
A Threshold Logistic Modelling Approach for Identifying Thresholds between Antibiotic Use and Methicillin-Resistant Staphylococcus aureus Incidence Rates in Hospitals

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Results
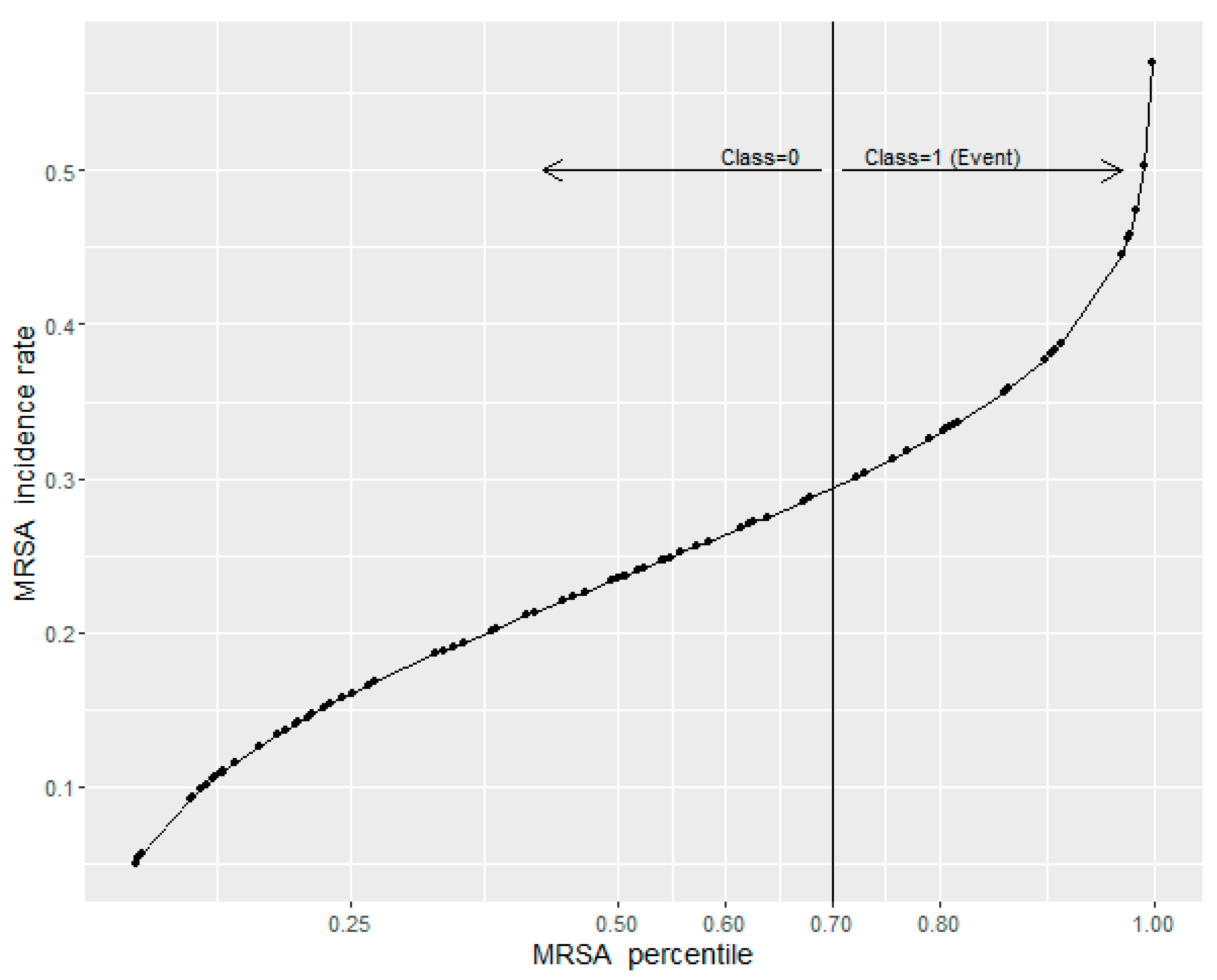
2.1. Defining a Critical Level of MRSA Incidence Rates
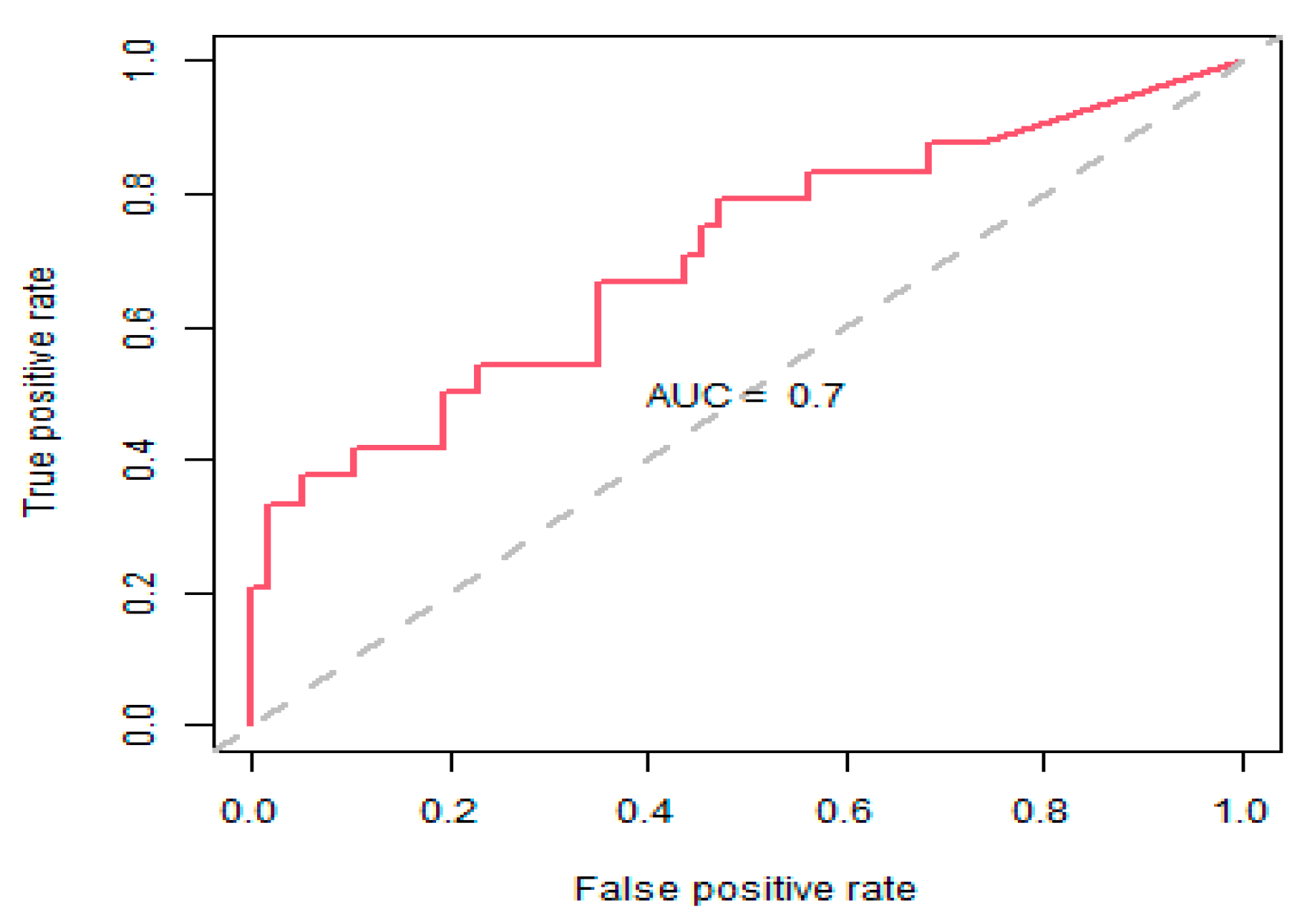
2.2. Threshold Logistic Method
2.3. Risk Scores
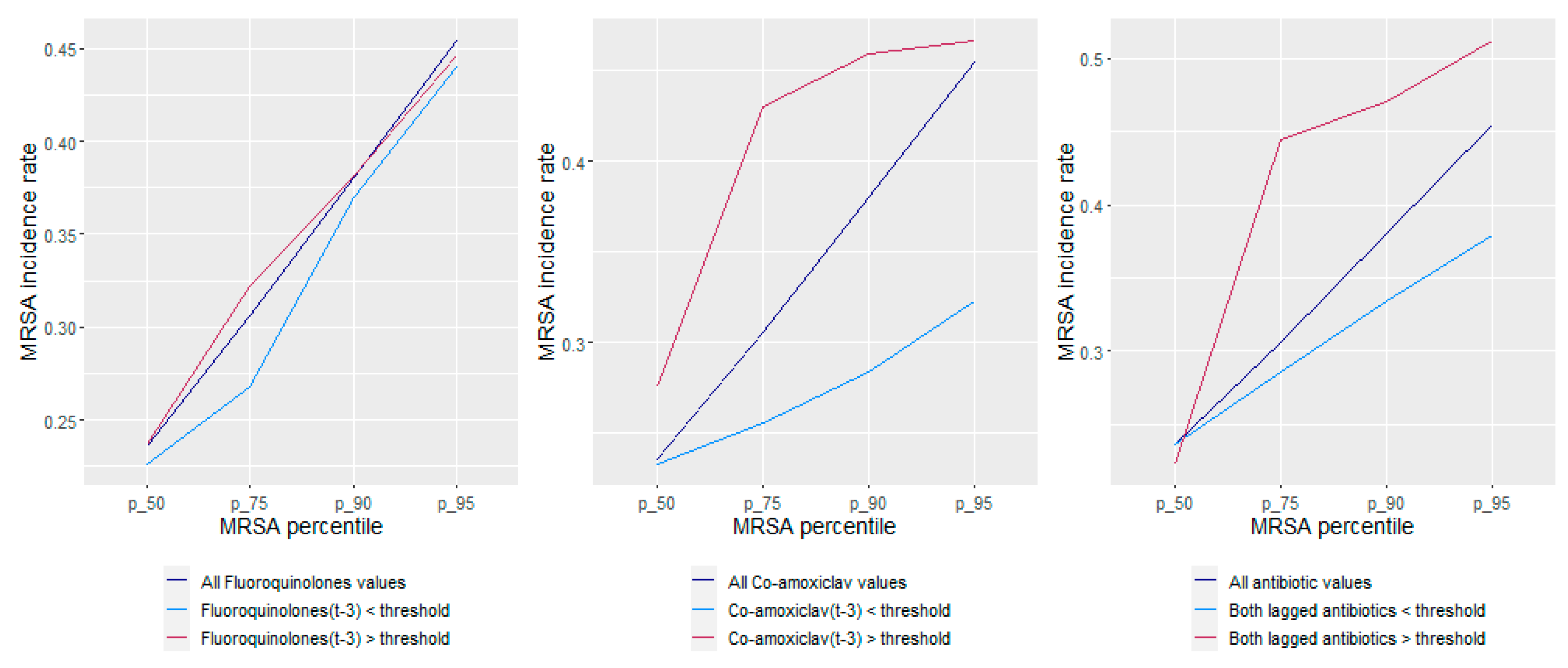
2.4. What-If Scenarios
2.5. Recommendations for Selected Antibiotic Use for Management of Both MRSA and ESBL-Producing E. coli [36]
3. Discussion
4. Methods
4.1. Study Design and Population
4.2. Microbiology and Pharmacy Data
4.3. Modelling and Statistical Analysis
4.3.1. Defining a Critical Level of Pathogen Incidence Rate
4.3.2. Threshold Logistic Method
- the critical level of the MRSA incidence rate between the historical 50th and 85th percentile range;
- the lag structure of the antibiotic series;
- antibiotic threshold values.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aldeyab, M.A.; López-Lozano, J.M.; Gould, I.M. Global antibiotics use and resistance. In Global Pharmaceutical Policy; Babar, Z.-U.-D., Ed.; Palgrave Macmillan: Singapore, 2020; pp. 331–344. ISBN 978-981-15-2723-4. [Google Scholar]
- O’Neill, J. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations. The Review on Antimicrobial Resistance. 2014. Available online: https://amr-review.org/Publications.html (accessed on 3 June 2022).
