

Overruling of Procalcitonin-Guided Antibiotics for Lower Respiratory Tract Infections in Primary Care: Ancillary Study of a Randomized Controlled Trial
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Results
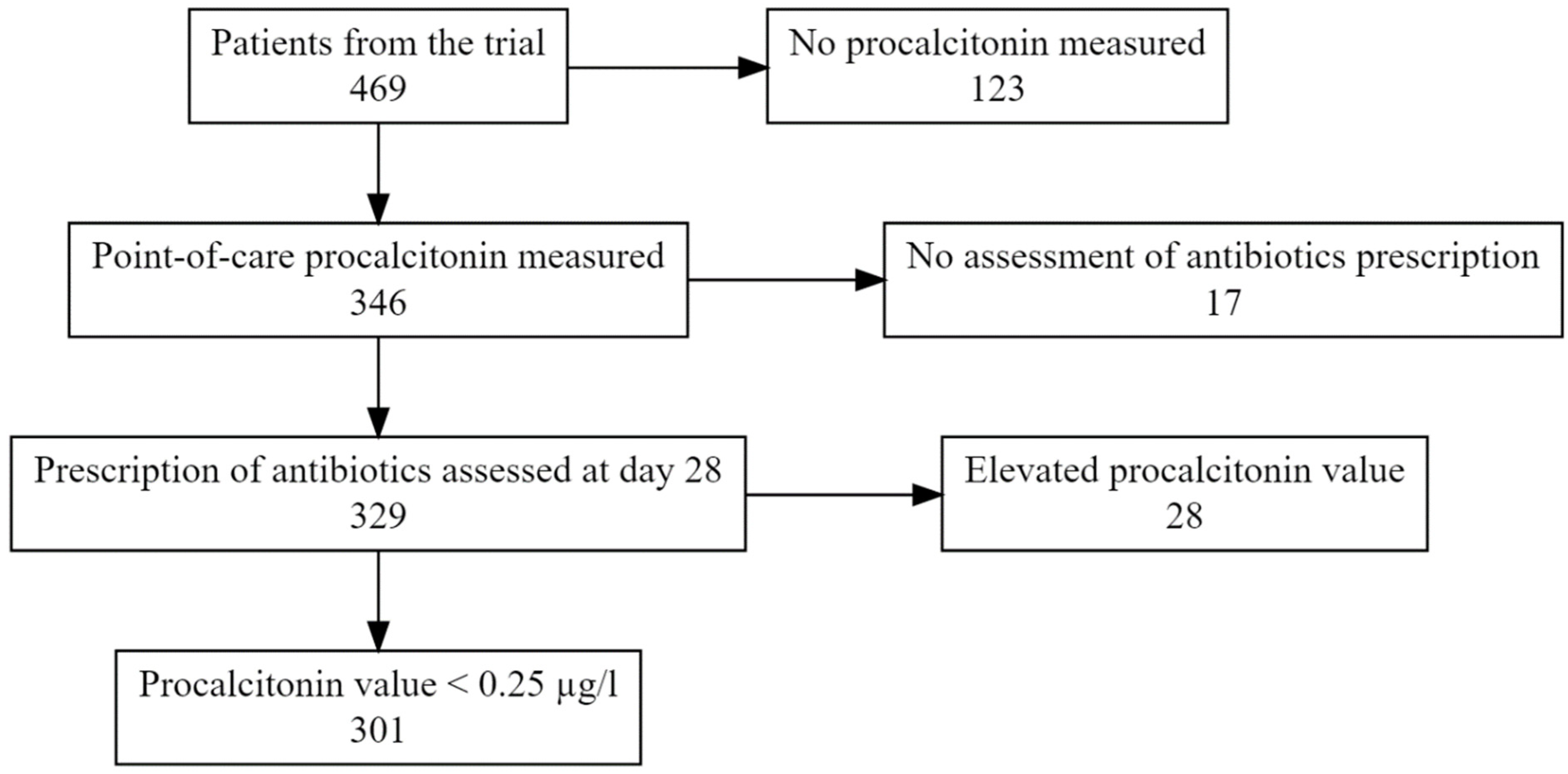
2.1. Participants
2.2. Univariate Analysis
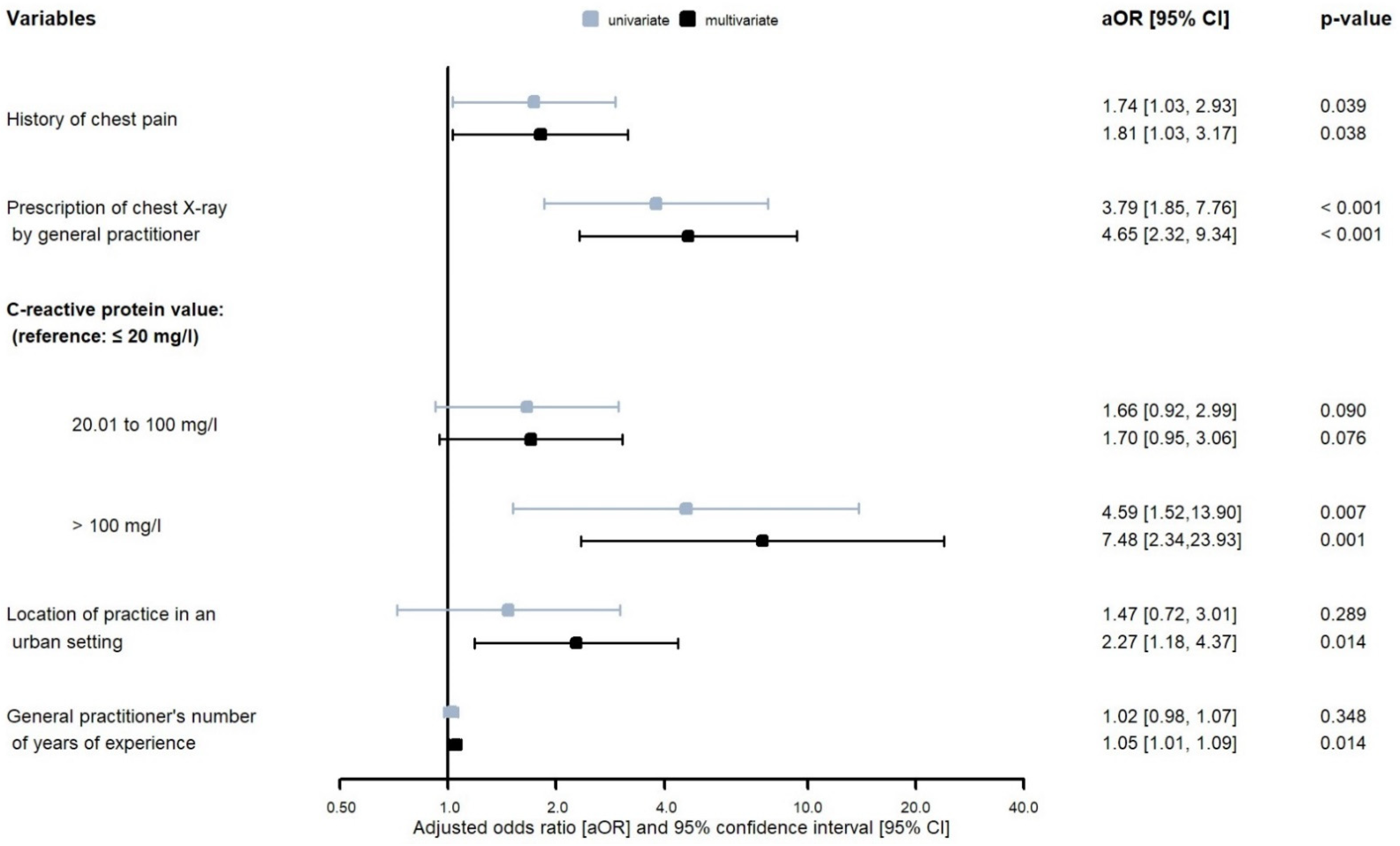
2.3. Multivariate Analysis
3. Discussion
3.1. Summary
3.2. Strengths and Limitations
3.3. Comparison with Previous Studies
3.4. Implications for Research and Practice
4. Materials & Methods
4.1. Study Design and Setting
4.2. Biological Samples and Retrospective Laboratory Analyses
4.3. Study Population and Outcome
4.4. Statistical Analyses
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Robles Aguilar, G.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, M.S.; Peterson, K.; Winthrop, K.; Cantor, A.; Lazur, B.H.; Buckley, D.I. Interventions to reduce inappropriate prescribing of antibiotics for acute respiratory tract infections: Summary and update of a systematic review. J. Int. Med. Res. 2018, 46, 3337–3357. [Google Scholar] [CrossRef] [PubMed]
- Federal Office of Public Health; Federal Food Safety and Veterinary Office. Swiss Antibiotic Resistance Report 2020. Usage of Antibiotics and Occurrence of Antibiotic Resistance in Switzerland; publication number: 2020-OEG-64; FOPH: Bern, Switzerland, 2020. [Google Scholar]
- Butler, C.C.; Hood, K.; Verheij, T.; Little, P.; Melbye, H.; Nuttall, J.; Kelly, M.J.; Mölstad, S.; Godycki-Cwirko, M.; Almirall, J.; et al. Variation in antibiotic prescribing and its impact on recovery in patients with acute cough in primary care: Prospective study in 13 countries. BMJ 2009, 338, b2242. [Google Scholar] [CrossRef] [PubMed]
- Ieven, M.; Coenen, S.; Loens, K.; Lammens, C.; Coenjaerts, F.; Vanderstraeten, A.; Henriques-Normark, B.; Crook, D.; Huygen, K.; Butler, C.C.; et al. Aetiology of lower respiratory tract infection in adults in primary care: A prospective study in 11 European countries. Clin. Microbiol. Infect. 2018, 24, 1158–1163. [Google Scholar] [CrossRef] [PubMed]
