Fluorescence-Based Microendoscopic Sensing System for Minimally Invasive In Vivo Bladder Cancer Diagnosis



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Preparation for BBN-Induced Bladder Cancer
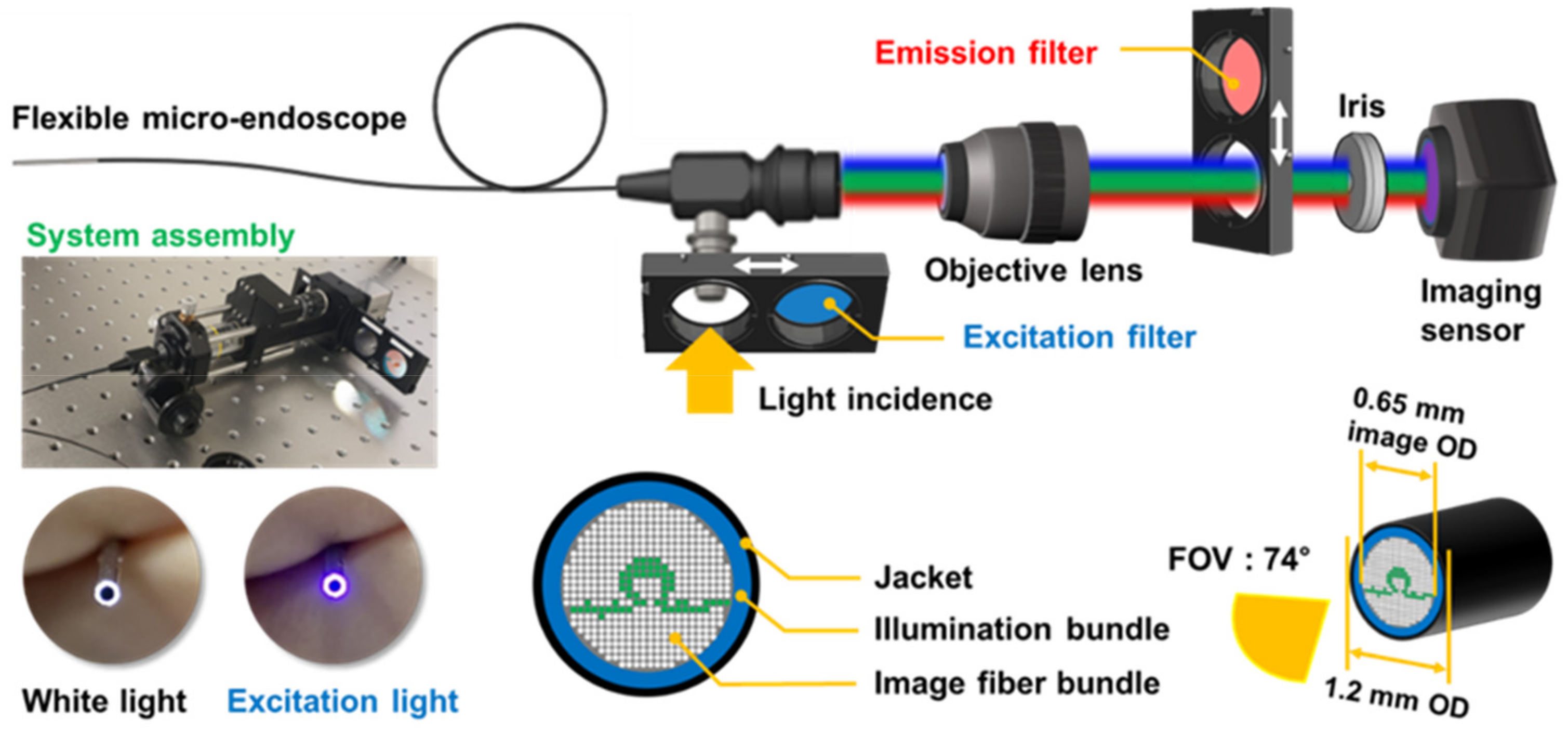
2.2. Preparation of the Microendoscopy-Based Fluorescence Sensing System
2.3. 5-ALA-Induced Fluorescence Imaging
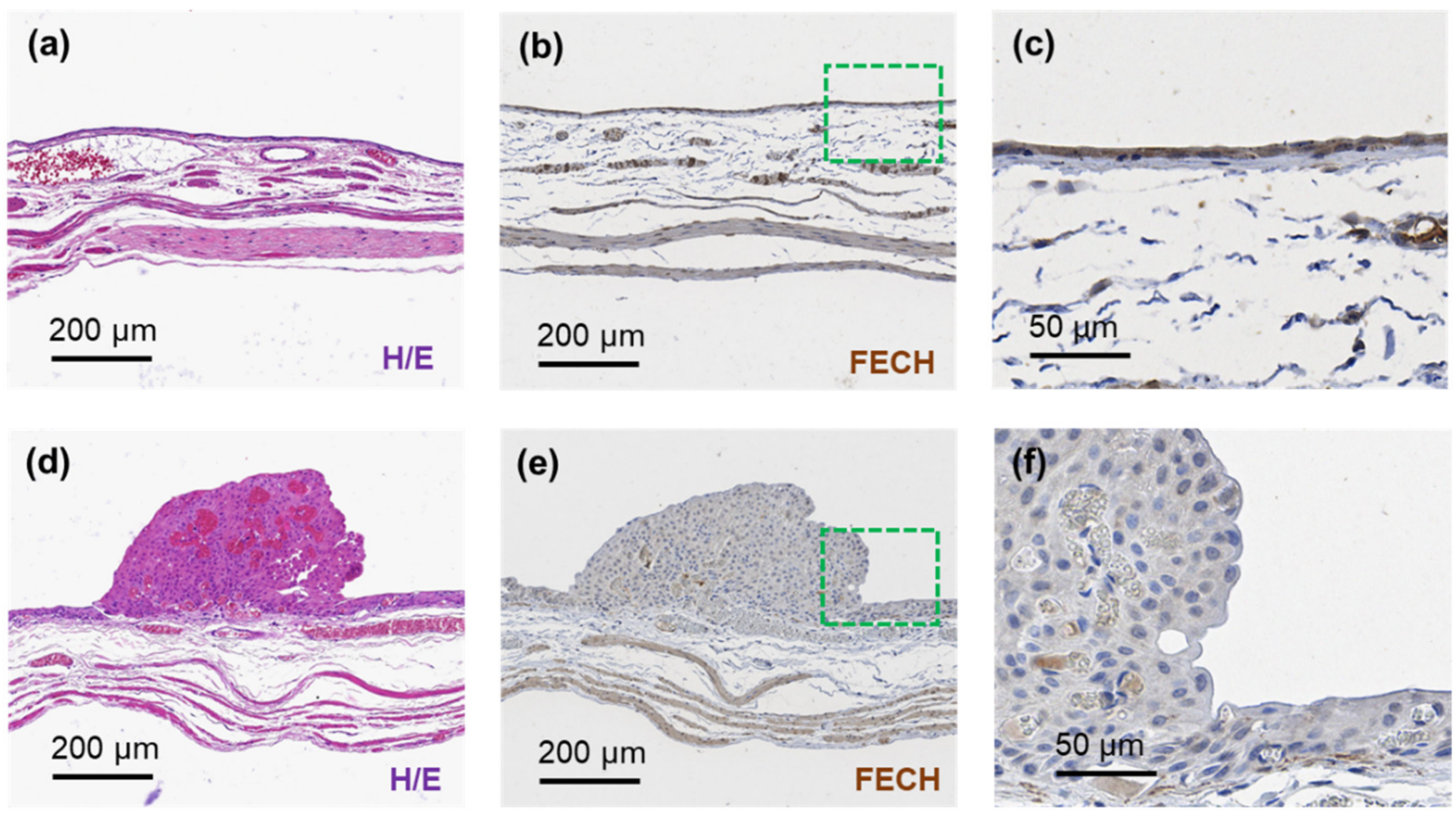
2.4. Hematoxylin/Eosin and Ferrochelatase (FECH) Staining for Bladder Cancer Histopathology
3. Results
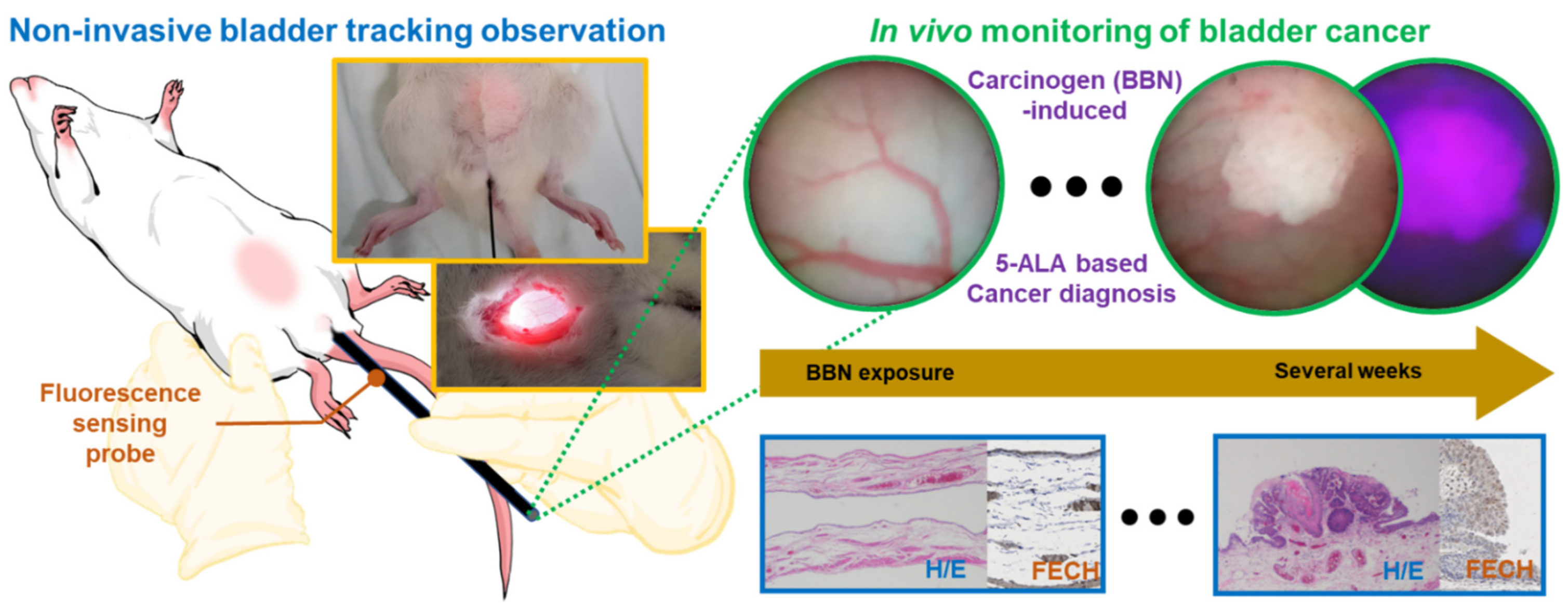
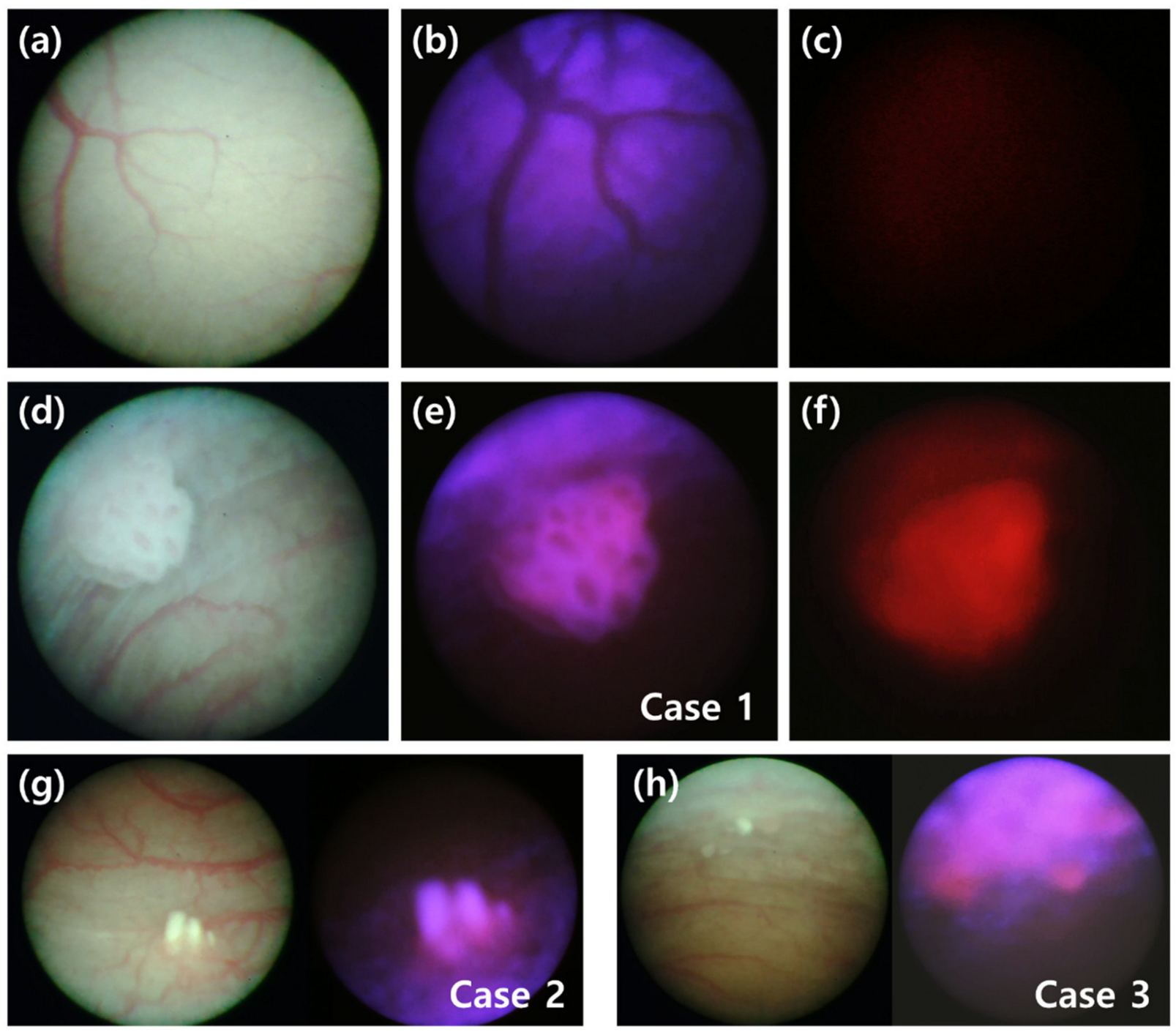
3.1. Minimally Invasive Brightfield and Fluorescence Images of Bladder Cancer In Vivo
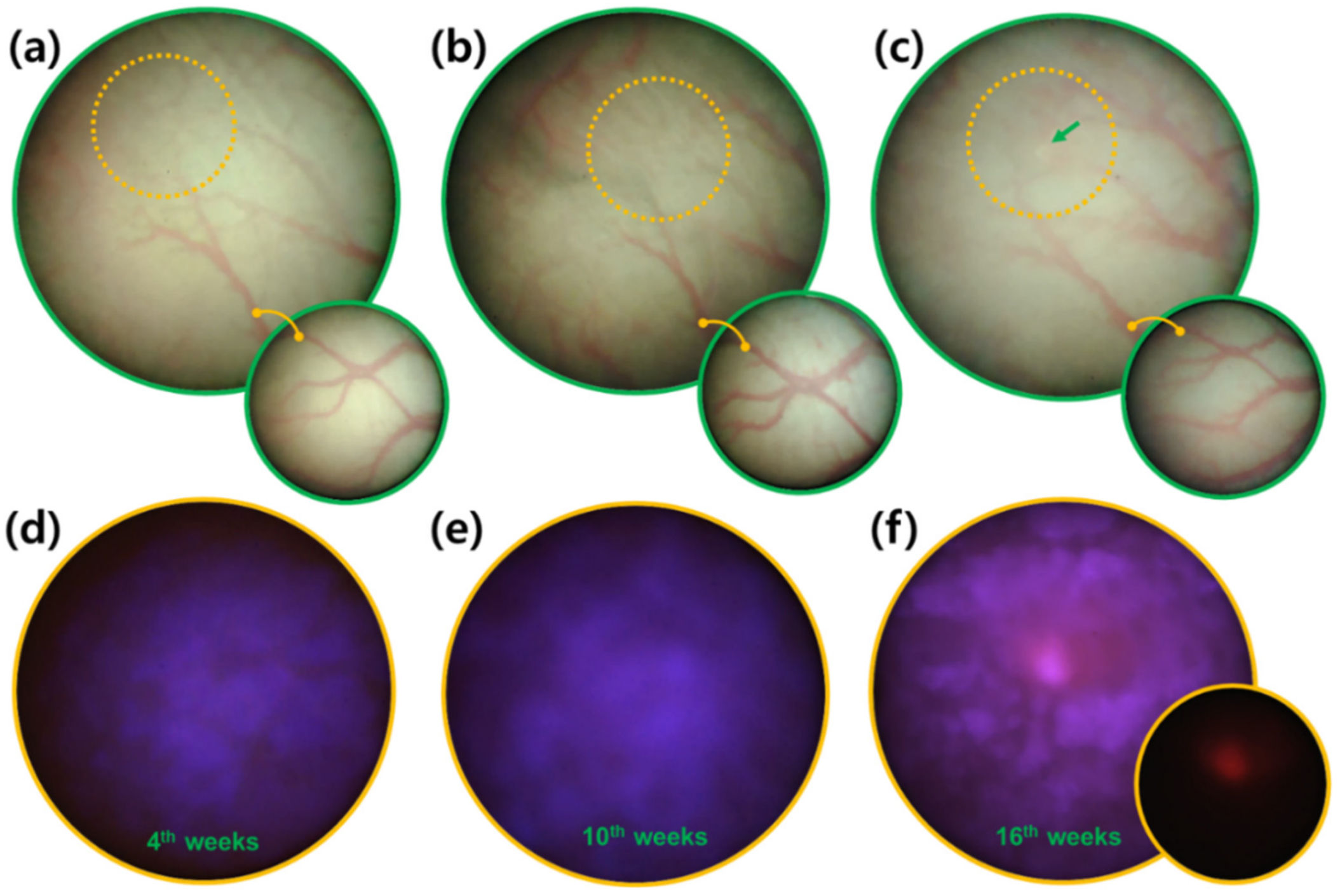
3.2. Early Diagnosis of Bladder Cancer via Fluorescence Sensing Follow-Up
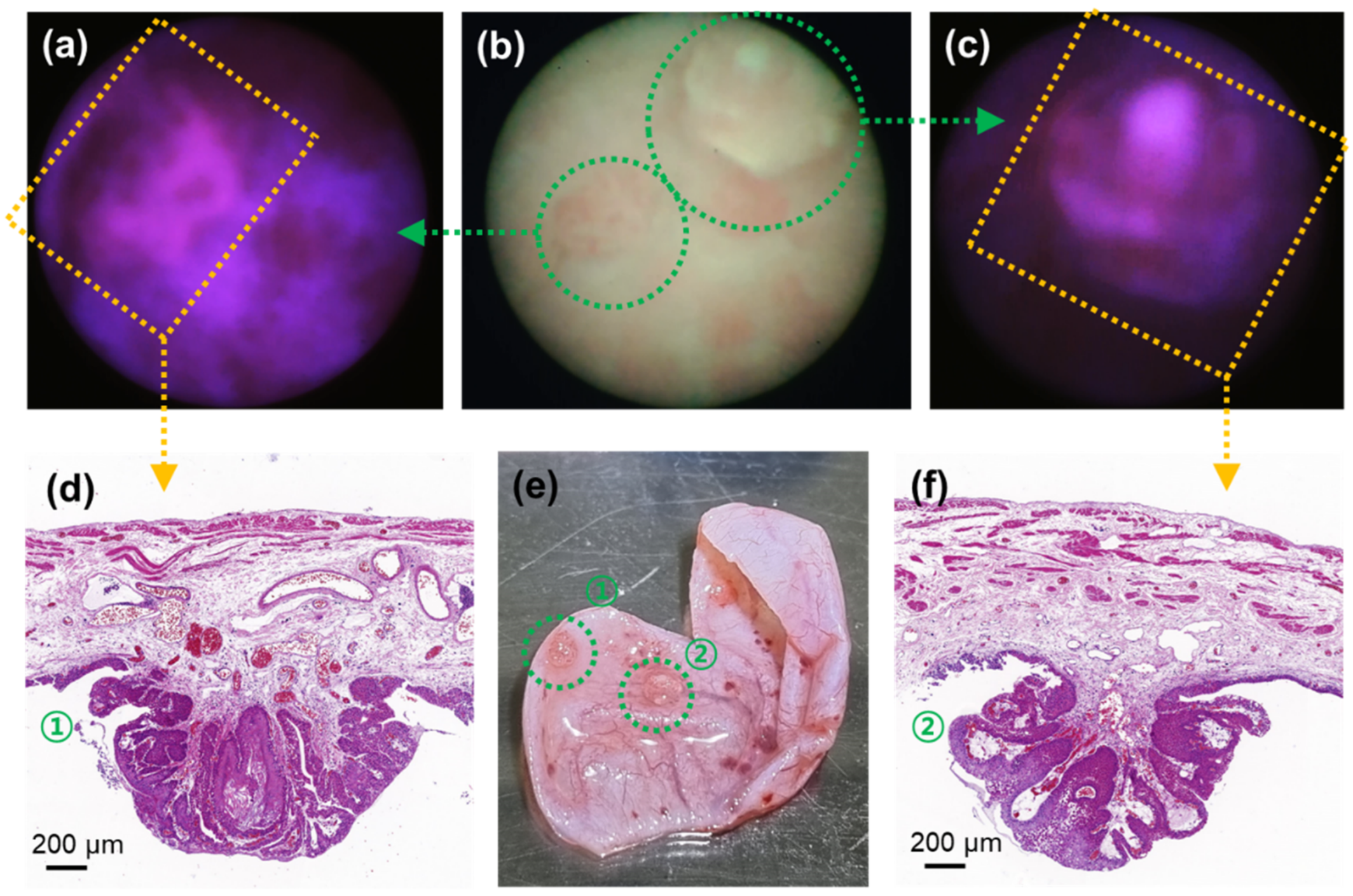
3.3. Tissue Biopsy Validation of Fluorometric Bladder Cancer Images
3.4. Feasibility of Fluorescence Sensing Diagnosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shim, M.G.; Song, L.M.W.M.; Marcon, N.E.; Wilson, B.C. In vivo near-infrared Raman spectroscopy: Demonstration of feasibility during clinical gastrointestinal endoscopy. Photochem. Photobiol. 2000, 72, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Molckovsky, A.; Song, L.M.W.K.; Shim, M.G.; Marcon, N.E.; Wilson, B.C. Diagnostic potential of near-infrared Raman spectroscopy in the colon: Differentiating adenomatous from hyperplastic polyps. Gastrointest. Endosc. 2003, 57, 396–402. [Google Scholar] [CrossRef]