- Cosgrove, S. The relationship between antimicrobial resistance and patient outcomes: Mortality, length of hospital stay, and health care costs. Clin. Infect. Dis. 2006, 42, S82–S89. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Giacobbe, D.R. A look at the clinical, economic, and societal impact of antimicrobial resistance in 2020. Expert Opin. Pharmacother. 2020, 21, 2067–2071. [Google Scholar] [CrossRef] [PubMed]
- World Bank. Drug-Resistant Infections: A Threat to Our Economic Future; World Bank: Washington, DC, USA, 2017. [Google Scholar]
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Tomson, G.; Vlad, I. The need to look at antibiotic resistance from a health systems perspective. Ups. J. Med. Sci. 2014, 119, 117–124. [Google Scholar] [CrossRef]
- World Health Organization. Everybody’s Business—Strengthening Health Systems to Improve Health Outcomes: WHO’s Framework for Action; World Health Organization: Geneva, Switzerland, 2007; Available online: https://apps.who.int/iris/handle/10665/43918 (accessed on 1 July 2022).
- Davey, P.; Marwick, C.A.; Scott, C.L.; Charani, E.; McNeil, K.; Brown, E.; Gould, I.M.; Ramsay, C.R.; Michie, S. Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane Database Syst. Rev. 2017, 2, CD003543. [Google Scholar] [CrossRef]
- Jirjees, F.J.; Al-Obaidi, H.J.; Sartaj, M.; Conlon-Bingham, G.; Farren, D.; Scott, M.G.; Gould, I.M.; López-Lozano, J.M.; Aldeyab, M.A. Antibiotic use and resistance in hospitals: Time-series analysis strategy for determining and prioritising interventions. Hosp. Pharm. Eur. 2020, 95, 13–19. Available online: https://hospitalpharmacyeurope.com/news/reviews-research/antibiotic-use-and-resistance-in-hospitals-time-series-analysis-strategy-for-determining-and-prioritising-interventions/ (accessed on 1 July 2022).
- Khan, S.; Hasan, S.S.; Bond, S.E.; Conway, B.R.; Aldeyab, M.A. Antimicrobial consumption in patients with COVID-19: A systematic review and meta-analysis. Expert Rev. Anti Infect. Ther. 2022, 20, 749–772. [Google Scholar] [CrossRef]
- Al-Taani, G.M.; Scott, M.; Farren, D.; Gilmore, F.; Mccullagh, B.; Hibberd, C.; Mccorry, A.; Versporten, A.; Goossens, H.; Zarb, P.; et al. Longitudinal point prevalence survey of antibacterial use in Northern Ireland using the European Surveillance of Antimicrobial Consumption (ESAC) PPS and Global-PPS tool. Epidemiol. Infect. 2018, 146, 985–990. [Google Scholar] [CrossRef]
- WHO Report on Surveillance of Antibiotic Consumption: 2016–2018 Early Implementation; World Health Organization: Geneva, Switzerland, 2018.
