
Long-Term Impact of an Educational Antimicrobial Stewardship Program on Management of Patients with Hematological Diseases

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
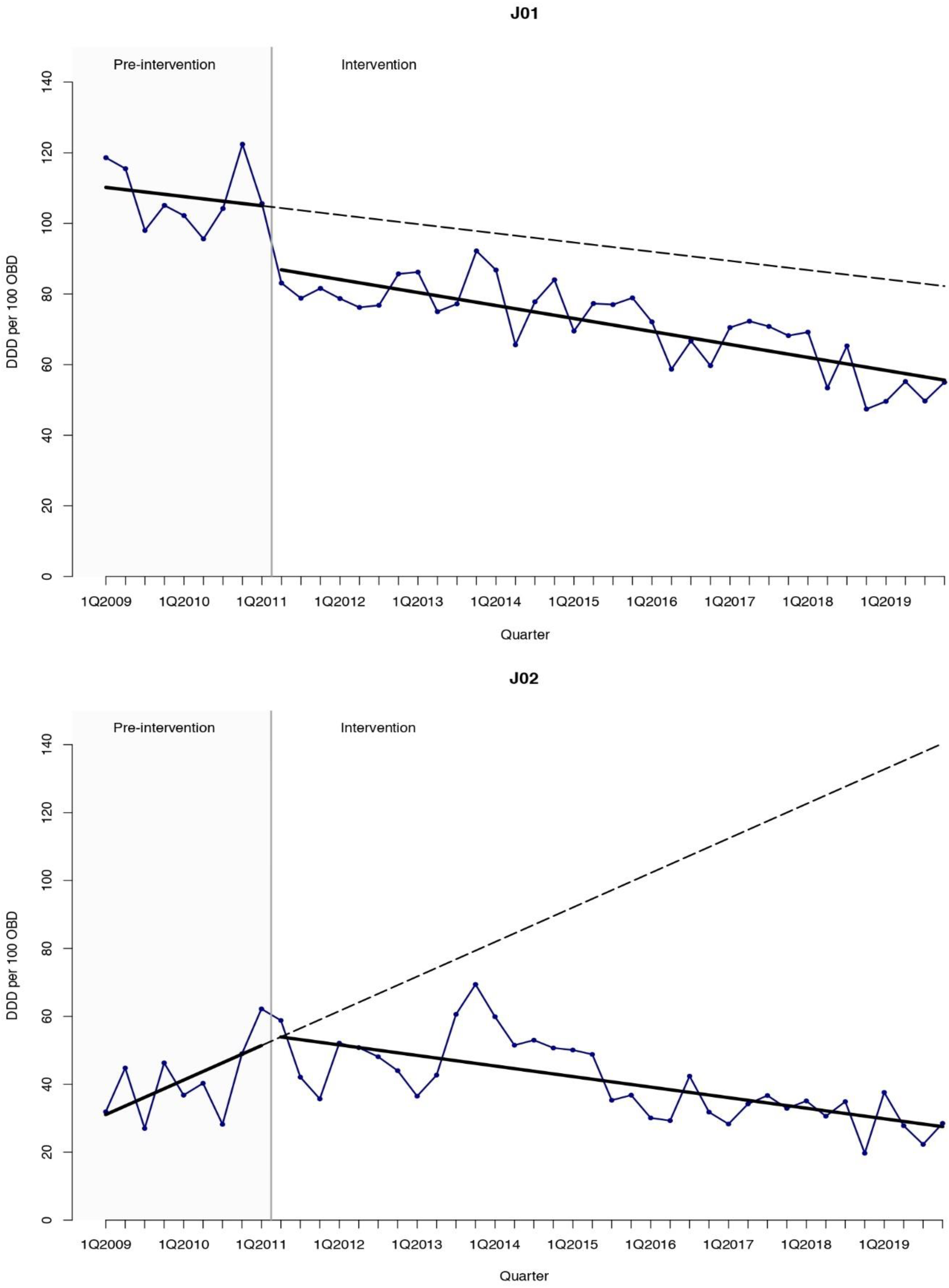
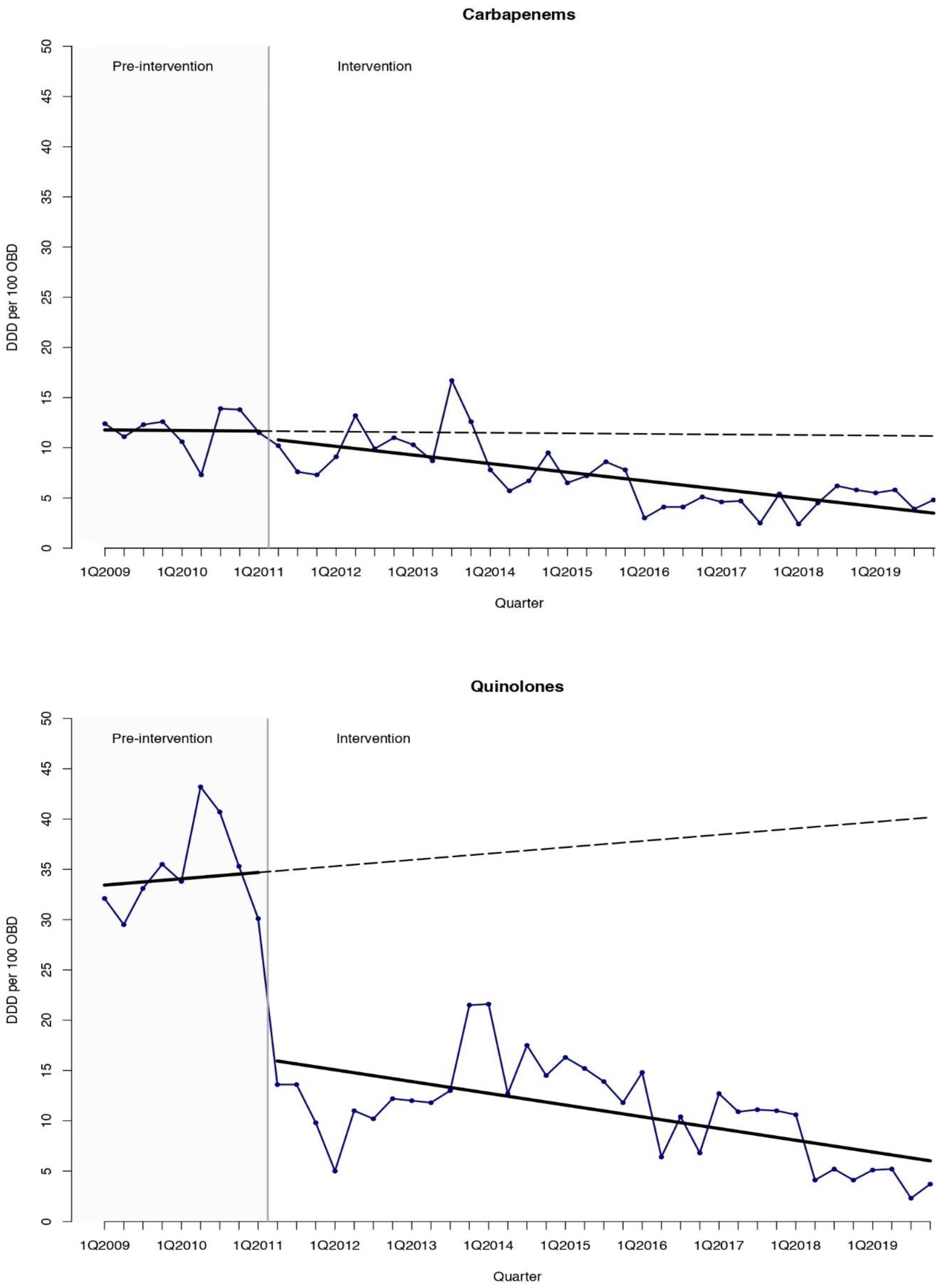
2.1. Antimicrobial Consumption
2.2. Clinical Outcomes
2.3. Changes in Healthcare during the Study Period
3. Discussion
4. Materials and Methods
4.1. Study Design and Period
4.2. Setting
4.3. Intervention
4.4. Study Measures
4.5. Statistical Analysis
4.6. Ethics Approval
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Implementing an antibiotic stewardship program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef] [PubMed]
- Alevizakos, M.; Gaitanidis, A.; Andreatos, N.; Arunachalam, K.; Flokas, M.E.; Mylonakis, E. Bloodstream infections due to extended-spectrum β-lactamase- producing Enterobacteriaceae among patients with malignancy: A systematic review and meta-analysis. Int. J. Antimicrob. Agents 2017, 50, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Das, I.; Nightingale, P.; Patel, M.; Jumaa, P. Epidemiology, clinical characteristics, and outcome of candidemia: Experience in a tertiary referral center in the UK. Int. J. Infect. Dis. 2011, 15, e759–e763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taur, Y.; Jenq, R.R.; Perales, M.A.; Littmann, E.R.; Morjaria, S.; Ling, L.; No, D.; Gobourne, A.; Viale, A.; Dahi, P.B.; et