
Impact of Antibiotic Consumption on the Acquisition of Extended-Spectrum β-Lactamase Producing Enterobacterales Carriage during the COVID-19 Crisis in French Guiana


 ,
,
Abstract
:1. Introduction
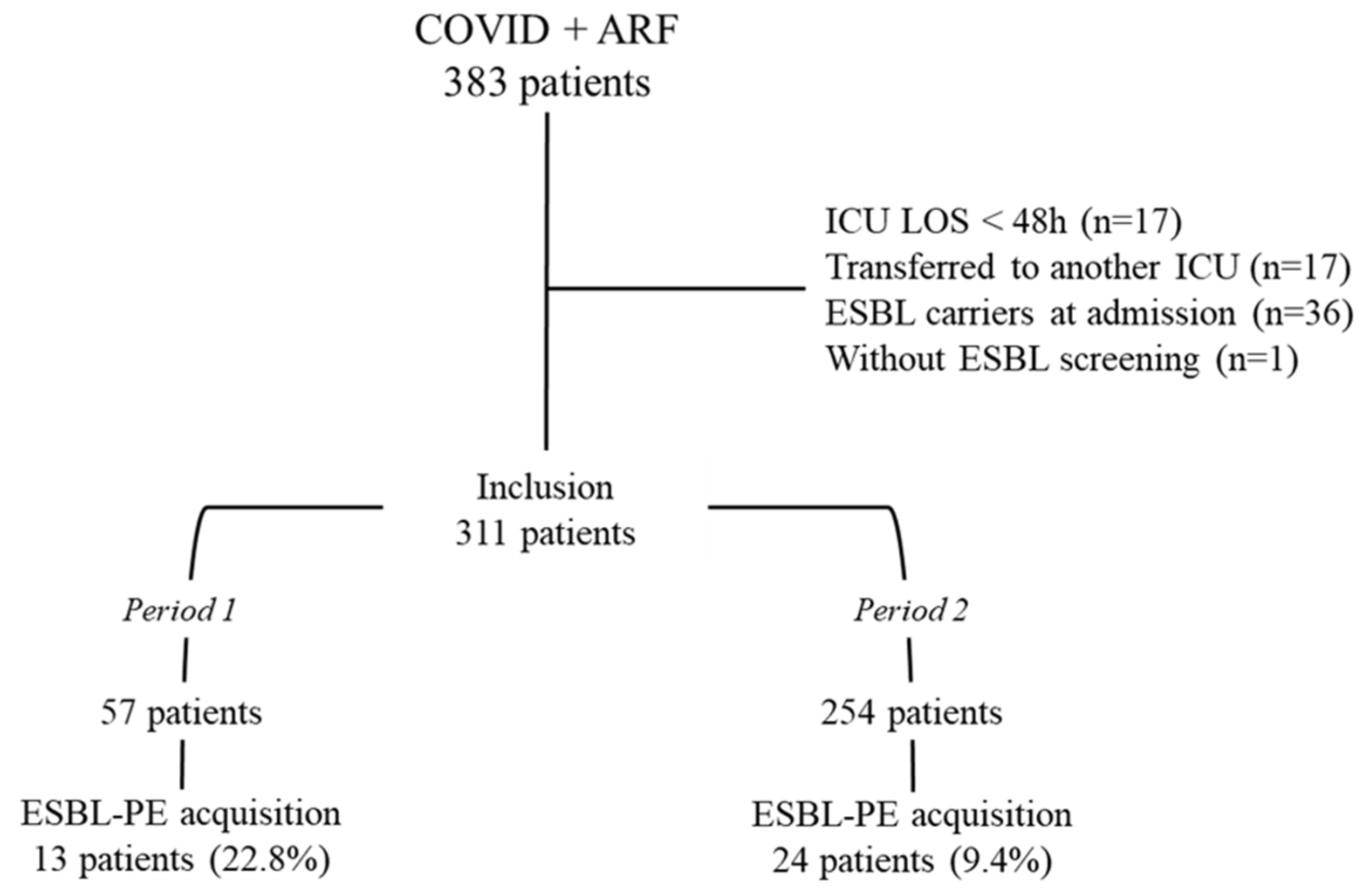
2. Results
3. Discussion
4. Materials and Methods
4.1. Setting and Patients
4.2. Data Collection and Definitions
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- CDC The Biggest Antibiotic-Resistant Threats in the U.S. Available online: https://www.cdc.gov/drugresistance/biggest_threats.html (accessed on 27 December 2018).
