
A Multicentric Observational Study to Determine Myocardial Injury in Severe Community-Acquired Pneumonia (sCAP)
 , , , and
, , , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Subjects
2.3. Data Collection and Definition
2.4. Biomarker Analysis
2.4.1. Cardiac Damage Biomarkers
2.4.2. Cell Damage Biomarkers
2.5. Cardiac Imaging
2.6. Objectives
2.7. Statistical Analysis
3. Results
3.1. Population Description
3.2. Cardiac Biomarkers
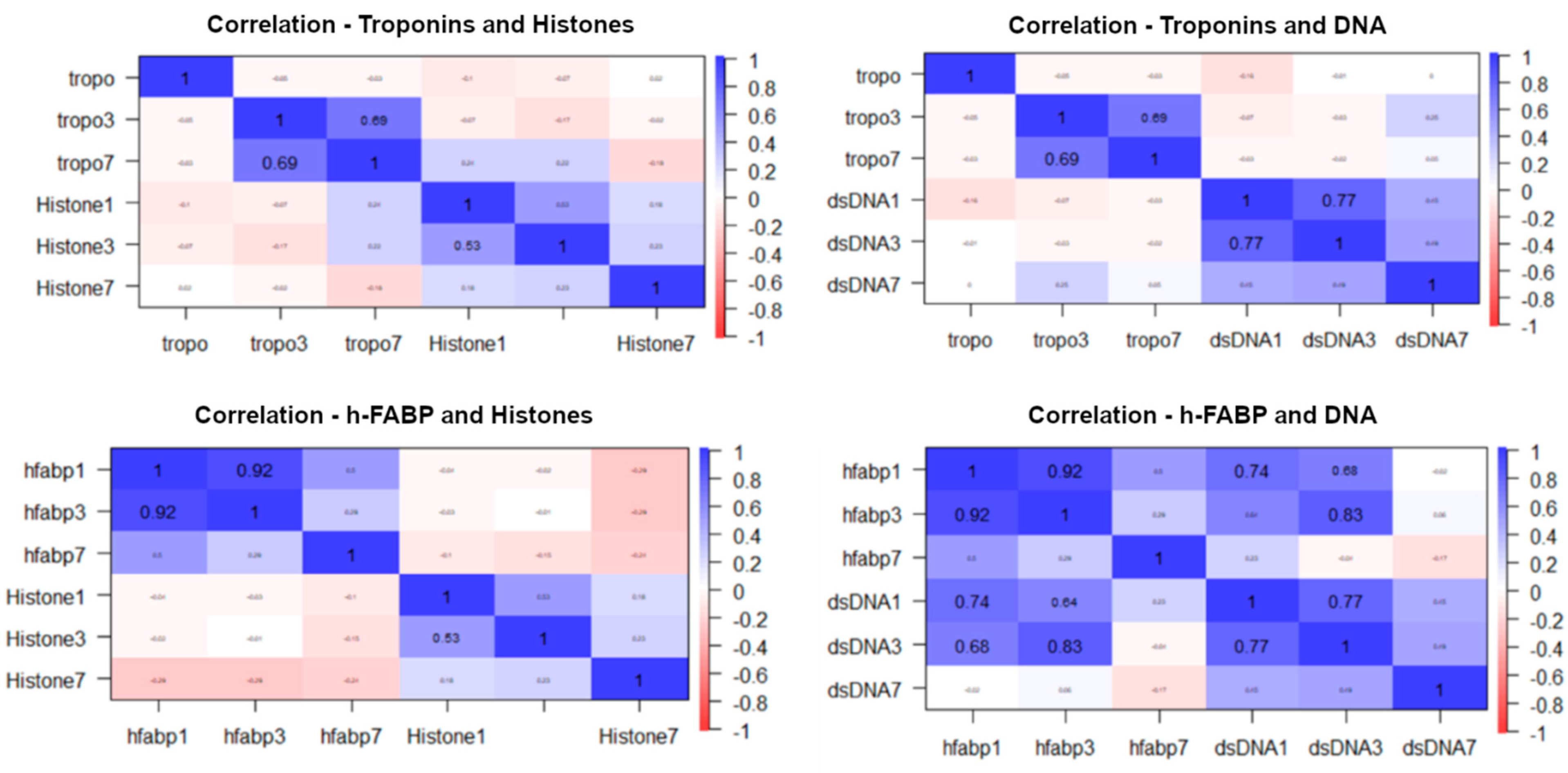
3.3. Inflammatory Biomarkers
3.4. Cardiac MRI
3.5. Clinical Outcomes and Myocardial Damage
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Troeger, C.; Forouzanfar, M.; Rao, P.C.; Khalil, I.; Brown, A.; Swartz, S.; Fullman, N.; Mosser, J.; Thompson, R.L.; Reiner, R.C., Jr.; et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory tract infections in 195 countries: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect. Dis. 2017, 17, 1133–1161. [Google Scholar] [CrossRef] [PubMed]
- Martin-Loeches, I.; Garduno, A.; Povoa, P.; Nseir, S. Choosing antibiotic therapy for severe community-acquired pneumonia. Curr. Opin. Infect. Dis. 2022, 35, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Martin-Loeches, I.; Torres, A. New guidelines for severe community-acquired pneumonia. Curr. Opin. Pulm. Med. 2021, 27, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Chalmers, J.D.; Dela Cruz, C.S.; Dominedò, C.; Kollef, M.; Martin-Loeches, I.; Niederman, M.; Wunderink, R.G. Challenges in severe community-acquired pneumonia: A point-of-view review. Intensive Care Med. 2019, 45, 159–171. [Google Scholar] [CrossRef] [PubMed]
- Corrales-Medina, V.F.; Alvarez, K.N.; Weissfeld, L.A.; Angus, D.C.; Chirinos, J.A.; Chang, C.C.; Newman, A.; Loehr, L.; Folsom, A.R.; Elkind, M.S.; et al. Association between hospitalization for pneumonia and subsequent risk of cardiovascular disease. JAMA 2015, 313, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, J.; Aliberti, S.; Mirsaeidi, M.; Peyrani, P.; Filardo, G.; Amir, A.; Moffett, B.; Gordon, J.; Blasi, F.; Bordon, J. Acute