- Self, W.H.; Balk, R.A.; Grijalva, C.G.; Williams, D.J.; Zhu, Y.; Anderson, E.J.; Waterer, G.W.; Courtney, D.M.; Bramley, A.M.; Trabue, C.; et al. Procalcitonin as a Marker of Etiology in Adults Hospitalized With Community-Acquired Pneumonia. Clin. Infect. Dis. 2017, 65, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Kutz, A.; Hausfater, P.; Oppert, M.; Alan, M.; Grolimund, E.; Gast, C.; Alonso, C.; Wissmann, C.; Kuehn, C.; Bernard, M.; et al. Comparison between B·R·A·H·M·S PCT direct, a new sensitive point-of-care testing device for rapid quantification of procalcitonin in emergency department patients and established reference methods—A prospective multinational trial. Clin. Chem. Lab. Med. 2016, 54, 577–584. [Google Scholar] [CrossRef]
- Lhopitallier, L.; Kronenberg, A.; Meuwly, J.-Y.; Locatelli, I.; Mueller, Y.; Senn, N.; D’Acremont, V.; Boillat-Blanco, N. Procalcitonin and lung ultrasonography point-of-care testing to determine antibiotic prescription in patients with lower respiratory tract infection in primary care: Pragmatic cluster randomised trial. BMJ 2021, 374, n2132. [Google Scholar] [CrossRef]
- Groeneveld, G.H.; van ’t Wout, J.W.; Aarts, N.J.; van Rooden, C.J.; Verheij, T.J.M.; Cobbaert, C.M.; Kuijper, E.J.; de Vries, J.J.C.; van Dissel, J.T. Prediction model for pneumonia in primary care patients with an acute respiratory tract infection: Role of symptoms, signs, and biomarkers. BMC Infect. Dis. 2019, 19, 976. [Google Scholar] [CrossRef]
- Siljan, W.W.; Holter, J.C.; Michelsen, A.E.; Nymo, S.H.; Lauritzen, T.; Oppen, K.; Husebye, E.; Ueland, T.; Mollnes, T.E.; Aukrust, P.; et al. Inflammatory biomarkers are associated with aetiology and predict outcomes in community-acquired pneumonia: Results of a 5-year follow-up cohort study. ERJ Open Res. 2019, 5, 00014–2019. [Google Scholar] [CrossRef]
- Hopstaken, R.M.; Muris, J.W.; Knottnerus, J.A.; Kester, A.D.; Rinkens, P.E.; Dinant, G.J. Contributions of symptoms, signs, erythrocyte sedimentation rate, and C-reactive protein to a diagnosis of pneumonia in acute lower respiratory tract infection. Br. J. Gen. Pract. 2003, 53, 358–364. [Google Scholar]
- Teepe, J.; Broekhuizen, B.D.L.; Loens, K.; Lammens, C.; Ieven, M.; Goossens, H.; Little, P.; Butler, C.C.; Coenen, S.; Godycki-Cwirko, M.; et al. Predicting the presence of bacterial pathogens in the airways of primary care patients with acute cough. CMAJ 2017, 189, E50–E55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, M.; Stuart, B.; Little, P.; Smith, S.; Thompson, M.J.; Knox, K.; van den Bruel, A.; Lown, M.; Mant, D. Predictors of pneumonia in lower respiratory tract infections: 3C prospective cough complication cohort study. Eur. Respir. J. 2017, 50, 1700434. [Google Scholar] [CrossRef] [PubMed]