- Thouverez, M.; Talon, D.; Bertrand, X. Control of Enterobacteriaceae Producing Extended-Spectrum Beta-Lactamase in Intensive Care Units: Rectal Screening May Not Be Needed in Non-Epidemic Situations. Infect. Control Hosp. Epidemiol. 2004, 25, 838–841. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.D.; McGregor, J.C.; Johnson, J.A.; Strauss, S.M.; Moore, A.C.; Standiford, H.C.; Hebden, J.N.; Morris, J.G. Risk Factors for Colonization with Extended-Spectrum Beta-Lactamase-Producing Bacteria and Intensive Care Unit Admission. Emerg. Infect. Dis. 2007, 13, 1144–1149. [Google Scholar] [CrossRef] [PubMed]
- Friedmann, R.; Raveh, D.; Zartzer, E.; Rudensky, B.; Broide, E.; Attias, D.; Yinnon, A.M. Prospective Evaluation of Colonization with Extended-Spectrum Beta-Lactamase (ESBL)-Producing Enterobacteriaceae among Patients at Hospital Admission and of Subsequent Colonization with ESBL-Producing Enterobacteriaceae among Patients during Hospitalization. Infect. Control Hosp. Epidemiol. 2009, 30, 534–542. [Google Scholar] [CrossRef]
- Blanco, N.; O’Hara, L.M.; Harris, A.D. Transmission Pathways of Multidrug-Resistant Organisms in the Hospital Setting: A Scoping Review. Infect. Control Hosp. Epidemiol. 2019, 40, 447–456. [Google Scholar] [CrossRef]
- Gurieva, T.; Dautzenberg, M.J.D.; Gniadkowski, M.; Derde, L.P.G.; Bonten, M.J.M.; Bootsma, M.C.J. The Transmissibility of Antibiotic-Resistant Enterobacteriaceae in Intensive Care Units. Clin. Infect. Dis. 2018, 66, 489–493. [Google Scholar] [CrossRef] [Green Version]
- Tacconelli, E.; Górska, A.; Angelis, G.D.; Lammens, C.; Restuccia, G.; Schrenzel, J.; Huson, D.H.; Carević, B.; Preoţescu, L.; Carmeli, Y.; et al. Estimating the Association between Antibiotic Exposure and Colonization with Extended-Spectrum β-Lactamase-Producing Gram-Negative Bacteria Using Machine Learning Methods: A Multicentre, Prospective Cohort Study. Clin. Microbiol. Infect. 2020, 26, 87–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchaim, D.; Gottesman, T.; Schwartz, O.; Korem, M.; Maor, Y.; Rahav, G.; Karplus, R.; Lazarovitch, T.; Braun, E.; Sprecher, H.; et al. National Multicenter Study of Predictors and Outcomes of Bacteremia upon Hospital Admission Caused by Enterobacteriaceae Producing Extended-Spectrum Beta-Lactamases. Antimicrob. Agents Chemother. 2010, 54, 5099–5104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilmis, B.; Cattoir, V.; Lecointe, D.; Limelette, A.; Grall, I.; Mizrahi, A.; Marcade, G.; Poilane, I.; Guillard, T.; Bourgeois Nicolaos, N.; et al. Carriage of ESBL-Producing Enterobacteriaceae in French Hospitals: The PORTABLSE Study. J. Hosp. Infect. 2018, 98, 247–252. [Google Scholar] [CrossRef]
- Barbier, F.; Pommier, C.; Essaied, W.; Garrouste-Orgeas, M.; Schwebel, C.; Ruckly, S.; Dumenil, A.-S.; Lemiale, V.; Mourvillier, B.; Clec’h, C.; et al. Colonization and Infection with Extended-Spectrum β-Lactamase-Producing Enterobacteriaceae in ICU Patients: What Impact on Outcomes and Carbapenem Exposure? J. Antimicrob. Chemother. 2016, 71, 1088–1097. [Google Scholar] [CrossRef] [Green Version]
