

Intravenous Polymyxin B as Adjunctive Therapy to High-Dose Tigecycline for the Treatment of Nosocomial Pneumonia Due to Carbapenem-Resistant Acinetobacter baumannii and Klebsiella pneumoniae: A Propensity Score-Matched Cohort Study
 ,
,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Definition and Diagnosis of Pneumonia
2.3. Microbiological Tests
2.4. Participants and Antimicrobial Therapy
2.5. Clinical Outcomes and Definitions
2.6. Data Extraction
2.7. Statistical Analysis
3. Results
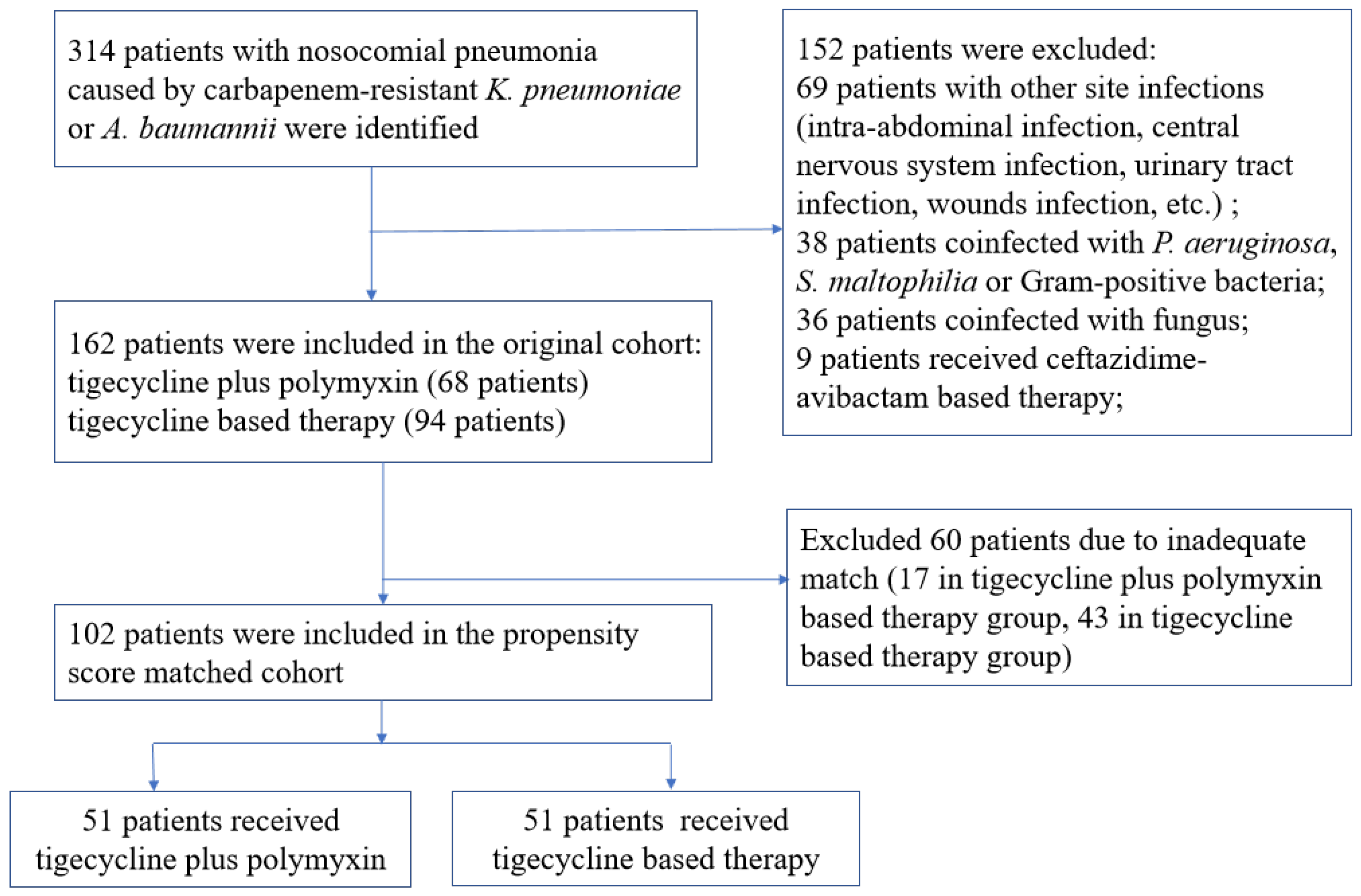
3.1. Study Cohort
3.2. Characteristics of Patients in the Matched Cohort
3.3. Clinical Outcomes
3.4. Subgroup Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Healthcare-Associated Infections in Intensive Care Units—Annual Epidemiological Report for 2016; ECDC: Stockholm, Sweden, 2018. [Google Scholar]
- Cassini, A.; Högberg, L.D.; Plachouras, D.; Quattrocchi, A.; Hoxha, A.; Simonsen, G.S.; Colomb-Cotinat, M.; Kretzschmar, M.E.; Devleesschauwer, B.; Cecchini, M.; et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. Lancet Infect. Dis. 2019, 19, 56–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.Y.; Yang, K.Y.; Peng, C.K.; Sheu, C.C.; Chan, M.C.; Feng, J.Y.; Wang, S.H.; Chen, C.M.; Zheng, Z.R.; Liang, S.J.; et al. Clinical outcome of nosocomial pneumonia caused by Carbapenem-resistant gram-negative bacteria in critically ill patients: A multicenter retrospective observational study. Sci. Rep. 2022, 12, 7501. [Google Scholar] [CrossRef]
- Hauck, C.; Cober, E.; Richter, S.S.; Perez, F.; Salata, R.A.; Kalayjian, R.C.; Watkins, R.R.; Scalera, N.M.; Doi, Y.; Kaye, K.S.; et al. Spectrum of excess mortality due to carbapenem-resistant Klebsiella pneumoniae infections. Clin. Microbiol. Infect. 2016, 22, 513–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zilberberg, M.D.; Nathanson, B.H.; Sulham, K.; Fan, W.; Shorr, A.F. A Novel Algorithm to Analyze Epidemiology and Outcomes of Carbapenem Resistance Among Patients With Hospital-Acquired and Ventilator-Associated Pneumonia: A Retrospective Cohort Study. Chest 2019, 155, 1119–1130. [Google Scholar] [CrossRef] [PubMed]
- Zha, L.; Li, S.; Ren, Z.; Li, X.; Zhang, D.; Zou, Y.; Pan, L.; Xu, Q.; Rui, Z.; Chen, S.; et al. Clinical management of infections caused by carbapenem-resistant Klebsiella pneumoniae in critically ill patients: A nationwide survey of tertiary hospitals in mainland China. J. Infect. 2022, 84, e108–e110. [Google Scholar] [CrossRef]
- Doi, Y. Treatment Options for Carbapenem-resistant Gram-negative Bacterial Infections. Clin. Infect. Dis. 2019, 69, S565–S575. [Google Scholar] [CrossRef] [Green Version]
- El-Sayed Ahmed, M.A.E.; Zhong, L.L.; Shen, C.; Yang, Y.; Doi, Y.; Tian, G.B. Colistin and its role in the Era of antibiotic resistance: An extended review (2000-2019). Emerg. Microbes Infect. 2020, 9, 868–885. [Google Scholar] [CrossRef] [Green Version]
- Paul, M.; Carrara, E.; Retamar, P.; Tängdén, T.; Bitterman, R.; Bonomo, R.A.; de Waele, J.; Daikos, G.L.; Akova, M.; Harbarth, S.; et al. European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines for the treatment of infections caused by multidrug-resistant Gram-negative bacilli (endorsed by European society of intensive care medicine). Clin. Microbiol. Infect. 2022, 28, 521–547. [Google Scholar] [CrossRef]
