Analytical Challenges in Diabetes Management: Towards Glycated Albumin Point-of-Care Detection



Abstract
:1. Introduction
2. Glycemic Control Biomarkers
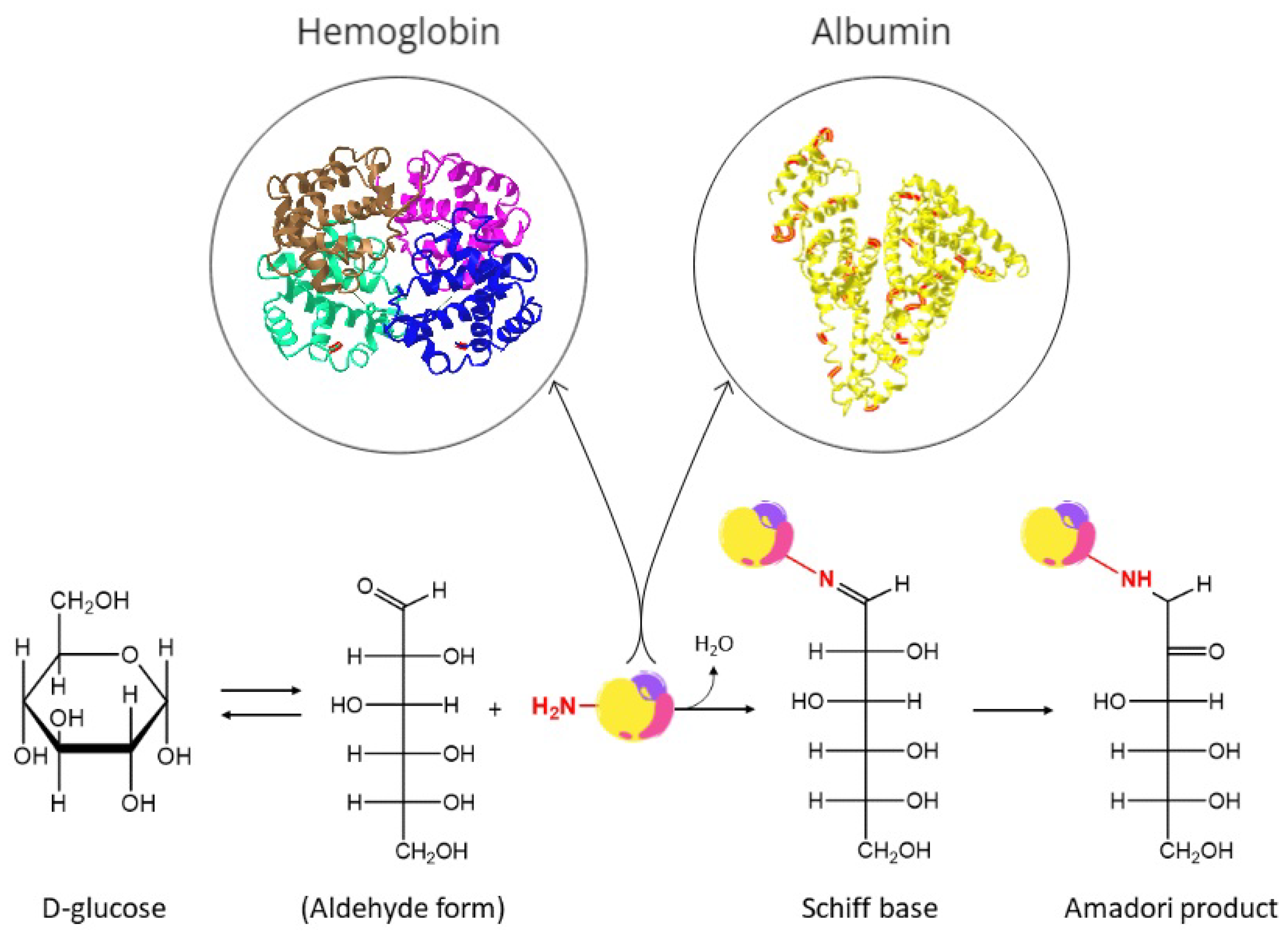
2.1. Glycated Proteins
2.1.1. Glycated Hemoglobin
2.1.2. Glycated Albumin
3. Glycated Albumin Analysis
3.1. Laboratory Techniques
3.2. Experimental Techniques
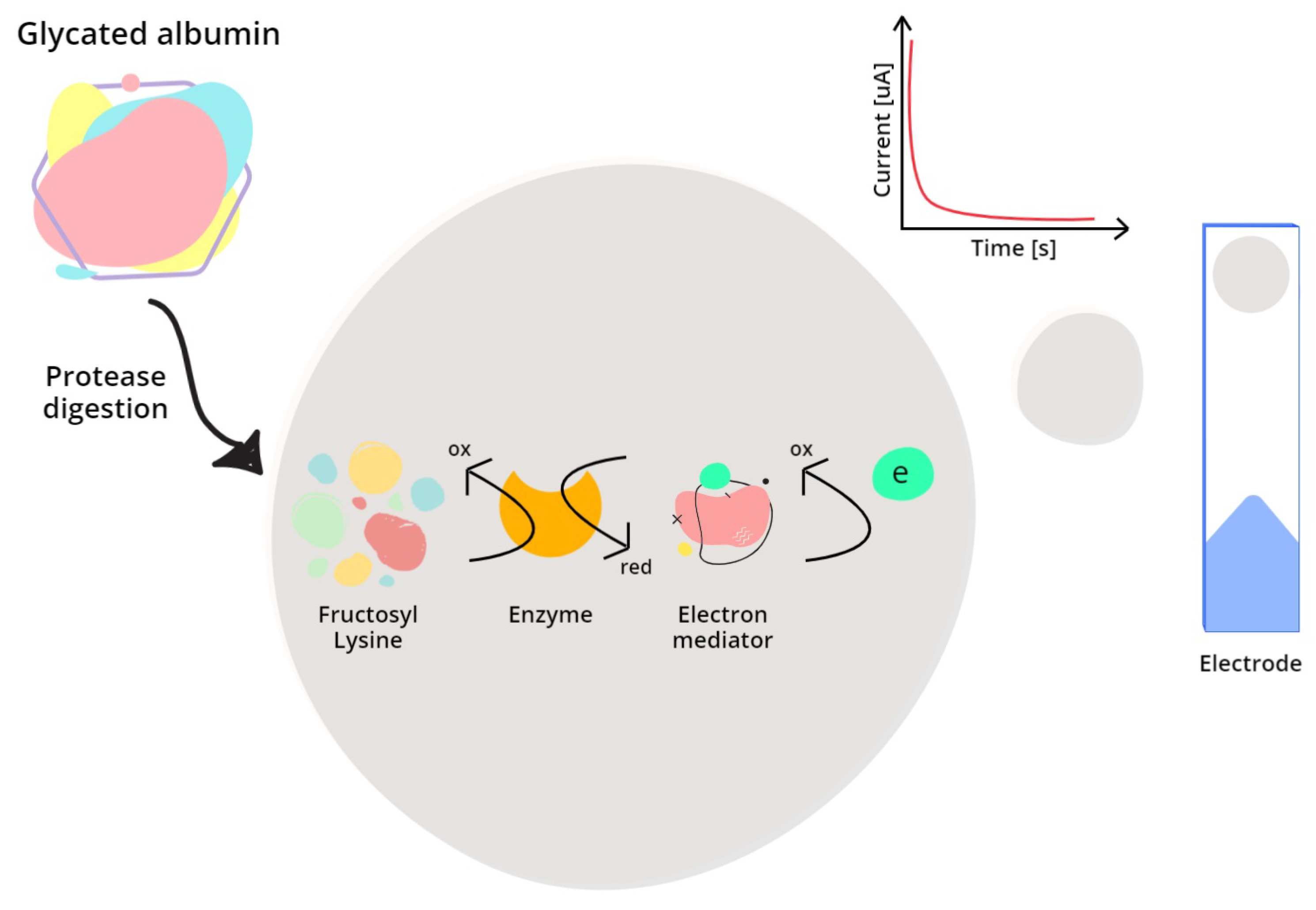
3.2.1. Enzymatic Methods
3.2.2. Affinity Methods
3.2.3. Additional Relevant Approaches
4. Operational and Technological Challenges towards Innovative Point-of-Care Testing for GA Detection
5. Conclusions
- adding GA to traditional glycemic control markers may contribute to improving overall DM monitoring;
- aptamer-based sensors are expected to overcome some issues typical of enzymatic-based sensors, but reading technologies still need to be systematically verified;
- GA-based POC devices are promising and may revolutionize remote glycemic monitoring.
