Lowering the Sampling Rate: Heart Rate Response during Cognitive Fatigue


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
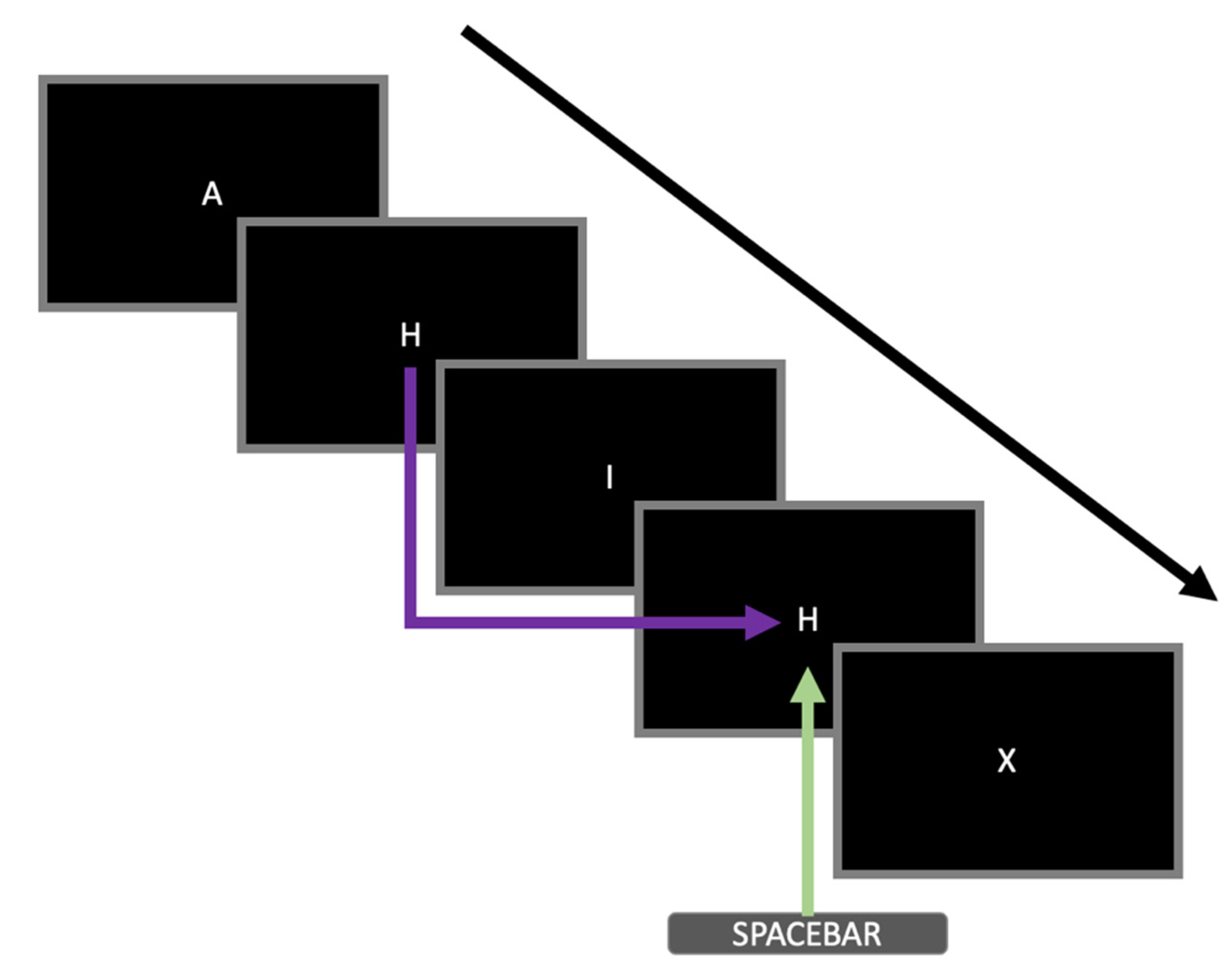
2.2. Cognitive Fatiguing Task
2.3. Electrocardiogram Data Acquisition and Processing
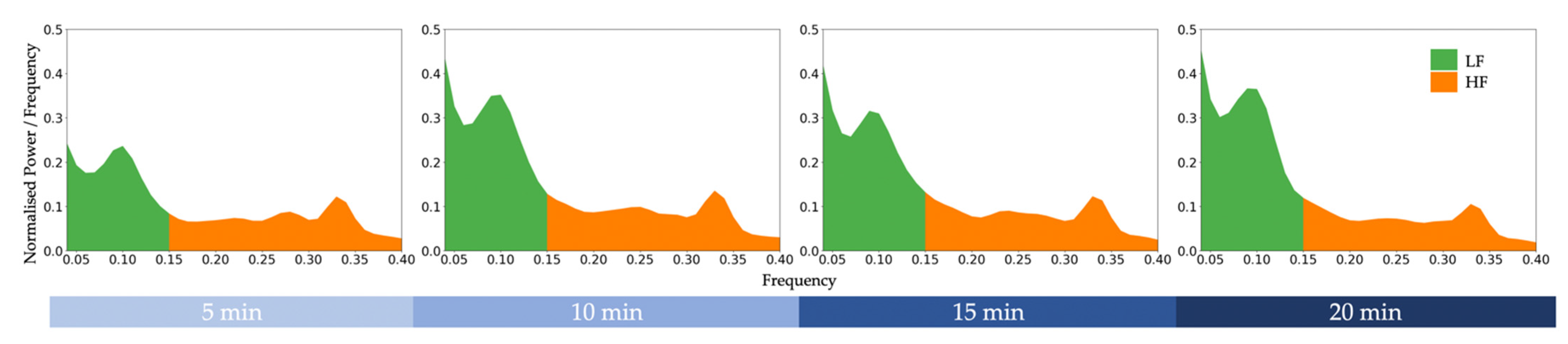
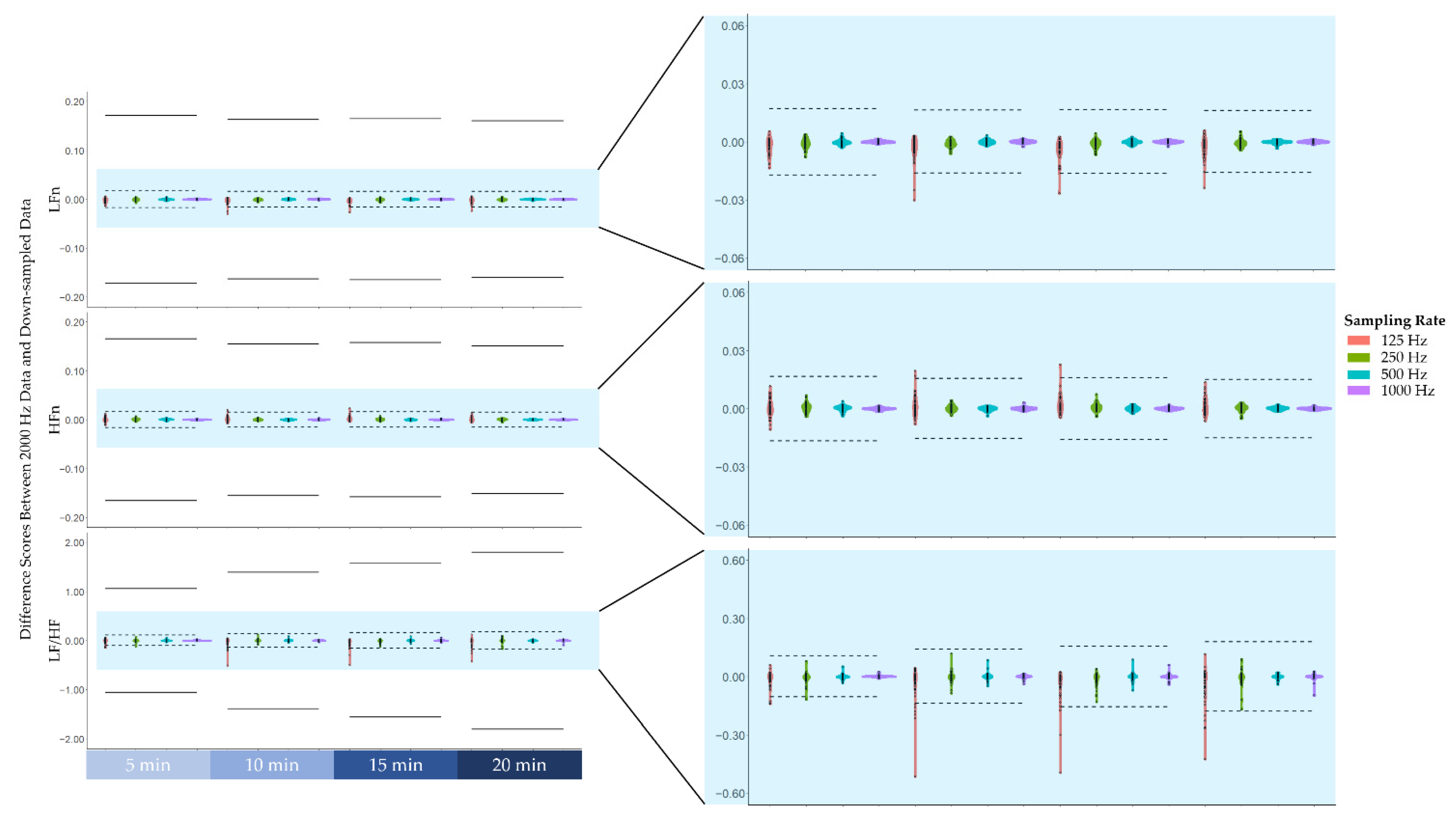
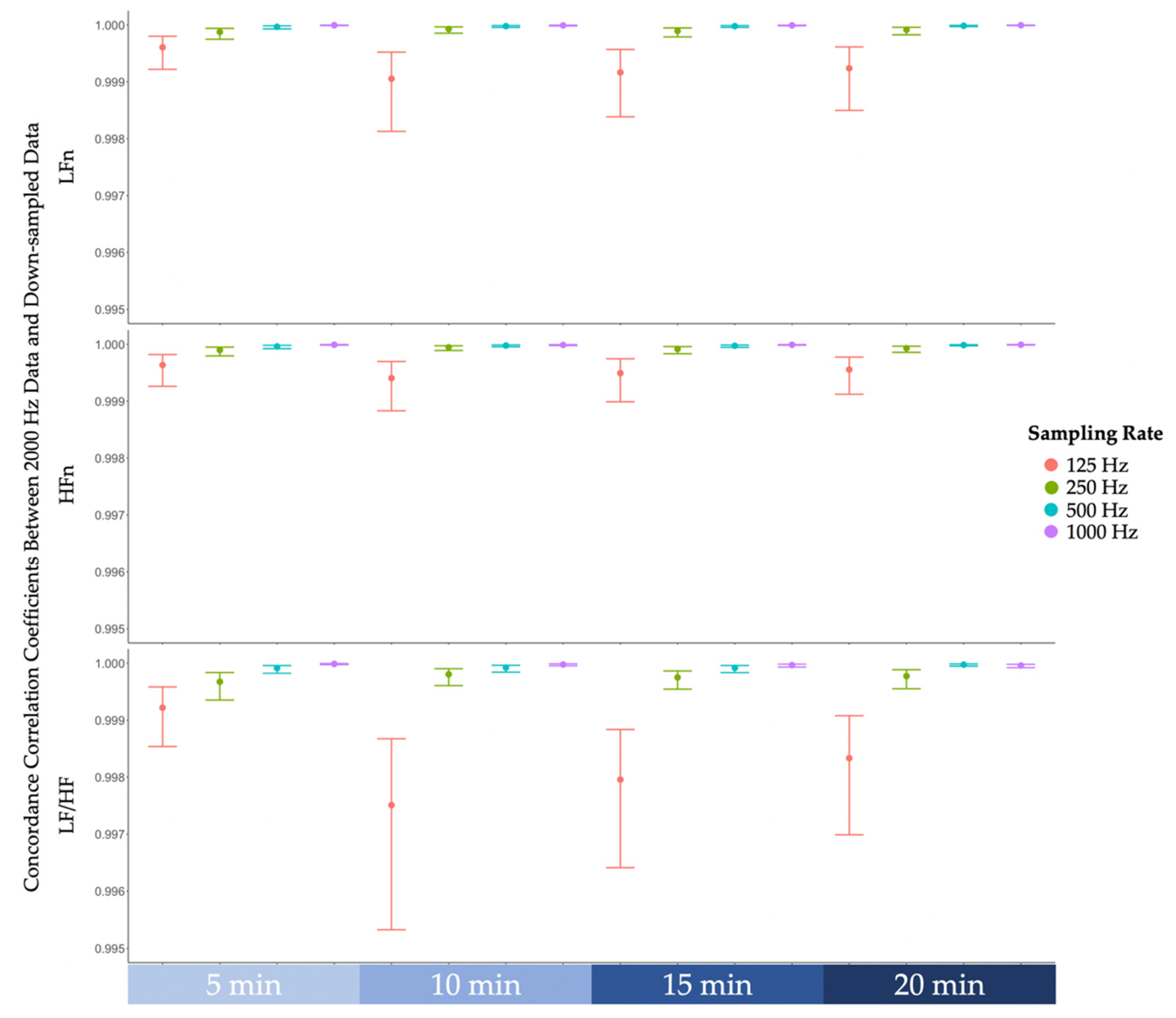
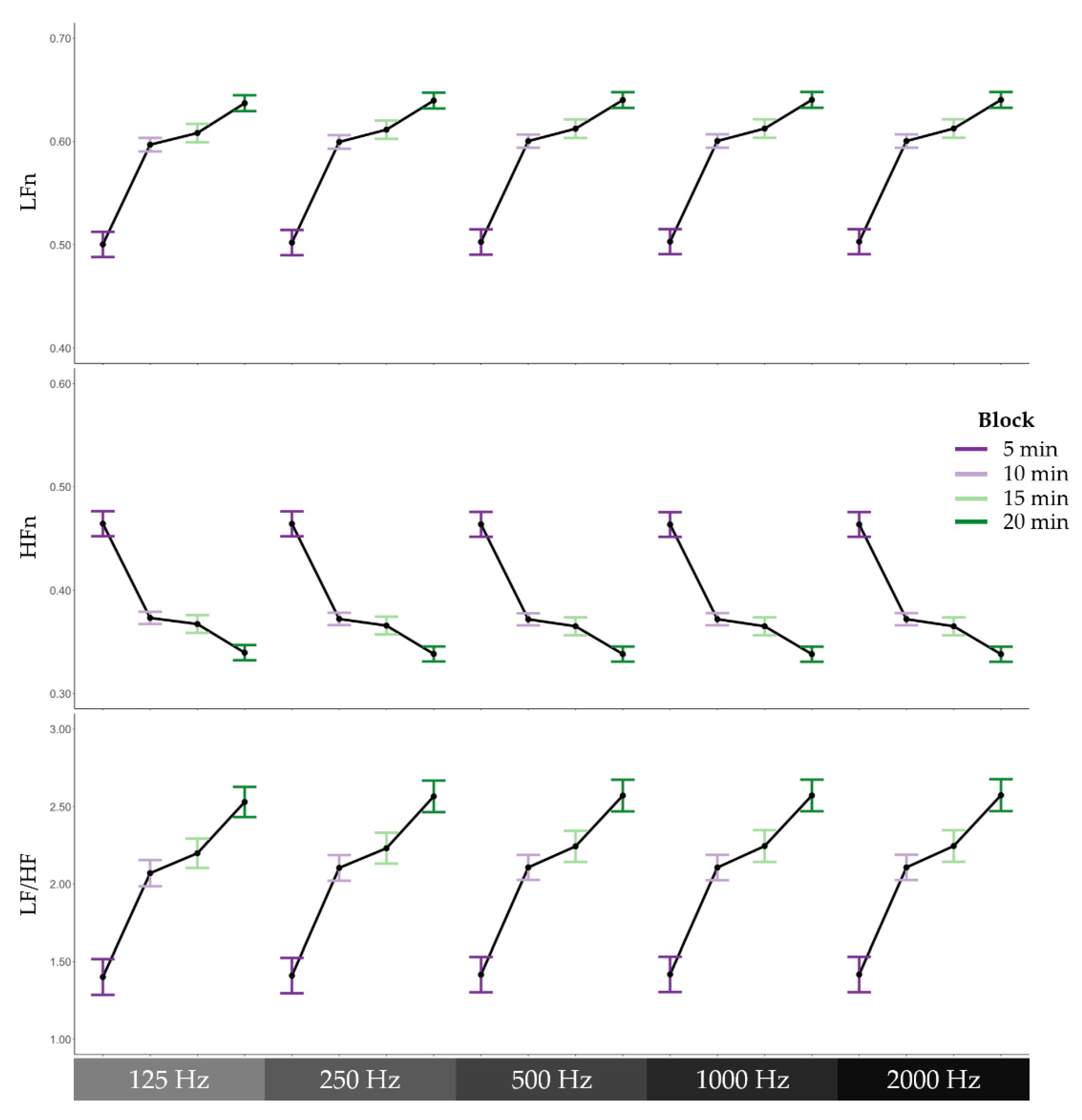
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boksem, M.A.; Tops, M. Mental fatigue: Costs and benefits. Brain Res. Rev. 2008, 59, 125–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kluger, B.M.; Krupp, L.; Enoka, R.M. Fatigue and fatigability in neurologic illnesses: Proposal for a unified taxonomy. Neurology 2013, 80, 409–416. [Google Scholar] [CrossRef]
- Grandjean, E. Fatigue in industry. Occup. Environ. Med. 1979, 36, 175–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Linden, D.; Frese, M.; Meijman, T.F. Mental fatigue and the control of cognitive processes: Effects on perseveration and planning. Acta Psychol. 2003, 113, 45–65. [Google Scholar] [CrossRef]
- Job, R.F.S.; Dalziel, J. Defining Fatigue as a Condition of the Organism and Distinguishing It from Habituation, Adaptation, and Boredom. In Stress, Workload, and Fatigue, 1st ed.; Hancock, P.A., Desmond, P.A., Eds.; CRC Press: Boca Raton, FL, USA, 2008; pp. 466–476, (Original work published 2001). [Google Scholar]
- Subramanyam, M.; Muralidhara, P.; Muralidhara, P. Mental Workload and Cognitive Fatigue: A Study. IUP J. Manag. Res. 2013, XII, 29–39. [Google Scholar]
