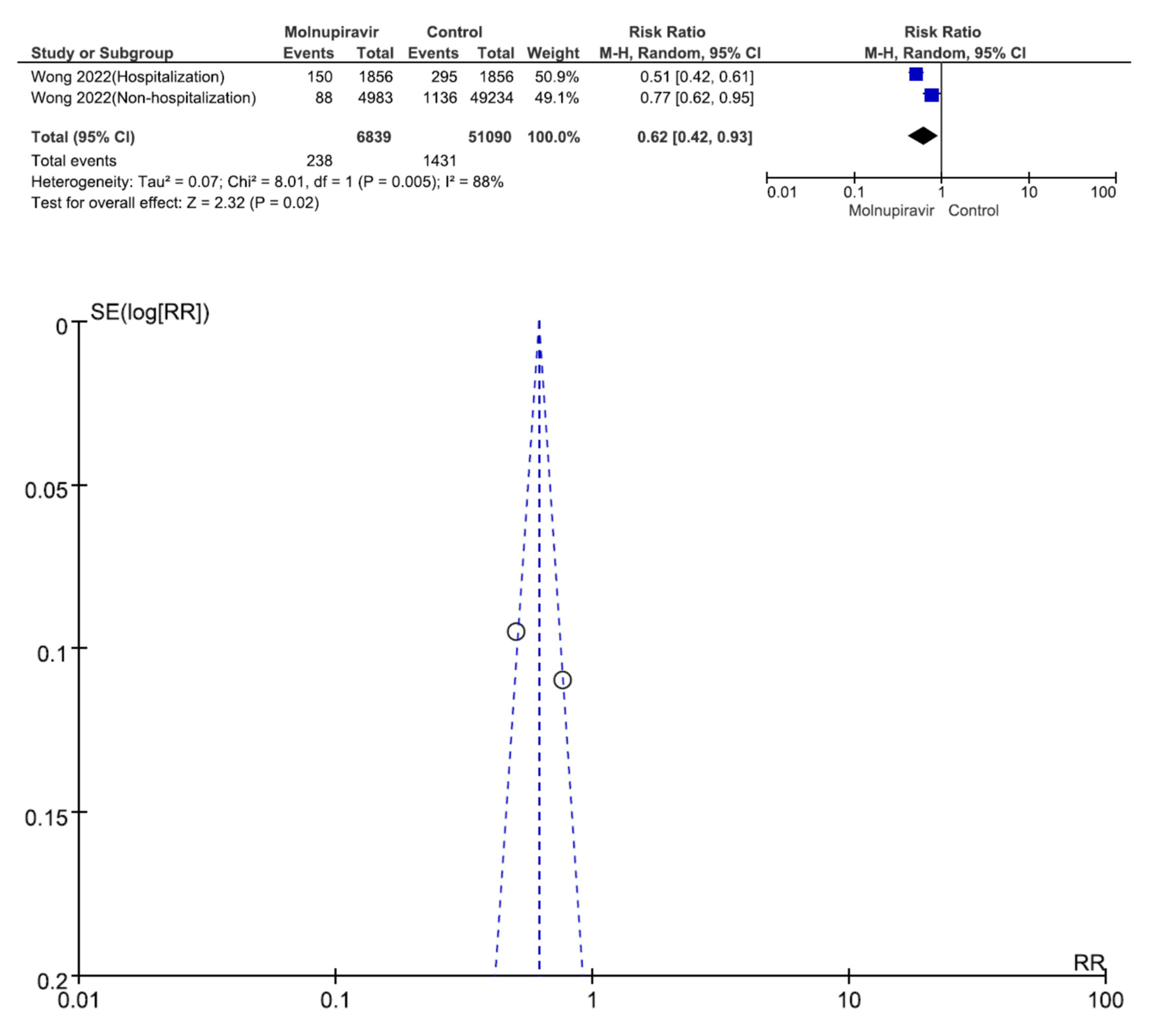
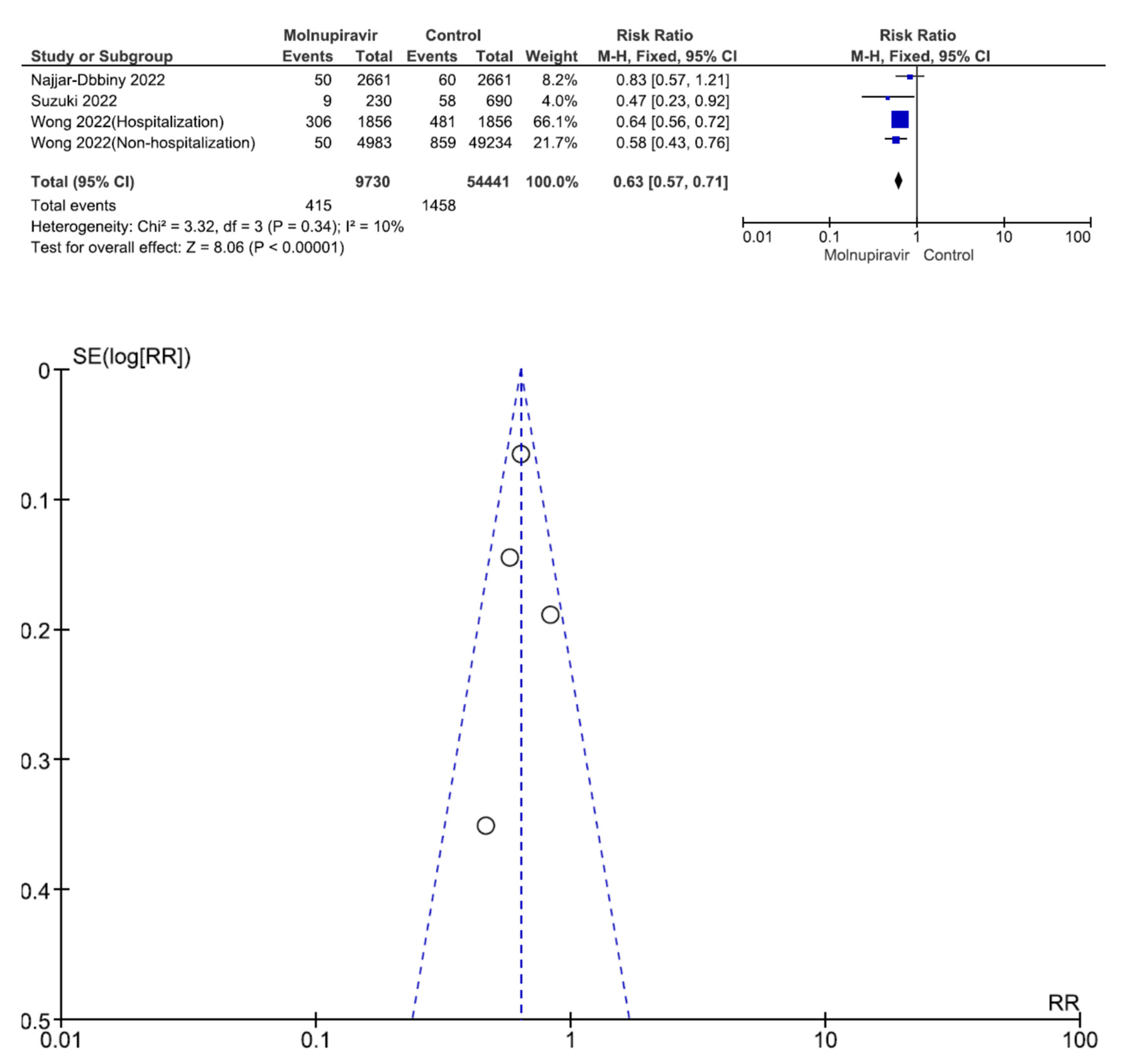
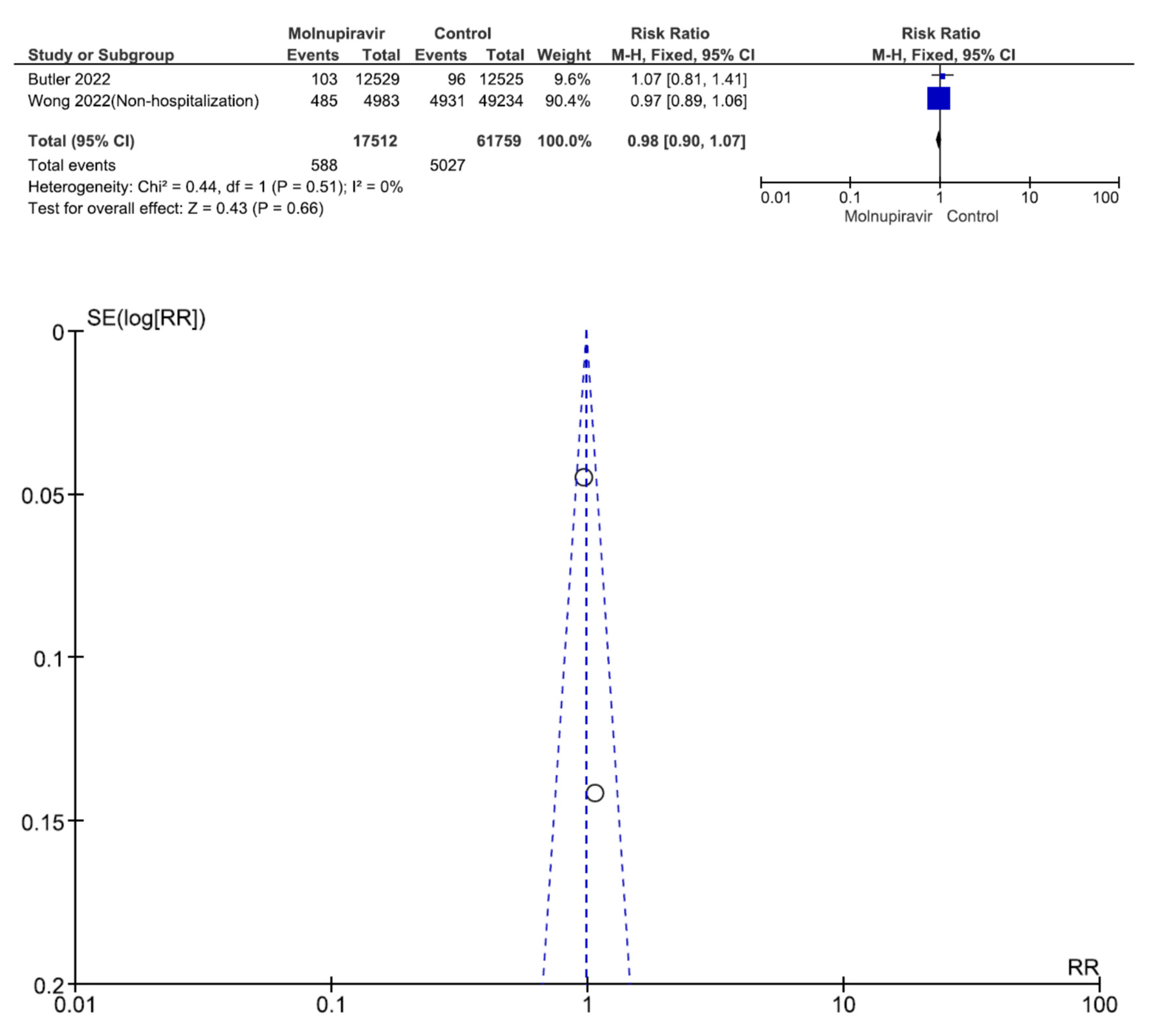
3.2. Effectiveness and Safety Outcomes
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Institutes of Health. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. 2022. Available online: https://www.covid19treatmentguidelines.nih.gov (accessed on 17 February 2022).
- Yuki, K.; Fujiogi, M.; Koutsogiannaki, S. COVID-19 pathophysiology: A review. Clin. Immunol. 2020, 215, 108427. [Google Scholar] [CrossRef] [PubMed]
- US Food and Drug Administration. Fact Sheet for Healthcare Providers: Emergency Use Authorization for Molnupiravir. Available online: https://www.fda.gov/media/155054/download (accessed on 15 January 2022).
- US Food and Drug Administration. Available online: https://www.fda.gov/media/155241/download (accessed on 17 July 2022).
