
Impact of the COVID-19 Outbreak on the Antibiotic Use Patterns among a Rural Community Population in Eastern China
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Characteristics of Participants
2.2. Changes in the Risk of Antibiotic Use between 2019 and 2020
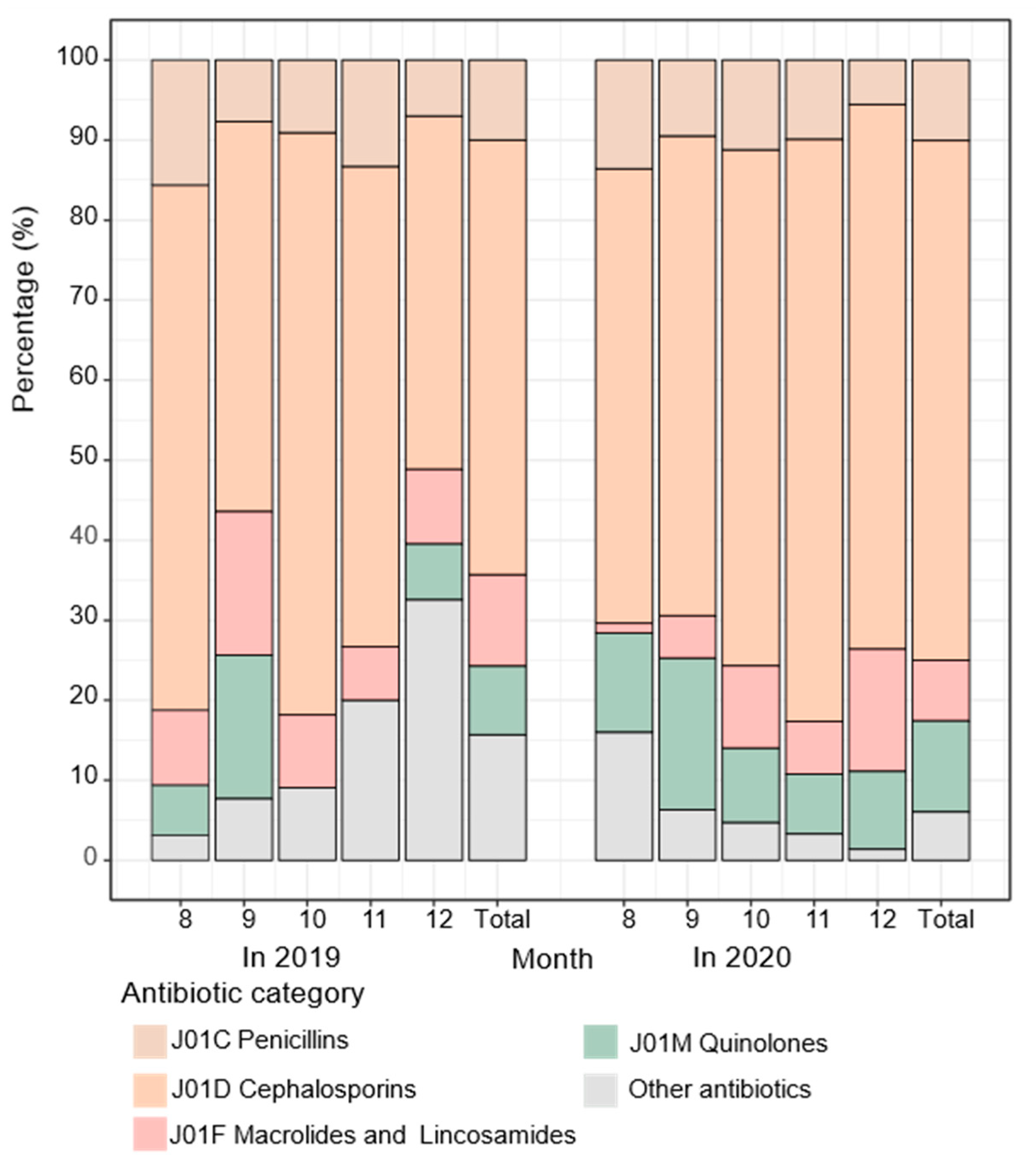
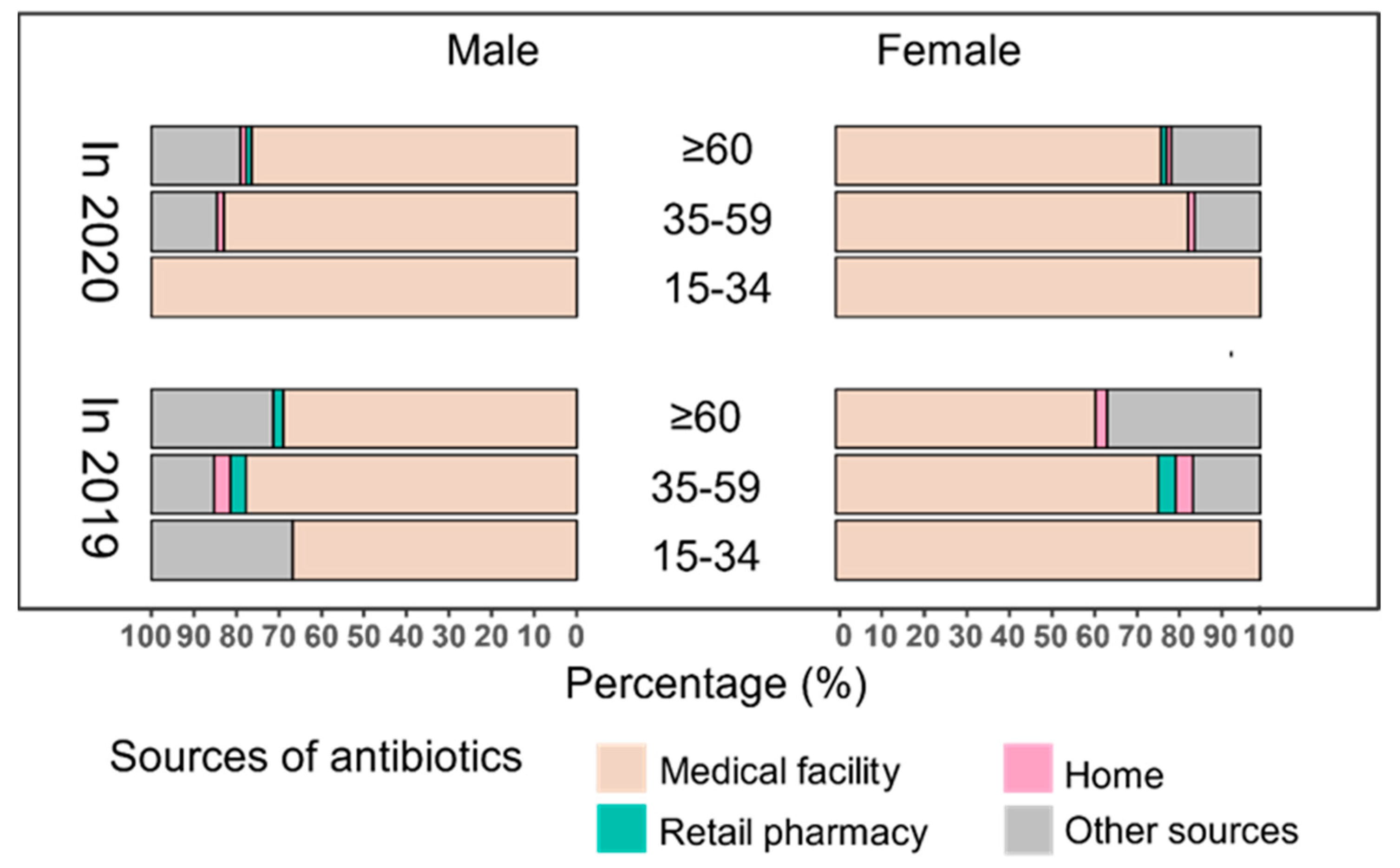
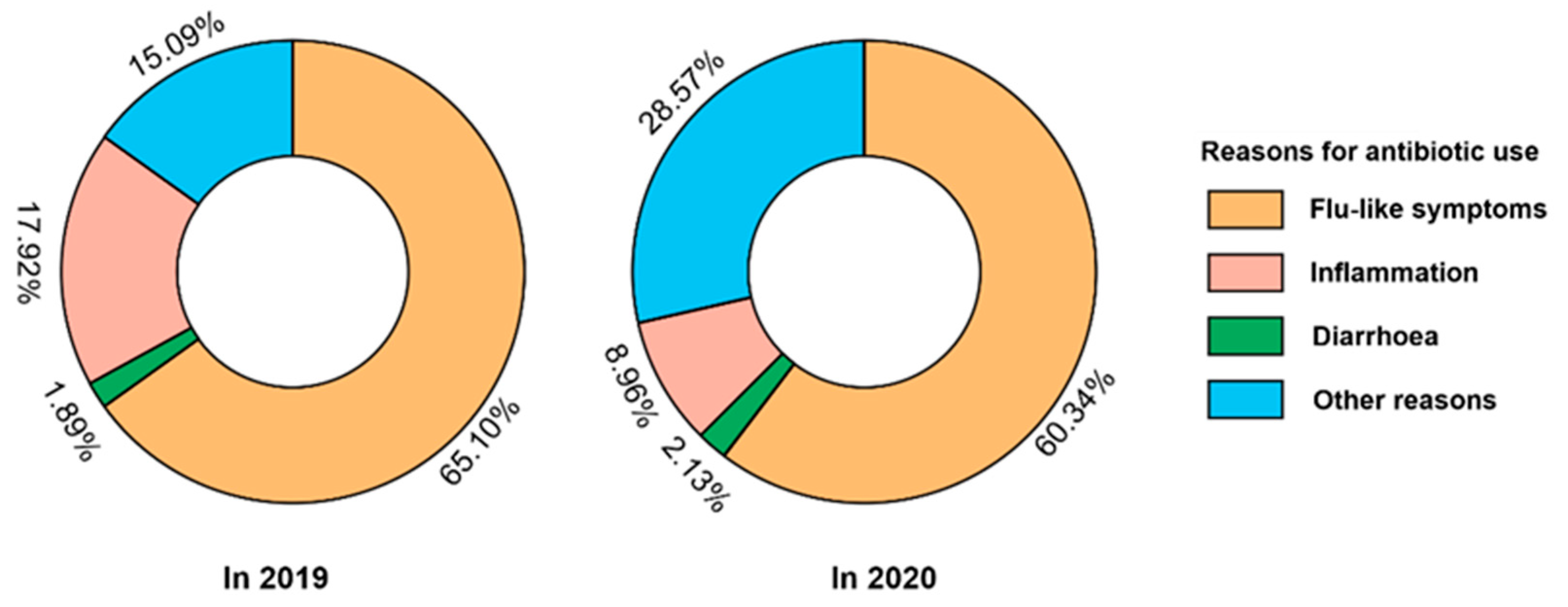
2.3. Changes in Antibiotic Categories and Access
3. Discussion
3.1. Summary
3.2. The Potential Reasons Why the Risk of Antibiotics Increased after the COVID-19 Outbreak
3.3. A More Pronounced Impact Occurred in Some Groups
3.4. Categories and Access of Antibiotic Use Changed Moderately
3.5. Strengths and Limitations
4. Materials and Methods
4.1. Study Design and Population
- (1)
- Study design: This study was from research carried out in a rural community in Eastern China in June 2019, as presented in our previous paper [66]. Data collected from August to December 2019 was the “prior” period of the COVID-19 outbreak in China, and those during the same five months in 2020 were the “post” period, during which no local cases of COVID-19 infection were reported in Deqing County.
- (2)
