
Impact of the COVID-19 Pandemic on Antibiotic Prescribing by Dentists in Galicia, Spain: A Quasi-Experimental Approach

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Antibiotic Prescribing by the WHO AWaRe Classification
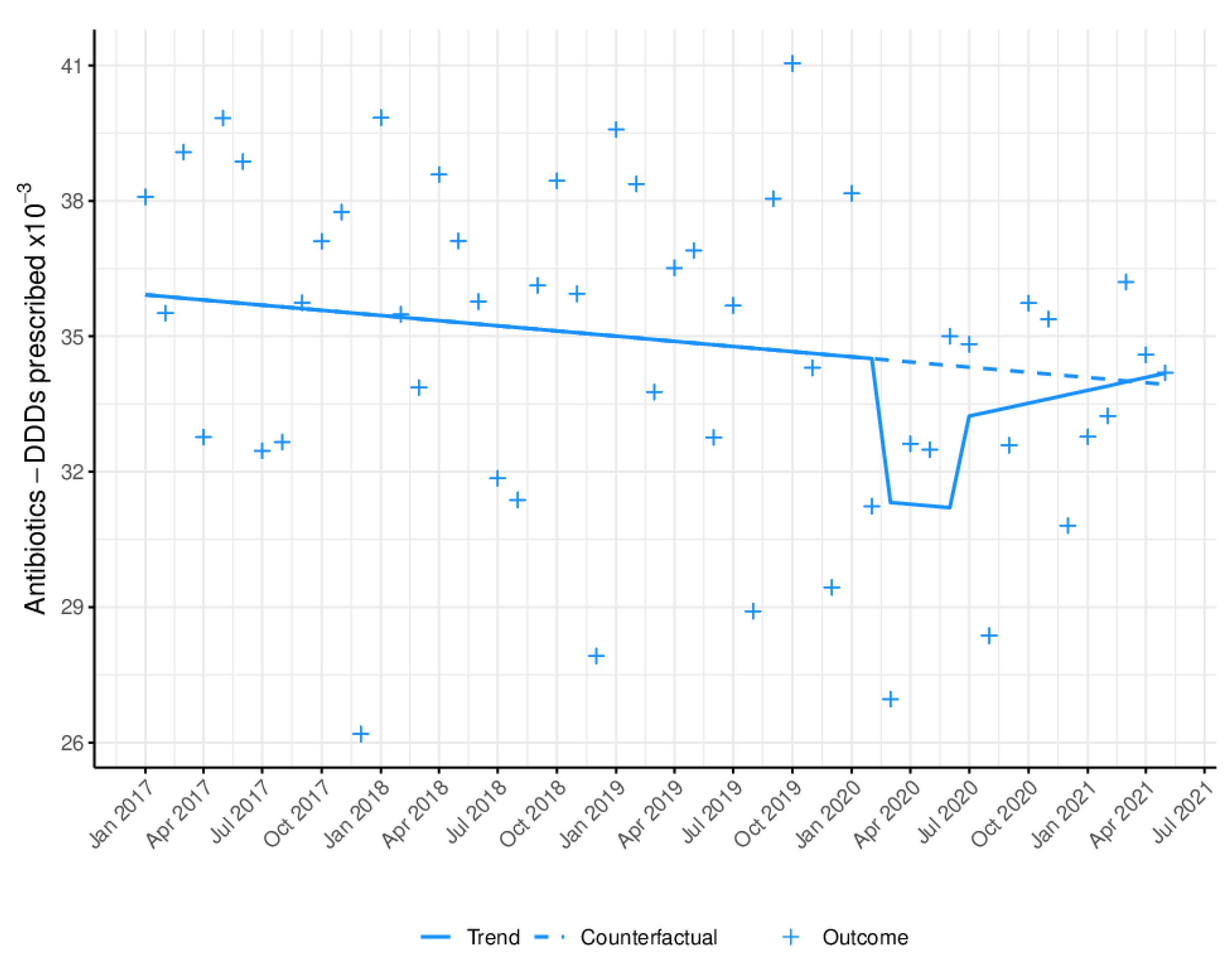
2.2. Impact of the COVID-19 Pandemic on Antibiotic Prescribing