- Hopstaken, R.M.; Butler, C.C.; Muris, J.W.M.; Knottnerus, J.A.; Kester, A.D.M.; Rinkens, P.E.L.M.; Dinant, G.-J. Do clinical findings in lower respiratory tract infection help general practitioners prescribe antibiotics appropriately? An observational cohort study in general practice. Fam. Pract. 2006, 23, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Russo, V.; Monetti, V.M.; Guerriero, F.; Trama, U.; Guida, A.; Menditto, E.; Orlando, V. Prevalence of antibiotic prescription in southern Italian outpatients: Real-world data analysis of socioeconomic and sociodemographic variables at a municipality level. CEOR 2018, 10, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Poss-Doering, R.; Kronsteiner, D.; Kamradt, M.; Andres, E.; Kaufmann-Kolle, P.; Wensing, M.; Szecsenyi, J.; Wensing, M.; Kamradt, M.; Poß-Doering, R.; et al. Antibiotic prescribing for acute, non-complicated infections in primary care in Germany: Baseline assessment in the cluster randomized trial ARena. BMC Infect. Dis. 2021, 21, 877. [Google Scholar] [CrossRef]
- Cadieux, G.; Tamblyn, R.; Dauphinee, D.; Libman, M. Predictors of inappropriate antibiotic prescribing among primary care physicians. CMAJ 2007, 177, 877–883. [Google Scholar] [CrossRef]
- Plate, A.; Kronenberg, A.; Risch, M.; Mueller, Y.; Di Gangi, S.; Rosemann, T.; Senn, O. Treatment of urinary tract infections in Swiss primary care: Quality and determinants of antibiotic prescribing. BMC Fam. Pract. 2020, 21, 125. [Google Scholar] [CrossRef]
- Llor, C.; Bjerrum, L.; Munck, A.; Hansen, M.P.; Córdoba, G.C.; Strandberg, E.L.; Ovhed, I.; Radzeviciene, R.; Cots, J.M.; Reutskiy, A.; et al. Predictors for antibiotic prescribing in patients with exacerbations of COPD in general practice. Ther. Adv. Respir. Dis. 2013, 7, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Teepe, J.; Broekhuizen, B.D.L.; Loens, K.; Lammens, C.; Ieven, M.; Goossens, H.; Little, P.; Butler, C.C.; Coenen, S.; Godycki-Cwirko, M.; et al. Disease Course of Lower Respiratory Tract Infection With a Bacterial Cause. Ann. Fam. Med. 2016, 14, 534–539. [Google Scholar] [CrossRef]