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America Guidance on the Treatment of AmpC β-lactamase-Producing Enterobacterales, Carbapenem-Resistant Acinetobacter baumannii, and Stenotrophomonas maltophilia Infections. Clin. Infect. Dis. 2021, 74, 2089–2114. [Google Scholar] [CrossRef]
- van Duin, D.; Lok, J.J.; Earley, M.; Cober, E.; Richter, S.S.; Perez, F.; Salata, R.A.; Kalayjian, R.C.; Watkins, R.R.; Doi, Y.; et al. Colistin Versus Ceftazidime-Avibactam in the Treatment of Infections Due to Carbapenem-Resistant Enterobacteriaceae. Clin. Infect. Dis. 2018, 66, 163–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, C.A.; Lin, Y.C.; Lu, P.L.; Chen, H.C.; Chang, H.L.; Sheu, C.C. Antibiotic strategies and clinical outcomes in critically ill patients with pneumonia caused by carbapenem-resistant Acinetobacter baumannii. Clin. Microbiol. Infect. 2018, 24, e901–e908. [Google Scholar] [CrossRef] [Green Version]
- Lou, T.; Du, X.; Zhang, P.; Shi, Q.; Han, X.; Lan, P.; Yan, R.; Hu, H.; Wang, Y.; Wu, X.; et al. Risk factors for infection and mortality caused by carbapenem-resistant Klebsiella pneumoniae: A large multicentre case-control and cohort study. J. Infect. 2022, 84, 637–647. [Google Scholar] [CrossRef] [PubMed]
- Barth, N.; Ribeiro, V.B.; Zavascki, A.P. In vitro activity of polymyxin B plus imipenem, meropenem, or tigecycline against KPC-2-producing Enterobacteriaceae with high MICs for these antimicrobials. Antimicrob. Agents Chemother. 2015, 59, 3596–3597. [Google Scholar] [CrossRef] [Green Version]
- Cai, Y.; Lim, T.P.; Teo, J.; Sasikala, S.; Lee, W.; Hong, Y.; Chan, E.C.; Tan, T.Y.; Tan, T.T.; Koh, T.H.; et al. In Vitro Activity of Polymyxin B in Combination with Various Antibiotics against Extensively Drug-Resistant Enterobacter cloacae with Decreased Susceptibility to Polymyxin B. Antimicrob. Agents Chemother. 2016, 60, 5238–5246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papst, L.; Beović, B.; Pulcini, C.; Durante-Mangoni, E.; Rodríguez-Baño, J.; Kaye, K.S.; Daikos, G.L.; Raka, L.; Paul, M. Antibiotic treatment of infections caused by carbapenem-resistant Gram-negative bacilli: An international ESCMID cross-sectional survey among infectious diseases specialists practicing in large hospitals. Clin. Microbiol. Infect. 2018, 24, 1070–1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amat, T.; Gutiérrez-Pizarraya, A.; Machuca, I.; Gracia-Ahufinger, I.; Pérez-Nadales, E.; Torre-Giménez, Á.; Garnacho-Montero, J.; Cisneros, J.M.; Torre-Cisneros, J. The combined use of tigecycline with high-dose colistin might not be associated with higher survival in critically ill patients with bacteraemia due to carbapenem-resistant Acinetobacter baumannii. Clin. Microbiol. Infect. 2018, 24, 630–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, A.; Chuang, Y.C.; Sun, H.Y.; Sheng, W.H.; Yang, C.J.; Liao, C.H.; Hsueh, P.R.; Yang, J.L.; Shen, N.J.; Wang, J.T.; et al. Excess Mortality Associated With Colistin-Tigecycline Compared With Colistin-Carbapenem Combination Therapy for Extensively Drug-Resistant Acinetobacter baumannii Bacteremia: A Multicenter Prospective Observational Study. Crit. Care Med. 2015, 43, 1194–1204. [Google Scholar] [CrossRef]
- Chusri, S.; Singkhamanan, K.; Wanitsuwan, W.; Suphasynth, Y.; Kositpantawong, N.; Panthuwong, S.; Doi, Y. Adjunctive therapy of intravenous colistin to intravenous tigecycline for adult patients with non-bacteremic post-surgical intra-abdominal infection due to carbapenem-resistant Acinetobacter baumannii. J. Infect. Chemother. 2019, 25, 681–686. [Google Scholar] [CrossRef]