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.K.M.; Wertheim, H.F.L.; Sumpradit, N.; Vlieghe, E.; Hara, G.L.; Gould, I.M.; Goossens, H.; et al. Antibiotic resistance-the need for global solutions. Lancet Infect. Dis. 2013, 13, 1057–1098. [Google Scholar] [CrossRef]
- Hecker, M.T.; Aron, D.C.; Patel, N.P.; Lehmann, M.K.; Donskey, C.J. Unnecessary use of antimicrobials in hospitalized patients: Current patterns of misuse with an emphasis on the antianaerobic spectrum of activity. Arch. Intern. Med. 2003, 163, 972–978. [Google Scholar] [CrossRef]
- Jirjees, F.; Ahmed, M.; Sayyar, S.; Amini, M.; Al-Obaidi, H.; Aldeyab, M.A. Self-Medication with Antibiotics during COVID-19 in the Eastern Mediterranean Region Countries: A Review. Antibiotics 2022, 11, 733. [Google Scholar] [CrossRef] [PubMed]
- Shbaklo, N.; Corcione, S.; Vicentini, C.; Giordano, S.; Fiorentino, D.; Bianco, G.; Cattel, F.; Cavallo, R.; Zotti, C.M.; De Rosa, F.G. An Observational Study of MDR Hospital-Acquired Infections and Antibiotic Use during COVID-19 Pandemic: A Call for Antimicrobial Stewardship Programs. Antibiotics 2022, 11, 695. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.Y.; Khan, R.A.; Khalid, K.E.; Chong, C.W.; Bakhtiar, A. Correlation between antibiotic consumption and the occurrence of multidrug-resistant organisms in a Malaysian tertiary hospital: A 3-year observational study. Sci. Rep. 2022, 12, 3106. [Google Scholar] [CrossRef] [PubMed]
- López-Lozano, J.-M.; THRESHOLDS Study Group; Lawes, T.; Nebot, C.; Beyaert, A.; Bertrand, X.; Hocquet, D.; Aldeyab, M.; Scott, M.; Conlon-Bingham, G.; et al. A nonlinear time-series analysis approach to identify thresholds in associations between population antibiotic use and rates of resistance. Nat. Microbiol. 2019, 4, 1160–1172. [Google Scholar] [CrossRef] [PubMed]
- Hayajneh, W.A.; Al-Azzam, S.; Yusef, D.; Lattyak, W.J.; Lattyak, E.A.; Gould, I.; López-Lozano, J.-M.; Conway, B.R.; Conlon-Bingham, G.; Aldeyab, M.A. Identification of thresholds in relationships between specific antibiotic use and carbapenem-resistant Acinetobacter baumannii (CRAb) incidence rates in hospitalized patients in Jordan. J. Antimicrob. Chemother. 2021, 76, 524–530. [Google Scholar] [CrossRef]
- Slimings, C.; Riley, T.V. Antibiotics and hospital-acquired Clostridium difficile infection: Update of systematic review and meta-analysis. J. Antimicrob. Chemother. 2014, 69, 881–891. [Google Scholar] [CrossRef]
- Tacconelli, E.; De Angelis, G.; Cataldo, M.A.; Pozzi, E.; Cauda, R. Does antibiotic exposure increase the risk of methicillin-resistant Staphylococcus aureus (MRSA) isolation? A systematic review and meta-analysis. J. Antimicrob. Chemother. 2008, 61, 26–38. [Google Scholar] [CrossRef]
- Lipsitch, M.; Samore, M.H. Antimicrobial use and antimicrobial resistance: A population perspective. Emerg. Infect. Dis. 2002, 8, 347–354. [Google Scholar] [CrossRef]
- Conlon-Bingham, G.M.; Aldeyab, M.; Scott, M.; Kearney, M.P.; Farren, D.; Gilmore, F.; McElnay, J. Effects of antibiotic cycling policy on incidence of healthcare-associated MRSA and Clostridioides difficile infection in secondary healthcare settings. Emerg. Infect. Dis. 2019, 25, 52–62. [Google Scholar] [CrossRef]