- Fernández, P.; Moreno, L.; Yagüe, G.; Andreu, E.; Jara, R.; Segovia, M. Colonization by Multidrug-Resistant Microorganisms in ICU Patients during the COVID-19 Pandemic. Med. Intensiv. 2021, 45, 313–315. [Google Scholar] [CrossRef]
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A. Bacterial and Fungal Coinfection in Individuals with Coronavirus: A Rapid Review to Support COVID-19 Antimicrobial Prescribing. Clin. Infect. Dis. 2020, 71, 2459–2468. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.-P.R.; Daneman, N. Bacterial Co-Infection and Secondary Infection in Patients with COVID-19: A Living Rapid Review and Meta-Analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef] [PubMed]
- ANZIC Influenza Investigators; Webb, S.A.R.; Pettilä, V.; Seppelt, I.; Bellomo, R.; Bailey, M.; Cooper, D.J.; Cretikos, M.; Davies, A.R.; Finfer, S.; et al. Critical Care Services and 2009 H1N1 Influenza in Australia and New Zealand. N. Engl. J. Med. 2009, 361, 1925–1934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bashir, A.; Abdullah, M.S.; Momin, N.R.; Chong, P.L.; Asli, R.; Ivan, B.M.; Chong, V.H. Prevalence of Primary Bacterial Co-Infections among Patients with COVID-19 in Brunei Darussalam. West. Pac. Surveill. Response J. 2021, 12, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Joseph, C.; Togawa, Y.; Shindo, N. Bacterial and Viral Infections Associated with Influenza. Influenza Other Respir. Virus. 2013, 7 (Suppl. S2), 105–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alhazzani, W.; Møller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). Intensive Care Med. 2020, 46, 854–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Hadidi, S.H.; Alhussain, H.; Abdel Hadi, H.; Johar, A.; Yassine, H.M.; Al Thani, A.A.; Eltai, N.O. The Spectrum of Antibiotic Prescribing During COVID-19 Pandemic: A Systematic Literature Review. Microb. Drug Resist. 2021, 27, 1705–1725. [Google Scholar] [CrossRef]
- Kallel, H.; Rozé, B.; Pons, B.; Mayence, C.; Mathien, C.; Resiere, D.; Melot, B.; Hommel, D.; Mehdaoui, H.; Carles, M. Infections tropicales graves dans les départements français d’Amérique, Antilles françaises et Guyane. Med. Intensive Rea. 2019, 28, 202–216. [Google Scholar] [CrossRef]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-Infections in People with COVID-19: A Systematic Review and Meta-Analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef]
- Rouzé, A.; Martin-Loeches, I.; Povoa, P.; Metzelard, M.; Du Cheyron, D.; Lambiotte, F.; Tamion, F.; Labruyere, M.; Geronimi, C.B.; Nieszkowska, A.; et al. Early Bacterial Identification among Intubated Patients with COVID-19 or Influenza Pneumonia: A European Multicenter Comparative Clinical Trial. Am. J. Respir. Crit. Care Med. 2021, 204, 546–556. [Google Scholar] [CrossRef]