- Barbour, A.; Schmidt, S.; Ma, B.; Schiefelbein, L.; Rand, K.H.; Burkhardt, O.; Derendorf, H. Clinical pharmacokinetics and pharmacodynamics of tigecycline. Clin. Pharmacokinet. 2009, 48, 575–584. [Google Scholar] [CrossRef]
- Conte, J.E., Jr.; Golden, J.A.; Kelly, M.G.; Zurlinden, E. Steady-state serum and intrapulmonary pharmacokinetics and pharmacodynamics of tigecycline. Int. J. Antimicrob. Agents 2005, 25, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Leng, B.; Yan, G.; Wang, C.; Shen, C.; Zhang, W.; Wang, W. Dose optimisation based on pharmacokinetic/pharmacodynamic target of tigecycline. J. Glob. Antimicrob. Resist. 2021, 25, 315–322. [Google Scholar] [CrossRef]
- Sato, Y.; Ubagai, T.; Tansho-Nagakawa, S.; Yoshino, Y.; Ono, Y. Effects of colistin and tigecycline on multidrug-resistant Acinetobacter baumannii biofilms: Advantages and disadvantages of their combination. Sci. Rep. 2021, 11, 11700. [Google Scholar] [CrossRef] [PubMed]
- Ni, W.; Li, G.; Zhao, J.; Cui, J.; Wang, R.; Gao, Z.; Liu, Y. Use of Monte Carlo simulation to evaluate the efficacy of tigecycline and minocycline for the treatment of pneumonia due to carbapenemase-producing Klebsiella pneumoniae. Infect. Dis. 2018, 50, 507–513. [Google Scholar] [CrossRef] [PubMed]
- De Pascale, G.; Montini, L.; Pennisi, M.; Bernini, V.; Maviglia, R.; Bello, G.; Spanu, T.; Tumbarello, M.; Antonelli, M. High dose tigecycline in critically ill patients with severe infections due to multidrug-resistant bacteria. Crit. Care 2014, 18, R90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zha, L.; Pan, L.; Guo, J.; French, N.; Villanueva, E.V.; Tefsen, B. Effectiveness and Safety of High Dose Tigecycline for the Treatment of Severe Infections: A Systematic Review and Meta-Analysis. Adv. Ther. 2020, 37, 1049–1064. [Google Scholar] [CrossRef] [PubMed]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spalding, M.C.; Cripps, M.W.; Minshall, C.T. Ventilator-Associated Pneumonia: New Definitions. Crit. Care Clin. 2017, 33, 277–292. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.W.; Chen, Y.H.; Lee, W.S.; Lin, J.C.; Huang, C.T.; Lin, H.H.; Liu, Y.C.; Chuang, Y.C.; Tang, H.J.; Chen, Y.S.; et al. Randomized Noninferiority Trial of Cefoperazone-Sulbactam versus Cefepime in the Treatment of Hospital-Acquired and Healthcare-Associated Pneumonia. Antimicrob. Agents Chemother. 2019, 63, e00023-19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Society, J.R. Diagnosis of hospital-acquired pneumonia and methods of testing for pathogens. Respirology 2009, 14 (Suppl. 2), S10–S22. [Google Scholar] [CrossRef]
- EUCAST. Breakpoint Tables for Interpretation of MICs and Zone Diameters, Version 12.0; EUCAST: Växjö, Sweden, 2022. [Google Scholar]
- Guo, W.; Guo, S.C.; Li, M.; Li, L.H.; Qu, Y. Successful treatment of extensively drug-resistant Acinetobacter baumannii ventriculitis with polymyxin B and tigecycline- a case report. Antimicrob. Resist. Infect. Control 2018, 7, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; An, Y.; Li, L.; Yi, H. Intrathecal Injection of Tigecycline and Polymyxin B in the Treatment of Extensively Drug-Resistant Intracranial Acinetobacter baumannii Infection: A Case Report and Review of the Literature. Infect. Drug Resist. 2022, 15, 1411–1423. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.; Wang, H.; Zhao, J.; Yang, X.; Wu, B.; Sun, W.; Huang, M.; Cheng, Z.; Chen, H.; Song, Y.; et al. Polymyxin B/Tigecycline Combination vs. Polymyxin B or Tigecycline Alone for the Treatment of Hospital-Acquired Pneumonia Caused by Carbapenem-Resistant Enterobacteriaceae or Carbapenem-Resistant Acinetobacter baumannii. Front. Med. 2022, 9, 772372. [Google Scholar] [CrossRef] [PubMed]