- Sampling method: Based on the population cohort previously established in Deqing County of the Zhejiang province in China, one village was selected as the study site using the rapid cluster sample survey methodology [67], and a total of 1112 residents were recruited into this study (441 in 2019 and 671 in 2020). One individual had missing data for most variables in 2019 and was therefore excluded. Finally, 1111 participants were eligible for the final analysis (440 in 2019 and 671 in 2020).
- (3)
- Sample size estimation: According to a study in the United States, the antimicrobial use prevalence was 8.2% [68]; we conservatively expected that the prevalence was 9.0% among this study population. A two-sided test was used with the following parameters: set α = 0.05, δ = 2.0%. Then the values were inputted into the following formula:Considering the non-response variable and increasing the sample size by 10%, the minimum sample size was estimated to be 440.
- (4)
- The inclusion criteria were as follows: (1) aged 15 years old and over, (2) lived in the study sites for no less than six months, and (3) consented to inclusion in the study.
- (5)
- Ethical statement: All participants read a consent form (including the study objectives, risks, and benefits for the participants, the confidentiality, and that participation was voluntary) and received clarification if requested before giving their oral consent to participate in the study. This study was reviewed and approved by the Institutional Review Board of the School of Public Health, Fudan University, China (number IRB#2019-03-0733).
4.2. Collections for General Information and Antibiotic Use
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Seethalakshmi, P.S.; Charity, O.J.; Giakoumis, T.; Kiran, G.S.; Sriskandan, S.; Voulvoulis, N.; Selvin, J. Delineating the impact of COVID-19 on antimicrobial resistance: An Indian perspective. Sci. Total Environ. 2022, 818, 151702. [Google Scholar] [CrossRef] [PubMed]
- Cars, H.; Hakansson, A. To prescribe—Or not to prescribe—Antibiotics. District physicians’ habits vary greatly, and are difficult to change. Scand. J. Prim. Health Care 1995, 13, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Stocker, M.; Ferrao, E.; Banya, W.; Cheong, J.; Macrae, D.; Furck, A. Antibiotic surveillance on a paediatric intensive care unit: Easy attainable strategy at low costs and resources. BMC Pediatr. 2012, 12, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Department of Health and Human Services. Antibiotic Resistance Threats in the United States 2013; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2013; pp. 1–113.
- O’Neill, J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations; Government of the United Kingdom: London, UK, 2016. [Google Scholar]
- World Health Organization. WHO Coronavirus (COVID-19) Ashboard. Available online: https://covid19.who.int/ (accessed on 23 June 2022).