- Baskaran, V.; Lawrence, H.; Lansbury, L.E.; Webb, K.; Safavi, S.; Zainuddin, N.I.; Huq, T.; Eggleston, C.; Ellis, J.; Thakker, C.; et al. Co-Infection in Critically Ill Patients with COVID-19: An Observational Cohort Study from England. J. Med. Microbiol. 2021, 70, 001350. [Google Scholar] [CrossRef] [PubMed]
- Morris, A.C.; Kohler, K.; De Corte, T.; Ercole, A.; De Grooth, H.-J.; Elbers, P.W.G.; Povoa, P.; Morais, R.; Koulenti, D.; Jog, S.; et al. Co-Infection and ICU-Acquired Infection in COIVD-19 ICU Patients: A Secondary Analysis of the UNITE-COVID Data Set. Crit. Care 2022, 26, 236. [Google Scholar] [CrossRef] [PubMed]
- Detsis, M.; Karanika, S.; Mylonakis, E. ICU Acquisition Rate, Risk Factors, and Clinical Significance of Digestive Tract Colonization with Extended-Spectrum Beta-Lactamase-Producing Enterobacteriaceae: A Systematic Review and Meta-Analysis. Crit. Care Med. 2017, 45, 705–714. [Google Scholar] [CrossRef]
- Kallel, H.; Houcke, S.; Resiere, D.; Court, T.; Roncin, C.; Raad, M.; Nkontcho, F.; Demar, M.; Pujo, J.; Hommel, D.; et al. Prior Carriage Predicts Intensive Care Unit Infections Caused by Extended-Spectrum Beta-Lactamase-Producing Enterobacteriaceae. Am. J. Trop. Med. Hyg. 2022, 106, 525. [Google Scholar] [CrossRef] [PubMed]
- Zahar, J.-R.; Blot, S.; Nordmann, P.; Martischang, R.; Timsit, J.-F.; Harbarth, S.; Barbier, F. Screening for Intestinal Carriage of Extended-Spectrum Beta-Lactamase-Producing Enterobacteriaceae in Critically Ill Patients: Expected Benefits and Evidence-Based Controversies. Clin. Infect. Dis. 2019, 68, 2125–2130. [Google Scholar] [CrossRef]
- Thomas, G.R.; Corso, A.; Pasterán, F.; Shal, J.; Sosa, A.; Pillonetto, M.; Peral, R.T.d.S.; Hormazábal, J.C.; Araya, P.; Saavedra, S.Y.; et al. Increased Detection of Carbapenemase-Producing Enterobacterales Bacteria in Latin America and the Caribbean during the COVID-19 Pandemic. Emerg. Infect. Dis. 2022, 28, 11. [Google Scholar] [CrossRef]
- Emeraud, C.; Figueiredo, S.; Bonnin, R.A.; Khecharem, M.; Ouzani, S.; Leblanc, P.-E.; Jousset, A.B.; Fortineau, N.; Duranteau, J.; Dortet, L. Outbreak of CTX-M-15 Extended-Spectrum β-Lactamase-Producing Klebsiella Pneumoniae ST394 in a French Intensive Care Unit Dedicated to COVID-19. Pathogens 2021, 10, 1426. [Google Scholar] [CrossRef]
- Tiri, B.; Sensi, E.; Marsiliani, V.; Cantarini, M.; Priante, G.; Vernelli, C.; Martella, L.A.; Costantini, M.; Mariottini, A.; Andreani, P.; et al. Antimicrobial Stewardship Program, COVID-19, and Infection Control: Spread of Carbapenem-Resistant Klebsiella Pneumoniae Colonization in ICU COVID-19 Patients. What Did Not Work? J. Clin. Med. 2020, 9, 2744. [Google Scholar] [CrossRef]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical Predictors of Mortality Due to COVID-19 Based on an Analysis of Data of 150 Patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [Green Version]