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| -FK | -Fructosyl Lysine |
| AGEs | Advanced Glycation End-products |
| Ag/SiNWs | Silver-coated Silicon Nanowires |
| BGM | Blood Glucose Monitoring |
| BMI | Body Mass Index |
| CGM | Continuous Glucose Monitoring |
| CMOS | Complementary Metal-Oxide Semiconductor |
| DCCT | Diabetes Control and Complications Trial |
| DHFR | Dihydrofolate Reductase |
| DM | Diabetes Mellitus |
| EIS | Electrochemical Impedance Spectroscopy |
| ELISA | Enzyme-Linked Immunosorbent Assay |
| ELBIA | Enzyme-Linked Boronate Immunoassay |
| FAOX | Fructosamine Oxidase |
| Fe | Iron |
| FET | Field Effect Transistor |
| FN6K | Fructosamine 6-Kinase |
| FPG | Fasting Plasma Glucose |
| GA | Glycated Albumin |
| GFP | Green Fluorescent Protein |
| GO | Graphene Oxide |
| HbA1c | Glycated Hemoglobin |
| HPLC | High-Performance Liquid Chromatography |
| HSA | Human Serum Albumin |
| IDEs | Interdigitated Electrodes |
| IFG | Impaired Fasting Glycemia |
| IGT | Impaired Glucose Tolerance |
| LFIA | Lateral Flow Immunoassay |
| LOD | Limit Of Detection |
| OGTT | Oral Glucose Tolerance Test |
| PEDOT | Poly-Ethylenedioxythiophene |
| POC | Point-of-Care |
| POCT | Point-of-Care Testing |
| rGO | Reduced Graphene Oxide |
| SERS | Surface-Enhanced Raman Spectroscopy |
| SiO2 | Silicon Dioxide |
| SPCEs | Screen-Printed Carbon Electrodes |
| SWV | Square Wave Voltammetry |
| UKPDS | UK Prospective Diabetes Study |
| ZnO | Zinc Oxide |
References
- International Diabetes Federation. IDF Diabetes Atlas—10th edition. 2021. Available online: https://diabetesatlas.org/ (accessed on 12 April 2022).
- World Health Organization. Diabetes. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes/ (accessed on 12 April 2022).
- Atkinson, M.A.; Eisenbarth, G.S.; Michels, A.W. Type 1 diabetes. Lancet 2014, 383, 69–82. [Google Scholar] [CrossRef]
- Chatterjee, S.; Khunti, K.; Davies, M.J. Type 2 diabetes. Lancet 2017, 389, 2239–2251. [Google Scholar] [CrossRef]
- McIntyre, H.D.; Catalano, P.; Zhang, C.; Desoye, G.; Mathiesen, E.R.; Damm, P. Gestational diabetes mellitus. Nat. Rev. Dis. Prim. 2019, 5, 47. [Google Scholar] [CrossRef] [PubMed]
- Farrar, D. Hyperglycemia in pregnancy: Prevalence, impact, and management challenges. Int. J. Women’s Health 2016, 8, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Unwin, N.; Shaw, J.; Zimmet, P.; Alberti, K.G.M.M. Impaired glucose tolerance and impaired fasting glycaemia: The current status on definition and intervention. Diabet. Med. J. Br. Diabet. Assoc. 2002, 19, 708–723. [Google Scholar] [CrossRef]
- Buse, J.B.; Caprio, S.; Cefalu, W.T.; Ceriello, A.; Del Prato, S.; Inzucchi, S.E.; McLaughlin, S.; Phillips, G.L.; Robertson, R.P.; Rubino, F.; et al. How Do We Define Cure of Diabetes? Diabetes Care 2009, 32, 2133–2135. [Google Scholar] [CrossRef]
- Morgan, C.L.; Currie, C.J.; Peters, J.R. Relationship between diabetes and mortality: A population study using record linkage. Diabetes Care 2000, 23, 1103–1107. [Google Scholar] [CrossRef]
- Young, B.A.; Lin, E.; Von Korff, M.; Simon, G.; Ciechanowski, P.; Ludman, E.J.; Everson-Stewart, S.; Kinder, L.; Oliver, M.; Boyko, E.J.; et al. Diabetes complications severity index and risk of mortality, hospitalization, and healthcare utilization. Am. J. Manag. Care 2008, 14, 15–23. [Google Scholar]
- Koga, M. Glycated albumin; clinical usefulness. Clin. Chim. Acta 2014, 433, 96–104. [Google Scholar] [CrossRef]
- Inaba, M.; Okuno, S.; Kumeda, Y.; Yamada, S.; Imanishi, Y.; Tabata, T.; Okamura, M.; Okada, S.; Yamakawa, T.; Ishimura, E.; et al. Glycated Albumin Is a Better Glycemic Indicator than Glycated Hemoglobin Values in Hemodialysis Patients with Diabetes: Effect of Anemia and Erythropoietin Injection. J. Am. Soc. Nephrol. 2007, 18, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Peacock, T.; Shihabi, Z.; Bleyer, A.; Dolbare, E.; Byers, J.; Knovich, M.; Calles-Escandon, J.; Russell, G.; Freedman, B. Comparison of glycated albumin and hemoglobin A1c levels in diabetic subjects on hemodialysis. Kidney Int. 2008, 73, 1062–1068. [Google Scholar] [CrossRef] [Green Version]
- Hay-Lombardie, A.; Kamel, S.; Bigot-Corbel, E. Le point sur l’albumine glyquée. Ann. Biol. Clin. 2019, 77, 407–414. [Google Scholar] [CrossRef]
- Zendjabil, M. Glycated albumin. Clin. Chim. Acta 2020, 502, 240–244. [Google Scholar] [CrossRef] [PubMed]
- Giglio, R.V.; Lo Sasso, B.; Agnello, L.; Bivona, G.; Maniscalco, R.; Ligi, D.; Mannello, F.; Ciaccio, M. Recent Updates and Advances in the Use of Glycated Albumin for the Diagnosis and Monitoring of Diabetes and Renal, Cerebro- and Cardio-Metabolic Diseases. J. Clin. Med. 2020, 9, 3634. [Google Scholar] [CrossRef] [PubMed]