- Beovic, B.; Dousak, M.; Ferreira-Coimbra, J.; Nadrah, K.; Rubulotta, F.; Belliato, M.; Berger-Estilita, J.; Ayoade, F.; Rello, J.; Erdem, H. Antibiotic use in patients with COVID-19: A ‘snapshot’ Infectious Diseases International Research Initiative (ID-IRI) survey. J. Antimicrob. Chemother. 2020, 75, 3386–3390. [Google Scholar] [CrossRef]
- Verroken, A.; Scohy, A.; Gérard, L.; Wittebole, X.; Collienne, C.; Laterre, P.-F. Co-infections in COVID-19 critically ill and antibiotic management: A prospective cohort analysis. Crit. Care 2020, 24, 1–3. [Google Scholar] [CrossRef]
- Nestler, M.J.; Godbout, E.; Lee, K.; Kim, J.; Noda, A.J.; Taylor, P.; Pryor, R.; Markley, J.D.; Doll, M.; Bearman, G.; et al. Impact of COVID-19 on pneumonia-focused antibiotic use at an academic medical center. Infect. Control. Hosp. Epidemiol. 2021, 42, 915–916. [Google Scholar] [CrossRef]
- Clancy, C.J.; Nguyen, M.H. Coronavirus disease 2019, superinfections, and antimicrobial development: What can we expect? Clin. Infect. Dis. 2020, 71, 2736–2743. [Google Scholar] [CrossRef]
- Huttner, B.; Catho, G.; Pano-Pardo, J.; Pulcini, C.; Schouten, J. COVID-19: Don’t neglect antimicrobial stewardship principles! Clin. Microbiol. Infect. 2020, 26, 808–810. [Google Scholar] [CrossRef]
- Cong, W.; Poudel, A.N.; Alhusein, N.; Wang, H.; Yao, G.; Lambert, H. Antimicrobial Use in COVID-19 Patients in the First Phase of the SARS-CoV-2 Pandemic: A Scoping Review. Antibiotics 2021, 10, 745. [Google Scholar] [CrossRef]
- Cong, W.; Stuart, B.; AIhusein, N.; Liu, B.; Tang, Y.; Wang, H.; Wang, Y.; Manchundiya, A.; Lambert, H. Antibiotic Use and Bacterial Infection in COVID-19 Patients in the Second Phase of the SARS-CoV-2 Pandemic: A Scoping Review. Antibiotics 2022, 11, 991. [Google Scholar] [CrossRef]
- Nature Microbiology. Antimicrobial resistance in the age of COVID-19. Nat. Microbiol. 2020, 5, 779. [Google Scholar] [CrossRef] [PubMed]
- Gagliotti, C.; Buttazzi, R.; Ricchizzi, E.; Di Mario, S.; Tedeschi, S.; Moro, M.L. Community use of antibiotics during the COVID-19 lockdown. Infect. Dis. 2020, 53, 142–144. [Google Scholar] [CrossRef] [PubMed]
- Butler, C.C.; Dorward, J.; Yu, L.-M.; Gbinigie, O.; Hayward, G.; Saville, B.R.; Van Hecke, O.; Berry, N.; Detry, M.; Saunders, C.; et al. Azithromycin for community treatment of suspected COVID-19 in people at increased risk of an adverse clinical course in the UK (PRINCIPLE): A randomised, controlled, open-label, adaptive platform trial. Lancet 2021, 397, 1063–1074. [Google Scholar] [CrossRef]
- Condes, E.; Arribas, J.R.; COVID-19 Madrid-S.P.P.M. Group. Impact of COVID-19 on Madrid hospital system. Enferm. Infecc. Microbiol. Clin. 2021, 39, 256–257. [Google Scholar] [CrossRef] [PubMed]
- Subramanya, S.H.; Czyż, D.M.; Acharya, K.P.; Humphreys, H. The potential impact of the COVID-19 pandemic on antimicrobial resistance and antibiotic stewardship. Virusdisease 2021, 32, 330–337. [Google Scholar] [CrossRef]
- Tartari, E.; Hopman, J.; Allegranzi, B.; Gao, B.; Widmer, A.; Cheng, V.C.-C.; Wong, S.C.; Marimuthu, K.; Ogunsola, F.; Voss, A. Perceived challenges of COVID-19 infection prevention and control preparedness: A multinational survey. J. Glob. Antimicrob. Resist. 2020, 22, 779–781. [Google Scholar] [CrossRef] [PubMed]
- Zhu, N.; Aylin, P.; Rawson, T.; Gilchrist, M.; Majeed, A.; Holmes, A. Investigating the impact of COVID-19 on primary care antibiotic prescribing in North West London across two epidemic waves. Clin. Microbiol. Infect. 2021, 27, 762–768. [Google Scholar] [CrossRef]
- Monnet, D.L.; Harbarth, S. Will coronavirus disease (COVID-19) have an impact on antimicrobial resistance? Eurosurveillance 2020, 25, 2001886. [Google Scholar] [CrossRef]
- Knight, G.M.; E Glover, R.; McQuaid, C.F.; Olaru, I.D.; Gallandat, K.; Leclerc, Q.J.; Fuller, N.M.; Willcocks, S.J.; Hasan, R.; van Kleef, E.; et al. Antimicrobial resistance and COVID-19: Intersections and implications. Elife 2021, 10, e64139. [Google Scholar] [CrossRef]