- Desmond, P.A.; Hancock, P.A. (Eds.) Active and Passive Fatigue States. In Stress, Workload, and Fatigue, 1st ed.; CRC Press: Boca Raton, FL, USA, 2008; pp. 455–465, (Original work published 2001). [Google Scholar]
- Tanaka, M.; Ishii, A.; Watanabe, Y. Effects of Mental Fatigue on Brain Activity and Cognitive Performance: A Magnetoencephalography Study. Anat. Physiol. 2015, 4, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Gergelyfi, M.; Jacob, B.; Olivier, E.; Zénon, A. Dissociation between mental fatigue and motivational state during prolonged mental activity. Front. Behav. Neurosci. 2015, 9, 176. [Google Scholar] [CrossRef] [Green Version]
- Holtzer, R.; Shuman, M.; Mahoney, J.R.; Lipton, R.; Verghese, J. Cognitive Fatigue Defined in the Context of Attention Networks. Aging, Neuropsychol. Cogn. 2011, 18, 108–128. [Google Scholar] [CrossRef]
- Simon, J.; Takács, E.; Orosz, G.; Berki, B.; Winkler, I. Short-term cognitive fatigue effect on auditory temporal order judgments. Exp. Brain Res. 2020, 238, 305–319. [Google Scholar] [CrossRef] [Green Version]
- Al-Mekhlafi, A.A.; Isha, A.S.N.; Naji, G.M.A. The relationship between fatigue and driving performance: A review and directions for future research. J. Crit. Rev. 2020, 7, 134–141. [Google Scholar] [CrossRef]
- Goode, J.H. Are pilots at risk of accidents due to fatigue? J. Saf. Res. 2003, 34, 309–313. [Google Scholar] [CrossRef]