- O’Brien, T.; Thomas, K. Photodynamic diagnosis can improve surgical outcome. Nat. Rev. Urol. 2010, 7, 598–599. [Google Scholar] [CrossRef] [PubMed]
- Lopez, A.; Liao, J.C. Emerging Endoscopic Imaging Technologies for Bladder Cancer Detection. Curr. Urol. Rep. 2014, 15, 406. [Google Scholar] [CrossRef] [Green Version]
- Hendricksen, K.; Molkenboer-Kuenen, J.; Oosterwijk, E.; Hulsbergen-van de Kaa, C.A.; Witjes, J.A. Evaluation of an Orthotopic Rat Bladder Urothelial Cell Carcinoma Model by Cystoscopy. BJU Int. 2008, 101, 889–893. [Google Scholar] [CrossRef] [PubMed]
- Asanuma, H.; Arai, T.; Seguchi, K.; Kawauchi, S.; Satoh, H.; Kikuchi, M.; Murai, M. Successful Diagnosis of Orthotopic Rat Superficial Bladder Tumor Model by Ultrathin Cystoscopy. J. Urol. 2003, 169, 718–720. [Google Scholar] [CrossRef]
- Arentsen, H.C.; Hendricksen, K.; Oosterwijk, E.; Witjes, J.A. Experimental Rat Bladder Urothelial Cell Carcinoma Models. World J. Urol. 2009, 27, 313–317. [Google Scholar] [CrossRef] [Green Version]
- Hadjipanayis, C.G.; Stummer, W. 5-ALA and FDA approval for glioma surgery. J. Neuro-Oncol. 2019, 141, 479–486. [Google Scholar] [CrossRef]