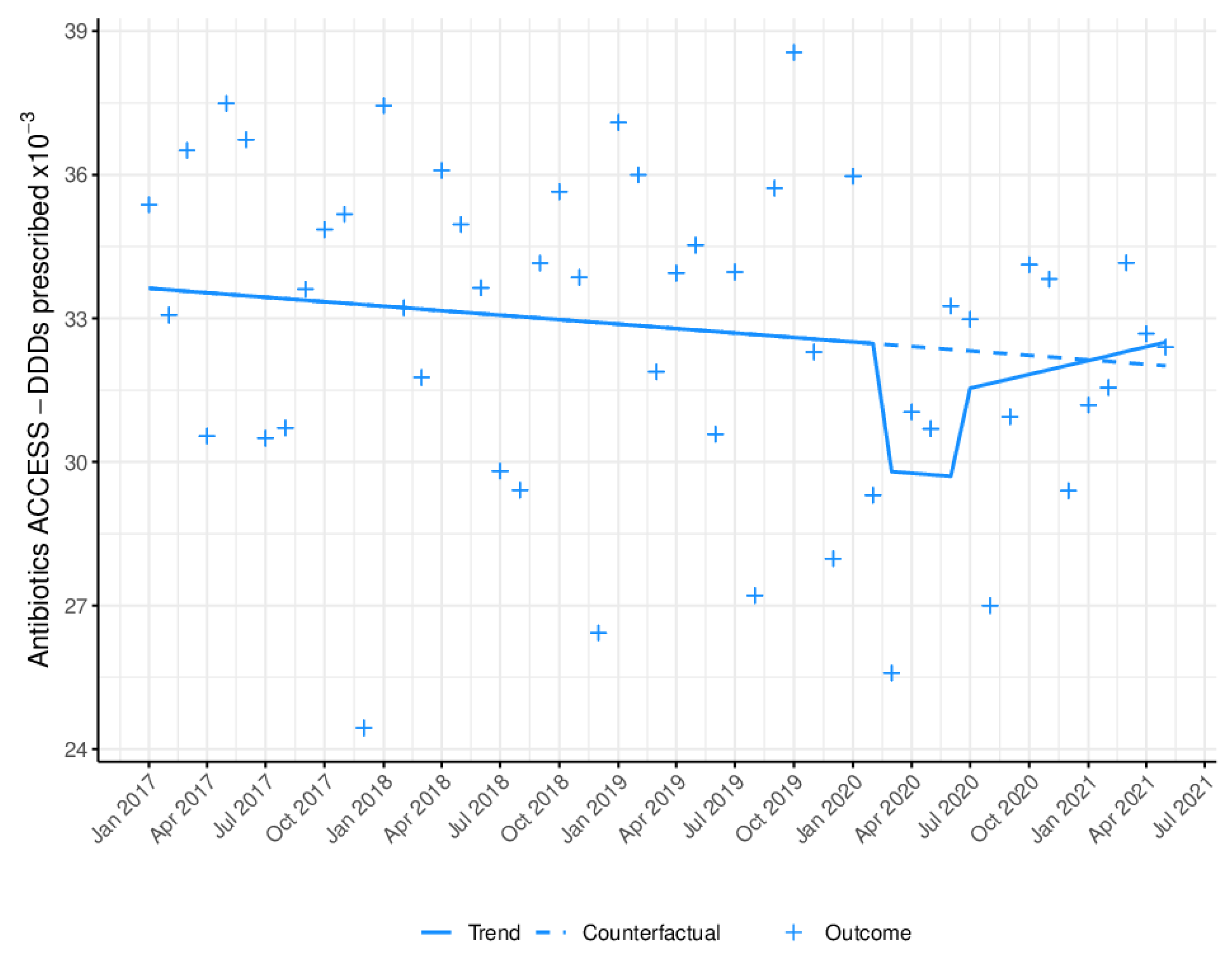
2.3. Impact of the COVID-19 Pandemic on the WHO Access Group
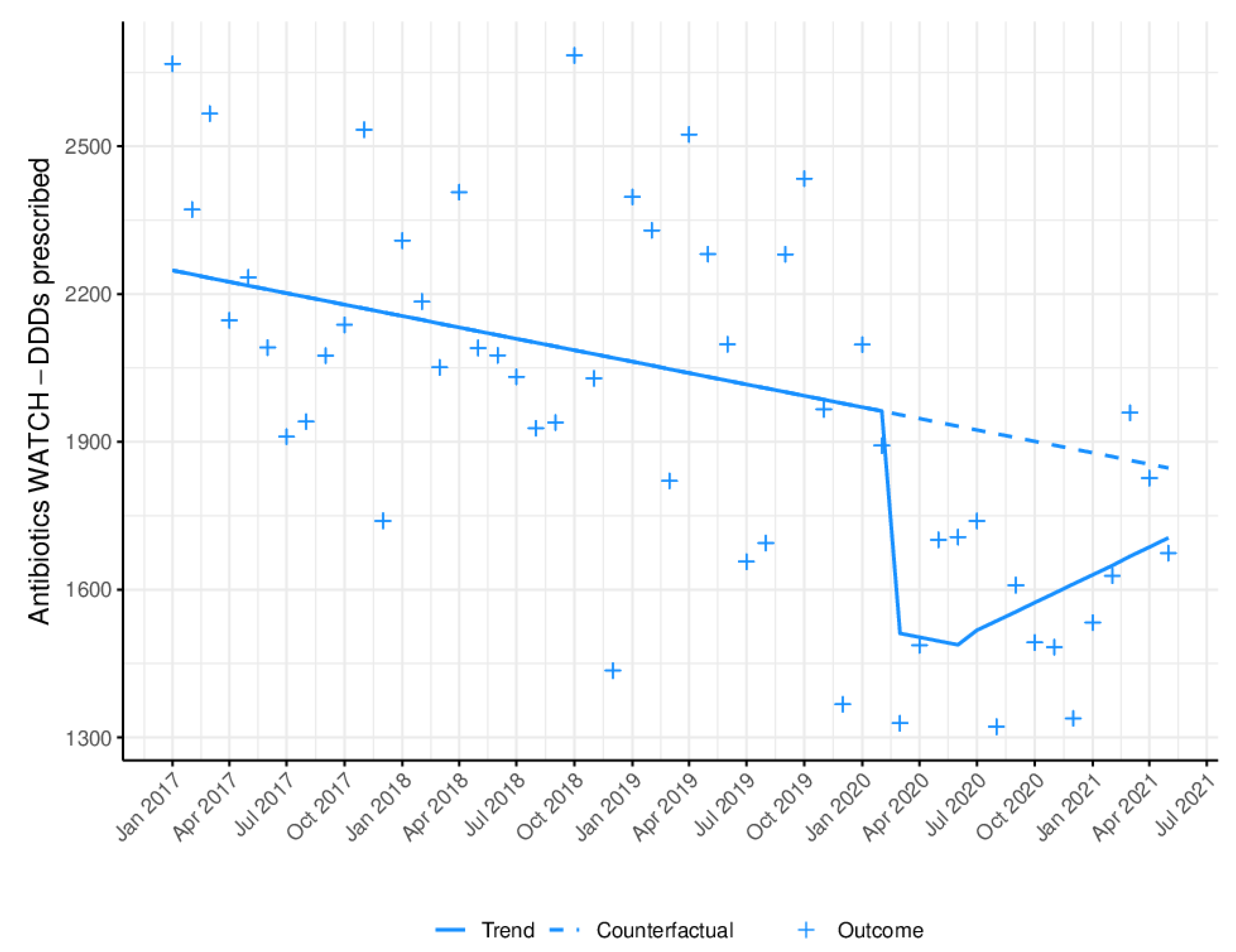
2.4. Impact of the COVID-19 Pandemic on the WHO Watch Group
3. Discussion
Strengths and Weaknesses of the Study
4. Materials and Methods
4.1. Settings
4.2. Study Design and Data Collection
4.3. Data Source
4.4. Definition of Variables
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization—WHO. Antibiotic Resistance. Available online: https://www.who.int/news-room/factsheets/detail/antimicrobial-resistance (accessed on 13 February 2022).