- Yazdanpanah, S.; Rabiee, M.; Tahriri, M.; Abdolrahim, M.; Rajab, A.; Jazayeri, H.E.; Tayebi, L. Evaluation of glycated albumin (GA) and GA/HbA1c ratio for diagnosis of diabetes and glycemic control: A comprehensive review. Crit. Rev. Clin. Lab. Sci. 2017, 54, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, K.; Sakamoto, Y.; Kawasaki, Y.; Miyake, T.; Tanaka, K.; Urata, T.; Katayama, Y.; Ueda, S.; Horiuchi, S. Determination of glycated albumin by enzyme-linked boronate immunoassay (ELBIA). Clin. Chem. 1998, 44, 256–263. [Google Scholar] [CrossRef]
- Kohzuma, T.; Koga, M. Lucica® GA-L Glycated Albumin Assay Kit. Mol. Diagn. Ther. 2010, 14, 49–51. [Google Scholar] [CrossRef]
- Bohli, N.; Chammem, H.; Meilhac, O.; Mora, L.; Abdelghani, A. Electrochemical Impedance Spectroscopy on Interdigitated Gold Microelectrodes for Glycosylated Human Serum Albumin Characterization. IEEE Trans. Nanobiosci. 2017, 16, 676–681. [Google Scholar] [CrossRef]
- Bunyarataphan, S.; Dharakul, T.; Fucharoen, S.; Paiboonsukwong, K.; Japrung, D. Glycated Albumin Measurement Using an Electrochemical Aptasensor for Screening and Monitoring of Diabetes Mellitus. Electroanalysis 2019, 31, 2254–2261. [Google Scholar] [CrossRef]
- Farzadfard, A.; Shayeh, J.S.; Habibi-Rezaei, M.; Omidi, M. Modification of reduced graphene/Au-aptamer to develop an electrochemical based aptasensor for measurement of glycated albumin. Talanta 2020, 211, 120722. [Google Scholar] [CrossRef]
- Waiwinya, W.; Putnin, T.; Pimalai, D.; Chawjiraphan, W.; Sathirapongsasuti, N.; Japrung, D. Immobilization-Free Electrochemical Sensor Coupled with a Graphene-Oxide-Based Aptasensor for Glycated Albumin Detection. Biosensors 2021, 11, 85. [Google Scholar] [CrossRef] [PubMed]
- Attar, A.M.; Richardson, M.B.; Speciale, G.; Majumdar, S.; Dyer, R.P.; Sanders, E.C.; Penner, R.M.; Weiss, G.A. Electrochemical Quantification of Glycated and Non-glycated Human Serum Albumin in Synthetic Urine. ACS Appl. Mater. Interfaces 2019, 11, 4757–4765. [Google Scholar] [CrossRef]
- Hatada, M.; Wilson, E.; Khanwalker, M.; Probst, D.; Okuda-Shimazaki, J.; Sode, K. Current and future prospective of biosensing molecules for point-of-care sensors for diabetes biomarker. Sens. Actuators Chem. 2022, 351, 130914. [Google Scholar] [CrossRef]
- Albisser, A.M.; Leibel, B.S.; Ewart, T.G.; Davidovac, Z.; Botz, C.K.; Zingg, W.; Schipper, H.; Gander, R. Clinical Control of Diabetes by the Artificial Pancreas. Diabetes 1974, 23, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Nelson, C.J. A Guide to Glucose Urine Testing Systems: For the Pharmacist Teaching the Diabetic Patient. Drug Intell. Clin. Pharm. 1974, 8, 422–429. [Google Scholar] [CrossRef]
- McArthur, R.G.; Tomm, K.M.; Leahey, M.D. Management of diabetes mellitus in children. Can. Med. Assoc. J. 1976, 114, 783–787. [Google Scholar]
- Goldstein, D.E.; Little, R.R.; Lorenz, R.A.; Malone, J.I.; Nathan, D.; Peterson, C.M.; Sacks, D.B. Tests of Glycemia in Diabetes. Diabetes Care 2004, 27, 1761–1773. [Google Scholar] [CrossRef]
- Laffel, L. Ketone bodies: A review of physiology, pathophysiology and application of monitoring to diabetes. Diabetes Metab. Res. Rev. 1999, 15, 412–426. [Google Scholar] [CrossRef]
- Clarke, W.L.; Cox, D.; Gonder-Frederick, L.A.; Carter, W.; Pohl, S.L. Evaluating Clinical Accuracy of Systems for Self-Monitoring of Blood Glucose. Diabetes Care 1987, 10, 622–628. [Google Scholar] [CrossRef]
- American Diabetes Association. Self-Monitoring of Blood Glucose. Diabetes Care 1994, 17, 81–86. [Google Scholar] [CrossRef]
- Walford, S.; Gale, E.; Allison, S.; Tattersall, R. SELF-MONITORING OF BLOOD-GLUCOSE: Improvement of Diabetic Control. Lancet 1978, 311, 732–735. [Google Scholar] [CrossRef]
- Hayford, J.T.; Weydert, J.A.; Thompson, R.G. Validity of Urine Glucose Measurements for Estimating Plasma Glucose Concentration. Diabetes Care 1983, 6, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Morris, L.R.; McGee, J.A.; Kitabchi, A.E. Correlation Between Plasma and Urine Glucose in Diabetes. Ann. Intern. Med. 1981, 94, 469–471. [Google Scholar] [CrossRef] [PubMed]
- Walford, S.; McB Page, M.; Allison, S.P. The Influence of Renal Threshold on the Interpretation of Urine Tests for Glucose in Diabetic Patients. Diabetes Care 1980, 3, 672–674. [Google Scholar] [CrossRef]
- American Diabetes Association. Urine Glucose and Ketone Determinations. Diabetes Care 1992, 15, 38. [Google Scholar] [CrossRef]
- The Diabetes Control and Complications Trial Research Group. The Effect of Intensive Treatment of Diabetes on the Development and Progression of Long-Term Complications in Insulin-Dependent Diabetes Mellitus. N. Engl. J. Med. 1993, 329, 977–986. [Google Scholar] [CrossRef]
- American Diabetes Association. Implications of the Diabetes Control and Complications Trial. Diabetes Care 2002, 25, s25–s27. [Google Scholar] [CrossRef]