- Koizumi, N.; Harada, Y.; Murayama, Y.; Harada, K.; Beika, M.; Yamaoka, Y.; Dai, P.; Komatsu, S.; Kubota, T.; Ichikawa, D.; et al. Detection of Metastatic Lymph Nodes Using 5-Aminolevulinic Acid in Patients with Gastric Cancer. Ann. Surg. Oncol. 2013, 20, 3541–3548. [Google Scholar] [CrossRef]
- Georges, J.F.; Valeri, A.; Wang, H.; Brooking, A.; Kakareka, M.; Cho, S.S.; Al-Atrache, Z.; Bamimore, M.; Osman, H.; Mach, J.; et al. Delta-Aminolevulinic Acid-Mediated Photodiagnoses in Surgical Oncology: A Historical Review of Clinical Trials. Front. Surg. 2019, 6, 45. [Google Scholar] [CrossRef]
- Lee, J.Y.K.; Cho, S.S.; Stummer, W.; Tanyi, J.L.; Vahrmeijer, A.L.; Rosenthal, E.; Smith, B.; Henderson, E.; Roberts, D.W.; Lee, A.; et al. Review of clinical trials in intraoperative molecular imaging during cancer surgery. J. Biomed. Opt. 2019, 24, 120901. [Google Scholar] [CrossRef]
- Choi, W.; Porten, S.; Kim, S.; Willis, D.; Plimack, E.R.; Hoffman-Censits, J.; Roth, B.; Cheng, T.W.; Tran, M.; Lee, I.L.; et al. Identification of Distinct Basal and Luminal Subtypes of Muscle-Invasive Bladder Cancer with Different Sensitivities to Frontline Chemotherapy. Cancer Cell 2014, 25, 152–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farina, M.S.; Lundgren, K.T.; Bellmunt, J. Immunotherapy in Urothelial Cancer: Recent Results and Future Perspectives. Drugs 2017, 77, 1077–1089. [Google Scholar] [CrossRef]