- Guisado-Gil, A.B.; Infante-Domínguez, C.; Peñalva, G.; Praena, J.; Roca, C.; Navarro-Amuedo, M.D.; Aguilar-Guisado, M.; Espinosa-Aguilera, N.; Poyato-Borrego, M.; Romero-Rodríguez, N.; et al. Impact of the COVID-19 Pandemic on Antimicrobial Consumption and Hospital-Acquired Candidemia and Multidrug-Resistant Bloodstream Infections. Antibiotics 2020, 9, 816. [Google Scholar] [CrossRef]
- Ng, T.M.; Tan, S.H.; Heng, S.T.; Tay, H.L.; Yap, M.Y.; Chua, B.H.; Teng, C.B.; Lye, D.C.; Lee, T.H. Effects of Coronavirus Disease 2019 (COVID-19) Pandemic on Antimicrobial Prevalence and Prescribing in a Tertiary Hospital in Singapore. Antimicrob. Resist. Infect. Control 2021, 10, 28. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, R.M.R.; de Mendonça, S.C.B.; Leão, I.N.; Dos Santos, Q.N.; Batista, A.M.; Melo, M.S.; Xavier, M.d.M.; Quintans, L.J., Jr.; da Silva, W.B.; Lobo, I.M.F. Use of Monitoring Indicators in Hospital Management of Antimicrobials. BMC Infect. Dis. 2021, 21, 827. [Google Scholar] [CrossRef] [PubMed]
- Assawatheptawee, K.; Kiddee, A.; Na-Udom, A.; Wangteeraprasert, A.; Treebupachatsakul, P.; Niumsup, P.R. Acquisition of Extended-Spectrum β-Lactamase-Producing Escherichia Coli and Klebsiella Pneumoniae in Intensive Care Units in Thailand. J. Infect. Chemother. 2021, 27, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Lan, C.-K.; Hsueh, P.-R.; Wong, W.-W.; Fung, C.-P.; Lau, Y.-T.; Yeung, J.Y.K.; Young, G.T.; Su, C.-C. Association of Antibiotic Utilization Measures and Reduced Incidence of Infections with Extended-Spectrum Beta-Lactamase-Producing Organisms. J. Microbiol. Immunol. Infect. 2003, 36, 182–186. [Google Scholar] [PubMed]
- Alsterlund, R.; Axelsson, C.; Olsson-Liljequist, B. Long-Term Carriage of Extended-Spectrum Beta-Lactamase-Producing Escherichia Coli. Scand. J. Infect. Dis. 2012, 44, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Kallel, H.; Resiere, D.; Houcke, S.; Hommel, D.; Pujo, J.M.; Martino, F.; Carles, M.; Mehdaoui, H. Antilles-Guyane Association of Critical Care Medicine Critical Care Medicine in the French Territories in the Americas: Current Situation and Prospects. Rev. Panam. Salud Pública 2021, 45, e46. [Google Scholar] [CrossRef] [PubMed]
- Munoz-Price, L.S.; Poirel, L.; Bonomo, R.A.; Schwaber, M.J.; Daikos, G.L.; Cormican, M.; Cornaglia, G.; Garau, J.; Gniadkowski, M.; Hayden, M.K.; et al. Clinical Epidemiology of the Global Expansion of Klebsiella Pneumoniae Carbapenemases. Lancet Infect. Dis. 2013, 13, 785–796. [Google Scholar] [CrossRef] [Green Version]
- Jolivet, S.; Lolom, I.; Bailly, S.; Bouadma, L.; Lortat-Jacob, B.; Montravers, P.; Armand-Lefevre, L.; Timsit, J.-F.; Lucet, J.-C. Impact of Colonization Pressure on Acquisition of Extended-Spectrum β-Lactamase-Producing Enterobacterales and Meticillin-Resistant Staphylococcus aureus in Two Intensive Care Units: A 19-Year Retrospective Surveillance. J. Hosp. Infect. 2020, 105, 10–16. [Google Scholar] [CrossRef]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A New Simplified Acute Physiology Score (SAPS II) Based on a European/North American Multicenter Study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Calandra, T.; Cohen, J. International Sepsis Forum Definition of Infection in the ICU. Crit. Care Med. 2005, 33, 1538–1548. [Google Scholar] [CrossRef] [PubMed]