- O’Neill, J. Review on Antimicrobial Resistance: Tackling a Global Health Crisis; AMR Review: London, UK, 2015. [Google Scholar]
- Founou, L.L.; Founou, R.C.; Essack, S.Y. Antibiotic Resistance in the Food Chain: A Developing Country-Perspective. Front. Microbiol. 2016, 7, 1881. [Google Scholar] [CrossRef]
- Davey, P.; Pagliari, C.; Hayes, A. The patient’s role in the spread and control of bacterial resistance to antibiotics. Clin. Microbiol. Infect. 2002, 8, 43–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawkings, N.J.; Butler, C.C.; Wood, F. Antibiotics in the community: A typology of user behaviours. Patient Educ. Couns. 2008, 73, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Beyene, K.A.; Sheridan, J.; Aspden, T. Prescription Medication Sharing: A Systematic Review of the Literature. Am. J. Public Health 2014, 104, e15–e26. [Google Scholar] [CrossRef] [PubMed]
- Okeke, I.N.; Lamikanra, A.; Edelman, R. Socioeconomic and behavioral factors leading to acquired bacterial resistance to antibiotics in developing countries. Emerg. Infect. Dis. 1999, 5, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, I.; Rabbi, M.B.; Sultana, S. Antibiotic resistance in Bangladesh: A systematic review. Int. J. Infect. Dis. 2019, 80, 54–61. [Google Scholar] [CrossRef] [Green Version]
- Hoque, R.; Ahmed, S.M.; Naher, N.; Islam, M.A.; Rousham, E.K.; Islam, B.Z.; Hassan, S. Tackling antimicrobial resistance in Bangladesh: A scoping review of policy and practice in human, animal and environment sectors. PLoS ONE 2020, 15, e0227947. [Google Scholar] [CrossRef] [Green Version]
- Aslam, A.; Gajdács, M.; Zin, C.S.; Ab Rahman, N.S.; Ahmed, S.I.; Zafar, M.Z.; Jamshed, S. Evidence of the Practice of Self-Medication with Antibiotics among the Lay Public in Low- and Middle-Income Countries: A Scoping Review. Antibiotics 2020, 9, 597. [Google Scholar] [CrossRef]
- Do, N.T.T.; Vu, H.T.L.; Nguyen, C.T.K.; Punpuing, S.; Khan, W.A.; Gyapong, M.; Asante, K.P.; Munguambe, K.; Gómez-Olivé, F.X.; John-Langba, J.; et al. Community-based antibiotic access and use in six low-income and middle-income countries: A mixed-method approach. Lancet Glob. Health 2021, 9, e610–e619. [Google Scholar] [CrossRef]
- Chowdhury, M.; Williams, J.S.; Wertheim, H.; Khan, W.A.; Matin, A.; Kinsman, J. Rural community perceptions of antibiotic access and understanding of antimicrobial resistance: Qualitative evidence from the Health and Demographic Surveillance System site in Matlab, Bangladesh. Glob. Health Action 2019, 12, 1824383. [Google Scholar] [CrossRef]
- World Health Organization. Antibiotic Resistance: Multi-Country Public Awareness Survey. 2015. Available online: http://apps.who.int/iris/bitstream/10665/194460/1/9789241509817_eng.pdf (accessed on 13 October 2022).
- Founou, R.C.; Blocker, A.J.; Noubom, M.; Tsayem, C.; Choukem, S.P.; Van Dongen, M.; Founou, L.L. The COVID-19 pandemic: A threat to antimicrobial resistance containment. Future Sci. OA 2021, 7, FSO736. [Google Scholar] [CrossRef]
- Vestesson, E.; Booth, J.; Hatcher, J.; McGarrity, O.; Sebire, N.J.; Steventon, A.; Alonso, C.S.; Tomlin, S.; Standing, J.F. The impact of the COVID-19 pandemic on antimicrobial prescribing at a specialist paediatric hospital: An observational study. J. Antimicrob. Chemother. 2022, 77, 1185–1188. [Google Scholar] [CrossRef] [PubMed]
- Nieuwlaat, R.; Mbuagbaw, L.; Mertz, D.; Burrows, L.L.; E Bowdish, D.M.; Moja, L.; Wright, G.D.; Schünemann, H.J. Coronavirus Disease 2019 and Antimicrobial Resistance: Parallel and Interacting Health Emergencies. Clin. Infect. Dis. 2021, 72, 1657–1659. [Google Scholar] [CrossRef] [PubMed]
- Hughes, S.; Troise, O.; Donaldson, H.; Mughal, N.; Moore, L.S.P. Bacterial and fungal coinfection among hospitalized patients with COVID-19: A retrospective cohort study in a UK secondary-care setting. Clin. Microbiol. Infect. 2020, 26, 1395–1399. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Geng, X.; Liu, X.; Wen, X.; Wu, R.; Cui, D.; Mao, Z. Antibiotic Use in China’s Public Healthcare Institutions during the COVID-19 Pandemic: An Analysis of Nationwide Procurement Data, 2018–2020. Front. Pharmacol. 2022, 13, 813213. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Antimicrobial Consumption in the EU/EEA (ESAC-Net)—Annual Epidemiological Report 2020; ECDC: Stockholm, Sweden, 2021. [Google Scholar]