- Vasconcelos-Nobrega, C.; Colaco, A.; Lopes, C.; Oliveira, P.A. BBN as an Urothelial Carcinogen. In Vivo 2012, 26, 727–739. [Google Scholar]
- Shin, K.; Lim, A.; Odegaard, J.I.; Honeycutt, J.D.; Kawano, S.; Hsieh, M.H.; Beachy, P.A. Cellular origin of bladder neoplasia and tissue dynamics of its progression to invasive carcinoma. Nat. Cell Biol. 2014, 16, 469–478. [Google Scholar] [CrossRef] [Green Version]
- Shin, K.; Lim, A.; Zhao, C.; Sahoo, D.; Pan, Y.; Spiekerkoetter, E.; Liao, J.C.; Beachy, P.A. Hedgehog Signaling Restrains Bladder Cancer Progression by Eliciting Stromal Production of Urothelial Differentiation Factors. Cancer Cell 2014, 26, 521–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gellert, L.L.; Warrick, J.; Al-Ahmadie, H.A. Urothelial carcinoma with squamous differentiation-The pathologists’ perspective. Urol. Oncol. Semin. Orig. Investig. 2015, 33, 437–443. [Google Scholar] [CrossRef]
- Murphy, W.M.; Soloway, M.S.; Jukkola, A.F.; Crabtree, W.N.; Ford, K.S. Urinary Cytology and Bladder-Cancer—The Cellular-Features of Transitional Cell Neoplasms. Cancer 1984, 53, 1555–1565. [Google Scholar] [CrossRef]
- Cheng, L.; MacLennan, G.T.; Lopez-Beltran, A. Histologic grading of urothelial carcinoma: A reappraisal. Hum. Pathol. 2012, 43, 2097–2108. [Google Scholar] [CrossRef]