- Hammond, J.; Leister-Tebbe, H.; Gardner, A.; Abreu, P.; Bao, W.; Wisemandle, W.; Baniecki, M.; Hendrick, V.M.; Damle, B.; Simón-Campos, A.; et al. EPIC-HR Investigators. Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with COVID-19. N. Engl. J. Med. 2022, 386, 1397–1408. [Google Scholar] [CrossRef] [PubMed]
- Malone, B.; Campbell, E.A. Molnupiravir: Coding for catastrophe. Nat. Struct. Mol. Biol. 2021, 28, 706–708. [Google Scholar] [CrossRef]
- Gordon, C.J.; Tchesnokov, E.P.; Schinazi, R.F.; Götte, M. Molnupiravir promotes SARS-CoV-2 mutagenesis via the RNA template. J. Biol. Chem. 2021, 297, 100770. [Google Scholar] [CrossRef] [PubMed]
- Vicenti, I.; Zazzi, M.; Saladini, F. SARS-CoV-2 RNA-dependent RNA polymerase as a therapeutic target for COVID-19. Expert Opin. Ther. Pat. 2021, 31, 325–337. [Google Scholar] [CrossRef]
- Cox, R.M.; Wolf, J.D.; Plemper, R.K. Therapeutically administered ribonucleoside analogue MK-4482/EIDD-2801 blocks SARS-CoV-2 transmission in ferrets. Nat. Microbiol. 2021, 6, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Wahl, A.; Gralinski, L.E.; Johnson, C.E.; Yao, W.; Kovarova, M.; Dinnon, K.H., III; Liu, H.; Madden, V.J.; Krzystek, H.M.; De, C.; et al. SARS-CoV-2 infection is effectively treated and prevented by EIDD-2801. Nature 2021, 591, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Abdelnabi, R.; Foo, C.S.; De Jonghe, S.; Maes, P.; Weynand, B.; Neyts, J. Molnupiravir Inhibits Replication of the Emerging SARS-CoV-2 Variants of Concern in a Hamster Infection Model. J. Infect. Dis. 2021, 224, 749–753. [Google Scholar] [CrossRef]
- Agostini, M.L.; Pruijssers, A.J.; Chappell, J.D.; Gribble, J.; Lu, X.; Andres, E.L.; Bluemling, G.R.; Lockwood, M.A.; Sheahan, T.P.; Sims, A.C.; et al. Small-Molecule Antiviral β-d-N4-Hydroxycytidine Inhibits a Proofreading-Intact Coronavirus with a High Genetic Barrier to Resistance. J. Virol. 2019, 93, e01348-19. [Google Scholar] [CrossRef] [Green Version]
- Saravolatz, L.D.; Depcinski, S.; Sharma, M. Molnupiravir and Nirmatrelvir-Ritonavir: Oral COVID Antiviral Drugs. Clin. Infect. Dis. 2023, 76, 165–171. [Google Scholar] [CrossRef]
- Minotti, C.; Mengato, D.; De Pieri, M.; Trivellato, S.; Francavilla, A.; Di Chiara, C.; Liberati, C.; Mattera, R.; Biffi, A.; Giaquinto, C.; et al. Early Treatments of Fragile Children with COVID-19-Results of CLEVER (Children COVID Early Treatment), a Retrospective, Observational Study. Viruses 2023, 15, 192. [Google Scholar] [CrossRef] [PubMed]
- Bernal, A.J.; Gomes da Silva, M.M.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Delos Reyes, V.; Martín-Quirós, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. MOVe-OUT Study Group. Molnupiravir for Oral Treatment of COVID-19 in Nonhospitalized Patients. N. Engl. J. Med. 2022, 386, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, T.; Ferguson, N.M.; Nash, S.G.; Webster, H.H.; Flaxman, S.; Andrews, N.; Hinsley, W.; Bernal, J.L.; Kall, M.; Bhatt, S.; et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: A cohort study. Lancet 2022, 399, 1303–1312. [Google Scholar] [CrossRef]