al. The effects of intestinal tract bacterial diversity on mortality following allogeneic hematopoietic stem cell transplantation. Blood 2014, 124, 1174–1182. [Google Scholar] [CrossRef] [PubMed]
- Madran, B.; Keske, Ş.; Tokça, G.; Dönmez, E.; Ferhanoğlu, B.; Çetiner, M.; Mandel, N.M.; Ergönül, Ö. Implementation of an antimicrobial stewardship program for patients with febrile neutropenia. Am. J. Infect. Control 2018, 46, 420–424. [Google Scholar] [CrossRef]
- Webb, B.J.; Majers, J.; Healy, R.; Jones, P.B.; Butler, A.M.; Snow, G.; Forsyth, S.; Lopansri, B.K.; Ford, C.D.; Hoda, D. Antimicrobial Stewardship in a Hematological Malignancy Unit: Carbapenem Reduction and Decreased Vancomycin-Resistant Enterococcus Infection. Clin. Infect. Dis. 2020, 71, 960–967. [Google Scholar] [CrossRef]
- Mardani, M.; Abolghasemi, S.; Shabani, S. Impact of an antimicrobial stewardship program in the antimicrobial-resistant and prevalence of clostridioides difficile infection and amount of antimicrobial consumed in cancer patients. BMC Res. Notes 2020, 13, 246. [Google Scholar] [CrossRef]
- Cisneros, J.M.; Neth, O.; Gil-Navarro, M.V.; Lepe, J.A.; Jiménez-Parrilla, F.; Cordero, E.; Rodríguez-Hernández, M.J.; Amaya-Villar, R.; Cano, J.; Gutiérrez-Pizarraya, A.; et al. Global impact of an educational antimicrobial stewardship program on prescribing practice in a tertiary hospital centre. Clin. Microbiol. Infect. 2014, 20, 82–88. [Google Scholar] [CrossRef] [Green Version]