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998, 352, 837–853. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee. 6. Glycemic Targets: Standards of Medical Care in Diabetes—2022. Diabetes Care 2021, 45, S83–S96. [Google Scholar] [CrossRef]
- Thorpe, S.R.; Baynes, J.W. Maillard reaction products in tissue proteins: New products and new perspectives. Amino Acids 2003, 25, 275–281. [Google Scholar] [CrossRef]
- Singh, V.P.; Bali, A.; Singh, N.; Jaggi, A.S. Advanced Glycation End Products and Diabetic Complications. Korean J. Physiol. Pharmacol. 2014, 18, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Freitas, P.A.C.; Ehlert, L.R.; Camargo, J.L. Glycated albumin: A potential biomarker in diabetes. Arch. Endocrinol. Metab. 2017, 61, 296–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohzuma, T.; Tao, X.; Koga, M. Glycated albumin as biomarker: Evidence and its outcomes. J. Diabetes Its Complicat. 2021, 35, 108040. [Google Scholar] [CrossRef] [PubMed]
- Pohanka, M. Glycated Hemoglobin and Methods for Its Point of Care Testing. Biosensors 2021, 11, 70. [Google Scholar] [CrossRef]
- Shapiro, R.; McManus, M.J.; Zalut, C.; Bunn, H.F. Sites of nonenzymatic glycosylation of human hemoglobin A. J. Biol. Chem. 1980, 255, 3120–3127. [Google Scholar] [CrossRef]
- Wang, S.H.; Wang, T.F.; Wu, C.H.; Chen, S.H. In-Depth Comparative Characterization of Hemoglobin Glycation in Normal and Diabetic Bloods by LC-MSMS. J. Am. Soc. Mass Spectrom. 2014, 25, 758–766. [Google Scholar] [CrossRef]
- Shemin, D.; Rittenberg, D. The life span of the human red blood cell. J. Biol. Chem. 1946, 166, 627–636. [Google Scholar] [CrossRef]
- Cohen, R.M.; Franco, R.S.; Khera, P.K.; Smith, E.P.; Lindsell, C.J.; Ciraolo, P.J.; Palascak, M.B.; Joiner, C.H. Red cell life span heterogeneity in hematologically normal people is sufficient to alter HbA1c. Blood 2008, 112, 4284–4291. [Google Scholar] [CrossRef]
- Franco, R.S. Measurement of Red Cell Lifespan and Aging. Transfus. Med. Hemotherapy 2012, 39, 302–307. [Google Scholar] [CrossRef]
- Koga, M.; Kasayama, S. Clinical impact of glycated albumin as another glycemic control marker. Endocr. J. 2010, 57, 751–762. [Google Scholar] [CrossRef]
- Yoshiuchi, K.; Matsuhisa, M.; Katakami, N.; Nakatani, Y.; Sakamoto, K.; Matsuoka, T.; Umayahara, Y.; Kosugi, K.; Kaneto, H.; Yamasaki, Y.; et al. Glycated Albumin is a Better Indicator for Glucose Excursion than Glycated Hemoglobin in Type 1 and Type 2 Diabetes. Endocr. J. 2008, advpub, 0804280122. [Google Scholar] [CrossRef] [PubMed]
- Murai, J.; Soga, S.; Saito, H.; Koga, M. Usefulness of glycated albumin for early detection of deterioration of glycemic control state after discharge from educational admission. Endocr. J. 2013, 60, 409–413. [Google Scholar] [CrossRef] [Green Version]
- Xiong, J.Y.; Wang, J.M.; Zhao, X.L.; Yang, C.; Jiang, X.S.; Chen, Y.M.; Chen, C.Q.; Li, Z.Y. Glycated albumin as a biomarker for diagnosis of diabetes mellitus: A systematic review and meta-analysis. World J. Clin. Cases 2021, 9, 9520–9534. [Google Scholar] [CrossRef] [PubMed]
- Khera, P.K.; Joiner, C.H.; Carruthers, A.; Lindsell, C.J.; Smith, E.P.; Franco, R.S.; Holmes, Y.R.; Cohen, R.M. Evidence for Interindividual Heterogeneity in the Glucose Gradient Across the Human Red Blood Cell Membrane and Its Relationship to Hemoglobin Glycation. Diabetes 2008, 57, 2445–2452. [Google Scholar] [CrossRef]
- Anguizola, J.; Matsuda, R.; Barnaby, O.S.; Hoy, K.; Wa, C.; DeBolt, E.; Koke, M.; Hage, D.S. Review: Glycation of human serum albumin. Clin. Chim. Acta 2013, 425, 64–76. [Google Scholar] [CrossRef]
- Rabbani, G.; Ahn, S.N. Structure, enzymatic activities, glycation and therapeutic potential of human serum albumin: A natural cargo. Int. J. Biol. Macromol. 2019, 123, 979–990. [Google Scholar] [CrossRef] [PubMed]
- Belinskaia, D.A.; Voronina, P.A.; Batalova, A.A.; Goncharov, N.V. Serum Albumin. Encyclopedia 2021, 1, 65–75. [Google Scholar] [CrossRef]
- Soboleva, A.; Mavropulo-Stolyarenko, G.; Karonova, T.; Thieme, D.; Hoehenwarter, W.; Ihling, C.; Stefanov, V.; Grishina, T.; Frolov, A. Multiple Glycation Sites in Blood Plasma Proteins as an Integrated Biomarker of Type 2 Diabetes Mellitus. Int. J. Mol. Sci. 2019, 20, 2329. [Google Scholar] [CrossRef]
- Suwa, T.; Ohta, A.; Matsui, T.; Koganei, R.; Kato, H.; Kawata, T.; Sada, Y.; Ishii, S.; Kondo, A.; Murakami, K.; et al. Relationship between Clinical Markers of Glycemia and Glucose Excursion Evaluated by Continuous Glucose Monitoring (CGM). Endocr. J. 2010, 57, 135–140. [Google Scholar] [CrossRef]
- Koga, M.; Murai, J.; Saito, H.; Kasayama, S.; Imagawa, A.; Hanafusa, T.; Kobayashi, T.; The Members of the Japan Diabetes Society’s Committee on Research on Type 1 Diabetes. Serum glycated albumin to haemoglobin A1C ratio can distinguish fulminant type 1 diabetes mellitus from type 2 diabetes mellitus. Ann. Clin. Biochem. 2010, 47, 313–317. [Google Scholar] [CrossRef]