- Wolter, N.; Jassat, W.; Walaza, S.; Welch, R.; Moultrie, H.; Groome, M.; Amoako, D.G.; Everatt, J.; Bhiman, J.N.; Scheepers, C.; et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: A data linkage study. Lancet 2022, 399, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Ulloa, A.C.; Buchan, S.A.; Daneman, N.; Brown, K.A. Estimates of SARS-CoV-2 Omicron Variant Severity in Ontario, Canada. JAMA 2022, 327, 1286–1288. [Google Scholar] [CrossRef]
- Veneti, L.; Bøås, H.; Bråthen Kristoffersen, A.; Stålcrantz, J.; Bragstad, K.; Hungnes, O.; Storm, M.L.; Aasand, N.; Rø, G.; Starrfelt, J.; et al. Reduced risk of hospitalisation among reported COVID-19 cases infected with the SARS-CoV-2 Omicron, B.A.;1 variant compared with the Delta variant, Norway, December 2021 to January 2022. Eurosurveillance 2022, 27, 2200077. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, F.; Myers, J.; Basu, D.; Tintinger, G.; Ueckermann, V.; Mathebula, M.; Ramlall, R.; Spoor, S.; de Villiers, T.; Van der Walt, Z.; et al. Decreased severity of disease during the first global omicron variant COVID-19 outbreak in a large hospital in tshwane, south africa. Int. J. Infect. Dis. 2022, 116, 38–42. [Google Scholar] [CrossRef]
- Yip, T.C.F.; Lui, G.C.Y.; Lai, M.S.M.; Wong, V.W.S.; Tse, Y.K.; Ma, B.H.M.; Hui, E.; Leung, M.K.W.; Chan, H.L.Y.; Hui, D.S.C.; et al. Impact of the Use of Oral Antiviral Agents on the Risk of Hospitalization in Community Coronavirus Disease 2019 Patients (COVID-19). Clin. Infect. Dis. 2023, 76, e26–e33. [Google Scholar] [CrossRef]
- Wai, A.K.; Chan, C.Y.; Cheung, A.W.; Wang, K.; Chan, S.C.; Lee, T.T.; Luk, L.Y.; Yip, E.T.; Ho, J.W.; Tsui, O.W.; et al. Association of Molnupiravir and Nirmatrelvir-Ritonavir with preventable mortality, hospital admissions and related avoidable healthcare system cost among high-risk patients with mild to moderate COVID-19. Lancet Reg Health West Pac. 2023, 30, 100602. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Atkins, D.; Eccles, M.; Flottorp, S.; Guyatt, G.H.; Henry, D.; Hill, S.; Liberati, A.; O’Connell, D.; Oxman, A.D.; Phillips, B.; et al. GRADE Working Group. Systems for grading the quality of evidence and the strength of recommendations I: Critical appraisal of existing approaches The GRADE Working Group. BMC Health Serv. Res. 2004, 4, 38. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butler, C.C.; Hobbs, F.D.R.; Gbinigie, O.A.; Rahman, N.M.; Hayward, G.; Richards, D.B.; Dorward, J.; Lowe, D.M.; Standing, J.F.; Breuer, J.; et al. PANORAMIC Trial Collaborative Group. Molnupiravir plus usual care versus usual care alone as early treatment for adults with COVID-19 at increased risk of adverse outcomes (PANORAMIC): An open-label, platform-adaptive randomised controlled trial. Lancet 2022, 401, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Flisiak, R.; Zarębska-Michaluk, D.; Rogalska, M.; Kryńska, J.A.; Kowalska, J.; Dutkiewicz, E.; Dobrowolska, K.; Jaroszewicz, J.; Moniuszko-Malinowska, A.; Rorat, M.; et al. Real-world experience with molnupiravir during the period of SARS-CoV-2 Omicron variant dominance. Pharmacol. Rep. 2022, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Najjar-Debbiny, R.; Gronich, N.; Weber, G.; Khoury, J.; Amar, M.; Stein, N.; Goldstein, L.H.; Saliba, W. Effectiveness of