- Ferri, M.; Ranucci, E.; Romagnoli, P.; Giaccone, V. Antimicrobial resistance: A global emerging threat to public health systems. Crit. Rev. Food Sci. Nutr. 2017, 57, 2857–2876. [Google Scholar] [CrossRef] [PubMed]
- Bunce, J.T.; Hellyer, P. Antibiotic resistance and antibiotic prescribing by dentists in England 2007–2016. Br. Dent. J. 2018, 225, 81–84. [Google Scholar] [CrossRef]
- Marra, F.; George, D.; Chong, M.; Sutherland, S.; Patrick, D.M. Antibiotic prescribing by dentists has increased Why? J. Am. Dent. Assoc. 2016, 147, 320–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chate, R.A.C.; White, S.; Hale, L.R.; Howat, A.P.; Bottomley, J.; Barnet-Lamb, J.; Lindsay, J.; Davies, T.I.; Heath, J.M. The impact of clinical audit on antibiotic prescribing in general dental practice. Br. Dent. J. 2006, 201, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Chopra, R.; Merali, R.; Paolinelis, G.; Kwok, J. An audit of antimicrobial prescribing in an acute dental care department. Prim. Dent. J. 2014, 3, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Swift, J.Q.; Gulden, W.S. Antibiotic therapy--managing odontogenic infections. Dent. Clin. Am. 2002, 46, 623–633. [Google Scholar] [CrossRef]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus disease 2019 (COVID-19): Emerging and future challenges for dental and oral medicine. J. Dent Res. 2020, 99, 481–487. [Google Scholar] [CrossRef] [Green Version]
- Trullols-Casas, M.C.; Ausina-Márquez, V.; Martínez-Beneyto, Y. Recommendations by the Spanish Society of Epidemiology and Oral Public Health (SESPO) for the healthcare adaptation of public health dental clinics in Spain during the COVID-19 pandemic. J. Clin. Exp. Dent. 2020, 12, e1183–e1188. [Google Scholar] [CrossRef]
- Ather, A.; Patel, B.; Ruparel, N.B.; Diogenes, A.; Hargreaves, K.M. Coronavirus Disease 19 (COVID-19): Implications for clinical dental care. J. Endod. 2020, 46, 584–595. [Google Scholar] [CrossRef]
- Ather, A.; Patel, B.; Ruparel, N.B.; Diogenes, A.; Hargreaves, K.M. Perceived vulnerability to Coronavirus infection: Impact on dental practice. Braz. Oral Res. 2020, 34, 584–595. [Google Scholar]
- Estai, M.; Bunt, S.; Kanagasingam, Y.; Kruger, E.; Tennant, M. Diagnostic accuracy of teledentistry in the detection of dental caries: A systematic review. J. Evid. Based Dent. Pract. 2016, 16, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Campus, G.; Betancourt, M.D.; Cagetti, M.; Giacaman, R.; Manton, D.; Douglas, G.; Carvalho, T.; Carvalho, J.; Vukovic, A.; Cortés-Martinicorena, F.; et al. The COVID-19 pandemic and its global effects on dental practice. An International survey. J. Dent. 2021, 114, 103749. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization-WHO—Home AWaRe. Available online: https://adoptaware.org/ (accessed on 13 February 2022).
