
Beyond Guidelines and Reports on Bacterial Co-/Superinfections in the Context of COVID-19: Why Uniformity Matters


Abstract
:1. Introduction
2. Antimicrobial Stewardship Applied to COVID-19 Patients: The Pursuit of Knowledge
3. Evidence on bCS Rates in COVID-19 Patients: A Critical Point of View
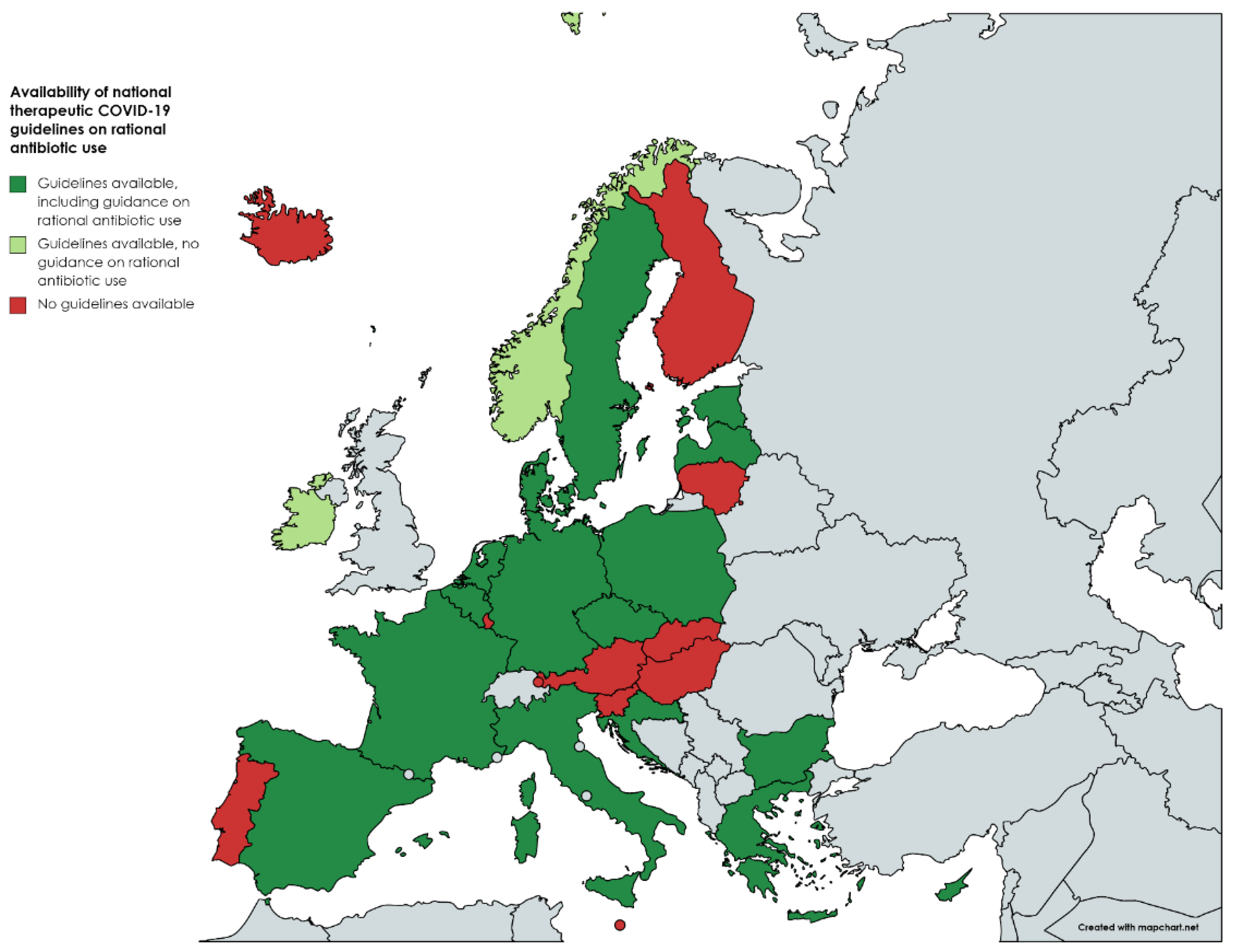
4. European Therapeutic COVID-19 Guidelines: An Emphasis on Antibiotic Guidance
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. AAntimicrobial Resistance. Global Report on Surveillance. 2014. Available online: https://www.who.int/publications/i/item/9789241564748 (accessed on 27 August 2022).