Molnupiravir in High Risk Patients: A Propensity Score Matched Analysis. Clin. Infect. Dis. 2023, 76, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Shibata, Y.; Minemura, H.; Nikaido, T.; Tanino, Y.; Fukuhara, A.; Kanno, R.; Saito, H.; Suzuki, S.; Inokoshi, Y.; et al. Real-world clinical outcomes of treatment with molnupiravir for patients with mild-to-moderate coronavirus disease 2019 during the Omicron variant pandemic. Clin. Exp. Med. 2022, 5, 1–9. [Google Scholar] [CrossRef]
- Wong, C.K.H.; Au, I.C.H.; Lau, K.T.K.; Lau, E.H.Y.; Cowling, B.J.; Leung, G.M. Real-world effectiveness of early molnupiravir or nirmatrelvir-ritonavir in hospitalised patients with COVID-19 without supplemental oxygen requirement on admission during Hong Kong’s omicron, B.A.;2 wave: A retrospective cohort study. Lancet Infect. Dis. 2022, 22, 1681–1693. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.K.H.; Au, I.C.H.; Lau, K.T.K.; Lau, E.H.Y.; Cowling, B.J.; Leung, G.M. Real-world effectiveness of molnupiravir and nirmatrelvir plus ritonavir against mortality, hospitalisation, and in-hospital outcomes among community-dwelling, ambulatory patients with confirmed SARS-CoV-2 infection during the omicron wave in Hong Kong: An observational study. Lancet 2022, 10359, 1213–1222. [Google Scholar] [CrossRef]
- Fatima, M.; Azeem, S.; Saeed, J.; Shahid, A.; Cheema, H.A. COVID-19 Therapeutics Study Group. Efficacy and safety of molnupiravir for COVID-19 patients. Eur. J. Intern Med. 2022, 102, 118–121. [Google Scholar] [CrossRef]
- Tippabhotla, S.K.; Lahiri, D.; Kandi, C. Efficacy and Safety of Molnupiravir for the Treatment of Non-Hospitalized Adults With Mild COVID-19: A Randomized, Open-Label, Parallel-Group Phase 3 Trial. Available online: https://ssrn.com/abstract=4042673 (accessed on 17 June 2021).
- Fischer, W.; Eron, J.J.; Holman, W.; Cohen, M.S.; Fang, L.; Szewczyk, L.J.; Sheahan, T.P.; Baric, R.; Mollan, K.R.; Wolfe, C.R.; et al. Molnupiravir, an Oral Antiviral Treatment for COVID-19. MedRxiv 2021, 17. [Google Scholar] [CrossRef]
- Caraco, Y.; Crofoot, G.E.; Moncada, P.A.; Galustyan, A.N.; Musungaie, D.B.; Payne, B.; Kovalchuk, E.; Gonzalez, A.; Brown, M.L.; Williams-Diaz, A.; et al. MOVe-OUT Study Group. Phase 2/3 Trial of Molnupiravir for Treatment of COVID-19 in Nonhospitalized Adults. N. Engl. J. Med. 2022, 1, 1–10. [Google Scholar] [CrossRef]
- Arribas, J.R.; Bhagani, S.; Lobo, S.M.; Khaertynova, I.; Mateu, L.; Fishchuk, R.; Park, W.Y.; Hussein, K.; Kim, S.W.; Ghosn, J.; et al. Randomized trial of molnupiravir or placebo in patients hospitalized with COVID-19. NEJM Evid. 2022, 1, EVIDoa2100044. [Google Scholar] [CrossRef]
- Bruno, G.; Giotta, M.; Perelli, S.; De Vita, G.; Bartolomeo, N.; Buccoliero, G.B. Early Access to Oral Antivirals in High-Risk Outpatients: Good Weapons to Fight COVID-19. Viruses 2022, 4, 2514. [Google Scholar] [CrossRef] [PubMed]