- Posse, J.L.; Álvarez-Fernández, M.; Feijoo, J.F.; Henríquez, J.M.; Lockhart, P.B.; Chu, V.H.; Dios, P.D. Intravenous amoxicillin/clavulanate for the prevention of bacteraemia following dental procedures: A randomized clinical trial. J. Antimicrob. Chemother. 2016, 71, 2022–2030. [Google Scholar] [CrossRef] [PubMed]
- Lafaurie, G.I.; Noriega, L.A.; Torres, C.C.; Castillo, Y.; Moscoso, S.B.; Mosquera, S.; Díaz-Báez, D.; Chambrone, L. Impact of antibiotic prophylaxis on the incidence, nature, magnitude, and duration of bacteremia associated with dental procedures: A systematic review. J. Am. Dent. Assoc. 2019, 150, 948–959.e4. [Google Scholar] [CrossRef] [PubMed]
- Diz Dios, P.; Tomás Carmona, I.; Limeres Posse, J.; Medina Henríquez, J.; Fernández Feijoo, J.; Alvarez Fernández, M. Comparative efficacies of amoxicillin, clindamycin, and moxifloxacin in prevention of bacteremia following dental extractions. Antimicrob. Agents Chemother. 2006, 50, 2996–3002. [Google Scholar] [CrossRef] [Green Version]
- González-Olmo, M.J.; Delgado-Ramos, B.; Ortega-Martínez, A.R.; Romero-Maroto, M.; Carrillo-Díaz, M. Fear of COVID-19 in Madrid. Will patients avoid dental care? Int. Dent. J. 2021, 72, 76–82. [Google Scholar] [CrossRef]
- Salgarello, S.; Salvadori, M.; Mazzoleni, F.; Salvalai, V.; Francinelli, J.; Bertoletti, P.; Lorenzi, D.; Audino, E.; Garo, M.L. Urgent Dental Care During Italian Lockdown: A Cross-sectional Survey. J. Endod. 2021, 47, 204–214. [Google Scholar] [CrossRef]
- Ramírez, J.M.; Varela-Montes, L.; Gómez-Costa, D.; Giovannini, G.; Romero-Maroto, M.; Gómez de Diego, R. Management of odonto-stomatological emergencies during the COVID-19 alarm state in dental clinics in the Autonomous Community of Madrid (CAM), Spain: An observational study. Med. Oral Patol. Oral Cir. Bucal 2021, 26, e114–e117. [Google Scholar] [CrossRef] [PubMed]
- Mian, M.; Teoh, L.; Hopcraft, M. Trends in dental medication prescribing in australia during the COVID-19 pandemic. JDR Clin. Trans. Res. 2021, 6, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Wordley, V.; Thompson, W. How did COVID-19 impact on dental antibiotic prescribing across England? Br. Dent. J. 2020, 229, 601–604. [Google Scholar] [CrossRef]
- Duncan, E.M.; Goulao, B.; Clarkson, J.; Young, L.; Ramsay, C.R. “You had to do something”: Prescribing antibiotics in Scotland during the COVID-19 pandemic restrictions and remobilisation. Br. Dent. J. 2021, 23, 1–6. [Google Scholar] [CrossRef]
- Thornhill, M.H.; Dayer, M.; Lockhart, P.B.; McGurk, M.; Shanson, D.; Prendergast, B.; Chambers, J.B. Guidelines on prophylaxis to prevent infective endocarditis. Br. Dent. J. 2016, 220, 51–56. [Google Scholar] [CrossRef] [Green Version]
- Centre for Clinical Practice at NICE (UK). Prophylaxis against Infective Endocarditis Antimicrobial Prophylaxis against Infective Endocarditis in Adults and Children; National Institute for Health and Clinical Excellence: London, UK, 2008. [Google Scholar]
- Palmer, N.O.A.; Seoudi, N. The effect of SARS-CoV-2 on the prescribing of antimicrobials and analgesics by NHS general dental practitioners in England. Br. Dent. J. 2021, 21, 1–6. [Google Scholar] [CrossRef]
- Sari, A.; Bilmez, Z.Y. Effects of Coronavirus (COVID-19) Fear on Oral Health Status. Oral Health Prev. Dent. 2021, 19, 411–423. [Google Scholar]