- Lee, K.F.A.; Gan, W.-S.; Christopoulos, G. Biomarker-informed machine learning model of cognitive fatigue from a heart rate response perspective. Sensors 2021, 21, 3843. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Mizuno, K.; Yamaguti, K.; Kuratsune, H.; Fujii, A.; Baba, H.; Matsuda, K.; Nishimae, A.; Takesaka, T.; Watanabe, Y. Autonomic nervous alterations associated with daily level of fatigue. Behav. Brain Funct. 2011, 7, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fairclough, S.H.; Venables, L.; Tattersall, A. The influence of task demand and learning on the psychophysiological response. Int. J. Psychophysiol. 2005, 56, 171–184. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Jiao, K.; Chen, M.; Yang, Y.; Wang, C.; Qi, S. Spectral analysis of heart rate variability as a quantitative indicator of driver mental fatigue. SAE Tech. Pap. 2002, 111, 249–253. [Google Scholar] [CrossRef]
- Zhang, C.; Yu, X. Estimating mental fatigue based on electroencephalogram and heart rate variability. Pol. J. Med. Phys. Eng. 2010, 16, 67–84. [Google Scholar] [CrossRef] [Green Version]
- Bernardi, L.; Leuzzi, S.; Radaelli, A.; Passino, C.; Johnston, J.A.; Sleight, P. Low-frequency spontaneous fluctuations of R-R interval and blood pressure in conscious humans: A baroreceptor or central phenomenon? Clin. Sci. 1994, 87, 649–654. [Google Scholar] [CrossRef]
- Pagani, M.; Lombardi, F.; Guzzetti, S.; Rimoldi, O.; Furlan, R.; Pizzinelli, P.; Sandrone, G.; Malfatto, G.; Dell’Orto, S.; Piccaluga, E. Power spectral analysis of heart rate and arterial pressure variabilities as a marker of sympatho-vagal interaction in man and conscious dog. Circ. Res. 1986, 59, 178–193. [Google Scholar] [CrossRef] [Green Version]