- Tiseo, G.; Barbieri, C.; Galfo, V.; Occhineri, S.; Matucci, T.; Almerigogna, F.; Kalo, J.; Sponga, P.; Cesaretti, M.; Marchetti, G.; et al. Efficacy and Safety of Nirmatrelvir/Ritonavir, Molnupiravir, and Remdesivir in a Real-World Cohort of Outpatients with COVID-19 at High Risk of Progression: The PISA Outpatient Clinic Experience. Infect. Dis. Ther. 2022, 28, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Khoo, S.H.; FitzGerald, R.; Saunders, G.; Middleton, C.; Ahmad, S.; Edwards, C.J.; Hadjiyiannakis, D.; Walker, L.; Lyon, R.; Shaw, V.; et al. A Randomised-Controlled Phase 2 trial of Molnupiravir in Unvaccinated and Vaccinated Individuals with Early SARS-CoV-2. MedRxiv 2022, 7, 1–33. [Google Scholar] [CrossRef]
- Pourkarim, F.; Pourtaghi-Anvarian, S.; Rezaee, H. Molnupiravir: A new candidate for COVID-19 treatment. Pharmacol. Res. Perspect. 2022, 10, e00909. [Google Scholar] [CrossRef]
- Painter, W.P.; Holman, W.; Bush, J.A.; Almazedi, F.; Malik, H.; Eraut, N.C.J.E.; Morin, M.J.; Szewczyk, L.J.; Painter, G.R. Human Safety, Tolerability, and Pharmacokinetics of Molnupiravir, a Novel Broad-Spectrum Oral Antiviral Agent with Activity Against SARS-CoV-2. Antimicrob Agents Chemother. 2021, 65, e02428-20. [Google Scholar] [CrossRef]
- Khoo, S.H.; Fitzgerald, R.; Fletcher, T.; Ewings, S.; Jaki, T.; Lyon, R.; Downs, N.; Walker, L.; Tansley-Hancock, O.; Greenhalf, W.; et al. Optimal dose and safety of molnupiravir in patients with early SARS-CoV-2: A Phase, I.; open-label, dose-escalating, randomized controlled study. J. Antimicrob. Chemother. 2021, 76, 3286–3295. [Google Scholar] [CrossRef]
- Khiali, S.; Khani, E.; Rouy, S.B.; Entezari-Maleki, T. Comprehensive review on molnupiravir in COVID-19: A novel promising antiviral to combat the pandemic. Future Microbiol. 2022, 17, 377–391. [Google Scholar] [CrossRef]
- Santi Laurini, G.; Montanaro, N.; Motola, D. Safety Profile of Molnupiravir in the Treatment of COVID-19: A Descriptive Study Based on FAERS Data. J. Clin. Med. 2022, 12, 34. [Google Scholar] [CrossRef]
- Mali, K.R.; Eerike, M.; Raj, G.M.; Bisoi, D.; Priyadarshini, R.; Ravi, G.; Chaliserry, L.F.; Janti, S.S. Efficacy and safety of Molnupiravir in COVID-19 patients: A systematic review. Ir. J. Med. Sci. 2022, 10, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Amani, B.; Zareei, S.; Amani, B. Rapid review and meta-analysis of adverse events associated with molnupiravir in patients with COVID-19. Br. J. Clin. Pharmacol. 2022, 88, 4403–4411. [Google Scholar] [CrossRef] [PubMed]
- Mazzitelli, M.; Mengato, D.; Sasset, L.; Ferrari, A.; Gardin, S.; Scaglione, V.; Bonadiman, N.; Calandrino, L.; Cavinato, S.; Trivellato, S.; et al. Molnupiravir and Nirmatrelvir/Ritonavir: Tolerability, Safety, and Adherence in a Retrospective Cohort Study. Viruses 2023, 15, 384. [Google Scholar] [CrossRef]
- Vena, A.; Traman, L.; Bavastro, M.; Limongelli, A.; Dentone, C.; Magnè, F.; Giacobbe, D.R.; Mikulska, M.; Taramasso, L.; Di Biagio, A.; et al. Early Clinical Experience with Molnupiravir for Mild to Moderate Breakthrough COVID-19 among Fully Vaccinated Patients at Risk for Disease Progression. Vaccines 2022, 10, 1141. [Google Scholar] [CrossRef] [PubMed]
- Arbel, R.; Sagy, Y.W.; Battat, E.; Lavie, G.; Sergienko, R.; Friger, M.; Peretz, A.; Yaron, S.; Serby, D.; Hammerman, A.; et al. Molnupiravir Use and Severe COVID-19 Outcomes during the Omicron Surge. Available online: https://www.researchsquare.com/article/rs-2115769/v1 (accessed on 29 September 2022).