- Ishizuka, M.; Abe, F.; Sano, Y.; Takahashi, K.; Inoue, K.; Nakajima, M.; Kohda, T.; Komatsu, N.; Ogura, S.; Tanaka, T. Novel development of 5-aminolevurinic acid (ALA) in cancer diagnoses and therapy. Int. Immunopharmacol. 2011, 11, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Nakai, Y.; Tatsumi, Y.; Miyake, M.; Anai, S.; Kuwada, M.; Onishi, S.; Chihara, Y.; Tanaka, N.; Hirao, Y.; Fujimoto, K. Expression of ferrochelatase has a strong correlation in protoporphyrin IX accumulation with photodynamic detection of bladder cancer. Photodiagn. Photodyn. Ther. 2016, 13, 225–232. [Google Scholar] [CrossRef]
- Huang, Y.Y.; Wintner, A.; Seed, P.C.; Brauns, T.; Gelfand, J.A.; Hamblin, M.R. Antimicrobial photodynamic therapy mediated by methylene blue and potassium iodide to treat urinary tract infection in a female rat model. Sci. Rep. 2018, 8, 7257. [Google Scholar] [CrossRef] [PubMed]
- Bochner, B.H.; Cote, R.J.; Weidner, N.; Groshen, S.; Chen, S.C.; Skinner, D.G.; Nichols, P.W. Angiogenesis in Bladder-Cancer—Relationship between Microvessel Density and Tumor Prognosis. J. Natl. Cancer Inst. 1995, 87, 1603–1612. [Google Scholar] [CrossRef]