- European Centre for Disease Prevention and Control. Antimicrobial Consumption in the EU/EEA (ESAC-Net)—Annual Epidemiological Report 2020; ECDC: Stockholm, Sweden, 2021. [Google Scholar]
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A.H. Bacterial and Fungal Coinfection in Individuals with Coronavirus: A Rapid Review to Support COVID-19 Antimicrobial Prescribing. Clin. Infect. Dis. 2020, 71, 2459–2468. [Google Scholar] [CrossRef] [PubMed]
- Langford, B.J.; So, M.; Raybardhan, S.; Leung, V.; Westwood, D.; MacFadden, D.R.; Soucy, J.-P.R.; Daneman, N. Bacterial co-infection and secondary infection in patients with COVID-19: A living rapid review and meta-analysis. Clin. Microbiol. Infect. 2020, 26, 1622–1629. [Google Scholar] [CrossRef]
- Langford, B.J.; So, M.; Leung, V.; Raybardhan, S.; Lo, J.; Kan, T.; Leung, F.; Westwood, D.; Daneman, N.; MacFadden, D.R.; et al. Predictors and microbiology of respiratory and bloodstream bacterial infection in patients with COVID-19: Living rapid review update and meta-regression. Clin. Microbiol. Infect. 2022, 28, 491–501. [Google Scholar] [CrossRef] [PubMed]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-infections in people with COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef]
- Musuuza, J.S.; Watson, L.; Parmasad, V.; Putman-Buehler, N.; Christensen, L.; Safdar, N. Prevalence and outcomes of co-infection and superinfection with SARS-CoV-2 and other pathogens: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0251170. [Google Scholar] [CrossRef]
- Russell, C.D.; Fairfield, C.J.; Drake, T.M.; Turtle, L.; Seaton, R.A.; Wootton, D.G.; Sigfrid, L.; Harrison, E.M.; Docherty, A.B.; I de Silva, T.; et al. ISARIC4C investigators. Co-infections, secondary infections, and antimicrobial use in patients hospitalised with COVID-19 during the first pandemic wave from the ISARIC WHO CCP-UK study: A multicentre, prospective cohort study. Lancet Microbe 2021, 2, e354–e365. [Google Scholar] [CrossRef]
- Bartoletti, M.; Azap, O.; Barac, A.; Bussini, L.; Ergonul, O.; Krause, R.; Paño-Pardo, J.R.; Power, N.R.; Sibani, M.; Szabo, B.G.; et al. ESCMID COVID-19 living guidelines: Drug treatment and clinical management. Clin. Microbiol. Infect. 2022, 28, 222–238. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19 Clinical Management: Living Guidance; 25 January 2021; Report No.: WHO/2019-nCoV/clinical/2021.1; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Dolci, A.; Robbiano, C.; Aloisio, E.; Chibireva, M.; Serafini, L.; Falvella, F.S.; Pasqualetti, S.; Panteghini, M. Searching for a role of procalcitonin determination in COVID-19: A study on a selected cohort of hospitalized patients. Clin. Chem. Lab. Med. 2020, 59, 433–440. [Google Scholar] [CrossRef]
- Vaughn, V.M.; Gandhi, T.N.; Petty, L.A.; Patel, P.K.; Prescott, H.C.; Malani, A.N.; Ratz, D.; McLaughlin, E.; Chopra, V.; Flanders, S.A. Empiric Antibacterial Therapy and Community-onset Bacterial Coinfection in Patients Hospitalized with Coronavirus Disease 2019 (COVID-19): A Multi-hospital Cohort Study. Clin. Infect. Dis. 2021, 72, e533–e541. [Google Scholar] [CrossRef] [PubMed]
- Van Laethem, J.; Wuyts, S.C.M.; Pierreux, J.; Seyler, L.; Verschelden, G.; Depondt, T.; Meuwissen, A.; Lacor, P.; Piérard, D.; Allard, S.D. Presumed Urinary Tract Infection in Patients Admitted with COVID-19: Are We Treating Too Much? Antibiotics 2021, 10, 1493. [Google Scholar] [CrossRef]
- Sieswerda, E.; de Boer, M.G.; Bonten, M.M.; Boersma, W.G.; Jonkers, R.E.; Aleva, R.M.; Kullberg, B.-J.; Schouten, J.A.; van de Garde, E.M.; Verheij, T.J.; et al. Recommendations for antibacterial therapy in adults with COVID-19—An evidence based guideline. Clin. Microbiol. Infect. 2021, 27, 61–66. [Google Scholar] [CrossRef]
- Recommendations for Antibiotic Treatment of Patients with COVID-19 Infection. Available online: https://www.mh.government.bg/media/filer_public/2021/08/09/preporki_-_mikrobiologiia.pdf (accessed on 25 August 2022).