myocardial infarction in hospitalized patients with community-acquired pneumonia. Clin. Infect. Dis. 2008, 47, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Reyes, L.F.; Restrepo, M.I.; Hinojosa, C.A.; Soni, N.J.; Anzueto, A.; Babu, B.L.; Gonzalez-Juarbe, N.; Rodriguez, A.H.; Jimenez, A.; Chalmers, J.D.; et al. Severe Pneumococcal Pneumonia Causes Acute Cardiac Toxicity and Subsequent Cardiac Remodeling. Am. J. Respir. Crit. Care. Med. 2017, 196, 609–620. [Google Scholar] [CrossRef] [PubMed]
- Corrales-Medina, V.F.; Suh, K.N.; Rose, G.; Chirinos, J.A.; Doucette, S.; Cameron, D.W.; Fergusson, D.A. Cardiac complications in patients with community-acquired pneumonia: A systematic review and meta-analysis of observational studies. PLoS Med. 2011, 8, e1001048. [Google Scholar] [CrossRef] [PubMed]
- Gilley, R.P.; González-Juarbe, N.; Shenoy, A.T.; Reyes, L.F.; Dube, P.H.; Restrepo, M.I.; Orihuela, C.J. Infiltrated Macrophages Die of Pneumolysin-Mediated Necroptosis following Pneumococcal Myocardial Invasion. Infect. Immun. 2016, 84, 1457–1469. [Google Scholar] [CrossRef] [PubMed]
- González-Juarbe, N.; Gilley, R.P.; Hinojosa, C.A.; Bradley, K.M.; Kamei, A.; Gao, G.; Dube, P.H.; Bergman, M.A.; Orihuela, C.J. Pore-Forming Toxins Induce Macrophage Necroptosis during Acute Bacterial Pneumonia. PLoS Pathog. 2015, 11, e1005337. [Google Scholar] [CrossRef]
- Tremblay, J.A.; Peron, F.; Kreitmann, L.; Textoris, J.; Brengel-Pesce, K.; Lukaszewicz, A.C.; Quemeneur, L.; Vedrine, C.; Tan, L.K.; Venet, F.; et al. A stratification strategy to predict secondary infection in critical illness-induced immune dysfunction: The REALIST score. Ann. Intensive Care 2022, 12, 76. [Google Scholar] [CrossRef] [PubMed]