- Schmidbauer, J.; Witjes, F.; Schmeller, N.; Donat, R.; Susani, M.; Marberger, M.; Hexvix PCB301/01 Study Group. Improved detection of urothelial carcinoma in situ with hexaminolevulinate fluorescence cystoscopy. J. Urol. 2004, 171, 135–138. [Google Scholar] [CrossRef]
- Jichlinski, P.; Guillou, L.; Karlsen, S.J.; Malmström, P.U.; Jocham, D.; Brennhovd, B.; Johansson, E.; Gärtner, T.; Lange, N.; van den Bergh, H.; et al. Hexyl aminolevulinate fluorescence cystoscopy: New diagnostic tool for photodiagnosis of superficial bladder cancer—A multicenter study. J. Urol. 2003, 170, 226–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaak, D.; Karl, A.; Knüchel, R.; Stepp, H.; Hartmann, A.; Reich, O.; Bachmann, A.; Siebels, M.; Popken, G.; Stief, C. Diagnosis of urothelial carcinoma of the bladder using fluorescence endoscopy. BJUI Int. 2005, 96, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Kushibiki, T.; Noji, T.; Ebihara, Y.; Hontani, K.; Ono, M.; Kuwabara, S.; Nakamura, T.; Tsuchikawa, T.; Okamura, K.; Ishizuka, M.; et al. 5-Aminolevulinic-acid-mediated Photodynamic Diagnosis Enhances the Detection of Peritoneal Metastases in Biliary Tract Cancer in Mice. In Vivo 2017, 31, 905–908. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, M.; Tanaka, M.; Ichikawa, H.; Suzuki, T.; Nishie, H.; Ozeki, K.; Shimura, T.; Kubota, E.; Tanida, S.; Kataoka, H. 5-aminolaevulinic acid (5-ALA) accumulates in GIST-T1 cells and photodynamic diagnosis using 5-ALA identifies gastrointestinal stromal tumors (GISTs) in xenograft tumor models. PLoS ONE 2021, 16, e0249650. [Google Scholar] [CrossRef] [PubMed]