- Koga, M.; Inada, S.; Nakao, T.; Kawamori, R.; Kasayama, S. The Glycated Albumin (GA) to HbA1c Ratio Reflects Shorter-Term Glycemic Control than GA: Analysis of Patients with Fulminant Type 1 Diabetes. J. Clin. Lab. Anal. 2017, 31, e22023. [Google Scholar] [CrossRef]
- Hellman, R. When are HBA1C Values Misleading? AACE Clin. Case Rep. 2016, 2, e377–e379. [Google Scholar] [CrossRef] [Green Version]
- Silva, J.F.; Pimentel, A.L.; Camargo, J.L. Effect of iron deficiency anaemia on HbA1c levels is dependent on the degree of anaemia. Clin. Biochem. 2016, 49, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Bry, L.; Chen, P.C.; Sacks, D.B. Effects of Hemoglobin Variants and Chemically Modified Derivatives on Assays for Glycohemoglobin. Clin. Chem. 2001, 47, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, K.; Noguchi, S.; Morimoto, Y.; Hamada, S.; Wasada, K.; Imai, S.; Murata, Y.; Kasayama, S.; Koga, M. A1C but Not Serum Glycated Albumin Is Elevated in Late Pregnancy Owing to Iron Deficiency. Diabetes Care 2008, 31, 1945–1948. [Google Scholar] [CrossRef]
- Hashimoto, K.; Osugi, T.; Noguchi, S.; Morimoto, Y.; Wasada, K.; Imai, S.; Waguri, M.; Toyoda, R.; Fujita, T.; Kasayama, S.; et al. A1C but Not Serum Glycated Albumin Is Elevated Because of Iron Deficiency in Late Pregnancy in Diabetic Women. Diabetes Care 2009, 33, 509–511. [Google Scholar] [CrossRef]
- Zheng, C.M.; Ma, W.Y.; Wu, C.C.; Lu, K.C. Glycated albumin in diabetic patients with chronic kidney disease. Clin. Chim. Acta 2012, 413, 1555–1561. [Google Scholar] [CrossRef]
- Furusyo, N.; Hayashi, J. Glycated albumin and diabetes mellitus. Biochim. Biophys. Acta Gen. Subj. 2013, 1830, 5509–5514. [Google Scholar] [CrossRef]
- Bhonsle, H.S.; Korwar, A.M.; Kote, S.S.; Golegaonkar, S.B.; Chougale, A.D.; Shaik, M.L.; Dhande, N.L.; Giri, A.P.; Shelgikar, K.M.; Boppana, R.; et al. Low Plasma Albumin Levels Are Associated with Increased Plasma Protein Glycation and HbA1c in Diabetes. J. Proteome Res. 2012, 11, 1391–1396. [Google Scholar] [CrossRef]
- Koga, M.; Kasayama, S.; Kanehara, H.; Bando, Y. CLD (chronic liver diseases)-HbA1C as a suitable indicator for estimation of mean plasma glucose in patients with chronic liver diseases. Diabetes Res. Clin. Pract. 2008, 81, 258–262. [Google Scholar] [CrossRef]
- Koga, M.; Murai, J.; Saito, H.; Matsumoto, S.; Kasayama, S. Effects of thyroid hormone on serum glycated albumin levels: Study on non-diabetic subjects. Diabetes Res. Clin. Pract. 2009, 84, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Okada, T.; Nakao, T.; Matsumoto, H.; Nagaoka, Y.; Tomaru, R.; Iwasawa, H.; Wada, T. Influence of Proteinuria on Glycated Albumin Values in Diabetic Patients with Chronic Kidney Disease. Intern. Med. 2011, 50, 23–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Xing, G.; Zhang, L. Chapter Eighteen—Glycated albumin level is significantly decreased in patients suffering nephrotic syndrome. In Glycans and Glycosaminoglycans as Clinical Biomarkers and Therapeutics—Part A; Progress in Molecular Biology and Translational Science; Zhang, L., Ed.; Academic Press: Cambridge, MA, USA, 2019; Volume 162, pp. 307–319. [Google Scholar] [CrossRef]
- Koga, M.; Matsumoto, S.; Saito, H.; Kasayama, S. Body Mass Index Negatively Influences Glycated Albumin, but not Glycated Hemoglobin, in Diabetic Patients. Endocr. J. 2006, advpub, 0605220014. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Mo, Y.; Ma, X.; Ying, L.; Zhu, W.; Wang, Y.; Bao, Y.; Zhou, J. Associations of body mass index with glycated albumin and glycated albumin/glycated hemoglobin A1c ratio in Chinese diabetic and non-diabetic populations. Clin. Chim. Acta 2018, 484, 117–121. [Google Scholar] [CrossRef]
- Suzuki, S.; Koga, M.; Niizeki, N.; Furuya, A.; Takahashi, H.; Matsuo, K.; Tanahashi, Y.; Kawata, Y.; Asai, H.; Tsuchida, E.; et al. Glycated albumin is lower in infants than in adults and correlated with both age and serum albumin. Pediatr. Diabetes 2013, 14, 25–30. [Google Scholar] [CrossRef]
- Zhou, Q.; Shi, D.B.; Lv, L.Y. The establishment of biological reference intervals of nontraditional glycemic markers in a Chinese population. J. Clin. Lab. Anal. 2017, 31, e22097. [Google Scholar] [CrossRef]
- Bellia, C.; Zaninotto, M.; Cosma, C.; Agnello, L.; Sasso, B.L.; Bivona, G.; Plebani, M.; Ciaccio, M. Definition of the upper reference limit of glycated albumin in blood donors from Italy. Clin. Chem. Lab. Med. CCLM 2018, 56, 120–125. [Google Scholar] [CrossRef]
- Japanese Diabetes Society. Treatment Guide for Diabetes 2016–2017. 2016. Available online: http://www.fa.kyorin.co.jp/jds/uploads/Treatment_Guide_for_Diabetes_2016-2017.pdf (accessed on 24 April 2022).