- Gentile, I.; Scotto, R.; Schiano Moriello, N.; Pinchera, B.; Villari, R.; Trucillo, E.; Ametrano, L.; Fusco, L.; Castaldo, G.; Buonomo, A.R.; et al. Nirmatrelvir/Ritonavir and Molnupiravir in the Treatment of Mild/Moderate COVID-19: Results of a Real-Life Study. Vaccines 2022, 10, 1731. [Google Scholar] [CrossRef] [PubMed]
- Wise, J. COVID-19: Molnupiravir does not cut hospital admissions or deaths in vaccinated people at high risk, trial finds. BMJ 2022, 379, o3055. [Google Scholar] [CrossRef] [PubMed]
- Graya, E.J.; Nguyen-Van-Tam, J.S. Molnupiravir for SARS-CoV-2 infection: Public health and policy Implications. J. Infect. 2023, 86, 121–122. [Google Scholar] [CrossRef]
- Kidd, M.R.; Kelly, P.M. PANORAMIC: Important insights into molnupiravir use in COVID-19. Lancet 2023, 401, 250–251. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Study Design | Region | Study Period | Two Vaccine Doses (%) | Setting/SAR-CoV-2 VOC | Mean Age of Patients | Number of Patients |
|---|---|---|---|---|---|---|
| Butler CC, RCT, [26] | UK | December 2021 to April 2022 | Mol (96%) Pla (97%) | Non-hospitalization /Omicron | Mol: 56.7 Y/O Pla: 56.5 Y/O | Mol: 12,529 Pla: 12,525 |
| Flisiak R, RET, [27] | Poland | January 2022 to April 2022 | No data | Hospitalization /Omicron | Mol: 67.4 Y/O Pla: 67.4 Y/O | Mol: 96 Pla: 159 |
| Najjar-Debbiny R, RET, [28] | Israel | January 2022 to February 2022 | Mol (77.3%) Pla (77.3%) | Non-hospitalization /Omicron | Mol: 74.2 Y/O Pla: 55.5 Y/O | Mol: 2661 Pla: 2661 |
| Suzuki Y, RET, [29] | Japan | January 2022 to April 2022 | Mol (82.2%) Pla (81.7%) | Hospitalization /Omicron | M: 64.1 Y/O Pla: 64.7 Y/O | Mol: 230 Pla: 690 |
| Wong CK, RET, [30] | Hong Kong | February 2022 to April 2022 | Mol (6.2%) Pla (9.0%) | Hospitalization /Omicron BA.2 | Mol: 80.8 Y/O Pla: 74.3 Y/O | Mol: 1856 Pla: 1856 |
| Wong CK, RET, [31] | Hong Kong | February 2022 to June 2022 | Mol (16.1%) Pla (12.4%) | Non-hospitalization /Omicron BA.2.2 | Mol: >60 Y/O (88.7%) Pla: >60 Y/O 92.2%) | Mol: 4983 Pla: 49,234 |
| Author/Year | Confounding | Selection | Interventions Classification | Interventions Deviations | Missing Data | Measurement of Outcomes | Selective Results |
|---|---|---|---|---|---|---|---|
| Flisiak R, 2022, [27] | moderate risk | low risk | moderate risk | moderate risk | moderate risk | low risk | moderate risk |
| Najjar-Debbiny R, 2022, [28] | low risk | low risk | moderate risk | moderate risk | moderate risk | low risk | low risk |
| Suzuki Y, 2022, [29] | moderate risk | moderate risk | moderate risk | moderate risk | moderate risk | moderate risk | moderate risk |
| Wong CK, 2022, [30] | moderate risk | low risk | moderate risk | moderate risk | moderate risk | low risk | low risk |
| Wong CK, 2022, [31] | moderate risk | low risk | moderate risk | moderate risk | moderate risk | low risk | low risk |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.; Lu, T.-L.; Lin, L. Real-World Clinical Outcomes of Molnupiravir for the Treatment of Mild to Moderate COVID-19 in Adult Patients during the Dominance of the Omicron Variant: A Meta-Analysis. Antibiotics 2023, 12, 393. https://doi.org/10.3390/antibiotics12020393
Huang C, Lu T-L, Lin L. Real-World Clinical Outcomes of Molnupiravir for the Treatment of Mild to Moderate COVID-19 in Adult Patients during the Dominance of the Omicron Variant: A Meta-Analysis. Antibiotics. 2023; 12(2):393. https://doi.org/10.3390/antibiotics12020393
Chicago/Turabian StyleHuang, Chienhsiu, Tsung-Lung Lu, and Lichen Lin. 2023. "Real-World Clinical Outcomes of Molnupiravir for the Treatment of Mild to Moderate COVID-19 in Adult Patients during the Dominance of the Omicron Variant: A Meta-Analysis" Antibiotics 12, no. 2: 393. https://doi.org/10.3390/antibiotics12020393