- Molina, J.; Peñalva, G.; Gil-Navarro, M.V.; Praena, J.; Lepe, J.A.; Pérez-Moreno, M.A.; Ferrándiz, C.; Aldabó, T.; Aguilar, M.; Olbrich, P.; et al. Long-Term Impact of an educational antimicrobial stewardship program on hospital-acquired candidemia and multidrug-resistant bloodstream infections: A quasi-experimental study of interrupted time-series analysis. Clin. Infect. Dis. 2017, 65, 1992–1999. [Google Scholar] [CrossRef] [Green Version]
- So, M.; Mamdani, M.M.; Morris, A.M.; Lau, T.T.Y.; Broady, R.; Deotare, U.; Grant, J.; Kim, D.; Schimmer, A.D.; Schuh, A.C.; et al. Effect of an antimicrobial stewardship programme on antimicrobial utilisation and costs in patients with leukaemia: A retrospective controlled study. Clin. Microbiol. Infect. 2018, 24, 882–888. [Google Scholar] [CrossRef] [Green Version]
- Yeo, C.L.; Chan, D.S.; Earnest, A.; Wu, T.S.; Yeoh, S.F.; Lim, R.; Jureen, R.; Fisher, D.; Hsu, L.Y. Prospective audit and feedback on antibiotic prescription in an adult haematology-oncology unit in Singapore. Eur. J. Clin. Microbiol. Infect. Dis. 2012, 31, 583–590. [Google Scholar] [CrossRef] [PubMed]
- WHO. Antimicrobial Resistance. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 12 December 2020).