- Roohk, H.V.; Zaidi, A.R. A Review of Glycated Albumin as an Intermediate Glycation Index for Controlling Diabetes. J. Diabetes Sci. Technol. 2008, 2, 1114–1121. [Google Scholar] [CrossRef]
- Guthrow, C.E.; Morris, M.A.; Day, J.F.; Thorpe, S.R.; Baynes, J.W. Enhanced nonenzymatic glucosylation of human serum albumin in diabetes mellitus. Proc. Natl. Acad. Sci. USA 1979, 76, 4258–4261. [Google Scholar] [CrossRef]
- Ney, K.A.; Colley, K.J.; Pizzo, S.V. The standardization of the thiobarbituric acid assay for nonenzymatic glucosylation of human serum albumin. Anal. Biochem. 1981, 118, 294–300. [Google Scholar] [CrossRef]
- Dolhofer, R.; Wieland, O. Improvement of the thiobarbituric acid assay for serum glycosylprotein determination. Clin. Chim. Acta 1981, 112, 197–204. [Google Scholar] [CrossRef]
- Mashiba, S.; Uchida, K.; Okuda, S.; Tomita, S. Measurement of glycated albumin by the nitroblue tetrazolium colorimetric method. Clin. Chim. Acta 1992, 212, 3–15. [Google Scholar] [CrossRef]
- Kobayashi, K.; Yoshimoto, K.; Hirauchi, K.; Uchida, K. Determination of Glycated Proteins in Biological Samples Based on Colorimetry of 2-Keto-glucose Released with Hydrazine. Biol. Pharm. Bull. 1994, 17, 365–369. [Google Scholar] [CrossRef] [PubMed]
- Day, J.; Thorpe, S.; Baynes, J. Nonenzymatically glucosylated albumin. In vitro preparation and isolation from normal human serum. J. Biol. Chem. 1979, 254, 595–597. [Google Scholar] [CrossRef]
- Leblanc, Y.; Bihoreau, N.; Chevreux, G. Characterization of Human Serum Albumin isoforms by ion exchange chromatography coupled online to native mass spectrometry. J. Chromatogr. B 2018, 1095, 87–93. [Google Scholar] [CrossRef]
- Yatscoff, R.W.; Tevaarwerk, G.J.; MacDonald, J.C. Quantification of nonenzymically glycated albumin and total serum protein by affinity chromatography. Clin. Chem. 1984, 30, 446–449. [Google Scholar] [CrossRef]
- Yasukawa, K.; Abe, F.; Shida, N.; Koizumi, Y.; Uchida, T.; Noguchi, K.; Shima, K. High-performance affinity chromatography system for the rapid, efficient assay of glycated albumin. J. Chromatogr. A 1992, 597, 271–275. [Google Scholar] [CrossRef]
- Shima, K.; Ito, N.; Abe, F.; Hirota, M.; Yano, M.; Yamamoto, Y.; Uchida, T.; Noguchi, K. High-performance liquid chromatographic assay of serum glycated albumin. Diabetologia 1988, 31, 627–631. [Google Scholar] [CrossRef]
- Cohen, M.P.; Hud, E. Measurement of plasma glycoalbumin levels with a monoclonal antibody based ELISA. J. Immunol. Methods 1989, 122, 279–283. [Google Scholar] [CrossRef]
- Paroni, R.; Ceriotti, F.; Galanello, R.; Battista Leoni, G.; Panico, A.; Scurati, E.; Paleari, R.; Chemello, L.; Quaino, V.; Scaldaferri, L.; et al. Performance characteristics and clinical utility of an enzymatic method for the measurement of glycated albumin in plasma. Clin. Biochem. 2007, 40, 1398–1405. [Google Scholar] [CrossRef]
- Testa, R.; Guerra, E.; Bonfigli, A.R.; Di Gaetano, N.; Santini, G.; Ceriotti, F. Analytical Performances of an Enzymatic Assay for the Measurement of Glycated Albumin. J. Appl. Lab. Med. 2016, 1, 162–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paleari, R.; Bonetti, G.; Callà, C.; Carta, M.; Ceriotti, F.; Di Gaetano, N.; Ferri, M.; Guerra, E.; Lavalle, G.; Cascio, C.L.; et al. Multicenter evaluation of an enzymatic method for glycated albumin. Clin. Chim. Acta 2017, 469, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, M.; Kambe, S.; Eto, T.; Yamakoshi, M.; Kouzuma, T.; Suzuki, N. Point of care testing system via enzymatic method for the rapid, efficient assay of glycated albumin. Biosens. Bioelectron. 2005, 21, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Hatada, M.; Tsugawa, W.; Kamio, E.; Loew, N.; Klonoff, D.C.; Sode, K. Development of a screen-printed carbon electrode based disposable enzyme sensor strip for the measurement of glycated albumin. Biosens. Bioelectron. 2017, 88, 167–173. [Google Scholar] [CrossRef]
- Hatada, M.; Loew, N.; Okuda-Shimazaki, J.; Khanwalker, M.; Tsugawa, W.; Mulchandani, A.; Sode, K. Development of an Interdigitated Electrode-Based Disposable Enzyme Sensor Strip for Glycated Albumin Measurement. Molecules 2021, 26, 734. [Google Scholar] [CrossRef]
- Kameya, M.; Tsugawa, W.; Yamada-Tajima, M.; Hatada, M.; Suzuki, K.; Sakaguchi-Mikami, A.; Ferri, S.; Klonoff, D.C.; Sode, K. Electrochemical sensing system employing fructosamine 6-kinase enables glycated albumin measurement requiring no proteolytic digestion. Biotechnol. J. 2016, 11, 797–804. [Google Scholar] [CrossRef]
- Sasar, M.; Farzadfard, A.; Abdi, Y.; Habibi-Rezaei, M. Detection of Glycated Albumin Using a Novel Field Effect Aptasensor. IEEE Sens. J. 2020, 20, 10387–10392. [Google Scholar] [CrossRef]
- Lee, J.O.; Thus, H.M.; Jeon, E.K.; Chang, H.; Won, K.; Kim, Y.H. Aptamers as molecular recognition elements for electrical nanobiosensors. Anal. Bioanal. Chem. 2008, 390, 1023–1032. [Google Scholar] [CrossRef]
- Song, K.M.; Lee, S.; Ban, C. Aptamers and Their Biological Applications. Sensors 2012, 12, 612–631. [Google Scholar] [CrossRef]
- Jayasena, S.D. Aptamers: An Emerging Class of Molecules That Rival Antibodies in Diagnostics. Clin. Chem. 1999, 45, 1628–1650. [Google Scholar] [CrossRef]
- Apiwat, C.; Luksirikul, P.; Kankla, P.; Pongprayoon, P.; Treerattrakoon, K.; Paiboonsukwong, K.; Fucharoen, S.; Dharakul, T.; Japrung, D. Graphene based aptasensor for glycated albumin in diabetes mellitus diagnosis and monitoring. Biosens. Bioelectron. 2016, 82, 140–145. [Google Scholar] [CrossRef]
- Belsare, S.; Coté, G. Development of a colorimetric paper fluidic dipstick assay for measurement of glycated albumin to monitor gestational diabetes at the point-of-care. Talanta 2021, 223, 121728. [Google Scholar] [CrossRef] [PubMed]
- Ki, H.; Oh, J.; Han, G.R.; Kim, M.G. Glycation ratio determination through simultaneous detection of human serum albumin and glycated albumin on an advanced lateral flow immunoassay sensor. Lab Chip 2020, 20, 844–851. [Google Scholar] [CrossRef] [PubMed]
- Paria, D.; Convertino, A.; Mussi, V.; Maiolo, L.; Barman, I. Silver-Coated Disordered Silicon Nanowires Provide Highly Sensitive Label-Free Glycated Albumin Detection through Molecular Trapping and Plasmonic Hotspot Formation. Adv. Healthc. Mater. 2021, 10, 2001110. [Google Scholar] [CrossRef]
- Coskun, A.F.; Nagi, R.; Sadeghi, K.; Phillips, S.; Ozcan, A. Albumin testing in urine using a smart-phone. Lab Chip 2013, 13, 4231–4238. [Google Scholar] [CrossRef]