- Interim Clinical Guidance for Adults with Confirmed COVID-19 in Belgium, July 2022; Version 29. Available online: https://covid-19.sciensano.be/sites/default/files/Covid19/COVID-19_InterimGuidelines_Treatment_ENG.pdf (accessed on 25 August 2022).
- Haut Conseil de la Santé Publique. Coronavirus SARS-CoV-2: Recommandations sur L’usage des Anti Infectieux. Available online: https://www.hcsp.fr/Explore.cgi/AvisRapportsDomaine?clefr=849 (accessed on 25 August 2022).
- Italian Society of Infectious and Tropical Diseases. Vademecum for the Care of People with COVID-19 Disease. Edition 2.0, 13 March 2020. Available online: https://www.eahp.eu/sites/default/files/covid19_vademecum_2.0_13_marzo_2020.03_11.pdf (accessed on 25 August 2022).
- Flisiak, R.; Horban, A.; Jaroszewicz, J. Diagnosis and therapy of SARS-CoV-2 infection: Recommendations of the Polish Association of Epidemiologists and Infectiologists as of 12 November 2021. Annex no. 1 to the Recommendations of 26 April 2021. Pol. Arch. Intern. Med. 2021, 131, 16140. [Google Scholar] [CrossRef]
- Recomendaciones SEIMC Para el Manejo Clínico de Pacientes Con COVID-19. Available online: https://covid19.seimc.org/wp-content/uploads/2022/05/SEIMC-Recomendaciones-COVID_24-mayo-2022.pdf (accessed on 25 August 2022).
- European Centre for Disease Prevention and Control. Treatment and Pharmaceutical Prophylaxis of COVID-19. Available online: https://www.ecdc.europa.eu/en/covid-19/latest-evidence/treatment (accessed on 25 August 2022).
- Ministry of Health of the Republic of Croatia. Guidelines for the Treatment of Patients with Coronavirus Disease 2019 (COVID-19). Version 5 of 8 February 2022. Available online: https://www.koronavirus.hr/uploads/Smjernice_za_lijecenje_oboljelih_od_koronavirusne_bolesti_2019_COVID_19_verzija_5_od_08_veljace_2022_edb7d62da1.pdf (accessed on 25 August 2022).
- Jeschke, K.N.; Bonnesen, B.; Hansen, E.F.; Jensen, J.-U.S.; Lapperre, T.S.; Weinreich, U.M.; Hilberg, O. Guideline for the management of COVID-19 patients during hospital admission in a non-intensive care setting. Eur. Clin. Respir. J. 2020, 7, 1761677. [Google Scholar] [CrossRef] [PubMed]
- Malin, J.J.; Spinner, C.D.; Janssens, U.; Welte, T.; Weber-Carstens, S.; Schälte, G.; Gastmeier, P.; Langer, F.; Wepler, M.; Westhoff, M.; et al. Key pharmacologic recommendations from a national German living guideline using an Evidence to Decision Framework (last updated 17 May 2021). Infection 2022, 50, 93–106. [Google Scholar] [CrossRef]
- Kluge, S.; Janssens, U.; Welte, T.; Weber-Carstens, S.; Marx, G.; Karagiannidis, C. Empfehlungen zur intensivmedizinischen Therapie von Patienten mit COVID-19. Med. Klin. Intensivmed. Notfmed. 2020, 115, 175–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Disease Prevention and Control Centre of Latvia (SPKC). RECOMMENDATIONS. SARS-CoV-2 Infection and Epidemiology of COVID-19, Diagnostics, Clinical Developments and Problems. March 2021. Available online: https://www.spkc.gov.lv/sites/spkc/files/media_file/covid_19_rekomendacijas_marts-gatavs-1.pdf (accessed on 25 August 2022).
- Štefan, M.; Chrdle, A.; Husa, P.; Beneš, J.; Dlouhý, P. COVID-19: Diagnosis and treatment. Klin Mikrobiol Infekc Lek. 2021, 27, 61–87. [Google Scholar] [PubMed]
- Hospital manual treatment of infection. COVID-19. November 2020. Not available online. To access the pdf file, please contact the corresponding author of this paper.
- Kallaste, A.; Härma, E.; Rätsep, H. COVID-19 patsiendi käsitlusjuhend Tartu Ülikooli Kliinikumis ja Põhja-Eesti Regionaalhaiglas. Version 1. Revised version: 11.11.2020. To access the pdf file, please contact the corresponding author of this paper.