- Gudiol, C.; Tubau, F.; Calatayud, L.; Garcia-Vidal, C.; Cisnal, M.; Sánchez-Ortega, I.; Duarte, R.; Calvo, M.; Carratalà, J. Bacteraemia due to multidrug-resistant Gram-negative bacilli in cancer patients: Risk factors, antibiotic therapy and outcomes. J. Antimicrob. Chemother. 2011, 66, 657–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montassier, E.; Batard, E.; Gastinne, T.; Potel, G.; de La Cochetière, M.F. Recent changes in bacteremia in patients with cancer: A systematic review of epidemiology and antibiotic resistance. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 841–850. [Google Scholar] [CrossRef]
- Garcia-Vidal, C.; Cardozo-Espinola, C.; Puerta-Alcalde, P.; Marco, F.; Tellez, A.; Agüero, D.; Romero-Santana, F.; Díaz-Beyá, M.; Giné, E.; Morata, L.; et al. Risk factors for mortality in patients with acute leukemia and bloodstream infections in the era of multiresistance. PLoS ONE 2018, 13, e0199531. [Google Scholar] [CrossRef] [PubMed]
- Averbuch, D.; Tridello, G.; Hoek, J.; Mikulska, M.; Akan, H.; Yanez San Segundo, L.; Pabst, T.; Özçelik, T.; Klyasova, G.; Donnini, I.; et al. Antimicrobial Resistance in Gram-Negative Rods Causing Bacteremia in Hematopoietic Stem Cell Transplant Recipients: Intercontinental Prospective Study of the Infectious Diseases Working Party of the European Bone Marrow Transplantation Group. Clin. Infect. Dis. 2017, 65, 1819–1828. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Nadal, G.; Puerta-Alcalde, P.; Gudiol, C.; Cardozo, C.; Albasanz-Puig, A.; Marco, F.; Laporte-Amargós, J.; Moreno-García, E.; Domingo-Doménech, E.; Chumbita, M.; et al. Inappropriate Empirical Antibiotic Treatment in High-risk Neutropenic Patients With Bacteremia in the Era of Multidrug Resistance. Clin. Infect. Dis. 2020, 70, 1068–1074. [Google Scholar] [CrossRef] [PubMed]
- Trecarichi, E.M.; Pagano, L.; Candoni, A.; Pastore, D.; Cattaneo, C.; Fanci, R.; Nosari, A.; Caira, M.; Spadea, A.; Busca, A.; et al. Current epidemiology and antimicrobial resistance data for bacterial bloodstream infections in patients with hematologic malignancies: An Italian multicentre prospective survey. Clin. Microbiol. Infect. 2015, 21, 337–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosa, R.G.; Goldani, L.Z.; dos Santos, R.P. Association between adherence to an antimicrobial stewardship program and mortality among hospitalised cancer patients with febrile neutropaenia: A prospective cohort study. BMC Infect. Dis. 2014, 14, 286. [Google Scholar] [CrossRef] [Green Version]
- La Martire, G.; Robin, C.; Oubaya, N.; Lepeule, R.; Beckerich, F.; Leclerc, M.; Barhoumi, W.; Toma, A.; Pautas, C.; Maury, S.; et al. De-escalation and discontinuation strategies in high-risk neutropenic patients: An interrupted time series analyses of antimicrobial consumption and impact on outcome. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1931–1940. [Google Scholar] [CrossRef]