- Dantu, V.; Vempati, J.; Srivilliputhur, S. Non-invasive blood glucose monitor based on spectroscopy using a smartphone. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 3695–3698. [Google Scholar] [CrossRef]
- Wang, T.T.; kit Lio, C.; Huang, H.; Wang, R.Y.; Zhou, H.; Luo, P.; Qing, L.S. A feasible image-based colorimetric assay using a smartphone RGB camera for point-of-care monitoring of diabetes. Talanta 2020, 206, 120211. [Google Scholar] [CrossRef]
- Kap, O.; Kılıç, V.; Hardy, J.G.; Horzum, N. Smartphone-based colorimetric detection systems for glucose monitoring in the diagnosis and management of diabetes. Analyst 2021, 146, 2784–2806. [Google Scholar] [CrossRef] [PubMed]
- Bruininks, B.; Juurlink, L.B.F. An Inexpensive 3D Printed Periscope-Type Smartphone-Based Spectrophotometer for Emission, Absorption, and Fluorescence Spectrometry. J. Chem. Educ. 2022, 99, 2168–2174. [Google Scholar] [CrossRef]
- McCracken, K.E.; Yoon, J.Y. Recent approaches for optical smartphone sensing in resource-limited settings: A brief review. Anal. Methods 2016, 8, 6591–6601. [Google Scholar] [CrossRef]
- Zhang, D.; Liu, Q. Biosensors and bioelectronics on smartphone for portable biochemical detection. Biosens. Bioelectron. 2016, 75, 273–284. [Google Scholar] [CrossRef]
- Lan, Y.; He, B.; Tan, C.S.; Ming, D. Applications of Smartphone-Based Aptasensor for Diverse Targets Detection. Biosensors 2022, 12, 477. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, I.B.; Farkas-Hirsch, R.; Skyler, J.S. Intensive Insulin Therapy for Treatment of Type I Diabetes. Diabetes Care 1990, 13, 1265–1283. [Google Scholar] [CrossRef] [PubMed]
- Koga, M.; Kanehara, H.; Bando, Y.; Morita, S.; Kasayama, S. Is glycated albumin useful for differential diagnosis between fulminant type 1 diabetes mellitus and acute-onset autoimmune type 1 diabetes mellitus? Clin. Chim. Acta 2015, 451, 297–300. [Google Scholar] [CrossRef] [PubMed]
- Inoue, Y.; Inoue, M.; Saito, M.; Yoshikawa, H.; Tamiya, E. Sensitive Detection of Glycated Albumin in Human Serum Albumin Using Electrochemiluminescence. Anal. Chem. 2017, 89, 5909–5915. [Google Scholar] [CrossRef]
- Murtaza, G.; Rizvi, A.S.; Irfan, M.; Li, L.; Qu, F. Determination of glycated albumin in serum and saliva by capillary electrophoresis utilizing affinity of 3-acrylamido phenylboronic acid selected by virtual screening and molecular docking. J. Chromatogr. A 2021, 1636, 461793. [Google Scholar] [CrossRef]
- Khoury, Z.; Illesca, P.; Sultan, A. Salivary Fructosamine as a Noninvasive Glycemic Biomarker: A Systematic Review. JDR Clin. Transl. Res. 2021, 6, 382–389. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | Main Criterion | Alternative Criteria |
|---|---|---|
| Diabetes | FPG 1 ≥ 126 mg/mL | OGTT 2 ≥ 200 mg/mL or HbA1c 3 ≥ 6.5% |
| IGT 4 | FPG 1 < 126 mg/mL with OGTT 2 140–200 mg/mL | |
| IFG 5 | FPG 1 110–125 mg/mL with OGTT 2 < 140 mg/mL |
| Condition | Brief Explanation | Reference |
|---|---|---|
| Intensive insulin therapy | HbA1c levels change too slowly, whereas GA tracks accurately the variations induced by the therapy. | [19] |
| Fulminant type 1 diabetes mellitus | HbA1c is usually normal or only slightly elevated in this clinical condition, whereas the GA/HbA1c ratio significantly increases due to the reactiveness of GA. In this case, the GA/HbA1c is even a better indicator than GA alone. | [62,63] |
| Anemia | Hemolytic anemia shortens the lifespan of erythrocytes hence HbA1c levels are lower, whereas iron deficiency anemia produces higher levels of HbA1c due to enhanced glycation processes and longer red blood cell survivability. Albumin instead is not affected by these pathologies. | [64,65] |
| Variant hemoglobin | The genetic structural variants affect the ability of hemoglobin to be glycated, hence HbA1c does not reflect properly the glycemic status. Albumin instead is not affected by this condition. | [66] |
| Pregnancy | Towards the end of pregnancy, iron deficiency affects HbA1c levels, whereas GA levels remain stable both in diabetic and non diabetic women. | [67,68] |
| Chronic kidney disease | Erythropoietin injections, blood transfusions and hemodialysis are frequent in patients with this condition. They all affect red blood cells’ lifespan and iron values, altering HbA1c levels. Special attention has to be put on proteinuria conditions that may develop in these patients because GA values can be altered. | [12,13,69] |
| Detection Mechanism | Advantages | Disadvantages | Complexity | Deployment Phase | Ref. |
|---|---|---|---|---|---|
| Three different enzymatic reactions on three different strips to analyze GA, total albumin, and ketoamine. Colorimetric evaluation of each strip | Measures both GA and HSA; accounts for ketoamine interference | Bulky; need for temperature control; possible sample evaporation | High | Laboratory | [97] |
| Electrochemical reaction involving an enzyme, FAOX, and -FK as a substrate. Electron transfer is mediated by a ruthenium complex and current vs. time is measured | Very fast measurement (1 min); embeddable | Time-consuming pre-digestion of the sample (long assay time); possible lot-to-lot variations | Moderate | Laboratory | [99] |
| Electrochemical reaction involving an enzyme, FN6K, and intact albumin as a substrate. Electron transfer is mediated by a methylsulfate element and current vs. time is measured | No digestion required; fast assay time (10 min); embeddable | Complex chain of reactions and presence of many solutes with different solubility are important sources of errors | High | Laboratory | [100] |
| Aptamer Sequence 5′-3′ | Modifications | Target | Reference |
|---|---|---|---|
| TGCGGTTGTAGTACTCGTGGCCG | Biotin at 5′ | GA | [21] |
| H8 aptamer 1 | HSA | ||
| GGTGGCTGGAGGGGGCGCGAACGTTTTTTTTTT | Thiol group at 3′ and methylene blue at 5′ | GA | [22] |
| TGCGGTTCGTGCGGTTGTAGTAC | Unmodified | GA | [23] |
| TGCGGTTCGTGCGGTTGTAGTAC | Fluorescein at 5′ | GA | |
| GGTGGCTGGAGGGGGCGCGAACGTTTTTTTTTT | Thiol group at 3′ | GA | [101] |
| Detection Mechanism | Advantages | Disadvantages | Complexity | Deployment Phase | Ref. |
|---|---|---|---|---|---|
| Anti-HSA monoclonal antibodies have been anchored to an electrode surface. The binding with the antigen (HSA or GA) changes the impedance of the sensor | Relatively fast assay time (15 min); embeddable | Possible cross-interference between HSA and GA, both present in a real sample, due to a-specificity of recognition element | Moderate | Laboratory | [20] |
| GA and HSA-specific aptamers immobilized on two different SPCEs. Under applied potential, electron transfer in ferricyanide solution is hindered by aptamer/ligand complex formation and current vs. voltage is measured | Elevated stability (4 weeks); embeddable | Long assay time (40 min) | Moderate | Pre-clinical | [21] |