- Ohyama, C.; Kawamura, S.; Satoh, M.; Saito, S.; Yoshikawa, K.; Hoshi, S.; Orikasa, S. Endoscopic observation for detection and monitoring of N-butyl-N-(4-hydroxybutyl)nitrosamine--induced bladder tumor in rats. Urol. Res. 1997, 25, 183–186. [Google Scholar] [CrossRef]
- D’Hallewin, M.-A.; El Khatib, S.; Leroux, A.; Bezdetnaya, L.; Guillemin, F. Endoscopic Confocal Fluorescence Microscopy of Normal and Tumor Bearing Rat Bladder. J. Urol. 2005, 174, 736–740. [Google Scholar] [CrossRef]
- Owari, T.; Iwamoto, T.; Anai, S.; Miyake, M.; Nakai, Y.; Hori, S.; Hara, T.; Ishii, T.; Ota, U.; Torimoto, K.; et al. The sustaining of fluorescence in photodynamic diagnosis after the administration of 5-aminolevulinic acid in carcinogen-induced bladder cancer orthotopic rat model and urothelial cancer cell lines. Photodiagn. Photodyn. Ther. 2021, 34, 102309. [Google Scholar] [CrossRef]
- Sroka, R.; Baumgartner, R.; Buser, A.; Ell, C.; Jocham, D.; Unsoeld, E. Laser-Assisted Detection of Endogenous Porphyrins in Malignant Diseases; Mang, T.S., Ed.; SPIE: Los Angeles, CA, USA, 1992; pp. 99–106. [Google Scholar]