- Aldeyab, M.A.; Monnet, D.L.; López-Lozano, J.M.; Hughes, C.M.; Scott, M.; Kearney, M.P.; Magee, F.A.; McElnay, J.C. Modelling the impact of antibiotic use and infection control practices on the incidence of hospital-acquired methicillin-resistant Staphylococcus aureus: A time-series analysis. J. Antimicrob. Chemother. 2008, 62, 593–600. [Google Scholar] [CrossRef]
- Aldeyab, M.A.; Harbarth, S.; Vernaz, N.; Kearney, M.P.; Scott, M.G.; Funston, C.; Savage, K.; Kelly, D.; Aldiab, M.A.; McElnay, J.C. Quasiexperimental study of the effects of antibiotic use, gastric acid-suppressive agents, and infection control practices on the incidence of Clostridium difficile-associated diarrhea in hospitalized patients. Antimicrob. Agents Chemother. 2009, 53, 2082–2088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monnet, D.L.; MacKenzie, F.M.; López-Lozano, J.M.; Beyaert, A.; Camacho, M.; Wilson, R.; Stuart, D.; Gould, I.M. Antimicrobial drug use and methicillin-resistant Staphylococcus aureus, Aberdeen, 1996–2000. Emerg. Infect. Dis. 2004, 10, 1432–1441. [Google Scholar] [CrossRef] [PubMed]
- Vernaz, N.; Sax, H.; Pittet, D.; Bonnabry, P.; Schrenzel, J.; Harbarth, S. Temporal effects of antibiotic use and hand rub consumption on the incidence of MRSA and Clostridium difficile. J. Antimicrob. Chemother. 2008, 62, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Kaier, K.; Hagist, C.; Frank, U.; Conrad, A.; Meyer, E. Two time-series analyses of the impact of antibiotic consumption and alcohol-based hand disinfection on the incidences of nosocomial methicillin-resistant Staphylococcus aureus infection and Clostridium difficile infection. Infect. Control Hosp. Epidemiol. 2009, 30, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Lawes, T.; Lopez-Lozano, J.M.; Nebot, C.A.; Macartney, G.; Subbarao-Sharma, R.; Dare, C.; Wares, K.D.; Gould, I.M. Effects of national antibiotic stewardship and infection control strategies on hospital-associated and community-associated meticillin-resistant Staphylococcus aureus infections across a region of Scotland: A non-linear time-series study. Lancet Infect. Dis. 2015, 15, 1438–1449. [Google Scholar] [CrossRef]
- Lawes, T.; Lopez-Lozano, J.M.; Nebot, C.; Macartney, G.; Subbarao-Sharma, R.; Dare, C.R.J.; Edwards, G.F.S.; Gould, I.M. Turning the tide or riding the waves? Impacts of antibiotic stewardship and infection control on MRSA strain dynamics in a Scottish region over 16 years: Non-linear time series analysis. BMJ Open 2015, 5, e006596. [Google Scholar] [CrossRef]
- Eliopoulos, G.M.; Shardell, M.; Harris, A.D.; El-Kamary, S.S.; Furuno, J.P.; Miller, R.R.; Perencevich, E.N. Statistical analysis and application of quasi experiments to antimicrobial resistance intervention studies. Clin. Infect. Dis. 2007, 45, 901–907. [Google Scholar] [CrossRef]
- Levy, S.B. Balancing the drug-resistance equation. Trends Microbiol. 1994, 2, 341–342. [Google Scholar] [CrossRef]
- Austin, D.J.; Kristinsson, K.G.; Anderson, R.M. The relationship between the volume of antimicrobial consumption in human communities and the frequency of resistance. Proc. Natl. Acad. Sci. USA 1999, 96, 1152–1156. [Google Scholar] [CrossRef]