- Samuel, S.R.; Kuduruthullah, S.; Khair, A.M.B.; Al Shayeb, M.; Elkaseh, A.; Varma, S.R.; Nadeem, G.; Elkhader, I.A.; Ashekhi, A. Impact of pain, psychological-distress, SARS-CoV2 fear on adults’ OHRQOL during COVID-19 pandemic. Saudi J. Biol. Sci. 2021, 28, 492–494. [Google Scholar] [CrossRef]
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental caries. Nat. Rev. Dis. Primers 2017, 25, 17030. [Google Scholar] [CrossRef] [Green Version]
- Lai, A.G.; Pasea, L.; Banerjee, A.; Hall, G.; Denaxas, S.; Chang, W.H.; Katsoulis, M.; Williams, B.; Pillay, D.; Noursadeghi, M.; et al. Estimated impact of the COVID-19 pandemic on cancer services and excess 1-year mortality in people with cancer and multimorbidity: Near real-time data on cancer care, cancer deaths and a population-based cohort study. BMJ Open 2020, 10, e043828. [Google Scholar] [CrossRef]
- Seidu, S.; Kunutsor, S.K.; Cos, X.; Khunti, K. Indirect impact of the COVID-19 pandemic on hospitalisations for cardiometabolic conditions and their management: A systematic review. Prim. Care Diabetes 2021, 15, 653–681. [Google Scholar] [CrossRef]
- Fisher, L.; Polonsky, W.; Asuni, A.; Jolly, Y.; Hessler, D. The early impact of the COVID-19 pandemic on adults with type 1 or type 2 diabetes: A national cohort study. J. Diabetes Complicat. 2020, 34, 107748. [Google Scholar] [CrossRef]
- Smith, A.; Al-Mahdi, R.; Malcolm, W.; Palmer, N.; Dahlen, G.; Al-Haroni, M. Comparison of antimicrobial prescribing for dental and oral infections in England and Scotland with Norway and Sweden and their relative contribution to national consumption 2010–2016. BMC Oral Health 2020, 20, 172. [Google Scholar] [CrossRef] [PubMed]
- Agencia Española de Medicamentos y Productos Sanitarios (AEMPS). Plan. Nacional Frente a La Resistencia a Los Antibióticos 2019–2021. 2019. Available online: https://www.resistenciaantibioticos.es/es/publicaciones/plan-nacional-frente-la-resistencia-los-antibioticos-pran-2019-2021 (accessed on 11 February 2022).
- Park, J.S.; Page, A.T.; Kruger, E.; Tennant, M. Dispensing patterns of medicines prescribed by australian dentists from 2006 to 2018—A Pharmacoepidemiological Study. Int. Dent. J. 2021, 71, 106–112. [Google Scholar] [CrossRef]
- Halling, F.; Neff, A.; Heymann, P.; Ziebart, T. Trends in antibiotic prescribing by dental practitioners in Germany. J. Craniomaxillofac. Surg. 2017, 45, 1854–1859. [Google Scholar] [CrossRef] [PubMed]
- Struyf, T.; Vandael, E.; Leroy, R.; Mertens, K.; Catry, B. Antimicrobial prescribing by Belgian dentists in ambulatory care, from 2010 to 2016. Int. Dent. J. 2019, 69, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Urrusuno, R.; Grupo de Trabajo de la Guía. Guía de Terapéutica Antimicrobiana Del Área Aljarafe 3a Edición; Distrito Sanitario Aljarafe-Sevilla Norte y Hospital San Juan de Dios del Aljarafe: Sevilla, Spain, 2018. [Google Scholar]
- Scottish Dental Clinical Effectiveness Programme. Drug Prescribing for Dentistry. Dental Clinical Guidelines, 3rd ed.; The Royal Pharmaceutical Society of Great Britain and the BMJ Publishing Group Ltd.: Dundee, UK, 2016. [Google Scholar]
- Segura-Egea, J.J.; Gould, K.; Şen, B.H.; Jonasson, P.; Cotti, E.; Mazzoni, A.; Sunay, H.; Tjäderhane, L.; Dummer, P.M.H. European Society of Endodontology position statement: The use of antibiotics in endodontics. Int. Endod. J. 2018, 51, 20–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, W.R.; Gewitz, M.; Lockhart, P.B.; Bolger, A.F.; DeSimone, D.C.; Kazi, D.S.; Couper, D.J.; Beaton, A.; Kilmartin, C.; Miro, J.M.; et al. Prevention of viridans group streptococcal infective endocarditis: A scientific statement from the american heart association. Circulation 2021, 143, E963–E978. [Google Scholar] [CrossRef]