- Kleiger, R.E.; Stein, P.K.; Bigger, J.T., Jr. Heart rate variability: Measurement and clinical utility. Ann. Noninvasive Electrocardiol. 2005, 10, 88–101. [Google Scholar] [CrossRef]
- Rahman, F.; Pechnik, S.; Gross, D.; Sewell, L.; Goldstein, D.S. Low frequency power of heart rate variability reflects baroreflex function, not cardiac sympathetic innervation. Clin. Auton. Res. 2011, 21, 133–141. [Google Scholar] [CrossRef] [Green Version]
- Pomeranz, B.; Macaulay, R.J.B.; Caudill, M.A.; Kutz, I.; Adam, D.; Gordon, D.; Kilborn, K.M.; Barger, A.C.; Shannon, D.C.; Cohen, R.J.; et al. Assessment of autonomic function in humans by heart rate spectral analysis. Am. J. Physiol. Heart Circ. Physiol. 1985, 248, H151–H153. [Google Scholar] [CrossRef]
- Malliani, A.; Lombardi, F.; Pagani, M. Power spectrum analysis of heart rate variability: A tool to explore neural regulatory mechanisms. Br. Heart J. 1994, 71, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamišalić, A.; Fister, I.; Turkanović, M.; Karakatič, S. Sensors and functionalities of non-invasive wrist-wearable devices: A review. Sensors 2018, 18, 1714. [Google Scholar] [CrossRef] [Green Version]
- Athavale, Y.; Krishnan, S. Biosignal monitoring using wearables: Observations and opportunities. Biomed. Signal Process. Control 2017, 38, 22–33. [Google Scholar] [CrossRef]
- Task Force of the European Society of Cardiology the North American Society of Pacing Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Merri, M.; Farden, D.C.; Mottley, J.G.; Titlebaum, E.L. Sampling frequency of the electrocardiogram for spectral analysis of the heart rate variability. IEEE Trans. Biomed. Eng. 1990, 37, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Ziemssen, T.; Gasch, J.; Ruediger, H. Influence of ECG sampling frequency on spectral analysis of RR intervals and baroreflex sensitivity using the EUROBAVAR data set. J. Clin. Monit. Comput. 