- Al-Hashimy, Z.S.; Conway, B.R.; Al-Yaqoobi, M.; Khamis, F.; Al Mawali, G.Z.; Al Maashani, A.M.; Al Hadhrami, Y.S.; Al Alawi, S.S.; Al Mamari, M.S.; Lattyak, W.J.; et al. Identifying Targets for Antibiotic Use for the Management of Carbapenem-Resistant Acinetobacter baumannii (CRAb) in Hospitals-A Multi-Centre Nonlinear Time-Series Study. Antibiotics 2022, 11, 775. [Google Scholar] [CrossRef]
- Aldeyab, M.A.; Bond, S.E.; Conway, B.R.; Lee-Milner, J.; Sarma, J.B.; Lattyak, W.J. Identifying Antibiotic Use Targets for the Management of Antibiotic Resistance Using an Extended-Spectrum β-Lactamase-Producing Escherichia coli Case: A Threshold Logistic Modeling Approach. Antibiotics 2022, 11, 1116. [Google Scholar] [CrossRef] [PubMed]
- Aldeyab, M.A.; McElnay, J.C.; Scott, M.G.; Elhajji, F.W.D.; Kearney, M.P. Hospital antibiotic use and its relationship to age-adjusted comorbidity and alcohol-based hand rub consumption. Epidemiol. Infect. 2014, 142, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Aldeyab, M.A.; McElnay, J.C.; Scott, M.G.; Lattyak, W.J.; Elhajji, F.D.; Aldiab, M.A.; Magee, F.A.; Conlon, G.; Kearney, M.P. A modified method for measuring antibiotic use in healthcare settings: Implications for antibiotic stewardship and benchmarking. J. Antimicrob. Chemother. 2014, 69, 1132–1141. [Google Scholar] [CrossRef] [PubMed]
- WHO Collaborating Centre for Drug Statistics Methodology, Guidelines for ATC Classification and DDD Assignment, 2022. Oslo. 2021. Available online: https://www.whocc.no/filearchive/publications/2022_guidelines_web.pdf (accessed on 20 June 2022).
- Yusef, D.; Hayajneh, W.A.; Bond, S.E.; Lee-Milner, J.; Al-Azzam, S.; Issa, A.B.; Jaradat, S.K.; Gould, I.; Conway, B.R.; Hasan, S.S.; et al. Analysis of hospital antimicrobial consumption to identify targets for antimicrobial stewardship. Infect. Control Hosp. Epidemiol. 2022, 43, 943–945. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J. Multivariate adaptive regression splines. Ann. Stat. 1991, 19, 1–67. [Google Scholar] [CrossRef]
- Hastie, T.; Tibshirani, R. Generalized Additive Models; Chapman & Hall: London, UK, 1990. [Google Scholar]
- Liu, L.-M. Time Series Analysis and Forecasting, 2nd ed.; Scientific Computing Associates Corp.: River Forest, IL, USA, 2009. [Google Scholar]
- Neter, J.; Wasserman, W.; Kutner, M.H. Applied Linear Statistical Models, 3rd ed.; Irwin: New York, NY, USA, 1990. [Google Scholar]
- Cox, D.R. The regression analysis of binary sequences (with discussion). J. R. Stat. Soc. B 1958, 20, 215–242. [Google Scholar]
- Ricardo, A.; Maronna, R.; Martin, D.; Yohai, V.J. Robust Statistics: Theory and Methods. John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2006. [Google Scholar]
- Huber, P.J.; Ronchetti, E.M. Robust Statistics, 2nd ed.; Wiley: New York, NY, USA, 2009. [Google Scholar]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Schisterman, E.F.; Perkins, N.J.; Liu, A.; Bondell, H. Optimal cut-point and its corresponding Youden Index to discriminate individuals using pooled blood samples. Epidemiology 2005, 16, 73–81. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Predictor Variable | Lag | Median Use (IQR) | Threshold (95% Confidence Limit) * | Relation to Threshold | Coefficient (95% CI) | p-Value | Odds Ratio (95% CI) |