- Verheij, T.J.; Cianci, D.; Velden, A.W.; van der Butler, C.C.; Bongard, E.; Coenen, S.; Colliers, A.; Francis, N.A.; Little, P.; Godycki-Cwirko, M.; et al. Clinical presentation, microbiological aetiology and disease course in patients with flu-like illness: A post hoc analysis of randomised controlled trial data. Br. J. Gen. Pract. 2022, 72, e217–e224. [Google Scholar] [CrossRef]
- Petursson, P. GPs’ reasons for “non-pharmacological” prescribing of antibiotics A phenomenological study. Scand. J. Prim. Health Care 2005, 23, 120–125. [Google Scholar] [CrossRef]
- Butler, C.C.; Rollnick, S.; Pill, R.; Maggs-Rapport, F.; Stott, N. Understanding the culture of prescribing: Qualitative study of general practitioners’ and patients’ perceptions of antibiotics for sore throats. BMJ 1998, 317, 637–642. [Google Scholar] [CrossRef] [PubMed]
- Albrich, W.C.; Dusemund, F.; Bucher, B.; Meyer, S.; Thomann, R.; Kuhn, F.; Bassetti, S.; Sprenger, M.; Bachli, E.; Sigrist, T.; et al. Effectiveness and safety of procalcitonin-guided antibiotic therapy in lower respiratory tract infections in “real life”: An international, multicenter poststudy survey (ProREAL). Arch. Intern. Med. 2012, 172, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Burkhardt, O.; Ewig, S.; Haagen, U.; Giersdorf, S.; Hartmann, O.; Wegscheider, K.; Hummers-Pradier, E.; Welte, T. Procalcitonin guidance and reduction of antibiotic use in acute respiratory tract infection. Eur. Respir. J. 2010, 36, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, D.; Butler, C.C.; Bates, J.; Hood, K.; Melbye, H.; Phillips, R.; Stanton, H.; Alam, M.F.; Cals, J.W.; Cochrane, A.; et al. Associations with antibiotic prescribing for acute exacerbation of COPD in primary care: Secondary analysis of a randomised controlled trial. Br. J. Gen. Pract. 2021, 71, e266–e272. [Google Scholar] [CrossRef] [PubMed]
- Lhopitallier, L.; Kronenberg, A.; Meuwly, J.-Y.; Locatelli, I.; Dubois, J.; Marti, J.; Mueller, Y.; Senn, N.; D’Acremont, V.; Boillat-Blanco, N. Procalcitonin and lung ultrasonography point-of-care testing to decide on antibiotic prescription in patients with lower respiratory tract infection in primary care: Protocol of a pragmatic cluster randomized trial. BMC Pulm. Med. 2019, 19, 143. [Google Scholar] [CrossRef] [PubMed]
- Woodhead, M.; Blasi, F.; Ewig, S.; Garau, J.; Huchon, G.; Ieven, M.; Ortqvist, A.; Schaberg, T.; Torres, A.; van der Heijden, G.; et al. Guidelines for the management of adult lower respiratory tract infections—Full version. Clin. Microbiol. Infect. 2011, 17, E1–E59. [Google Scholar] [CrossRef]