- Al-Azzam, S.; Mhaidat, N.; Banat, H.; Alfaour, M.; Ahmad, D.; Muller, A.; Al-Nuseirat, A.; Lattyak, E.; Conway, B.; Aldeyab, M. An Assessment of the Impact of Coronavirus Disease (COVID-19) Pandemic on National Antimicrobial Consumption in Jordan. Antibiotics 2021, 10, 690. [Google Scholar] [CrossRef]
- Mustafa, Z.U.; Salman, M.; Aldeyab, M.; Kow, C.S.; Hasan, S.S. Antimicrobial consumption among hospitalized patients with COVID-19 in Pakistan. SN Compr. Clin. Med. 2021, 3, 1691–1695. [Google Scholar] [CrossRef]
- Hamidi, A.A.; Yilmaz, Ş. Antibiotic consumption in the hospital during COVID-19 pandemic, distribution of bacterial agents and antimicrobial resistance: A single-center study. J. Surg. Med. 2021, 5, 124–127. [Google Scholar] [CrossRef]
- Grau, S.; Echeverria-Esnal, D.; Gómez-Zorrilla, S.; Navarrete-Rouco, M.E.; Masclans, J.R.; Espona, M.; Gracia-Arnillas, M.P.; Duran, X.; Comas, M.; Horcajada, J.P.; et al. Evolution of Antimicrobial Consumption during the First Wave of COVID-19 Pandemic. Antibiotics 2021, 10, 132. [Google Scholar] [CrossRef]
- Gonzalez-Zorn, B. Antibiotic use in the COVID-19 crisis in Spain. Clin. Microbiol. Infect. 2021, 27, 646–647. [Google Scholar] [CrossRef]
- Buehrle, D.J.; Wagener, M.M.; Nguyen, M.H.; Clancy, C.J. Trends in Outpatient Antibiotic Prescriptions in the United States during the COVID-19 Pandemic in 2020. JAMA Netw. Open 2021, 4, e2126114. [Google Scholar] [CrossRef]
- King, L.M.; Lovegrove, M.C.; Shehab, N.; Tsay, S.; Budnitz, D.S.; I Geller, A.; Lind, J.N.; Roberts, R.M.; A Hicks, L.; Kabbani, S. Trends in US Outpatient Antibiotic Prescriptions during the Coronavirus Disease 2019 Pandemic. Clin. Infect. Dis. 2021, 73, e652–e660. [Google Scholar] [CrossRef] [PubMed]
- Ng, T.M.; Tan, S.H.; Heng, S.T.; Tay, H.L.; Yap, M.Y.; Chua, B.H.; Teng, C.B.; Lye, D.C.; Lee, T.H. Effects of coronavirus disease 2019 (COVID-19) pandemic on antimicrobial prevalence and prescribing in a tertiary hospital in Singapore. Antimicrob. Resist. Infect. Control. 2021, 10, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Högberg, L.D.; Vlahović-Palčevski, V.; Pereira, C.; Weist, K.; Monnet, D.L. ESAC-Net study group Decrease in community antibiotic consumption during the COVID-19 pandemic, EU/EEA 2020. EuroSurveillance 2021, 26, 2101020. [Google Scholar] [CrossRef]
- Kalam, M.A.; Shano, S.; Afrose, S.; Uddin, M.N.; Rahman, N.; Jalal, F.A.; Akter, S.; Islam, A.; Anam, M.M.; Hassan, M.M. Antibiotics in the Community during the COVID-19 Pandemic: A Qualitative Study to Understand Users’ Perspectives of Antibiotic Seeking and Consumption Behaviors in Bangladesh. Patient Prefer. Adherence 2022, 16, 217–233. [Google Scholar] [CrossRef]
- Akhtar, Z.; Mah, E.M.S.; Rashid, M.M.; Ahmed, M.S.; Islam, M.A.; Chowdhury, S.; Khan, Z.; Hassan, M.Z.; Islam, K.; Parveen, S.; et al. Antibiotics Use and Its Knowledge in the Community: A Mobile Phone Survey during the COVID-19 Pandemic in Bangladesh. Antibiotics 2021, 10, 1052. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.T.; Lee, V.; Lee, J.C.Y.; Lee, N.C.T.; Ng, T.Y.; Shafie, A.A.; Thong, K.S. Public KAP towards COVID-19 and Antibiotics Resistance: A Malaysian Survey of Knowledge and Awareness. Int. J. Environ. Res. Public Health 2021, 18, 3964. [Google Scholar] [CrossRef] [PubMed]
- Welschen, I.; Kuyvenhoven, M.; Hoes, A.; Verheij, T. Antibiotics for acute respiratory tract symptoms: Patients’ expectations, GPs’ management and patient satisfaction. Fam. Pract. 2004, 21, 234–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quispe-Cañari, J.F.; Fidel-Rosales, E.; Manrique, D.; Mascaró-Zan, J.; Huamán-Castillón, K.M.; Chamorro–Espinoza, S.E.; Garayar–Peceros, H.; Ponce–López, V.L.; Sifuentes-Rosales, J.; Alvarez-Risco, A.; et al. Self-medication practices during the COVID-19 pandemic among the adult population in Peru: A cross-sectional survey. Saudi Pharm. J. 2021, 29, 1–11. [Google Scholar] [CrossRef]