- Thornhill, M.; Dayer, M.; Durkin, M.; Lockhart, P.; Baddour, L. Risk of Adverse Reactions to Oral Antibiotics Prescribed by Dentists. J. Dent. Res. 2019, 98, 1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, T.M.; Estrela, M.; Gomes, E.R.; Piñeiro-Lamas, M.; Figueiras, A.; Roque, F.; Herdeiro, M.T. The impact of the COVID-19 pandemic on antibiotic prescribing trends in outpatient care: A nationwide, quasi-experimental approach. Antibiotics 2021, 25, 1040. [Google Scholar] [CrossRef]
- Bernal, J.L.; Cummins, S.; Gasparrini, A. Interrupted time series regression for the evaluation of public health interventions: A tutorial. Int. J. Epidemiol. 2017, 46, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Servizo Galego de Saude. SERGAS. Memoria de Actividade Sergas. 2018. Available online: https://www.sergas.es/A-nosa-organizacion/Documents/832/MemoriaActividade2018.pdf (accessed on 13 February 2022).
- Sruamsiri, R.; Wagner, A.K.; Ross-Degnan, D.; Lu, C.Y.; Dhippayom, T.; Ngorsuraches, S.; Chaiyakunapruk, N. Expanding access to high-cost medicines through the E2 access program in Thailand: Effects on utilisation, health outcomes and cost using an interrupted time-series análisis. BMJ Open 2016, 6, e008671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, A.K.; Soumerai, S.B.; Zhang, F.; Ross-Degnan, D. Segmented regression analysis of interrupted time series studies in medication use research. J. Clin. Pharm. Ther. 2002, 27, 299–309. [Google Scholar] [CrossRef]
- Kontopantelis, E.; Doran, T.; Springate, D.A.; Buchan, I.; Reeves, D. Regression based quasi-experimental approach when randomisation is not an option: Interrupted time series analysis. BMJ 2015, 350, h2750. [Google Scholar] [CrossRef] [Green Version]
- WHOCC—ATC/DDD—Collaborating Centre for Drug Statistics Methodology, ATC Classification Index with DDDs. Available online: https://www.whocc.no/atc_ddd_index_and_guidelines/atc_ddd_index/ (accessed on 14 February 2022).
- WHOCC—Collaborating Centre for Drug Statistics Methodology. Definition and General Considerations for DDD Assignment. Available online: https://www.whocc.no/ddd/defi (accessed on 14 February 2022).
- Rodrigues, A.T.; Roque, F.; Piñeiro-Lamas, M.; Falcão, A.; Figueiras, A.; Herdeiro, M.T. Effectiveness of an intervention to improve antibiotic-prescribing behaviour in primary care: A controlled, interrupted time-series study. J. Antimicrob. Chemother. 2019, 74, 2788–2796. [Google Scholar] [CrossRef] [PubMed]
- Vázquez-Mourelle, R.; Carracedo-Martínez, E.; Figueiras, A. Impact of a change of bronchodilator medications in a hospital drug formulary on intra-and out-of-hospital drug prescriptions: Interrupted time series design with comparison group. Implement Sci. 2020, 15, 33. [Google Scholar] [CrossRef] [PubMed]
- Sax, C.; Eddelbuettel, D. Seasonal Adjustment by X-13ARIMA-SEATS in R. J. Stat. Softw. 2018, 87, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.; Wagner, A.K.; Soumerai, S.B.; Ross-Degnan, D. Methods for estimating confidence intervals in interrupted time series analyses of health interventions. J. Clin. Epidemiol. 2009, 62, 143–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R: The R Foundation. Available online: https://www.r-project.org/foundation/ (accessed on 13 February 2022).