- Ambale-Venkatesh, B.; Lima, J.A. Cardiac MRI: A central prognostic tool in myocardial fibrosis. Nat. Rev. Cardiol. 2015, 12, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Todiere, G.; Barison, A.; Baritussio, A.; Cipriani, A.; Guaricci, A.I.; Pica, S.; Indolfi, C.; Pontone, G.; Dellegrottaglie, S. Acute clinical presentation of nonischemic cardiomyopathies: Early detection by cardiovascular magnetic resonance. J. Cardiovasc. Med. 2022, 24, e36–e46. [Google Scholar] [CrossRef] [PubMed]
- Thomas, K.E.; Fotaki, A.; Botnar, R.M.; Ferreira, V.M. Imaging Methods: Magnetic Resonance Imaging. Circ. Cardiovasc Imaging 2023, 16, e014068. [Google Scholar] [CrossRef] [PubMed]
- Capone, F.; Cipriani, A.; Molinari, L.; Poretto, A.; Sella, N.; Boscolo, A.; Campello, E.; Saller, A.; Vettor, R.; Navalesi, P.; et al. Cardiac injury and COVID-19 associated coagulopathy in patients with acute SARS-CoV-2 pneumonia: A rotational thromboelastometry study. Adv. Med. Sci. 2022, 67, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Counseller, Q.; Aboelkassem, Y. Recent technologies in cardiac imaging. Front. Med. Technol. 2022, 4, 984492. [Google Scholar] [CrossRef] [PubMed]
- Cangemi, R.; Carnevale, R.; Cammisotto, V.; Nocella, C.; Bartimoccia, S.; Taliani, G.; Falcone, M.; Calvieri, C.; Pignatelli, P.; Violi, F. Corticosteroid use, myocardial injury and in-hospital cardiovascular events in patients with community-acquired pneumonia. Br. J. Clin. Pharmacol. 2022, 88, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Africano, H.F.; Serrano-Mayorga, C.C.; Ramirez-Valbuena, P.C.; Bustos, I.G.; Bastidas, A.; Vargas, H.A.; Gómez, S.; Rodriguez, A.; Orihuela, C.J.; Reyes, L.F. Major Adverse Cardiovascular Events during Invasive Pneumococcal Disease Are Serotype Dependent. Clin. Infect. Dis. 2021, 72, e711–e719. [Google Scholar] [CrossRef] [PubMed]
- Siddiq, M.M.; Chan, A.T.; Miorin, L.; Yadaw, A.S.; Beaumont, K.G.; Kehrer, T.; Cupic, A.; White, K.M.; Tolentino, R.E.; Hu, B.; et al. Functional Effects of Cardiomyocyte Injury in COVID-19. J. Virol. 2022, 96, e0106321. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, M.D.; Cunningham, W.A. Type I and Type II error concerns in fMRI research: Re-balancing the scale. Soc. Cogn. Affect. Neurosci. 2009, 4, 423–428. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall (n = 23) | Pn (n = 13) | No Pn (n = 10) * | p | |