- Delclaux, C.; Roupie, E.; Blot, F.; Brochard, L.; Lemaire, F.; Brun-Buisson, C. Lower Respiratory Tract Colonization and Infection during Severe Acute Respiratory Distress Syndrome: Incidence and Diagnosis. Am. J. Respir. Crit. Care Med. 1997, 156, 1092–1098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, G. A Modified Poisson Regression Approach to Prospective Studies with Binary Data. Am. J. Epidemiol. 2004, 159, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Cook, R.J.; Sackett, D.L. The Number Needed to Treat: A Clinically Useful Measure of Treatment Effect. BMJ 1995, 310, 452–454. [Google Scholar] [CrossRef]


{kind=link}
| Total | ESBL-PE Carriers | Non-ESBL-PE Carriers | p | ||||
|---|---|---|---|---|---|---|---|
| Nb | Result | Nb | Result | Nb | Result | ||
| Age (years) | 311 | 63 (53–71) | 37 | 66 (60–71) | 274 | 63 (53–71) | 0.173 |
| Male gender | 311 | 159 (51.1%) | 37 | 22 (59.5%) | 274 | 137 (50%) | 0.280 |
| BMI (kg/m2) | 283 | 30 (27–34) | 36 | 28 (27–32) | 247 | 30 (27–35) | 0.298 |
| Simplified Acute Physiology Score | 310 | 29 (24–35) | 37 | 33 (29–37) | 273 | 29 (24–35) | 0.003 |
| Period 1 | 311 | 57 (18.3%) | 37 | 13 (35.1%) | 274 | 44 (16.1%) | 0.005 |
| Period 2 | 311 | 254 (81.7%) | 37 | 24 (64.6%) | 274 | 230 (83.9%) | 0.005 |
| Comorbidities | |||||||
| Diabetes mellitus | 311 | 127 (40.8%) | 37 | 20 (54.1%) | 274 | 107 (39.1%) | 0.081 |
| Hypertension | 311 | 193 (62.1%) | 37 | 25 (67.6%) | 274 | 168 (61.3%) | 0.462 |
| Chronic respiratory failure | 311 | 25 (8%) | 37 | 2 (5.4%) | 274 | 23 (8.4%) | 0.751 |
| Chronic renal failure | 311 | 30 (9.6%) | 37 | 7 (18.9%) | 274 | 23 (8.4%) | 0.042 |
| Dialysis | 311 | 9 (2.9%) | 37 | 3 (8.1%) | 274 | 6 (2.2%) | 0.044 |
| Renal transplantation | 311 | 3 (1%) | 37 | 1 (2.7%) | 274 | 2 (0.7%) | 0.317 |
| Cardiac failure | 311 | 22 (7.1%) | 37 | 4 (10.8%) | 274 | 18 (6.6%) | 0.313 |
| Obesity | 311 | 149 (47.9%) | 37 | 16 (43.2%) | 274 | 133 (48.5%) | 0.545 |
| Sickle cell disease | 311 | 6 (1.9%) | 37 | 0 (0%) | 274 | 6 (2.2%) | 1.000 |
| Malignancy | 311 | 9 (2.9%) | 37 | 0 (0%) | 274 | 9 (3.3%) | 0.606 |
| Delays | |||||||
| Between the symptom onset and hospitalization (days) | 297 | 7 (4–9) | 37 | 6 (4–8) | 260 | 7 (4–9) | 0.623 |
| Between Hospitalization and ICU admission (days) | 311 | 1 (0–3) | 37 | 2 (1–5) | 274 | 1 (0–3) | 0.082 |
| Organ failures at admission to ICU | |||||||
| SOFA score | 311 | 1 (1–1) | 37 | 1 (1–2) | 274 | 1 (1–1) | 0.053 |
| Hemodynamic failure | 311 | 15 (4.8%) | 37 | 2 (5.4%) | 274 | 13 (4.7%) | 0.695 |
| Respiratory failure | 311 | 311 (100%) | 37 | 37 (100%) | 274 | 274 (100%) | - |