- Paul, M.; Daikos, G.L.; Durante-Mangoni, E.; Yahav, D.; Carmeli, Y.; Benattar, Y.D.; Skiada, A.; Andini, R.; Eliakim-Raz, N.; Nutman, A.; et al. Colistin alone versus colistin plus meropenem for treatment of severe infections caused by carbapenem-resistant Gram-negative bacteria: An open-label, randomised controlled trial. Lancet Infect. Dis. 2018, 18, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Durante-Mangoni, E.; Signoriello, G.; Andini, R.; Mattei, A.; De Cristoforo, M.; Murino, P.; Bassetti, M.; Malacarne, P.; Petrosillo, N.; Galdieri, N.; et al. Colistin and rifampicin compared with colistin alone for the treatment of serious infections due to extensively drug-resistant Acinetobacter baumannii: A multicenter, randomized clinical trial. Clin. Infect. Dis. 2013, 57, 349–358. [Google Scholar] [CrossRef] [Green Version]
- Nutman, A.; Lellouche, J.; Temkin, E.; Daikos, G.; Skiada, A.; Durante-Mangoni, E.; Dishon-Benattar, Y.; Bitterman, R.; Yahav, D.; Daitch, V.; et al. Colistin plus meropenem for carbapenem-resistant Gram-negative infections: In vitro synergism is not associated with better clinical outcomes. Clin. Microbiol. Infect. 2020, 26, 1185–1191. [Google Scholar] [CrossRef]
- Katip, W.; Oberdorfer, P. Clinical Efficacy and Nephrotoxicity of Colistin Alone versus Colistin Plus Vancomycin in Critically Ill Patients Infected with Carbapenem-Resistant Acinetobacter baumannii: A Propensity Score-Matched Analysis. Pharmaceutics 2021, 13, 162. [Google Scholar] [CrossRef]
- Tsuji, B.T.; Pogue, J.M.; Zavascki, A.P.; Paul, M.; Daikos, G.L.; Forrest, A.; Giacobbe, D.R.; Viscoli, C.; Giamarellou, H.; Karaiskos, I.; et al. International Consensus Guidelines for the Optimal Use of the Polymyxins: Endorsed by the American College of Clinical Pharmacy (ACCP), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), Infectious Diseases Society of America (IDSA), International Society for Anti-infective Pharmacology (ISAP), Society of Critical Care Medicine (SCCM), and Society of Infectious Diseases Pharmacists (SIDP). Pharmacotherapy 2019, 39, 10–39. [Google Scholar] [CrossRef] [Green Version]
- Scheetz, M.H.; Qi, C.; Warren, J.R.; Postelnick, M.J.; Zembower, T.; Obias, A.; Noskin, G.A. In vitro activities of various antimicrobials alone and in combination with tigecycline against carbapenem-intermediate or -resistant Acinetobacter baumannii. Antimicrob. Agents Chemother. 2007, 51, 1621–1626. [Google Scholar] [CrossRef] [Green Version]
- Petersen, P.J.; Labthavikul, P.; Jones, C.H.; Bradford, P.A. In vitro antibacterial activities of tigecycline in combination with other antimicrobial agents determined by chequerboard and time-kill kinetic analysis. J. Antimicrob. Chemother. 2006, 57, 573–576. [Google Scholar] [CrossRef]