- Petteys, M.M.; Kachur, E.; Pillinger, K.E.; He, J.; Copelan, E.A.; Shahid, Z. Antimicrobial de-escalation in adult haematopoietic cell transplantation recipients with febrile neutropenia of unknown origin. J. Oncol. Pharm. Pract. 2020, 26, 632–640. [Google Scholar] [CrossRef]
- Snyder, M.; Pasikhova, Y.; Baluch, A. Early Antimicrobial De-escalation and Stewardship in Adult Haematopoietic Stem Cell Transplantation Recipients: Retrospective Review. Open Forum Infect. Dis. 2017, 4, ofx226. [Google Scholar] [CrossRef] [PubMed]
- De Kraker, M.E.A.; Abbas, M.; Huttner, B.; Harbarth, S. Good epidemiological practice: A narrative review of appropriate scientific methods to evaluate the impact of antimicrobial stewardship interventions. Clin. Microbiol. Infect. 2017, 23, 819–825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguilar-Guisado, M.; Espigado, I.; Martín-Peña, A.; Gudiol, C.; Royo-Cebrecos, C.; Falantes, J.; Vázquez-López, L.; Montero, M.I.; Rosso-Fernández, C.; de la Luz Martino, M.; et al. Optimisation of empirical antimicrobial therapy in patients with haematological malignancies and febrile neutropenia (How Long study): An open-label, randomised, controlled phase 4 trial. Lancet Haematol. 2017, 4, e573–e583. [Google Scholar] [CrossRef]
- Averbuch, D.; Orasch, C.; Cordonnier, C.; Livermore, D.M.; Mikulska, M.; Viscoli, C.; Gyssens, I.C.; Kern, W.V.; Klyasova, G.; Marchetti, O.; et al. European guidelines for empirical antibacterial therapy for febrile neutropenic patients in the era of growing resistance: Summary of the 2011 4th European Conference on Infections in Leukemia. Haematologica 2013, 98, 1826–1835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina, J.; Noguer, M.; Lepe, J.A.; Pérez-Moreno, M.A.; Aguilar-Guisado, M.; de la Vega, R.L.; Peñalva, G.; Crespo-Rivas, J.C.; Gil-Navarro, M.V.; Salvador, J.; et al. Clinical impact of an educational antimicrobial stewardship program associated with infectious diseases consultation targeting patients with cancer: Results of a 9-year quasi-experimental study with an interrupted time-series analysis. J. Infect. 2019, 79, 206–211. [Google Scholar] [CrossRef] [PubMed]
- Tissot, F.; Agrawal, S.; Pagano, L.; Petrikkos, G.; Groll, A.H.; Skiada, A.; Lass-Flörl, C.; Calandra, T.; Viscoli, C.; Herbrecht, R. ECIL-6 guidelines for the treatment of invasive candidiasis, aspergillosis and mucormycosis in leukemia and hematopoietic stem cell transplant patients. Haematologica 2017, 102, 433–444. [Google Scholar] [CrossRef] [Green Version]
- WHO. Collaborating Center for Drug Statistics Methodology. DDD Definition and General Considerations. 2019. Available online: https://www.whocc.no/ddd/ (accessed on 12 December 2020).