| Neurologic failure | 311 | 17 (5.5%) | 37 | 0 (0%) | 274 | 17 (6.2%) | 0.239 |
| Hematologic failure | 311 | 4 (1.3%) | 37 | 2 (5.4%) | 274 | 2 (0.7%) | 0.071 |
| Renal failure | 311 | 48 (15.4%) | 37 | 10 (27%) | 274 | 38 (13.9%) | 0.038 |
| Liver failure | 311 | 3 (1%) | 37 | 0 (0%) | 274 | 3 (1.1%) | 1.000 |
| Documented infection at admission to ICU | 311 | 5 (1.6%) | 37 | 1 (2.7%) | 274 | 4 (1.5%) | 0.471 |
| ESBL-PE | Period 1 | Period 2 | Total |
|---|---|---|---|
| Klebsiella pneumoniae | 11 (84.6%) | 14 (58.3%) | 25 (67.6%) |
| Esherichia coli | 1 (7.7%) | 7 (29.2%) | 8 (21.6%) |
| Enterobacter cloacae | 1 (7.7%) | 1 (4.2%) | 2 (5.4%) |
| Klebsiella aerogenes | 0 | 1 (4.2%) | 1 (2.7%) |
| Enterobacter bugandensis | 0 | 1 (4.2%) | 1 (2.7%) |
| Total | 13 (100%) | 24 (100%) | 37 (100%) |
| Total | ESBL-PE Carriers | Non-ESBL-PE Carriers | p | ||||
|---|---|---|---|---|---|---|---|
| Nb | Result | Nb | Result | Nb | Result | ||
| Antibiotics upon admission | 311 | 119 (38.3%) | 37 | 26 (70.3%) | 274 | 93 (33.9%) | 0.000 |
| Maximal respiratory support | |||||||
| High-flow nasal cannula | 311 | 119 (38.3%) | 37 | 4 (10.8%) | 274 | 115 (42%) | 0.000 |
| Non-invasive ventilation | 311 | 53 (17%) | 37 | 1 (2.7%) | 274 | 52 (19%) | 0.100 |
| Invasive mechanical ventilation | 311 | 139 (44.7%) | 37 | 32 (86.5%) | 274 | 107 (39.1%) | 0.000 |
| Delay from admission to MV (days) | 139 | 2 (0–6) | 32 | 4 (1–8) | 107 | 2 (0–5) | 0.088 |
| MV duration (days) | 139 | 14 (7–24) | 32 | 25 (15–44) | 107 | 11 (5–18) | 0.000 |
| Catecholamines | 311 | 115 (37%) | 37 | 28 (75.7%) | 274 | 87 (31.8%) | 0.000 |
| Delay from admission to catecholamines | 115 | 3 (0–7) | 28 | 4 (0–13) | 87 | 3 (0–7) | 0.275 |
| Catecholamines duration (days) | 115 | 8 (3–17) | 28 | 18 (9–25) | 87 | 6 (2–14) | 0.000 |
| RRT | 311 | 44 (14.1%) | 37 | 10 (27%) | 274 | 34 (12.4%) | 0.017 |
| Delay from admission to RRT (days) | 44 | 7 (1–14) | 10 | 10 (3–16) | 34 | 7 (1–13) | 0.456 |
| RRT duration (days) | 44 | 11 (6–19) | 10 | 10 (6–23) | 34 | 11 (6–16) | 0.844 |
| BLSE-PE carriage | 311 | 37 (11.9%) | 37 | 37 (100%) | 274 | 0 (0%) | - |
| Delay from admission to ESBL-PE carriage | 37 | 14 (10–20) | 37 | 14 (10–20) | 0 | - | - |
| Antibiotics exposure * | 311 | 155 (49.8%) | 37 | 30 (81.1%) | 274 | 125 (45.6%) | 0.000 |
| Amoxicillin clavulanate | 311 | 7 (2.3%) | 37 | 2 (5.4%) | 274 | 5 (1.8%) | 0.197 |
| Cefotaxime | 311 | 115 (37%) | 37 | 25 (67.6%) | 274 | 90 (32.8%) | 0.000 |
| Piperacillin Tazobactam | 311 | 41 (13.2%) | 37 | 7 (18.9%) | 274 | 34 (12.4%) | 0.272 |
| Cefepim | 311 | 19 (6.1%) | 37 | 4 (10.8%) | 274 | 15 (5.5%) | 0.260 |
| Carbapenems | 311 | 19 (6.1%) | 37 | 7 (18.9%) | 274 | 12 (4.4%) | 0.001 |
| Levofloxacin | 311 | 72 (23.2%) | 37 | 19 (51.4%) | 274 | 53 (19.3%) | 0.000 |
| Aminoglycosides | 311 | 29 (9.3%) | 37 | 8 (21.6%) | 274 | 21 (7.7%) | 0.006 |
| ICU-AI | 311 | 78 (25.1%) | 37 | 29 (78.4%) | 274 | 49 (17.9%) | 0.000 |