- Kluge, S.; Janssens, U.; Spinner, C.D.; Pfeifer, M.; Marx, G.; Karagiannidis, C.; Guideline, group. Clinical practice guideline: Recommendations on in-hospital treatment of patients with COVID-19. Dtsch. Arztebl. Int. 2021, 118, 1–7. [Google Scholar]
- Greece: Hellenic Society of Infectious Diseases. Therapeutic Algorithm of Adult Hospitalized Patients with COVID-19*. February 2022. Available online: https://eody.gov.gr/wp-content/uploads/2022/02/covid_19_algorithmos-nosileuomenon_20220217.pdf (accessed on 10 September 2022).
- HSE Interim Guidance for the Pharmacological Management of Patients with COVID-19. Available online: https://hse-ie.libguides.com/ld.php?content_id=33534048 (accessed on 25 August 2022).
- Norwegian Institute of Public Health. NIPH Systematic and Living Map on COVID-19 Evidence. Available online: https://www.nornesk.no/forskningskart/NIPH_interventionsTreatMap.html (accessed on 25 August 2022).
- Nationellt Vårdprogram för Misstänkt Och Bekräftad COVID-19. Version 4 maj 2022. Framtaget av Svenska Infektionsläkarföreningen, Svenska Hygienläkarföreningen och Föreningen för Klinisk Mikrobiologi. Available online: https://infektion.net/wp-content/uploads/2022/09/nationellt-vardprogram-covid-version-4-1.pdf (accessed on 30 August 2022).


{kind=link}
| Reference and Type of Study | Co-/Superinfection * Definitions | Used Diagnostic Criteria | Reported Pathogens | Reported Infections | Setting (Ward/ICU) | Age Group | Co-/Superinfection Rate | Antibiotic Prescription Rate |
|---|---|---|---|---|---|---|---|---|
| Langford et al. (2020) [4] Systematic meta-analysis | co-infection: “on presentation” Superinfection: “emerging during the course of illness or during hospitalization” | Not mentioned if clinical and/or microbiological diagnosis | Bacterial | Respiratory tract infections and bloodstream infections | Ward and ICU | Pediatric and adult patients (25%/75%) | co-infection 3.5% superinfection 14.3% | 72% |
| Langford et al. (2022) [5] Systematic meta-analysis | co-infection: not defined | Microbiological diagnosis Exclusion of “presumed” or “suspected” bacterial infection | Bacterial | Respiratory tract infections and bloodstream infections | Ward and ICU | Pediatric and adult patients | co-infection 5.1% secondary infection 13.1% | 75% |
| Lansburry et al. [6] Systematic meta-analysis | co-infection: not defined. Unclear if this term was used to group “co-infections” and “superinfections” | Microbiological diagnosis (culture and PCR) | Bacterial, viral, fungal | Respiratory tract infections and bloodstream infections | Ward and ICU | Pediatric and adult patients | co-infection 7% (bacterial) | NR |
| Musuuza et al. [7] Systematic meta-analysis | co-infection: “at the time of a SARS-CoV-2 infection” superinfection: “during care for SARS-CoV-2 infection” | Microbiological diagnosis | Bacterial, viral, fungal | Respiratory tract infections | Ward and ICU | Pediatric and adult patients | co-infection 8% superinfection 20% (bacterial) | NR |
| Russell et al. [8] Original paper | Co-infection: clinically significant positive results from samples collected within 2 days of admission Superinfection: infection occurring > 2 days after hospital admission | Microbiological diagnosis | Bacterial, fungal | Respiratory tract infections and bloodstream infections | Ward and ICU | Not reported | co-infection 0.7% “secondary” infection 1.5% | 85% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Laethem, J.; Piérard, D.; Allard, S.D. Beyond Guidelines and Reports on Bacterial Co-/Superinfections in the Context of COVID-19: Why Uniformity Matters. Antibiotics 2022, 11, 1446. https://doi.org/10.3390/antibiotics11101446
Van Laethem J, Piérard D, Allard SD. Beyond Guidelines and Reports on Bacterial Co-/Superinfections in the Context of COVID-19: Why Uniformity Matters. Antibiotics. 2022; 11(10):1446. https://doi.org/10.3390/antibiotics11101446
Chicago/Turabian StyleVan Laethem, Johan, Denis Piérard, and Sabine D. Allard. 2022. "Beyond Guidelines and Reports on Bacterial Co-/Superinfections in the Context of COVID-19: Why Uniformity Matters" Antibiotics 11, no. 10: 1446. https://doi.org/10.3390/antibiotics11101446