| rGO and gold nanoparticles-treated electrode surface with methylene blue-modified, GA-specific aptamers immobilized. Under applied potential, electron transfer is hindered by aptamer/ligand complex formation and current vs. voltage is measured | Elimination of electron mediator through modified aptamer | Embeddability: conventional electrochemical cell was used instead of disposable electrodes; complex measurement procedure | High | Laboratory | [22] |
| In the presence of GA, aptamers previously attached to GO sheets in a solution selectively detach from the sheets and bind to the target. Deposition of free GO sheets onto the electrode surface cause changes in the collected current | Does not require immobilization step; relatively fast assay time (30 min); embeddable | Low stability (less than 7 days) | Low | Pre-clinical | [23] |
| FET with thiol-modified, GA-specific aptamers anchored at gold-coated ZnO nanorods deposited on its gate. Ligand/aptamer complex formation induces changes in the conductivity of the FET visible in the source–drain current vs. source–drain voltage plot | Very fast assay time (few minutes); embeddable | The article lacks a clear identification of a calibration curve, as well as information on important parameters such as the LOD for this technology | Moderate | Laboratory | [101] |
| PEDOT-coated electrode coupled with a protein-based recognition element allows the measurement of HSA+GA concentration through impedance analysis; a following enzymatic reaction allows quantification of GA alone by measuring current vs. applied voltage | Measures both GA and HSA; relatively fast assay time (15 min); embeddable | Attention to the stability of recognition element and enzyme is crucial | Moderate | Pre-clinical | [24] |
| Detection Mechanism | Advantages | Disadvantages | Complexity | Deployment Phase | Ref. |
|---|---|---|---|---|---|
| ELISA-like assay based on fluorescent quenching interactions between GO and modified aptamers. In the presence of GA, aptamers detach from GO to bind to target analyte and fluorescent signal previously quenched is restored | Relatively fast assay time (30 min); stability in human serum (DNase resistance) | The readout mechanism can not be easily incorporated in a POC device | Moderate | Pre-clinical | [105] |
| Paper dipstick strip exposing general albumin aptamers to trap albumin. GA or HSA-specific aptamers/gold nanoparticle complex later attaches to the trapped analyte in a sandwich structure that generates a colorimetric signal | The same dipstick can measure either HSA or GA, it is the aptamers/gold nanoparticle complex solution that discriminates the measurement; long-term stability at room temperature (30 days) | The readout mechanism can not be easily incorporated in a POC device | Low | Laboratory | [106] |
| Two-strip LIFA with disconnected bridge structure to separate the loading from the sample solution. Target analyte in the sample solution is captured by specific antibodies and then forms a sandwich structure with a-specific antibodies/gold nanoparticle complex transported by the loading solution to generate a colorimetric signal | Measures both GA and HSA; Relatively fast assay time (30 min) | The readout mechanism can not be easily incorporated in a POC device; multiple injections required | Moderate | Laboratory | [107] |
| Randomly oriented Ag/SiNWs cluster around target molecules and trap them. Raman spectra within these regions provide information on GA concentration in the sample. A chemometric classifier quantifies glycation ratios | Measures both GA and HSA; moderate stability (3 weeks, but signal intensity decreases) | The readout mechanism can not be easily incorporated in a POC device; complex technology (possible high cost) | High | Laboratory | [108] |
| Method | Target | Test Sample | Measurement Range | Technology | Ref. | |
|---|---|---|---|---|---|---|
| Target Absolute Values | Relative GA [%] | |||||
| Enzymatic | GA and HSA | 20 L serum | / | 9.6–20 | Disposable test-strip + portable optical analyzer with temperature control unit and data processing/visualization unit | [97] |
| 0.8 L Z-FK solution | 0.33–3.33 g/dL | / | Disposable IDE + potentiostat (chronoamperometry measurement) | [99] | ||
| GA | 0.8 L reaction mixture | 0.13–0.67 g/dL | / | Disposable SPCE + potentiostat (chronoamperometry measurement) | [100] | |
| Affinity | GA or HSA | n.a. | GA: 0.1–42 g/dL HSA: 0.1–62 g/dL | / | IDE + potentiostat (EIS measurement) | [20] |
| GA or HSA | <1 L diluted plasma | GA: 0.16 g/dL–1.6 g/dL HSA: 5 g/dL-10 g/dL | / | SPCE + potentiostat (SWV measurement) | [21] | |
| GA | 40 L GA solution | 0.2–1 mg/dL | / | Electrochemical cell + potentiostat (SWV measurement) | [22] | |
| GA | 200 L reaction mixture | 1 g/dL–5 mg/dL | / | SPCE + potentiostat (SWV measurement) | [23] | |
| GA | n.a. | 7.7–33.4 mg/dL | / | FET + voltage control and current acquisition system | [101] | |
| GA and HSA | n.a. | GA: 33 g/dL–6.7 mg/dL HSA: 33 g/dL–6.7 mg/dL | 5–80 | PEDOT electrode + potentiostat (SWV measurement) | [24] | |
| GA | Diluted serum | 5–30 mg/dL | / | ELASA assay + spectrometric technology (fluorescence measurement) | [105] | |
| GA or HSA | 25 L reaction mixture in bovine serum | GA: 0–2 g/dL HSA: 0–5 g/dL | / | Paper dipstick assay + optical scanner (colorimetry measurement) | [106] | |
| GA and HSA | 2.5 L sample solution and 130 L loading solution | GA: 100 ng/dL–100 mg/dL HSA: 50 g/dL-360 mg/dL | 5–36 | LFIA + imaging system (colorimetry measurement) | [107] | |
| GA and HSA | n.a. | GA: 3.33 mg/dL-0.67 g/dL | 5–25 | Ag-coated silicon nanowires + laser source and detector (SERS measurement) | [108] | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rescalli, A.; Varoni, E.M.; Cellesi, F.; Cerveri, P. Analytical Challenges in Diabetes Management: Towards Glycated Albumin Point-of-Care Detection. Biosensors 2022, 12, 687. https://doi.org/10.3390/bios12090687
Rescalli A, Varoni EM, Cellesi F, Cerveri P. Analytical Challenges in Diabetes Management: Towards Glycated Albumin Point-of-Care Detection. Biosensors. 2022; 12(9):687. https://doi.org/10.3390/bios12090687
Chicago/Turabian StyleRescalli, Andrea, Elena Maria Varoni, Francesco Cellesi, and Pietro Cerveri. 2022. "Analytical Challenges in Diabetes Management: Towards Glycated Albumin Point-of-Care Detection" Biosensors 12, no. 9: 687. https://doi.org/10.3390/bios12090687