- Urban, C.; Mariano, N.; Rahal, J.J. In vitro double and triple bactericidal activities of doripenem, polymyxin B, and rifampin against multidrug-resistant Acinetobacter baumannii, Pseudomonas aeruginosa, Klebsiella pneumoniae, and Escherichia coli. Antimicrob. Agents Chemother. 2010, 54, 2732–2734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landersdorfer, C.B.; Wang, J.; Wirth, V.; Chen, K.; Kaye, K.S.; Tsuji, B.T.; Li, J.; Nation, R.L. Pharmacokinetics/pharmacodynamics of systemically administered polymyxin B against Klebsiella pneumoniae in mouse thigh and lung infection models. J. Antimicrob. Chemother. 2018, 73, 462–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hagihara, M.; Housman, S.T.; Nicolau, D.P.; Kuti, J.L. In vitro pharmacodynamics of polymyxin B and tigecycline alone and in combination against carbapenem-resistant Acinetobacter baumannii. Antimicrob. Agents Chemother. 2014, 58, 874–879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michail, G.; Labrou, M.; Pitiriga, V.; Manousaka, S.; Sakellaridis, N.; Tsakris, A.; Pournaras, S. Activity of Tigecycline in combination with Colistin, Meropenem, Rifampin, or Gentamicin against KPC-producing Enterobacteriaceae in a murine thigh infection model. Antimicrob. Agents Chemother. 2013, 57, 6028–6033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, B.; Guan, J.; Wang, X.; Cong, Y. Activity of Colistin in Combination with Meropenem, Tigecycline, Fosfomycin, Fusidic Acid, Rifampin or Sulbactam against Extensively Drug-Resistant Acinetobacter baumannii in a Murine Thigh-Infection Model. PLoS ONE 2016, 11, e0157757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Pascale, G.; Lisi, L.; Ciotti, G.M.P.; Vallecoccia, M.S.; Cutuli, S.L.; Cascarano, L.; Gelormini, C.; Bello, G.; Montini, L.; Carelli, S.; et al. Pharmacokinetics of high-dose tigecycline in critically ill patients with severe infections. Ann. Intensive Care 2020, 10, 94. [Google Scholar] [CrossRef] [PubMed]
- Tuon, F.F.; Graf, M.E.; Merlini, A.; Rocha, J.L.; Stallbaum, S.; Arend, L.N.; Pecoit-Filho, R. Risk factors for mortality in patients with ventilator-associated pneumonia caused by carbapenem-resistant Enterobacteriaceae. Braz. J. Infect. Dis. 2017, 21, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Cheah, S.E.; Wang, J.; Nguyen, V.T.; Turnidge, J.D.; Li, J.; Nation, R.L. New pharmacokinetic/pharmacodynamic studies of systemically administered colistin against Pseudomonas aeruginosa and Acinetobacter baumannii in mouse thigh and lung infection models: Smaller response in lung infection. J. Antimicrob. Chemother. 2015, 70, 3291–3297. [Google Scholar] [CrossRef] [Green Version]
- Katip, W.; Uitrakul, S.; Oberdorfer, P. Clinical Efficacy and Nephrotoxicity of the Loading Dose Colistin for the Treatment of Carbapenem-Resistant Acinetobacter baumannii in Critically Ill Patients. Pharmaceutics 2021, 14, 31. [Google Scholar] [CrossRef]
- Wertheim, H.; Van Nguyen, K.; Hara, G.L.; Gelband, H.; Laxminarayan, R.; Mouton, J.; Cars, O. Global survey of polymyxin use: A call for international guidelines. J. Glob. Antimicrob. Resist. 2013, 1, 131–134. [Google Scholar] [CrossRef]
- Athanassa, Z.E.; Markantonis, S.L.; Fousteri, M.Z.; Myrianthefs, P.M.; Boutzouka, E.G.; Tsakris, A.; Baltopoulos, G.J. Pharmacokinetics of inhaled colistimethate sodium (CMS) in mechanically ventilated critically ill patients. Intensive Care Med. 2012, 38, 1779–1786. [Google Scholar] [CrossRef] [PubMed]