|---|---|---|---|---|
| Demographics | ||||
| Age, median (IQR) | 45 (40–50) | 48 (43–51) | 42 (40–50) | 0.43 |
| Sex male, n (%) | 11 (47) | 6 (46.1) | 5 (50) | 1.00 |
| APACHE II score, median (IQR) | 13 (7–17) | 13 (9–15) | 16 (11–17) | 0.15 |
| CURB-65, median (IQR) | 2 (1–3) | 1 (1–2) | 2 (2–3) | 0.03 |
| CPIS, median (IQR) | 6 (4–7) | 6 (4–7) | 5.5 (4–6) | 0.90 |
| SOFA, median (IQR) | 4 (3–6) | 3 (3–6) | 5 (4–6) | 0.16 |
| Symptoms onset (days), median (IQR) | 4 (2–5) | 4 (2–4) | 5 (2–7) | 0.20 |
| Treatment received | ||||
| Hours to ATB, median (IQR) | 3 (1.5–4.0) | 2 (2–4) | 3.5 (2–4) | 0.63 |
| Combination ATB treatment, n (%) | 21 (95.4) | 12 (92.3) | 10 (100) | 1.00 |
| ATB treatment duration, median (IQR) | 8 (7–14) | 7 (7–8) | 12 (10–26) | 0.03 |
| Corticosteroids on admission, n (%) | 5 (22.7) | 2 (15.4) | 3 (30) | 0.73 |
| Complications | ||||
| Bacteremia, n (%) | 10 (45.4) | 9 (69.2) | 1 (10) | 0.01 |
| ARDS, n (%) | 6 (26.0) | 4 (30.8) | 2 (20) | 0.91 |
| Empyema, n (%) | 4 (17.4) | 2 (15.4) | 2 (20) | 1.00 |
| Abscess, n (%) | 1 (4.5) | 0 | 1 (10) | 0.89 |
| Ventilatory support | ||||
| Invasive MV, n (%) | 2 (8.5) | 1 (7.7) | 1 (10) | 1.00 |
| NIV, n (%) | 2 (8.5) | 0 | 2 (20) | 0.34 |
| HFNO, n (%) | 12 (52.2) | 10 (76.9) | 2 (20) | 0.02 |
| Clinical resolution time | ||||
| Highest/lowest leukocytosis, median (IQR), days | 5.5 (3–10) | 3 (2–6) | 6 (5–9) | 0.06 |
| Highest/lowest fever, median (IQR) days | 0.5 (0–1) | 0.3 (0–1) | 1 (0–1.5) | 0.03 |
| Highest/lowest secretions, median (IQR) days | 3 (2–5) | 2 (2–4) | 3.5 (1.5–5) | 0.47 |
| Highest/lowest infiltrates, median (IQR) days | 9 (5–12) | 7 (5–11) | 11 (9–20) | 0.02 |
| Highest/lowest PaO2/FiO2, median (IQR) days | 3 (2–5) | 3 (2–6) | 3 (2–4) | 0.90 |
| Outcomes | ||||
| Crude mortality in ICU, n (%) | 2 (8.7) | 2 (15.4) | 0 | 0.58 |