- Shubham Rajkoshor, P.; Hareshwar, P.D.; Swati, S.R. Trends in the use of home-remedies and over-the-counter drugs during COVID-19 Pandemic: A Cross-Sectional Study. Indian J. Prev. Soc. Med. 2021, 52, 169–176. [Google Scholar]
- Azhar, H.; Tauseef, A.; Usman, T.; Azhar, Y.; Ahmed, M.; Umer, K.; Shoaib, M. Prevalence, Attitude and Knowledge of Self Medication during COVID-19 Disease Pandemic. Pak. J. Med. Health Sci. 2021, 15, 902–905. [Google Scholar] [CrossRef]
- Ayosanmi, O.S.; Alli, B.Y.; Akingbule, O.A.; Alaga, A.H.; Perepelkin, J.; Marjorie, D.; Sansgiry, S.S.; Taylor, J. Prevalence and Correlates of Self-Medication Practices for Prevention and Treatment of COVID-19: A Systematic Review. Antibiotics 2022, 11, 808. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. Perceived Behavioral Control, Self-Efficacy, Locus of Control, and the Theory of Planned Behavior. J. Appl. Soc. Psychol. 2002, 32, 665–683. [Google Scholar] [CrossRef]
- McNulty, C.A.M.; Boyle, P.; Nichols, T.; Clappison, P.; Davey, P. The public’s attitudes to and compliance with antibiotics. J. Antimicrob. Chemother. 2007, 60 (Suppl. 1), i63–i68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Zhao, X.; Li, Y.; Wang, N.; Jiang, F.; Lambert, H.; Yan, F.; Fu, C.; Jiang, Q. Patterns and Determinants of Antibiotic Use Behaviors among Rural Community Residents in Eastern China. Antibiotics 2022, 11, 823. [Google Scholar] [CrossRef] [PubMed]
- Waaseth, M.; Adan, A.; Røen, I.L.; Eriksen, K.; Stanojevic, T.; Halvorsen, K.H.; Garcia, B.H.; Holst, L.; Ulshagen, K.M.; Blix, H.S.; et al. Knowledge of antibiotics and antibiotic resistance among Norwegian pharmacy customers—A cross-sectional study. BMC Public Health 2019, 19, 66. [Google Scholar] [CrossRef] [PubMed]
- Zucco, R.; Lavano, F.; Anfosso, R.; Bianco, A.; Pileggi, C.; Pavia, M. Internet and social media use for antibiotic-related information seeking: Findings from a survey among adult population in Italy. Int. J. Med. Inform. 2018, 111, 131–139. [Google Scholar] [CrossRef]
- Elsayed, A.A.; Darwish, S.F.; Zewail, M.B.; Mohammed, M.; Saeed, H.; Rabea, H. Antibiotic misuse and compliance with infection control measures during COVID-19 pandemic in community pharmacies in Egypt. Int. J. Clin. Pract. 2021, 75, e14081. [Google Scholar] [CrossRef]
- Chen, J.; Wang, Y.; Chen, X.; Hesketh, T. Widespread illegal sales of antibiotics in Chinese pharmacies—A nationwide cross-sectional study. Antimicrob. Resist. Infect. Control. 2020, 9, 1–8. [Google Scholar] [CrossRef]
- Deqing County Market Supervision Administration. Notice on Uspension of Sales of “Antipyretic, Antitussive, Antiviral, Antimicrobial”. Available online: http://www.deqing.gov.cn/hzgov/front/s170/zfxxgk/yqfk/tzgg/20220624/i3218597.html (accessed on 24 April 2022).
- Cai, S.; Wang, N.; Xu, L.; Yan, F.; Jiang, Q.; Zhao, X.; Wang, W.; Wang, H.; Jiang, L.; Cong, W.; et al. Impacts of Antibiotic Residues in the Environment on Bacterial Resistance and Human Health in Eastern China: An Interdisciplinary Mixed-Methods Study Protocol. Int. J. Environ. Res. Public Health 2022, 19, 8145. [Google Scholar] [CrossRef]
- World Health Organization. Manual for the Household Survey to Measure Access and Use of Medicines. 2015. Available online: https://www.scirp.org/reference/ReferencesPapers.aspx?ReferenceID=1608696 (accessed on 26 June 2022).
- Thompson, N.D.; Stone, N.D.; Brown, C.J.; Penna, A.R.; Eure, T.R.; Bamberg, W.M.; Barney, G.R.; Barter, D.; Clogher, P.; DeSilva, M.B. Antimicrobial use in a cohort of US nursing homes, 2017. JAMA 2021, 325, 1286–1295. [Google Scholar]
- World Health Organization. Guidelines for ATC Classification and DDD Assignment. 2022. Available online: https://www.whocc.no/atc_ddd_index_and_guidelines/guidelines/ (accessed on 20 April 2022).