- Boisson, M.; Jacobs, M.; Grégoire, N.; Gobin, P.; Marchand, S.; Couet, W.; Mimoz, O. Comparison of intrapulmonary and systemic pharmacokinetics of colistin methanesulfonate (CMS) and colistin after aerosol delivery and intravenous administration of CMS in critically ill patients. Antimicrob. Agents Chemother. 2014, 58, 7331–7339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, D.; Zhang, J.; Liu, H.X.; Zhu, Y.G.; Qu, J.M. Intravenous combined with aerosolised polymyxin versus intravenous polymyxin alone in the treatment of pneumonia caused by multidrug-resistant pathogens: A systematic review and meta-analysis. Int. J. Antimicrob. Agents 2015, 46, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Valachis, A.; Samonis, G.; Kofteridis, D.P. The role of aerosolized colistin in the treatment of ventilator-associated pneumonia: A systematic review and metaanalysis. Crit. Care Med. 2015, 43, 527–533. [Google Scholar] [CrossRef]
- Feng, J.Y.; Peng, C.K.; Sheu, C.C.; Lin, Y.C.; Chan, M.C.; Wang, S.H.; Chen, C.M.; Shen, Y.C.; Zheng, Z.R.; Lin, Y.T.; et al. Efficacy of adjunctive nebulized colistin in critically ill patients with nosocomial carbapenem-resistant Gram-negative bacterial pneumonia: A multi-centre observational study. Clin. Microbiol. Infect. 2021, 27, 1465–1473. [Google Scholar] [CrossRef]
- Rattanaumpawan, P.; Lorsutthitham, J.; Ungprasert, P.; Angkasekwinai, N.; Thamlikitkul, V. Randomized controlled trial of nebulized colistimethate sodium as adjunctive therapy of ventilator-associated pneumonia caused by Gram-negative bacteria. J. Antimicrob. Chemother. 2010, 65, 2645–2649. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, A.; Azim, A.; Gurjar, M.; Baronia, A.K. Current concepts in combination antibiotic therapy for critically ill patients. Indian J. Crit. Care Med. 2014, 18, 310–314. [Google Scholar] [CrossRef] [Green Version]
- Anthony, K.B.; Fishman, N.O.; Linkin, D.R.; Gasink, L.B.; Edelstein, P.H.; Lautenbach, E. Clinical and microbiological outcomes of serious infections with multidrug-resistant gram-negative organisms treated with tigecycline. Clin. Infect. Dis. 2008, 46, 567–570. [Google Scholar] [CrossRef] [Green Version]
- Du, X.; He, F.; Shi, Q.; Zhao, F.; Xu, J.; Fu, Y.; Yu, Y. The Rapid Emergence of Tigecycline Resistance in bla(KPC-2) Harboring Klebsiella pneumoniae, as Mediated in Vivo by Mutation in tetA During Tigecycline Treatment. Front. Microbiol. 2018, 9, 648. [Google Scholar] [CrossRef] [Green Version]
- Cheong, H.S.; Kim, S.Y.; Wi, Y.M.; Peck, K.R.; Ko, K.S. Colistin Heteroresistance in Klebsiella Pneumoniae Isolates and Diverse Mutations of PmrAB and PhoPQ in Resistant Subpopulations. J. Clin. Med. 2019, 8, 1444. [Google Scholar] [CrossRef]
- Zheng, J.X.; Lin, Z.W.; Sun, X.; Lin, W.H.; Chen, Z.; Wu, Y.; Qi, G.B.; Deng, Q.W.; Qu, D.; Yu, Z.J. Overexpression of OqxAB and MacAB efflux pumps contributes to eravacycline resistance and heteroresistance in clinical isolates of Klebsiella pneumoniae. Emerg. Microbes Infect. 2018, 7, 139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiu, S.K.; Chan, M.C.; Huang, L.Y.; Lin, Y.T.; Lin, J.C.; Lu, P.L.; Siu, L.K.; Chang, F.Y.; Yeh, K.M. Tigecycline resistance among carbapenem-resistant Klebsiella Pneumoniae: Clinical characteristics and expression levels of efflux pump genes. PLoS ONE 2017, 12, e0175140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, X.; Yang, Z.; Dai, J.; Chen, K.; Zhang, L.; Ni, W.; Wei, C.; Cui, J. Pharmacodynamics of tigecycline alone and in combination with colistin against clinical isolates of multidrug-resistant Acinetobacter baumannii in an in vitro pharmacodynamic model. Int. J. Antimicrob. Agents 2017, 49, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Ni, W.; Cui, J.; Liang, B.; Cai, Y.; Bai, N.; Cai, X.; Wang, R. In vitro effects of tigecycline in combination with colistin (polymyxin E) and sulbactam against multidrug-resistant Acinetobacter baumannii. J. Antibiot. 2013, 66, 705–708. [Google Scholar] [CrossRef] [Green Version]