| Delay ICU-AI from admission (days) | 78 | 10 (6–15) | 29 | 12 (8–16) | 49 | 10 (6–15) | 0.188 |
| ICU-AI caused by ESBL-PE | 78 | 9 (11.5%) | 29 | 9 (31%) | 49 | 0 (0%) | 0.000 |
| Bacteremia | 78 | 45 (57.7%) | 29 | 12 (41.4%) | 49 | 33 (67.3%) | 0.025 |
| Ventilator-associated pneumonia | 139 | 52 (37.4%) | 32 | 23 (71.9%) | 107 | 29 (27.1%) | 0.000 |
| Delay from MV to VAP (days) | 52 | 9 (6–13) | 23 | 10 (8–14) | 29 | 8 (5–11) | 0.110 |
| Candidemia | 311 | 7 (2.3%) | 37 | 4 (10.8%) | 274 | 3 (1.1%) | 0.005 |
| Delay from admission to candidemia (days) | 7 | 16 (9–29) | 4 | 22 (14–29) | 3 | 10 (8–20) | 0.480 |
| Outcome | |||||||
| ICU length of stay (days) | 311 | 10 (6–19) | 37 | 28 (20–48) | 274 | 9 (6–15) | 0.000 |
| Hospital length of stay (days) | 311 | 18 (13–29) | 37 | 37 (25–62) | 274 | 17 (12–24) | 0.000 |
| ICU mortality | 311 | 114 (36.7%) | 37 | 21 (56.8%) | 274 | 93 (33.9%) | 0.007 |
| Withdrawal or withholding life support | 114 | 47 (41.2%) | 21 | 3 (14.3%) | 93 | 44 (47.3%) | 0.006 |
| Hospital mortality | 311 | 119 (38.3%) | 37 | 21 (56.8%) | 274 | 98 (35.8%) | 0.014 |
| p | IRR | 95% CI | ||
|---|---|---|---|---|
| Min | Max | |||
| SAPS II score | 0.817 | 1.001 | 0.985 | 1.018 |
| Renal failure upon admission | 0.465 | 1.263 | 0.674 | 2.364 |
| Mechanical ventilation use | 0.071 | 3.380 | 0.902 | 12.660 |
| Catecholamines use | 0.169 | 2.101 | 0.728 | 6.056 |
| ATB use *: | ||||
| Amoxicillin Clavulanate | 0.280 | 2.537 | 0.624 | 5.076 |
| Cefotaxime | 0.002 | 2.598 | 1.420 | 4.752 |
| Piperacillin Tazobactam | 0.690 | 0.841 | 0.360 | 1.966 |
| Cefepim | 0.577 | 0.784 | 0.334 | 1.839 |
| Carbapenems | 0.292 | 1.450 | 0.725 | 2.898 |
| Constant | 0.000 | 0.017 | 0.006 | 0.046 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lontsi Ngoula, G.; Houcke, S.; Matheus, S.; Nkontcho, F.; Pujo, J.M.; Higel, N.; Ba, A.; Cook, F.; Gourjault, C.; Mounier, R.; et al. Impact of Antibiotic Consumption on the Acquisition of Extended-Spectrum β-Lactamase Producing Enterobacterales Carriage during the COVID-19 Crisis in French Guiana. Antibiotics 2023, 12, 58. https://doi.org/10.3390/antibiotics12010058
Lontsi Ngoula G, Houcke S, Matheus S, Nkontcho F, Pujo JM, Higel N, Ba A, Cook F, Gourjault C, Mounier R, et al. Impact of Antibiotic Consumption on the Acquisition of Extended-Spectrum β-Lactamase Producing Enterobacterales Carriage during the COVID-19 Crisis in French Guiana. Antibiotics. 2023; 12(1):58. https://doi.org/10.3390/antibiotics12010058
Chicago/Turabian StyleLontsi Ngoula, Guy, Stéphanie Houcke, Séverine Matheus, Flaubert Nkontcho, Jean Marc Pujo, Nicolas Higel, Absettou Ba, Fabrice Cook, Cyrille Gourjault, Roman Mounier, and et al. 2023. "Impact of Antibiotic Consumption on the Acquisition of Extended-Spectrum β-Lactamase Producing Enterobacterales Carriage during the COVID-19 Crisis in French Guiana" Antibiotics 12, no. 1: 58. https://doi.org/10.3390/antibiotics12010058