- Marchello, C.S.; Ebell, M.H.; Dale, A.P.; Harvill, E.T.; Shen, Y.; Whalen, C.C. Signs and Symptoms That Rule out Community-Acquired Pneumonia in Outpatient Adults: A Systematic Review and Meta-Analysis. J. Am. Board Fam. Med. 2019, 32, 234–247. [Google Scholar] [CrossRef]
- Wu, S.; Crespi, C.M.; Wong, W.K. Comparison of methods for estimating the intraclass correlation coefficient for binary responses in cancer prevention cluster randomized trials. Contemp. Clin. Trials 2012, 33, 869–880. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Total Number | All Patients | No Overruling of Guidance | Overruling of Guidance | OR [95% CI] | p-Value |
|---|---|---|---|---|---|
| N = 301 | 206 (68%) | 95 (32%) | |||
| Demographics and comorbidities | |||||
| Female | 184 (61) | 129 (63) | 55 (58) | 0.84 [0.50, 1.42] | 0.52 |
| Age ≥ 65 years | 88 (29) | 58 (28) | 30 (32) | 1.31 [0.74, 2.32] | 0.35 |
| Active smoker | 62 (21) | 38 (18) | 24 (26) | 1.47 [0.79, 2.74] | 0.23 |
| Any comorbidity among the following | 84 (28) | 63 (32) | 21 (23) | 0.65 [0.35, 1.19] | 0.16 |
| Diabetes | 16 (5) | 11 (5) | 5 (5) | 0.99 [0.31, 3.14] | 0.99 |
| Chronic obstructive pulmonary disease | 17 (6) | 12 (6) | 5 (5) | 0.96 [0.30, 3.00] | 0.94 |
| Asthma | 52 (17) | 41 (20) | 11 (12) | 0.52 [0.25, 1.12] | 0.09 |
| Heart failure | 4 (1) | 4 (2) | 0 (0) | - | - |
| Other * | 4 (1) | 4 (2) | 0 (0) | - | - |
| Clinical presentation | |||||
| History of fever | 194 (65) | 128 (62) | 66 (70) | 1.37 [0.78, 2.40] | 0.27 |
| History of dyspnea | 205 (69) | 144 (70) | 61 (66) | 0.84 [0.47, 1.48] | 0.54 |
| History of chest pain | 140 (47) | 87 (43) | 53 (56) | 1.74 [1.03, 2.93] | 0.04 |
| History of sputum production | 209 (70) | 143 (70) | 66 (70) | 1.06 [0.60, 1.87] | 0.85 |
| Heart rate ≥ 100/min | 47 (16) | 30 (15) | 17 (18) | 1.29 [0.64, 2.58] | 0.48 |
| Respiratory rate > 22/min | 49 (16) | 36 (18) | 13 (14) | 0.87 [0.40, 1.87] | 0.72 |
| Systolic blood pressure ≤ 100 mmHg | 15 (5) | 7 (3) | 8 (9) | 2.21 [0.70, 6.99] | 0.18 |
| Temperature ≥ 37.8 °C | 44 (15) | 25 (12) | 19 (20) | 2.16 [1.04, 4.48] | 0.04 |
| Focal abnormal finding upon lung auscultation | 137 (46) | 86 (42) | 51 (54) | 1.83 [1.06, 3.16] | 0.03 |
| Management | |||||