- Jin, X.; Chen, Q.; Shen, F.; Jiang, Y.; Wu, X.; Hua, X.; Fu, Y.; Yu, Y. Resistance evolution of hypervirulent carbapenem-resistant Klebsiella pneumoniae ST11 during treatment with tigecycline and polymyxin. Emerg. Microbes Infect. 2021, 10, 1129–1136. [Google Scholar] [CrossRef]
- Shields, R.K.; Clancy, C.J.; Gillis, L.M.; Kwak, E.J.; Silveira, F.P.; Massih, R.C.; Eschenauer, G.A.; Potoski, B.A.; Nguyen, M.H. Epidemiology, clinical characteristics and outcomes of extensively drug-resistant Acinetobacter baumannii infections among solid organ transplant recipients. PLoS ONE 2012, 7, e52349. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Original Cohort | Propensity Score-Matched Cohort | |||||
|---|---|---|---|---|---|---|---|
| Tigecycline- Polymyxin B, n = 68, 42% | Tigecycline, n = 94, 58% | p | Tigecycline- Polymyxin B, n = 51, 50% | Tigecycline, n = 51, 50% | p | Standardized Differences | |
| Age, years, median [IQR] | 63 [52, 74.25] | 63 [51, 75.75] | 0.764 | 67 [54, 76.5] | 56 [49, 75.5] | 0.235 | 0.238 |
| Male Gender, n (%) | 48 (70.6) | 64 (68.1) | 0.867 | 36 (70.6) | 35 (68.6) | 1.000 | 0.043 |
| Preexisting Medical Conditions, n (%) | |||||||
| Hypertension | 26 (38.2) | 44 (46.8) | 0.354 | 20 (39.2) | 21 (41.2) | 1.000 | 0.04 |
| Diabetes Mellitus | 16 (23.5) | 24 (25.5) | 0.915 | 14 (27.5) | 11 (21.6) | 0.645 | 0.137 |
| Chronic Heart Disease | 16 (23.5) | 14 (14.9) | 0.233 | 13 (25.5) | 7 (13.7) | 0.212 | 0.3 |
| Chronic Kidney Disease | 4 (5.9) | 3 (3.2) | 0.660 | 3 (5.9) | 3 (5.9) | 1.000 | <0.001 |
| Chronic Liver Disease | 5 (7.4) | 8 (8.5) | 1.000 | 2 (3.9) | 6 (11.8) | 0.269 | 0.295 |
| Malignancy | 10 (14.7) | 17 (18.1) | 0.722 | 8 (15.7) | 11 (21.6) | 0.611 | 0.152 |
| History of Surgery | 29 (42.6) | 38 (40.4) | 0.903 | 20 (39.2) | 20 (39.2) | 1.000 | <0.001 |
| Charlson Comorbidity Index, median [IQR] | 3 [1, 4] | 3 [1, 5] | 0.506 | 4 [2, 6] | 4 [2, 6] | 0.935 | 0.027 |
| Type of Pneumonia, n (%) | 0.730 | 0.222 | 0.285 | ||||
| Hospital-acquired Pneumonia | 28 (41.2) | 35 (37.2) | 23 (45.1) | 16 (31.4) | |||
| Ventilator-associated Pneumonia | 40 (58.8) | 59 (62.8) | 28 (54.9) | 35 (68.6) | |||
| Pathogen, n (%) | 0.26 | 0.828 | 0.086 | ||||
| A. baumannii | 45 (66.2) | 71 (75.5) | 35 (68.6) | 37 (72.5) | |||
| K. pneumonia | 23 (33.8) | 23 (24.5) | 16 (31.4) | 14 (27.5) | |||
| Polymicrobial Pneumonia, n (%) | 7 (10.3) | 14 (14.9) | 0.533 | 5 (9.8) | 5 (9.8) | 1.000 | <0.001 |
| Concomitant Antibiotics, n (%) | 0.23 | 0.253 | 0.651 | ||||
| Aminoglycoside | 0 (0.0) | 2 (2.4) | 0 (0.0) | 2 (4.3) | |||
| Fluoroquinolone | 1 (1.8) | 2 (2.4) | 0 (0.0) | 0 (0.0) | |||
| Carbapenems | 27 (48.2) | 21 (25.6) | 21 (53.8) | 15 (32.6) | |||
| Piperacillin-Tazobactam | 0 (0.0) | 4 (4.9) | 0 (0.0) | 2 (4.3) | |||
| Cefoperazone-Sulbactam | 24 (42.9) | 50 (61.0) | 16 (41.0) | 25 (54.3) | |||
| Carbapenem plus Sulbactam | 4 (7.1) | 2 (2.4) | 2 (5.1) | 2 (4.4) | |||