- Bolenz, C.; Wenzel, M.; Cao, Y.; Trojan, L.; Häcker, A.; Arancibia, M.F.; Alken, P.; Michel, M.S. Newly Developed Mini-Endoscope for Diagnosis and Follow-Up of Orthotopic Bladder Transitional-Cell Carcinoma in Vivo. J. Endourol. 2007, 21, 789–794. [Google Scholar] [CrossRef]
- Cauberg, E.C.C.; de Bruin, D.M.; Faber, D.J.; van Leeuwen, T.G.; de la Rosette, J.J.M.C.H.; de Reijke, T.M. A New Generation of Optical Diagnostics for Bladder Cancer: Technology, Diagnostic Accuracy, and Future Applications. Eur. Urol. 2009, 56, 287–297. [Google Scholar] [CrossRef]
- Jocham, D.; Stepp, H.; Waidelich, R. Photodynamic Diagnosis in Urology: State-of-the-Art. Eur. Urol. 2008, 53, 1138–1150. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Oh, J.; Cho, M.; Kim, J.K. Fluorescence-Based Microendoscopic Sensing System for Minimally Invasive In Vivo Bladder Cancer Diagnosis. Biosensors 2022, 12, 631. https://doi.org/10.3390/bios12080631
Lee S, Oh J, Cho M, Kim JK. Fluorescence-Based Microendoscopic Sensing System for Minimally Invasive In Vivo Bladder Cancer Diagnosis. Biosensors. 2022; 12(8):631. https://doi.org/10.3390/bios12080631
Chicago/Turabian StyleLee, Sanghwa, Jeongmin Oh, Minju Cho, and Jun Ki Kim. 2022. "Fluorescence-Based Microendoscopic Sensing System for Minimally Invasive In Vivo Bladder Cancer Diagnosis" Biosensors 12, no. 8: 631. https://doi.org/10.3390/bios12080631