- StataCorp. Stata Statistical Software: Release 12; StataCorp LP: College Station, TX, USA, 2011. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Pre-Lockdown | Lockdown | Post-Lockdown | |
|---|---|---|---|
| (DDD) | (DDD) | (DDD) | |
| Total Antibiotics | |||
| Mean (SD) | 3,5344.73 (3606.63) | 3,1767.37 (3406.07) | 3,3517.72 (2329.37) |
| Median | 35,856.17 | 32,554.32 | 34,190.74 |
| PCT25, PCT75 | 3,2734.07, 3,8218.76 | 2,8342.59, 3,4405.20 | 3,2584.43, 3,5381.73 |
| Access Antibiotics | |||
| Mean (SD) | 3,3170.23 (3360.40) | 3,0147.09 (3243.56) | 3,1839.90 (2181.16) |
| Median | 33,900.87 | 30,869.28 | 32,398.21 |
| PCT25, PCT75 | 3,0569.86, 3,5783.69 | 2,6866.07, 3,2705.93 | 3,0942.64, 3,3819.73 |
| Watch Antibiotics | |||
| Mean (SD) | 2116.26 (309.18) | 1555.75 (182.75) | 1600.35 (195.29) |
| Median | 2094.33 | 1594.00 | 1609.00 |
| PCT25, PCT75 | 1936.13, 2340.00 | 1368.13, 1705.13 | 1483.00, 1739.17 |
| Antibiotic Prescribing (DDD) | |||
|---|---|---|---|
| Overall | Access | Watch | |
| Per Month Trend in Pre-Lockdown Period | |||
| B | −42.39 | −35.09 | −7.41 |
| 95%CI | −96.47; 11.69 | −87.35; 17.16 | −13.52; −1.30 |
| p-value | 0.1214 | 0.183 | 0.0187 |
| Effect of Lockdown (1) | |||
| B | −3572.73 | −2976.5 | −651.02 |
| 95%CI | −6018.90; −1126.57 | −5304.34; −648.65 | −891.02; −411.01 |
| p-value | 0.0051 | 0.0133 | <0.0001 |
| Post-Lockdown Change (1) | |||
| B | −1363.82 | −991.28 | −688.91 |
| 95%CI | −4001.04; 1273.40 | −3537.90; 1555.34 | −1029.54; −348.28 |
| p-value | 0.3033 | 0.4373 | 0.0002 |
| Change Per Month in Trend in Post-Lockdown Period (2) | |||
| B | 142.74 | 136.05 | 29.15 |
| 95%CI | −193.39; 478.86 | −190.25; 462.35 | −2.28; 60.58 |
| p-value | 0.3971 | 0.4057 | 0.0682 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Fernández, A.; Vázquez-Cancela, O.; Piñeiro-Lamas, M.; Figueiras, A.; Zapata-Cachafeiro, M. Impact of the COVID-19 Pandemic on Antibiotic Prescribing by Dentists in Galicia, Spain: A Quasi-Experimental Approach. Antibiotics 2022, 11, 1018. https://doi.org/10.3390/antibiotics11081018
Rodríguez-Fernández A, Vázquez-Cancela O, Piñeiro-Lamas M, Figueiras A, Zapata-Cachafeiro M. Impact of the COVID-19 Pandemic on Antibiotic Prescribing by Dentists in Galicia, Spain: A Quasi-Experimental Approach. Antibiotics. 2022; 11(8):1018. https://doi.org/10.3390/antibiotics11081018
Chicago/Turabian StyleRodríguez-Fernández, Almudena, Olalla Vázquez-Cancela, María Piñeiro-Lamas, Adolfo Figueiras, and Maruxa Zapata-Cachafeiro. 2022. "Impact of the COVID-19 Pandemic on Antibiotic Prescribing by Dentists in Galicia, Spain: A Quasi-Experimental Approach" Antibiotics 11, no. 8: 1018. https://doi.org/10.3390/antibiotics11081018