| Carbapenem plus Moxifloxacin | 0 (0.0) | 1 (1.2) | 0 (0.0) | 0 (0.0) | |||
| Inappropriate Initial Antibiotic Therapy | 33 (48.5) | 58 (61.7) | 0.132 | 26 (51.0) | 28 (54.9) | 0.843 | 0.079 |
| Duration of antibiotic therapy, days, median [IQR] | 16 [10, 25] | 14 [10, 21] | 0.378 | 16 [10, 25] | 15 [10, 25.5] | 0.730 | 0.011 |
| Septic Shock, n (%) | 60 (88.2) | 70 (74.5) | 0.049 | 46 (90.2) | 43 (84.3) | 0.553 | 0.177 |
| Duration of Vasopressors, days, median [IQR] | 12 [7, 21.25] | 8 [4, 15] | 0.03 | 12.5 [8, 21.75] | 9 [5, 15] | 0.063 | 0.286 |
| SOFA score, median [IQR] | 10 [7, 12] | 8 [5, 11] | 0.018 | 10 [7.5, 12] | 9 [7.5, 12.5] | 0.944 | 0.043 |
| Clinical Outcomes | Patients Included in Analysis, No./Total No. (%) | ||
|---|---|---|---|
| Tigecycline- Polymyxin B | Tigecycline | Odds Ratio a (95% CI), p Tigecycline as Reference | |
| Overall analysis | |||
| 14-day mortality | 14/68 (20.6%) | 23/94 (24.5%) | 0.73 (0.32–1.62), 0.449 |
| Clinical cure | 39/68 (57.4%) | 57/94 (60.6%) | 0.95 (0.47–1.92), 0.895 |
| Microbiological cure | 19/68 (28.4%) | 32/94 (34.0%) | 0.84 (0.39–1.72), 0.627 |
| Nephrotoxicity rate | 31/68 (45.6%) | 37/94 (39.4%) | 0.91 (0.44–1.85), 0.792 |
| Matched cohort | |||
| 14-day mortality | 11/51 (21.6%) | 14/51 (27.5%) | 0.72 (0.27–1.83), 0.486 |
| Clinical cure | 28/51 (54.9%) | 27/51 (52.9%) | 1.09 (0.48–2.54), 0.823 |
| Microbiological cure | 13/51 (25.5%) | 15/51 (29.4%) | 0.96 (0.39–2.35), 0.928 |
| Nephrotoxicity rate | 24/51 (47.1%) | 26/51 (51.0%) | 0.85 (0.36–1.99), 0.712 |
| Subgroup Analysis a | OR (95% CI) | p |
|---|---|---|
| Age | ||
| ≤65 | 1.22 (0.21–7.21) | 0.812 |
| >65 | 0.40 (0.12–1.31) | 0.137 |
| Pneumonia type | ||
| HAP | 1.15 (0.31–4.47) | 0.832 |
| VAP | 0.25 (0.04–1.11) | 0.09 |
| Pathogen | ||
| A. baumannii | 0.43 (0.13–1.28) | 0.139 |
| K. pneumoniae | 2.72 (0.48–21.9) | 0.283 |
| Initial empirical antibiotic therapy | ||
| Appropriate | 0.39 (0.07–1.69) | 0.221 |
| Inappropriate | 1.11 (0.34–3.62) | 0.859 |
| Excluded polymicrobial pneumonia | 0.56 (0.21–1.44) | 0.231 |
| Excluded patients without septic shock | 0.65 (0.25–1.65) | 0.366 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zha, L.; Zhang, X.; Cheng, Y.; Xu, Q.; Liu, L.; Chen, S.; Lu, Z.; Guo, J.; Tefsen, B. Intravenous Polymyxin B as Adjunctive Therapy to High-Dose Tigecycline for the Treatment of Nosocomial Pneumonia Due to Carbapenem-Resistant Acinetobacter baumannii and Klebsiella pneumoniae: A Propensity Score-Matched Cohort Study. Antibiotics 2023, 12, 273. https://doi.org/10.3390/antibiotics12020273
Zha L, Zhang X, Cheng Y, Xu Q, Liu L, Chen S, Lu Z, Guo J, Tefsen B. Intravenous Polymyxin B as Adjunctive Therapy to High-Dose Tigecycline for the Treatment of Nosocomial Pneumonia Due to Carbapenem-Resistant Acinetobacter baumannii and Klebsiella pneumoniae: A Propensity Score-Matched Cohort Study. Antibiotics. 2023; 12(2):273. https://doi.org/10.3390/antibiotics12020273
Chicago/Turabian StyleZha, Lei, Xue Zhang, Yusheng Cheng, Qiancheng Xu, Lingxi Liu, Simin Chen, Zhiwei Lu, Jun Guo, and Boris Tefsen. 2023. "Intravenous Polymyxin B as Adjunctive Therapy to High-Dose Tigecycline for the Treatment of Nosocomial Pneumonia Due to Carbapenem-Resistant Acinetobacter baumannii and Klebsiella pneumoniae: A Propensity Score-Matched Cohort Study" Antibiotics 12, no. 2: 273. https://doi.org/10.3390/antibiotics12020273