2008, 22, 159. [Google Scholar] [CrossRef] [PubMed]
- Kwon, O.; Jeong, J.; Kim, H.B.; Kwon, I.H.; Park, S.Y.; Kim, J.E.; Choi, Y. Electrocardiogram sampling frequency range acceptable for heart rate variability analysis. Healthc. Inform. Res. 2018, 24, 198–206. [Google Scholar] [CrossRef]
- Ellis, R.J.; Zhu, B.; Koenig, J.; Thayer, J.F.; Wang, Y. A careful look at ECG sampling frequency and R-peak interpolation on short-term measures of heart rate variability. Physiol. Meas. 2015, 36, 1827–1852. [Google Scholar] [CrossRef] [Green Version]
- Tudosa, I.; Adochiei, N. LMS algorithm derivatives used in real-time filtering of ECG signals: A study case on performance evaluation. In Proceedings of the 2012 International Conference and Exposition on Electrical and Power Engineering, Iasi, Romania, 25–27 October 2012; Haba, C.-G., Chiriac, G., Eds.; IEEE: Piscataway, NJ, USA, 2012; pp. 565–570. [Google Scholar]
- Kirchner, W.K. Age differences in short-term retention of rapidly changing information. J. Exp. Psychol. 1958, 55, 352–358. [Google Scholar] [CrossRef]
- Tanaka, M.; Mizuno, K.; Tajima, S.; Sasabe, T.; Watanabe, Y. Central nervous system fatigue alters autonomic nerve activity. Life Sci. 2009, 84, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Makowski, D.; Pham, T.; Lau, Z.J.; Brammer, J.C.; Lespinasse, F.; Pham, H.; Schölzel, C.; Chen, S.H.A. NeuroKit2: A Python toolbox for neurophysiological signal processing. Behav. Res. Methods 2021, 53, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Welch, P. The use of fast Fourier transform for the estimation of power spectra: A method based on time averaging over short, modified periodograms. IEEE Trans. Audio Electroacoust. 1967, 15, 70–73. [Google Scholar] [CrossRef] [Green Version]
- Lin, L.I.-K. A concordance correlation coefficient to evaluate reproducibility. Biometrics 1989, 45, 255–268. [Google Scholar] [CrossRef] [PubMed]
- McBride, G.B. A Proposal for Strength-of-agreement Criteria for Lin’s Concordance Correlation Coefficient; HAM2005-062; NIWA Client Report for the Ministry of Health: Hamilton, New Zealand, 2005. [Google Scholar]
- Satterthwaite, F.E. Synthesis of variance. Psychometrika 1941, 6, 309–316. [Google Scholar] [CrossRef]
- Nyquist, H. Certain topics in telegraph transmission theory. Trans. Am. Inst. Electr. Eng. 1928, 47, 617–644. [Google Scholar] [CrossRef]
- Shannon, C.E. Communication in the presence of noise. Proc. IRE 1949, 37, 10–21. [Google Scholar] [CrossRef]
- Shannon, C.E. A mathematical theory of communication. Bell Syst. Tech. J. 1948, 27, 379–423. [Google Scholar] [CrossRef] [Green Version]
- Nyquist, H. Certain factors affecting telegraph speed. Trans. Am. Inst. Electr. Eng. 1924, 43, 412–422. [Google Scholar] [CrossRef]
- Hartley, R.V.L. Transmission of information. Bell Syst. Tech. J. 1928, 7, 535–563. [Google Scholar] [CrossRef]