- Mattner, F.; Bange, F.C.; Meyer, E.; Seifert, H.; Wichelhaus, T.A.; Chaberny, I.F. Preventing the spread of multidrug-resistant gram-negative pathogens: Recommendations of an expert panel of the German Society for Hygiene and Microbiology. Dtsch. Arztebl. Int. 2012, 109, 39–45. [Google Scholar] [CrossRef]
- The European Committee on Antimicrobial Susceptibility Testing. EUCAST Guideline for the Detection of Resistance Mechanisms and Specific Resistances of Clinical and/or Epidemiological Importance. Version 2.0. 2017. Available online: https://www.eucast.org/resistance_mechanisms/ (accessed on 12 December 2020).
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 10.0. 2020. Available online: http://www.eucast.org (accessed on 12 December 2020).
- Porta, M. (Ed.) A Dictionary of Epidemiology, 6th ed.; Oxford University Press: New York, NY, USA, 2014. [Google Scholar]
- López-Cortés, L.E.; Del Toro, M.D.; Gálvez-Acebal, J.; Bereciartua-Bastarrica, E.; Fariñas, M.C.; Sanz-Franco, M.; Natera, C.; Corzo, J.E.; Lomas, J.M.; Pasquau, J.; et al. Impact of an evidence-based bundle intervention in the quality-of-care management and outcome of Staphylococcus aureus bacteremia. Clin. Infect. Dis. 2013, 57, 1225–1233. [Google Scholar] [CrossRef] [Green Version]
- Lee Rachael, A.; Joanna, Z.; Camins, B.C.; Griffin, R.L.; Martin Rodriguez, J.; McCarty, T.P.; Magadia, J.; Pappas, P.G. Impact of infectious disease consultation on clinical management and mortality in patients with candidemia. Clin. Infect. Dis. 2018, 68, 1585–1587. [Google Scholar] [CrossRef]
- Penfold, R.B.; Zhang, F. Use of interrupted time series analysis in evaluating health care quality improvements. Acad. Pediatr. 2013, 13, S38–S44. [Google Scholar] [CrossRef]
- Kim, H.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Outcomes | Pre-Intervention Trend | Change in Level a | Change in Trend b | Relative Effect c % |
|---|---|---|---|---|
| Total J01+J02 | 1.83 (−2.14 to 5.80) | −13.98 (−35.65 to 7.69) | −3.52 (−7.57 to 0.52) | −62.3 (−84.5 to −40.1) |
| Total antibiotics (J01) | −0.65 (−2.84 to 1.54) | −17.22 (−29.17 to −5.28) | −0.27 (−2.49 to 1.95) | −32.4 (−99.2 to 34.5) |
| Total antifungals (J02) | 2.54 (−0.12 to 5.20) | 3.31 (−11.12 to 17.74) | −3.32 (−6.04 to −0.60) | −80.4 (−90.9 to −69.9) |
| Carbapenems | −0.01 (−0.69 to 0.66) | −0.67 (−4.33 to 2.99) | −0.20 (−0.89 to 0.49) | −68.8 (−126.0 to −10.6) |
| Piperacillin-tazobactam | 0.63 (−0.25 to 1.51) | 7.78 (3.30 to 12.27) | −0.86 (−1.78 to 0.07) | −67.3 (−96.9 to −38.6) |
| Antipseudomonal cephalosporins | −0.55 (−1.57 to 0.47) | −10.79 (−16.18 to −5.41) | 0.77 (−0.29 to 1.82) | 105.1 (−195.6 to 405.8) |
| Quinolones | 0.16 (−1.16 to 1.47) | −18.45 (−25.29 to −11.62) | −0.45 (−1.82 to 0.93) | −85.0 (−102.0 to −68.1) |