| Crude mortality in Hospital, n (%) | 2 (8.7) | 2 (15.4) | 0 | 0.58 |
| ICU stay (days), median (IQR) | 5.5 (3–10) | 5 (3–8) | 6 (4–10) | 0.70 |
| Hospital stay (days), median (IQR) | 13.5 (9–20) | 13 (10–17) | 15 (9–26) | 0.53 |
| Overall (n = 23) | MyD | Pn (n = 13) | MyD | Non-Pn (n = 10) | MyD | p | |
|---|---|---|---|---|---|---|---|
| Tn | |||||||
| Day 1 (median, IQR) | 19.3 (14–27) | 1 (4%) | 22.0 (14–27) | 1 (7.7%) | 14.0 (14.23) | 0 | 0.25 |
| Day 3 (median, IQR) | 13.8 (13–14) | 0 | 14.0 (13.6–13.9) | 0 | 14.0 (17.8–14.4) | 0 | 0.06 |
| day 7 (median, IQR) | 39 (15–61) | 11 (48%) | 49 (18–58) | 7 (54%) | 30 (14–63) | 4 (40%) | 0.45 |
| h-FABP | |||||||
| Day 1 (median, IQR) | 2.4 (1.5–4.3) | 2 (8.7%) | 2.3 (1.4–3.1) | 0 | 2.4 (1.9–4.7) | 2 (20%) | 0.43 |
| Day 3 (median, IQR) | 2.4 (1.2–3.6) | 1 (4.4%) | 2.6 (0.9–3.8) | 1 (7.7%) | 2.0 (1.3–3.3) | 1 (10%) | 0.92 |
| Day 7 (median, IQR) | 1.3 (0.9–1.5) | 1 (4.4%) | 1.4 (1.0–1.6) | 0 | 1.0 (0.6–1.4) | 1 (10%) | 0.25 |
| NT-proBNP | |||||||
| Day 1 (median, IQR) | 1800 (1570–2033) | 20 (87%) | 1730 (1090–1860) | 10 (77%) | 1848 (1690–2166) | 10 (100%) | 0.33 |
| Day 3 (median, IQR) | 1424 (1100–1695) | 18 (78%) | 1370 (967–1600) | 10 (77%) | 1500 (1300–2265) | 8 (80%) | 0.43 |
| Day 7 (median, IQR) | 1170 (941–1455) | 17 (74%) | 1250 (1040–1500) | 10 (77%) | 1150 (898–1295) | 7 (70%) | 0.87 |
| Overall (n = 23) | PN (n = 13) | Non-Pn (n = 10) | p-Value | |
|---|---|---|---|---|
| IL-1 | ||||
| Day 1 (median, IQR) | 48.8 (35.9–53.4) | 48.8 (43.2–54.0) | 45.3 (33.8–52.0) | 1.0 |
| Day 3 (median, IQR) | 44.1 (20.9–53.1) | 46.3 (35.5–51.2) | 36.7 (16.4–72.6) | 0.9 |
| Day 7 (median, IQR) | 19.9 (16.5–21.0) | 19.8 (17.3–21.6) | 16.8 (9.7–19.0) | 0.2 |
| Histone | ||||
| Day 1 (median, IQR) | 0.26 (0.23–0.28) | 0.27 (0.23–0.29) | 0.24 (0.23–0.27) | 0.41 |
| Day 3 (median, IQR) | 0.28 (0.26–0.30) | 0.28 (0.27–0.30) | 0.27 (0.24–0.30) | 0.43 |
| Day 7 (median, IQR) | 0.46 (0.38–0.52) | 0.48 (0.45–0.53) | 0.34 (0.23–0.47) | 0.05 |