- Gersten, A.; Gersten, O.; Ronen, A.; Cassuto, Y. The RR interval spectrum, the ECG signal, and aliasing. In Fourier Transforms—Century of Digitalization and Increasing Expectations; Nikolić, G.S., Marković-Nikolić, D.Z., Eds.; IntechOpen: London, UK, 2019; pp. 1–17. [Google Scholar]
- Bousseljot, R.; Kreiseler, D.; Schnabel, A. Nutzung der EKG-signaldatenbank CARDIODAT der PTB über das internet. Biomed. Tech. 1995, 40, 317–318. [Google Scholar] [CrossRef]
- Wang, D.; Wu, Y.; Wang, A.; Chen, Y.; Zhang, T.; Hu, N. Electrocardiogram changes of donepezil administration in elderly patients with ischemic heart disease. Cardiol. Res. Pract. 2018, 2018, 9141320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park-Wyllie, L.Y.; Mamdani, M.M.; Li, P.; Gill, S.S.; Laupacis, A.; Juurlink, D.N. Cholinesterase inhibitors and hospitalization for bradycardia: A population-based study. PLoS Med. 2009, 6, e1000157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dickinson, D.F. The normal ECG in childhood and adolescence. Heart 2005, 91, 1626–1630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.-Y.; Chu, C.-H. Analysis of energy consumption for wearable ECG devices. In Proceedings of the SENSORS, 2014 IEEE, Valencia, Spain, 2–5 November 2014; IEEE: Piscataway, NJ, USA, 2014; pp. 962–965. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HRV | Block 1 (5 min) | Block 2 (10 min) | Block 3 (15 min) | Block 4 (20 min) | ||||
|---|---|---|---|---|---|---|---|---|
| Features | M | SD | M | SD | M | SD | M | SD |
| 2000 Hz | ||||||||
| LFn | 0.50 | 0.17 | 0.60 | 0.16 | 0.61 | 0.16 | 0.64 | 0.16 |
| HFn | 0.46 | 0.17 | 0.37 | 0.15 | 0.36 | 0.16 | 0.34 | 0.15 |