|---|---|---|---|---|---|---|---|
| Constant | NA | NA | NA | NA | −1.862 (−2.717 to 1.008) | <0.001 | 0.1553 (0.07 to 0.37) |
| Fluoroquinolones use (DDD/1000 OBD) | 3 | 64.55 (53.58–76.39) | 55.96 (37.37 to 75.15) | Above | 0.0486 (0.012 to 0.085) | 0.0099 | 1.0498 (1.01 to 1.09) |
| Co-amoxiclav use (DDD/1000 OBD) | 3 | 270.90 (247.3–297.0) | 312.19 (213.72 to 333.16) | Above | 0.0493 (0.010 to 0.089) | 0.0139 | 1.0505 (1.01 to 1.09) |
| Date | MRSA Rate Observed above 70th Percentile (0.276 Cases/1000 OBD) | Fluoroquinolones Use (DDD/1000 OBD) at Lag 3 (Threshold-Adjusted) | Co-Amoxiclav Use (DDD/1000 OBD) at Lag 3 (Threshold-Adjusted) | Predicted Probability MRSA above 70th Percentile | Coded Alert Signal |
|---|---|---|---|---|---|
| January | Above | 2.29 | 0.00 | 0.148 | Low |
| February | Below | 3.72 | 0.00 | 0.157 | Low |
| March | Below | 0.00 | 0.00 | 0.134 | Low |
| April | Below | 0.00 | 0.00 | 0.134 | Low |
| May | Below | 0.00 | 0.00 | 0.134 | Low |
| June | Below | 37.39 | 0.00 | 0.489 | High |
| July | Below | 12.88 | 0.00 | 0.225 | Medium |
| August | Below | 0.00 | 0.00 | 0.134 | Low |
| September | Below | 3.86 | 0.00 | 0.158 | Low |
| October | Below | 15.25 | 0.00 | 0.246 | Medium |
| November | Above | 0.00 | 0.00 | 0.134 | Low |
| December | Below | 1.13 | 0.00 | 0.141 | Low |
| MRSA Observed above or below 70th Percentile (0.276 Cases/1000 OBD)) | |||
|---|---|---|---|
| Above | Below | ||
| Coded Alert Signal | Low | 5 | 28 (5.6:1) |
| Medium | 6 | 15 | |
| High | 13 (1:1) | 13 | |
| Date | Fluoroquinolones Use (DDD/1000 OBD) at Lag 3 * | Co-Amoxiclav Use (DDD/1000 OBD) at Lag 3 * | Predicted Probability MRSA above 70th Percentile | Coded Alert Signal |
|---|---|---|---|---|
| January 2022 | 73.76 | 213.72 | 0.269 | Medium |
| February 2022 | 66.40 | 233.59 | 0.205 | Low |
| March 2022 | 75.15 | 273.90 | 0.283 | Medium |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aldeyab, M.A.; Bond, S.E.; Conway, B.R.; Lee-Milner, J.; Sarma, J.B.; Lattyak, W.J. A Threshold Logistic Modelling Approach for Identifying Thresholds between Antibiotic Use and Methicillin-Resistant Staphylococcus aureus Incidence Rates in Hospitals. Antibiotics 2022, 11, 1250. https://doi.org/10.3390/antibiotics11091250
Aldeyab MA, Bond SE, Conway BR, Lee-Milner J, Sarma JB, Lattyak WJ. A Threshold Logistic Modelling Approach for Identifying Thresholds between Antibiotic Use and Methicillin-Resistant Staphylococcus aureus Incidence Rates in Hospitals. Antibiotics. 2022; 11(9):1250. https://doi.org/10.3390/antibiotics11091250
Chicago/Turabian StyleAldeyab, Mamoon A., Stuart E. Bond, Barbara R. Conway, Jade Lee-Milner, Jayanta B. Sarma, and William J. Lattyak. 2022. "A Threshold Logistic Modelling Approach for Identifying Thresholds between Antibiotic Use and Methicillin-Resistant Staphylococcus aureus Incidence Rates in Hospitals" Antibiotics 11, no. 9: 1250. https://doi.org/10.3390/antibiotics11091250