| DNAs | ||||
| Day 1 (median, IQR) | 37.3 (33.2–45.7) | 37.3 (35.7–45.4) | 38.6 (33.1–45.8) | 0.87 |
| Day 3 (median, IQR) | 37.4 (34.7–40.5) | 38.2 (35.5–42.8) | 35.5 (33.5–38.2) | 0.16 |
| Day 7 (median, IQR) | 33.7 (33.0–35.0) | 33.8 (33.4–35.3) | 33.6 (29.4–34.5) | 0.40 |
| Alive (n = 21) | Dead (n = 2) | |||||
|---|---|---|---|---|---|---|
| Day 1 | Day 3 | Day 7 | Day 1 | Day 3 | Day 7 | |
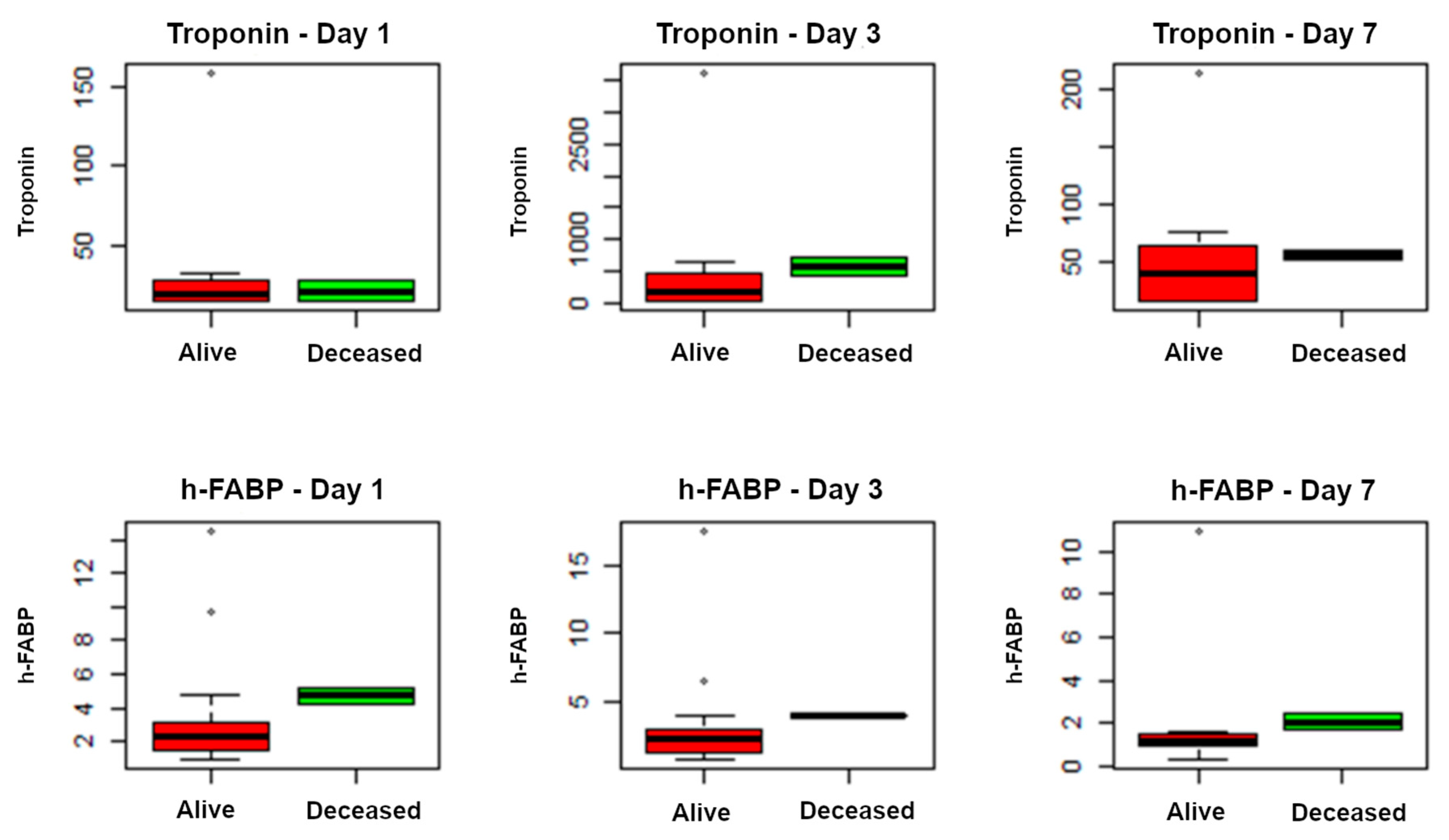
| Tn (median, IQR) | 19 (14–27) | 171 (14–471) | 38 (14–64) | 21 (18–24) | 571 (500–640) | 55 (53–57) |
| h-FABP (median, IQR) | 2.2 (1.4–3.1) | 2.2 (1.2–3.0) | 1.1 (0.9–1.5) * | 4.7 (4.5–4.9) | 3.9 (3.8–3.9) | 2.0 (1.8–2.2) * |
| Histones (median, IQR) | 0.25 (0.23–0.27) | 0.27 (0.26–0.30) | 0.47 (0.38–0.53) | 0.28 (0.28–0.29) | 0.30 (0.30–0.30) | 0.45 (0.44–0.46) |
| IL-1 (median, IQR) | 48 (31–50) | 36 (19–54) | 17 (16–20) | 54 (54–54) | 49 (48–51) | 23 (22–24) |
| DNA (median, IQR) | 37 (33–44) | 37 (34–39) | 33 (32–34) | 47 (46–48) | 47 (46–47) | 36 (35–36) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin-Loeches, I.; Maggi, G.; Diaz, E.; Marín-Corral, J.; Guedea, A.; Restrepo, M.I.; Reyes, L.F.; Rodríguez, A. A Multicentric Observational Study to Determine Myocardial Injury in Severe Community-Acquired Pneumonia (sCAP). Antibiotics 2023, 12, 1710. https://doi.org/10.3390/antibiotics12121710
Martin-Loeches I, Maggi G, Diaz E, Marín-Corral J, Guedea A, Restrepo MI, Reyes LF, Rodríguez A. A Multicentric Observational Study to Determine Myocardial Injury in Severe Community-Acquired Pneumonia (sCAP). Antibiotics. 2023; 12(12):1710. https://doi.org/10.3390/antibiotics12121710
Chicago/Turabian StyleMartin-Loeches, Ignacio, Giampaolo Maggi, Emili Diaz, Judith Marín-Corral, Alfonso Guedea, Marcos I. Restrepo, Luis F. Reyes, and Alejandro Rodríguez. 2023. "A Multicentric Observational Study to Determine Myocardial Injury in Severe Community-Acquired Pneumonia (sCAP)" Antibiotics 12, no. 12: 1710. https://doi.org/10.3390/antibiotics12121710