| Prescription of chest X-ray by GP | 56 (19) | 26 (13) | 30 (32) | 3.79 [1.85, 7.76] | <0.001 |
| Biomarkers | |||||
| CRP measured by GP | 97 (33) | 51 (25) | 46 (49) | 2.77 [1.58, 4.86] | <0.001 |
| CRP value (measured retrospectively) | |||||
| ≤20 mg/L | 159 (58) | 116 (62) | 43 (48) | ref | ref |
| 20.01–100 mg/L | 99 (36) | 64 (34) | 35 (39) | 1.66 [0.92, 2.99] | 0.09 |
| >100 mg/L | 18 (7) | 7 (4) | 11 (12) | 4.59 [1.52, 13.90] | 0.007 |
| Microbiology | |||||
| Viral infection | 117 (41) | 79 (40) | 38 (43) | ref | ref |
| Bacterial or mixed infection | 112 (39) | 75 (38) | 37 (42) | 1.19 [0.65, 2.19] | 0.58 |
| No pathogen identified | 56 (20) | 42 (21) | 14 (16) | 0.75 [0.35, 1.60] | 0.45 |
| General practitioner’s characteristics | |||||
| Francophone | 274 (91) | 190 (92) | 84 (88) | 0.66 [0.22, 1.96] | 0.45 |
| >5 general practitioners in practice | 89 (30) | 57 (28) | 32 (34) | 1.37 [0.64, 2.94] | 0.42 |
| Location of practice in an urban setting | 187 (62) | 121 (59) | 66 (70) | 1.47 [0.72, 3.01] | 0.29 |
| Years of experience in practice (median [IQR]) | 9.0 [5.0, 19] | 8.0 [5.0, 19] | 10 [5.0, 19] | 1.02 [0.98, 1.07] | 0.35 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knüsli, J.; Lhopitallier, L.; Kronenberg, A.; Meuwly, J.-Y.; Opota, O.; Perrenoud, M.-A.; Page, M.-A.; Kain, K.C.; Mamin, A.; D’Acremont, V.; et al. Overruling of Procalcitonin-Guided Antibiotics for Lower Respiratory Tract Infections in Primary Care: Ancillary Study of a Randomized Controlled Trial. Antibiotics 2023, 12, 377. https://doi.org/10.3390/antibiotics12020377
Knüsli J, Lhopitallier L, Kronenberg A, Meuwly J-Y, Opota O, Perrenoud M-A, Page M-A, Kain KC, Mamin A, D’Acremont V, et al. Overruling of Procalcitonin-Guided Antibiotics for Lower Respiratory Tract Infections in Primary Care: Ancillary Study of a Randomized Controlled Trial. Antibiotics. 2023; 12(2):377. https://doi.org/10.3390/antibiotics12020377
Chicago/Turabian StyleKnüsli, José, Loïc Lhopitallier, Andreas Kronenberg, Jean-Yves Meuwly, Onya Opota, Marc-Antoine Perrenoud, Marie-Anne Page, Kevin C. Kain, Aline Mamin, Valérie D’Acremont, and et al. 2023. "Overruling of Procalcitonin-Guided Antibiotics for Lower Respiratory Tract Infections in Primary Care: Ancillary Study of a Randomized Controlled Trial" Antibiotics 12, no. 2: 377. https://doi.org/10.3390/antibiotics12020377