- Nai-Qing, Z. Statistical Methods for incidence rate. Chin. J. Health Stat. 2006, 23, 534–535. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | 2019 | 2020 | χ2 or t | p Value |
|---|---|---|---|---|---|
| n = 1111 | n = 440 | n = 671 | |||
| Gender | |||||
| Male | 533 (47.97) | 217 (49.32) | 316 (47.09) | 0.441 | 0.506 |
| Female | 578 (52.03) | 223 (50.68) | 355 (52.91) | ||
| Age (years; mean ± SD) | 59.17 ± 14.07 | 57.63 ± 14.70 | 60.14 ± 13.57 | 35.3 | 0.004 |
| 15–34 | 68 (6.12) | 34 (7.73) | 34 (5.07) | 6.630 | <0.036 |
| 35–59 | 464 (41.76) | 195 (44.32) | 269 (40.09) | ||
| ≥60 | 579 (52.12) | 211 (47.95) | 368 (54.84) | ||
| Education (years) * | |||||
| ≤6 | 768 (69.13) | 297 (67.50) | 471 (70.19) | 0.782 | 0.377 |
| >6 | 343 (30.87) | 143 (32.50) | 200 (29.81) | ||
| Farmer * | |||||
| No | 687 (62.74) | 249 (58.73) | 438 (65.28) | 4.491 | 0.034 |
| Yes | 408 (37.26) | 175 (41.27) | 233 (34.72) | ||
| Annual household income (CNY) * | |||||
| ≤100,000 | 491 (49.25) | 144 (36.64) | 347 (57.45) | 40.419 | <0.001 |
| >100,000 | 506 (50.75) | 249 (63.36) | 257 (42.55) | ||
| History of chronic diseases | |||||
| No | 615 (57.32) | 243 (60.45) | 372 (55.44) | 2.377 | <0.123 |
| Yes | 458 (42.68) | 159 (39.55) | 299 (44.56) | ||
| Characteristics | 2019 | 2020 | RR | Z Value | p Value | ||||
|---|---|---|---|---|---|---|---|---|---|
| Person Months | Cases | IR (100 PMs) | Person Months | Cases | IR (100 PMs) | ||||
| Overall | 2116 | 115 | 5.43 | 3273 | 422 | 12.89 | 2.37 | 77.981 | <0.001 |
| Gender | |||||||||
| Male | 1020 | 59 | 5.86 | 1520 | 187 | 12.30 | 2.10 | 33.276 | <0.001 |
| Female | 1095 | 56 | 5.11 | 1753 | 235 | 13.41 | 2.62 | 43.558 | <0.001 |
| Age (years) | |||||||||
| 15–34 | 147 | 4 | 2.72 | 152 | 7 | 4.61 | 1.53 | 1.082 | 0.280 |
| 35–59 | 914 | 41 | 4.49 | 1205 | 147 | 12.20 | 2.72 | 32.079 | <0.001 |
| ≥60 | 968 | 66 | 6.82 | 1754 | 252 | 14.37 | 2.11 | 39.053 | <0.001 |
| Education (years) * | |||||||||
| ≤6 | 1384 | 71 | 5.13 | 2203 | 295 | 13.39 | 2.61 | 54.904 | <0.001 |
| >6 | 645 | 40 | 6.20 | 908 | 111 | 12.22 | 1.97 | 19.937 | <0.001 |
| Farmer * | |||||||||
| No | 1130 | 53 | 4.69 | 1993 | 257 | 12.90 | 2.75 | 44.457 | <0.001 |
| Yes | 899 | 58 | 6.45 | 1117 | 149 | 13.34 | 2.07 | 30.338 | <0.001 |
| Annual household income (CNY) * | |||||||||
| ≤100,000 | 624 | 42 | 6.73 | 1618 | 230 | 14.22 | 2.11 | 26.518 | <0.001 |
| >100,000 | 1185 | 53 | 4.47 | 1195 | 139 | 11.63 | 2.60 | 36.663 | <0.001 |
| History of chronic diseases | |||||||||
| No | 1148 | 57 | 4.97 | 1695 | 220 | 12.98 | 2.61 | 43.43 | <0.001 |
| Yes | 724 | 39 | 5.39 | 1416 | 186 | 13.14 | 2.44 | 28.76 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, B.; Zhao, X.; Li, Y.; Wang, N.; Lambert, H.; Yan, F.; Jiang, Q.; Fu, C. Impact of the COVID-19 Outbreak on the Antibiotic Use Patterns among a Rural Community Population in Eastern China. Antibiotics 2022, 11, 1544. https://doi.org/10.3390/antibiotics11111544
Zhu B, Zhao X, Li Y, Wang N, Lambert H, Yan F, Jiang Q, Fu C. Impact of the COVID-19 Outbreak on the Antibiotic Use Patterns among a Rural Community Population in Eastern China. Antibiotics. 2022; 11(11):1544. https://doi.org/10.3390/antibiotics11111544
Chicago/Turabian StyleZhu, Bingbing, Xinping Zhao, Yurong Li, Na Wang, Helen Lambert, Fei Yan, Qingwu Jiang, and Chaowei Fu. 2022. "Impact of the COVID-19 Outbreak on the Antibiotic Use Patterns among a Rural Community Population in Eastern China" Antibiotics 11, no. 11: 1544. https://doi.org/10.3390/antibiotics11111544