| Amikacin | −0.03 (−0.46 to 0.39) | 1.68 (−0.51 to 3.87) | −0.05 (−0.48 to 0.39) | 0.1 (−410.8 to 413.6) |
| Glycopeptides | 0.01 (−0.55 to 0.56) | 0.68 (−2.27 to 3.62) | −0.17 (−0.74 to 0.40) | −70.5 (−138.9 to −2.1) |
| Outcomes | Pre-Intervention Trend | Change in Level a | Change in Trend b | Relative Effect c % |
|---|---|---|---|---|
| Incidence density | −0.09 (−0.25 to 0.07) | −0.11 (−1.00 to 0.77) | 0.10 (−0.06 to 0.26) | 98.9 (−301.4 to 499.2) |
| Early mortality | 0.009 (−0.03 to 0.05) | 0.06 (−0.14 to 0.26) | −0.01 (−0.05 to 0.03) | −72.1 (−147.8 to 3.5) |
| Late mortality | 0.01 (−0.06 to 0.08) | −0.03 (−0.42 to 0.36) | −0.005 (−0.08 to 0.07) | −35.55 (−346.9 to 275.8) |
| Outcomes | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | APC (95% CI) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Blood cultures per 1000 OBD | 72 | 71 | 59 | 71 | 100 | 121 | 92 | 100 | 100 | 133 | 102 | 6.014 (2.348 to 9.811) |
| AML | 21 | 33 | 35 | 47 | 35 | 37 | 35 | 29 | 43 | 35 | 37 | 4.400 (−6.186 to 16.279) |
| Admissions | 1005 | 1055 | 1081 | 946 | 1052 | 1148 | 1169 | 1120 | 1133 | 1290 | 1265 | 2.336 (1.253 to 3.430) |
| OBD | 8966 | 9128 | 10,616 | 10,463 | 10,343 | 10,620 | 10,840 | 11,135 | 11,753 | 11,719 | 14,463 | 3.540 (2.358 to 4.735) |
| Length of stay, mean | 16 | 15 | 18 | 17 | 17 | 16 | 16 | 16 | 17 | 14 | 16 | −0.843 (−1.908 to 0.235) |
| Allogeneic HSCT | 19 | 20 | 33 | 40 | 47 | 55 | 56 | 58 | 44 | 43 | 47 | 8.609 (4.436 to 12.948) |
| HSCT−related mortality, % | 5.3 | 5.0 | 0 | 0 | 6.4 | 1.8 | 7.1 | 1.7 | 0 | 2.3 | 2.1 | −7.007 (−16.347 to 3.376) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guisado-Gil, A.B.; Aguilar-Guisado, M.; Peñalva, G.; Lepe, J.A.; Espigado, I.; Rodríguez-Arbolí, E.; González-Campos, J.; Rodríguez-Torres, N.; Montero-Cuadrado, M.I.; Falantes-González, J.F.; et al. Long-Term Impact of an Educational Antimicrobial Stewardship Program on Management of Patients with Hematological Diseases. Antibiotics 2021, 10, 136. https://doi.org/10.3390/antibiotics10020136
Guisado-Gil AB, Aguilar-Guisado M, Peñalva G, Lepe JA, Espigado I, Rodríguez-Arbolí E, González-Campos J, Rodríguez-Torres N, Montero-Cuadrado MI, Falantes-González JF, et al. Long-Term Impact of an Educational Antimicrobial Stewardship Program on Management of Patients with Hematological Diseases. Antibiotics. 2021; 10(2):136. https://doi.org/10.3390/antibiotics10020136
Chicago/Turabian StyleGuisado-Gil, Ana Belén, Manuela Aguilar-Guisado, Germán Peñalva, José Antonio Lepe, Ildefonso Espigado, Eduardo Rodríguez-Arbolí, José González-Campos, Nancy Rodríguez-Torres, María Isabel Montero-Cuadrado, José Francisco Falantes-González, and et al. 2021. "Long-Term Impact of an Educational Antimicrobial Stewardship Program on Management of Patients with Hematological Diseases" Antibiotics 10, no. 2: 136. https://doi.org/10.3390/antibiotics10020136