| LF/HF | 1.42 | 1.06 | 2.11 | 1.39 | 2.24 | 1.56 | 2.57 | 1.80 |
| 1000 Hz | ||||||||
| LFn | 0.50 | 0.17 | 0.60 | 0.16 | 0.61 | 0.16 | 0.64 | 0.16 |
| HFn | 0.46 | 0.17 | 0.37 | 0.15 | 0.36 | 0.16 | 0.34 | 0.15 |
| LF/HF | 1.42 | 1.06 | 2.11 | 1.39 | 2.24 | 1.57 | 2.57 | 1.79 |
| 500 Hz | ||||||||
| LFn | 0.50 | 0.17 | 0.60 | 0.16 | 0.61 | 0.16 | 0.64 | 0.16 |
| HFn | 0.46 | 0.17 | 0.37 | 0.15 | 0.36 | 0.16 | 0.34 | 0.15 |
| LF/HF | 1.42 | 1.06 | 2.11 | 1.39 | 2.24 | 1.56 | 2.57 | 1.79 |
| 250 Hz | ||||||||
| LFn | 0.50 | 0.17 | 0.60 | 0.16 | 0.61 | 0.16 | 0.64 | 0.16 |
| HFn | 0.46 | 0.17 | 0.37 | 0.15 | 0.37 | 0.16 | 0.34 | 0.15 |
| LF/HF | 1.41 | 1.05 | 2.10 | 1.40 | 2.23 | 1.55 | 2.57 | 1.79 |
| 125 Hz | ||||||||
| LFn | 0.50 | 0.17 | 0.60 | 0.16 | 0.61 | 0.16 | 0.64 | 0.16 |
| HFn | 0.46 | 0.16 | 0.37 | 0.15 | 0.37 | 0.16 | 0.34 | 0.15 |
| LF/HF | 1.40 | 1.04 | 2.07 | 1.34 | 2.20 | 1.51 | 2.53 | 1.74 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, K.F.A.; Chan, E.; Car, J.; Gan, W.-S.; Christopoulos, G. Lowering the Sampling Rate: Heart Rate Response during Cognitive Fatigue. Biosensors 2022, 12, 315. https://doi.org/10.3390/bios12050315
Lee KFA, Chan E, Car J, Gan W-S, Christopoulos G. Lowering the Sampling Rate: Heart Rate Response during Cognitive Fatigue. Biosensors. 2022; 12(5):315. https://doi.org/10.3390/bios12050315
Chicago/Turabian StyleLee, Kar Fye Alvin, Elliot Chan, Josip Car, Woon-Seng Gan, and Georgios Christopoulos. 2022. "Lowering the Sampling Rate: Heart Rate Response during Cognitive Fatigue" Biosensors 12, no. 5: 315. https://doi.org/10.3390/bios12050315